Abstract
This article presents an overview of the current research literature that reveals some controversy, discussion of the need for more research, and report of some definitive success. In addition, four case studies of hair pulling and thumb-sucking are highlighted.
INTRODUCTION
The suggested correlation between multiple behavioral habits is not new to the literature. You just have to dig deep to find it. Multiple resources in a variety of professions have done limited studies with similar outcomes. Ultimately, the postulation is often the same. Eliminate the thumb habit, and the hair pulling will follow. However, often the techniques that have been utilized to achieve this goal, and subsequently reported in the literature, have been less than positive. There is potential for Certified Orofacial Myologists (COM) to play a crucial role in informing parents, the public, and the research community on how the positive techniques that have been in used in orofacial myology treatment for over 30 years could make a vast contribution to this process. This article focuses on providing information for the orofacial myologist on hair pulling that may occur as a concomitant behavior with thumb-sucking or other digit habit. This article does not suggest that hair pulling is within the scope of practice for an orofacial myologist. However, when hair pulling does occur as a concomitant behavior, the orofacial myologist has a responsibility to be informed about the topic.
THE ROLE OF THE OROFACIAL MYOLOGIST
A certified orofacial myologist is familiar with the techniques utilized for the elimination of a retained digit sucking habit. Certified orofacial myologists would most likely agree that the preferred therapy process used for a complex and potentially life-changing issue such as an oral habit is to approach this behavior by utilizing a positive approach. COMs traditionally utilize a positive behavior modification program in their practices to help encourage a variety of changes in oral habit behavior.
Van Norman discussed her success with thumb-sucking elimination utilizing a positive approach in her landmark analysis published in the IJOM in 1997. This analysis consisted of 732 patients utilizing multi-faceted, organized, and supportive positive habit elimination techniques. Utilizing a positive approach, Van Norman concluded that 87% of subjects studied displayed complete cessation in thumb-sucking behavior, with 79% habit cessation occurring within the first day of treatment. This comprehensive review reinforces the idea that using a positive approach is an effective and desirable protocol for the elimination of a thumb-sucking habit with the right client. Positive techniques are critical to the essence of what orofacial myologists do, and who orofacial myologists are. Certified orofacial myologists are extensively trained in using positive techniques. Certified orofacial myologists are expected to be able to demonstrate exceptional proficiency with these essential skills. For those unfamiliar with techniques used by orofacial myologists, the premise of the techniques used are based on third party support by the parent/s or primary caregiver. Habit cessation programs developed by orofacial myologists are designed specifically for each individual within the consistent framework of a positive approach, after thorough interview and brainstorming with the parent/s caregivers or other professionals who may be involved with the child. Consistent monitoring by the orofacial myologist continues for a minimum of sixty days. The family is heavily engaged in the process, and the child is encouraged to take ownership for their habit.
As clinicians, COMs are dealing with changing a life-long habit - A life-long habit in a child. This is frustrating, challenging, and of course, extremely rewarding. The children enrolled for treatment have often been chronically and habitually teased, despite having made diligent efforts to change their own behaviors. However, despite their best efforts, some children continue to fail. Many children become fearful to attend school, begin to withdraw from social situations, or exhibit a change in affect. If this were any other significant life challenge or transition, finding the child a support system of engaged and compassionate experts to help assist them on their journey would be a priority. The journey of habit elimination encompasses many of the characteristics of a transition or loss.
TRICHOTILLOMANIA, TTM, OR ‘TRICH’ - WHAT IS IT?
Trichotillomania (TTM), hair pulling or ‘trich’ is defined by the Mayo Clinic staff (www.MayoClinic.com/health/trichotillomania, 2009) as “an irresistible urge to pull out hair from your scalp, eyebrows or other areas of your body”. According to Bruce, Barwick, and Wright, (2005), trich appears to span all age groups and peak in the pre-school years and adolescence. There is some research being conducted to identify the probable causes, but as stated by The Mayo Clinic, trich is most likely the result of genetic and environmental factors.
Some researchers have felt that there is a possible link between trich and Tourette’s Syndrome (a neurological movement and sound related disorder) via the Slit and Trk-like 1 (SLITRK1) gene. These researchers include, Abelson, (2005), and Stillman, Krsnik, Sun, Rasin, State, Sestan, and Louvi, (2009).
In 1996, researchers Christenson and Crow note that comorbid OCD and TTM are common, and these two behaviors via neurobiological investigations demonstrated both differences and similarities between OCD and TTM via paralleled etiologic studies. They note current treatment includes selective serotonin reuptake inhibitors (SSRI), hypnosis, and behavioral habit reversal. They note TTM is an impulse control disorder.
Meunier, Tolin, and Franklin, (2009), however question if TTM should be judged as an impulse control disorder. Shusterman, Feld, Baer, and Keuthen, (2009), conducted large-scale research exploring the relationship between affective regulation and TTM. They found a small to moderate relationship was suggested between affective regulation and TTM that suggested a link between the regulation of emotion with triggers for TTM and its severity.
The researchers appear to be agreeing, and agreeing to disagree. As paraphrased from an update on pathological skin picking, Grant and Odlaug, (2009), the repetitive and compulsive behaviors seen in PSP are phenomenologically and clinically similar to the behaviors seen in obsessive-compulsive disorder and other body-focused repetitive behaviors, such as trichotillomania and pathological nail biting (NB). Trichotillomania is attributed to be ‘clinically similar’ to nail-biting (Odlug et al, 2009), and nail biting which may be considered a form of pathological skin picking occasionally appears to co-exist with thumb-sucking behavior. Some researchers speculate a possible connection between trichotillomania and thumb-sucking (Grant and Odlaug, 2009; Bohne, Keithen, Wilhelm, 2005). Bohne et al (2005), indicated that PSP, TTM, and NB do appear to be viewed as similar in the literature. They further suggest this represents a joint diagnostic categorization. This research also seemed to indicate that PSP, hair pulling, and nail biting are related specifically by the fact that the consequences, triggers, functionality, and phenomenology all appear similar in nature.
In the body of research encompassing a larger subject population on concomitant habits with hair behavior and digit habits, Troster’s (1994) study is noteworthy in linking the concomitant habits of hair twisting and thumb-sucking . Troster conducted research regarding typical situations where various stereotyped habitual activities occurred and their prevalence in a subset of 142 non-handicapped subjects in residential care, age 10 months to 11 years. He reported that preliminary findings suggest that children with concomitant thumb-sucking and hair twisting both occurred predominantly in isolation with boredom and monotony, while other various stereotyped behaviors seemed to occur in different situations. For example, he indicated that pulling faces and scratching occurred most frequently in isolation with arousal/frustration, and concentration/demand situations.
According to Bruce, Barwick, and Wright (2009) there have been no controlled treatment trials in child and adolescent populations regarding the underlying cause/s, the course of the behavior. He indicated that treatment procedures for TTM need to be defined. He suggests that although first line single behavioral based modalities do appear promising when treating TTM, controlled studies of single modalities and combined treatment approaches are clearly needed. Other researchers agree that more research desperately needs to be conducted in this area (Munier, 2009; Shusterman, Feld, Baer, Keuthen, 2009; Bruce, et al, 2005; Christenson & Crow, 1996).
Additional insight into trichotillomania may be gained by reviewing the following quotes from trich sufferers on their own experience of this behavior from descriptions taken from their web journals at trichotillomaniaBlog.com/PullingOutHair (2009).
- mspennylane “... one of their first questions might be ‘does it hurt when you pull your hair out?’. They might also silently wonder if what you are doing is a form of self-harm, and if the pain is the main reason that you do it. The main point for me, and for anyone else who pulls out their hair, is that it feels good. Even if there is some pain, the main reason we do it is that it feels good”.
- Lizzie “…the pain/pleasure thing: pulling single hairs causes minute degrees of pain and as a result of the shock of that pain (which for some may be imperceptible at this point) the body sends endorphins/natural painkillers to sooth that pain. I sincerely believe that that is what we are addicted to–the body’s natural pain killers, which it sends to a very sensitive part of your body (face/head). We pull because we want the calming effect associated with these endorphin fixes”.
- Daniela “But….I feel awful about myself. I hate that this physical sensation is craved so much by my body and my mind that I let it ruin every other aspect. I pray this will stop”.
- C.C. Lemons “I do it because it’s very calming to me. If I’m under a lot of stress, the sensation isn’t so much painful as it is just a distraction from whatever is troubling me”.
- Delilah “I pull out my hair too and the strange thing is,...I never realize when I start to pull, I just find myself in the middle”.
- ms.pennylane “Yes, I do it subconsciously too. Sometimes I’ll notice once my head does start to hurt a little. But I think I can relate to what you are saying about a pleasant twinge of pain. It feels good”.
- Teenage Trichster “It’s that subconscious thing that I just can’t seem to control…but we’ve all been there, right”?
The website, Trich.org, (2009), has shed some light on a suggested first line treatment of choice for most children and adolescents with isolated trich, (although medical intervention may be utilized when warranted). This site states, “ behavior therapy should be considered as the initial treatment of choice, adding a common behavior therapy approach for trichotillomania is called ‘habit reversal.’ It involves increasing the person’s awareness of each occurrence of hair pulling and interrupting it by performing a response that competes with that behavior. Techniques to increase awareness of hair pulling include identifying triggers and sequences of events associated with hair pulling”.
Bruce, et al, (2005), also reports favorably on that particular behavioral model and the modality also mentioned by Trich.org. According to Bruce, case reports favor a behavioral approach as the first-line single modality of treatment for trich independent of other variables. He suggests that first line single behavioral-based modalities do appear promising.
DIGIT HABITS
Pleasure is one of the common elements between trich and thumb-sucking. In Van Norman’s (1997) narrative, she indicates that “ When infants are given a pacifier or discover their thumb, and the comforting, pleasurable physical associations of sucking, they repeat the behavior” (p15). Thumb-sucking is pleasurable for the majority of our clients thus positively reinforcing the behavior. Most children will continue to suck in the presence of cracked or open skin or skin irregularities, red and engorged thumbs, and medically diagnosed dermatitis, etc. Despite the presence of a sore finger or thumb, their sucking will, for the most part, continue even if there is some pain, they will continue sucking because it feels good.
Van Norman (2001) relates that alterations in brain chemistry as a result of thumb-sucking behavior created by mood fluctuations via neurotransmitter level changes may be a factor in the relaxation response of thumb-sucking. Relaxation is a result of this neurotransmitter shift and lowering of neurotransmitter levels. This is what makes digit sucking so calming and relaxing to most children. The basis of the neurotransmitter shift is the production of beta endorphin. Endorphin production during the sucking process may have the potential to alleviate discomfort and pain as the child sucks, self-soothes and ultimately relaxes.
TRICHOTILLOMANIA and DIGIT HABITS
It is indeed possible to find a few studies by researchers that link small populations of individuals who experienced cessation of their trichotillomania/hair pulling as the result of eliminating their coexisting chained behavior of thumb-sucking. They are there, buried deep in the literature. However, the majority of the research that is available to review appears to be written and reported by clinicians who choose to utilize more negatively based techniques. However, a positive approach can and has been successfully utilized in this venue. It has not been extensively reported, and it often remains anecdotal in nature.
Meunier, et al, 2009, confirms that repeated hair pulling is associated with pleasure and pain whereas recent hair pulling was associated with pleasure only. He concludes that research seems to indicate that hair pulling is reinforced by positive feelings of pleasure and thus is maintained primarily through reinforcement. The subconscious nature of their hair pulling behavior is indicated in Delliah’s, mspennylane’s, and Teenage Trichster’s comments above. It is generally accepted by orofacial myologists that thumb-sucking is also a subconscious behavior. In discussing thumb-sucking, Green (1998) indicated that many children often are not aware they are doing it. In addition, thumb-sucking behavior tends to appear more frequently in times of stress, fatigue, boredom, upset, fear, hunger, etc. (Van Norman, 2001).
Shusterman et al (2009) confirms that confirms that cycles of emotional states induce, reinforce, or otherwise contribute to hair pulling behavior. Troster’s (1994) research suggested that children with concomitant thumb-sucking and hair twisting both occurred predominantly in isolation with boredom and monotony.
As noted above, it appears Trich.org and Bruce, et al (2005) are on the right track independently regarding the need for further treatment exploration for trich, but how does this relate to thumb-sucking? A behavioral approach has been the orofacial myologist’s model for successful thumb-sucking elimination for over thirty years. Practical applications and strategies, although unpopular, exist within the research community when both trich and thumb behaviors coincide.
According to Friman and Hove, (1987) it was concluded that concomitant successful treatment of thumb-sucking as the primary goal, resulted in hair pulling cessation. They suggest that their study results seem to indicate that this indirect approach is an efficient method for changing behaviors that are difficult to treat directly. However, a limitation of their work is the small study population of only two subjects. The exclusive technique employed was aversive taste treatment.
For some oral habits, such as nail-biting elimination, and in some isolated individuals, the short term usage of a slightly aversive-tasting substance may be necessary. However, it is never the first line of defense, but rather the last resort. If a child makes a request for an aversive tasting substance in lieu of more visible reminders, it is only utilized in the presence of a strict and well-moderated program of positive reinforcement with a child who wants to conquer their habit, and with the presence of an adult.
Watson and Allen (1993) confirm the findings of Friman and Hove (1987). The thumb was targeted as a treatment for trichotillomania. They evaluated the relative effectiveness of several specific techniques, comparing standard aversive taste treatments, a physical response disrupting thumb (crib/habit appliance) post, and a response dependent alarm in their research. They concluded that an effective treatment alternative for a benign hair pulling disorder, when it is just a benign habit disorder, is to treat the retained digit sucking behavior. Again, a negative approach, but it still ultimately confirmed the suggested connection. Once again, the existence of a relationship between thumb-sucking and hair pulling was implicated.
In addition, discussion in the literature regarding this topic is offered by Knell and Moore (1988) in their research of a developmentally normal 3 year old’s quest to eradicate hair pulling. Treatment was provided indirectly by addressing the thumb as the main target. They reported their findings on one isolated case stating that chained behaviors of thumb and hair pulling could expediently and successfully be eradicated in a preschooler by once again choosing the finger sucking as the primary behavior to focus on. The parents utilized an aversive approach and the patient continued to demonstrate complete cessation of both habits at their child’s 40 month follow up appointment.
Again, potential concerns are that although the literature reflects that by stopping/eradicating the thumb-sucking behavior, (if postulated as the primary habit), the hair pulling eradication (secondary habit) will follow. When the two habits are concomitant, and they are tested or studied together, it is apparent that there is a propensity to utilize more negatively based techniques of habit elimination in these situations, and publish the results as they occur.
As cited above, only several studies with limited patient populations have been reported on thumb-sucking elimination and its relationship with the cessation of trichotillomania. Unfortunately, the lack of readily available research further indicates that more research is needed in this area, especially in relation to children. On a more positive note, the research presented in this article does highlight the benefit of utilizing positive techniques in lieu of negative ones.
Dr. Nick Moore, IJOM, (2003), in his comprehensive and unique dissertation on the exploration of thumb-sucking elimination techniques, also confirmed the existence of multiple negative techniques being utilized to achieve cessation of oral habits in the past, and their predominance in the research literature to date. He reports that many of these negative approaches continue to be utilized by the medical and dental community.
Moore postulates that until techniques that are more positive are published in the literature, by those who utilize them regularly, a more negative approach may continue on as the a predominant methodology for select clinicians, given that these methodologies have been the most intensively researched, studied, and published to date. Dr. Moore also challenges professionals who consistently and routinely utilize a more positive approach to publish their results for the elimination of oral habits.
Positive Techniques Are Out There
The research and literature on concomitant TTM and digit habits may be scant and buried, however, it does exist. Replication studies may be conducted by orofacial myologists using their expertise. It is time for orofacial myologists to develop case studies and bring their information to a professional, public forum. Single cases may be reported, such as that of Knell and Moore (1988) cited above. As a group, certified orofacial myologists who have similar outcomes in their own practices could contribute to the literature based on the relationship between trich and digit habits by presenting evidence from their own clinical experiences that a positive program may be extremely successful.
Ultimately, this positive approach can be of great assistance to those seeking help and remediation with chained oral habits. Perhaps the presentation of the following four hair pulling cases, will encourage more clinicians practicing in the field of orofacial myology to continue to research this topic, and ultimately promote the publication of additional documented success in this arena.
CONCOMITANT BEHAVIORS: CASE STUDIES
The following four case studies are presented in chronological order of treatment. These case studies indicate that a positive approach is beneficial for both the family and the child, and rewarding for the clinician who contributes to positive outcomes.
Case Study #1: Thumb-sucking Elimination with Concomitant Hair Pulling Behavior Elimination Via a Positive Approach
A seven-year-old female, upon referral from her pediatrician, presents with a history of concurrent daytime and nocturnal thumb-sucking and daytime hair pulling of a severe nature. Her mother also noted some dental concerns with possible suspected anterior protrusion of teeth 8 and 9. Her mother reported that these teeth were appearing to erupt at a slow pace, and noted a space was also present interproximally (possible diastema suspected) on teeth 8 and 9.
The patient was concurrently under the care of a physician and a psychologist for self-esteem issues. Several attempts had been made by the psychologist to try assisting the child in eliminating the hair pulling and substitution strategies such as hair brushing and rewards had been suggested to assist with the trich behavior independently. She had some limited success with these strategies but still struggled. Antidepressant medication had been administered by her medical professionals to assist in the repetitive nature of the hair pulling as well prior to her seeking therapy to eliminate her thumb-sucking habit. The child’s mother reported observing limited success from the anti-depressant medication.
The two habits had become an enormous family concern. The mother had reported that her daughter experienced severe teasing in school, and increasing social isolation, both from the thumb-sucking, and the hair pulling. The social aspect had become so debilitating, according to the mother, that the family was in the process of preparing to move out of state in an effort to remove her child from the negative environment she was constantly being exposed to at school and in the neighborhood.
Her mother’s motivation to seek additional help at this time was an effort to eliminate her thumb-sucking habit, which, according to the mother, was contributing to a portion of the teasing. The parent was not anticipating any significant extinction of the hair pulling, but her psychologist was very was supportive in the mother’s efforts to seek help from an orofacial myologist. Her psychologist did not know if it would help with the hair pulling habit, but encouraged her participation. The psychologist was hopeful there might be a connection between the hair pulling and the digit habit. The psychologist was not experienced in thumb-sucking elimination because of the bite issues the child’s dentist had observed, the referral to an orofacial myologist was determined to be an appropriate adjunct to a team approach. The psychologist and this author spoke several times in throughout the treatment process. It was an excellent working relationship for this author and the family.
One of the goals the family was working towards in regards to the hair was diminishing or eliminating hair pulling (Fig. 1) so that she could ultimately wear her lace head covering for her First Holy Communion, which was coming up in several months. The client was extremely motivated to participate in all aspects of habit elimination, and came to the initial appointment willingly and enthusiastically.
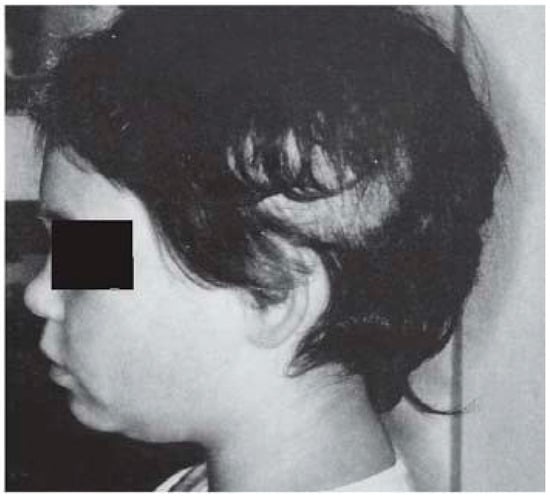
Figure 1.
Case Study 1 Initial Evaluation.
A behavior modification program with a positive approach for thumb-sucking elimination commonly utilized by certified orofacial myologists was initiated. The child eliminated her thumb-sucking behavior within the first day. In addition, by the second day, her mother had reported that the vast majority of the hair pulling had ceased.
She was observed five times within a 60 day period to follow up. (Fig. 2 & Fig. 3) The child and parent reported complete cessation of thumb and hair pulling behaviors and increased self-esteem per her exit survey. Progress was observed once again, approximately six months post-habit. Although no photos were taken during this child’s First Holy Communion, there continued to be evidence of hair length, and her beautiful lace head covering remained on her head the entire ceremony. She received a gift of a brush and comb set with beautiful mirror. This child’s gift to herself was obvious.
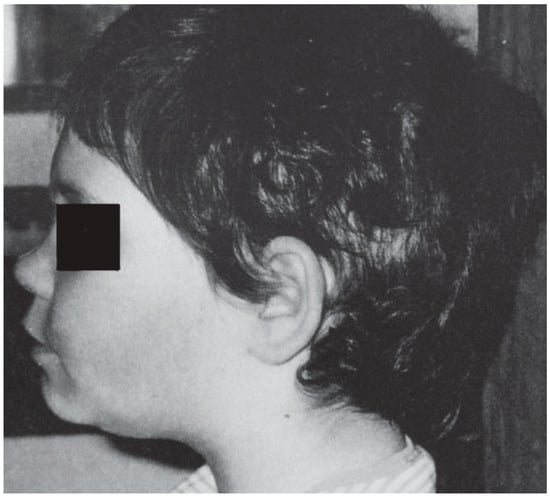
Figure 2.
Case Study 1 30 days after Initial Visit.
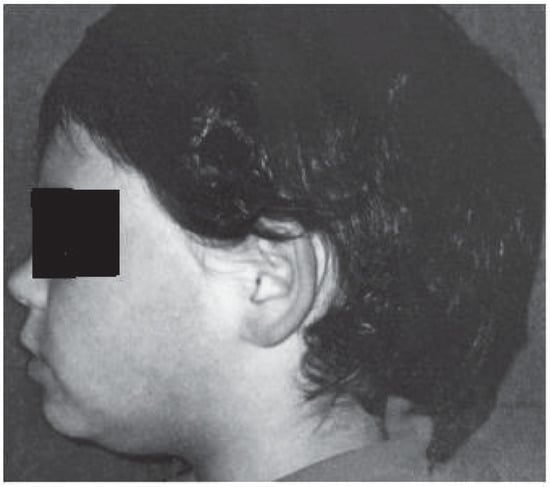
Figure 3.
Case Study 1 60 Days after Initial Eval.
Discussion Case Study 1: Klicpera and Klicpera, (2001), discuss the potential negative effects of victimization or bullying in early childhood. They determined that 10% of all students are affected by bullying and this phenomenon of victimization within peer groups is often characterized by repeated verbal or physical attacks by one or more of their fellow students. Short-term consequences of victimization are reflected in the presence of low self-esteem and a negative mood. Over the long haul, loneliness, helplessness, and sadness ensue as a result of this type of victimization, underscoring a probable connection between long term victimization and the development of depressive disorders. Finding a positive way to help a child who is struggling under such trying circumstance only seems fitting. These children have been exposed to enough of the ‘negative spiral effect’. Positive techniques to help children succeed enable them to feel good about themselves.
It does not appear that the majority of clinicians cited in the studies presented within this review were not supportive nor actively present to care for their patients. However, it is essential to mention the importance and the role this type of consistent intense support plays in an orofacial myology program for habit elimination and it’s propensity to result in overwhelmingly successful outcomes in addressing thumb-sucking elimination. It is the absolute cornerstone of techniques utilized by orofacial myologists.
Case Study #2: Thumb-sucking Elimination with Concomitant Hair Pulling Behavior Elimination Via a Positive Approach
Female, age 3.5 years, presents for habit elimination. Her mother initially phoned to inquire, in particular, about participation in a thumb-sucking elimination program. The mother reports daytime and nocturnal thumb-sucking behavior, with concomitant chained nocturnal hair pulling behavior. Parent was advised that the most positive age for a child to pursue thumb-sucking elimination is beyond age 4. Mother later stated that her pediatrician confirmed the desire to address the habit immediately, due to the trichotillomania, which he felt, might be affecting her socially. Only with the pediatrician’ s recommendation was the client scheduled for an appointment to eliminate the thumb habit. It was the pediatrician’s hope that the eradication or severity of the trich would improve over time with thumb-sucking elimination.
At the initial evaluation the patient presented with extremely scant hair appearance. (Fig. 4A & 4B) She reports a history of significant teasing and social concerns that has significantly influenced her desire to continue to attend pre-school, and her insistence on wearing dresses and extremely feminine appearing clothing exclusively-especially whenever in public.
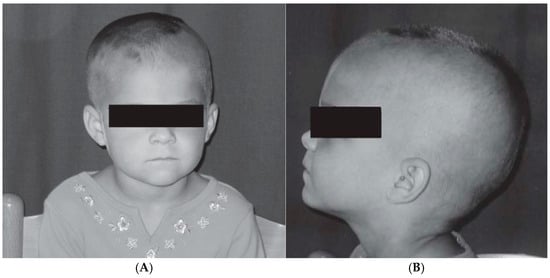
Figure 4.
(A) Case Study 2 Initial Visit. (B) Case Study 2 Initial Visit.
Reports of teasing included statements from peers such as, “Why do you wear a dress when you are a boy”? Her mother shared that she was concerned about others mistaking her daughter’s gender and how it would affect her gender identity in the future. Her daughter felt extremely self-conscious about her appearance, and even at this age, she was able to verbalize some of these feelings to her family. This child was extremely motivated to participate.
A behavior modification approach for thumb-sucking elimination commonly utilized by certified orofacial myologists, was then initiated. The child eliminated the vast majority her thumb-sucking behavior within the first three days. It was reported that she did struggle a little at night the first few nights, but her mother did not feel it was significant enough to warrant concern. In addition, by the third day, her mother had reported that the hair pulling had steadily diminished, keeping pace and closely mirroring the elimination of the thumb-sucking behavior.
She continued to be observed in my office six times within a 120 day period in follow up, with her mother reporting increased self-esteem per her 30 day survey. In addition, it was reported to me that she was seeing her daughter’s sullen initial mood improve a little each day (after the first few days) as she continued with the home reinforcement program. According to her mother’s account at 30 days, “she still wants to suck sometimes, but she doesn’t. She is pulling her hair some at night but has eliminated 98% pulling of the hair”. (Fig. 5A, 5B) She had a brief slip approximately 8 months post-habit program with the thumb. Mom was concerned the hair pulling might follow, and she was brought in immediately for a recall visit. The thumb program was briefly reviewed, contact and follow up was maintained. The concern was successfully addressed.
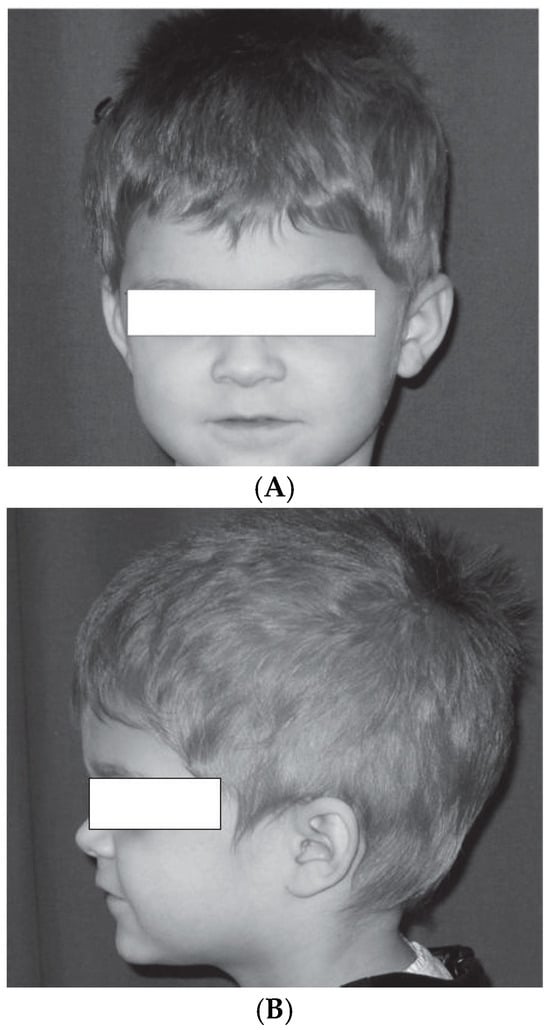
Figure 5.
(A: Above) Case Study 2 2+ months after first visit. (B: Below) Case Study 2 2+ months after first visit.
The client was seen again at approximately 12 months post-thumb habit. (Fig. 6) Her mother later called and wanted ‘her daughter seen’on an additional follow up visit, which was then scheduled. Having received this call, understandably, this clinician was concerned about potential relapse of both detrimental behaviors. However, there was no need for concern. The purpose of the call and request for a follow-up appointment was that the mother wanted this clinician to meet with them both as an opportunity to meet casually and coincidentally observe the client’s current hair.
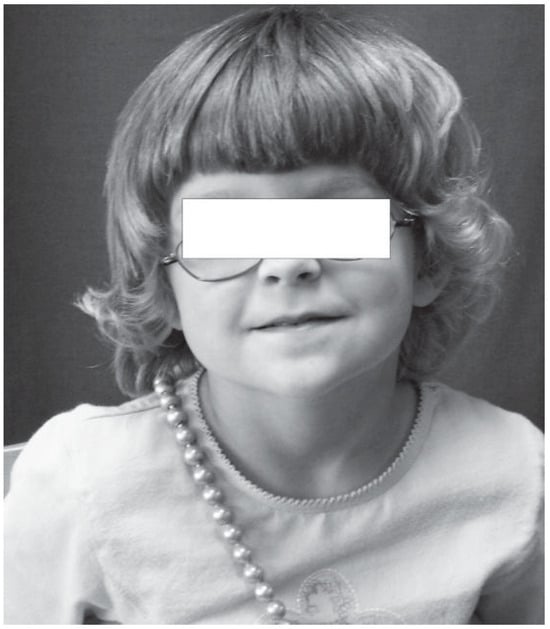
Figure 6.
Case Study 2 1 year + 5 days after Initial Visit.
Discussion Case Study 2: Occasionally, a child will present at an exceptionally early age with a concomitant thumb and hair pulling habit. Friman and Schmitt, (1989), conveyed their pediatric guidelines in regards to thumb-sucking elimination at various ages. It is interesting and reassuring to see that their preferred treatment regimen consisted of charts, incentives, and cues, all considered positive in nature. However, they are consistent in their belief that thumb-sucking elimination treatment initiated prior to age four is rarely necessary except with a few rare exceptions, their rationale being based on ‘risk potential.’
They specifically name hair pulling as an exception to their favored age of four years, citing that if physical or emotional sequelae are of an imminent concern, or a child requests help in quitting, after this age, then treatment may be recommended.
According to Trich.org, it is extremely common for individuals with hair pulling to have mild recurrences throughout life. That is the nature of the disorder. However, a clinician can be encouraged that treatment outcomes, when that treatment is provided in a positive manner, can be beneficial with some little girls of 3.5 years, such as this one who made a life-changing improvement. (It should also be noted in that in all of the photo series included with this article, that the facial expressions captured on the children seem to evolve over time to the degree that even the casual observer can see the change in affect.)
Case Study #3: Thumb-sucking Elimination with Concomitant Hair Pulling Behavior Elimination Via a Positive Approach
Female, age 5, presented with significant daytime and nocturnal thumb-sucking behaviors with severe concurrent daytime and possible nocturnal hair pulling. Client reported having multiple siblings, with absence of a sibling history of thumb-sucking past age 3, pacifier past age 2, or current or previous familial hair pulling behavior. She exhibited sparse hair growth, and it was reported that she wears a pink cap habitually. She refuses to remove her cap at any point during the intake interview.
Referral for thumb-sucking elimination was initiated by her pediatric dentist in the hope of avoiding future bite issues, encouraging a proper growth pattern of the hard palate, slowing down the progression of a more vertically-based palatal growth pattern, and indirectly in the hopes of diminishing the hair pulling behavior.
Mother states one of her major concerns is that her daughter refuses to remove her pink baseball cap because she is so worried about her scalp being observed by others. (Fig. 7) The mother continued that the only opportunity to wash the cap was for her to wait for her daughter to go to sleep, launder it, dry it, and then replace back on her night table by the time she awakened. The client only wore dresses at each appointment, but never pants nor slacks

Figure 7.
Case Study 3 Initial Visit.
The child eliminated her thumb-sucking behavior and the hair pulling within the first day as per family report. She was observed five times within a 60 day (Fig. 8, 9) period to follow up, then again at 6 months post-program initiation, and at one year. The client reported complete remediation of both habits and ‘no slips’. Photos were taken at most follow up visits, (Fig. 10, 11, 12) Note, she is not wearing a cap. However, according to the family she is now substituting the cap with hair ornaments and barrettes. Her mother requested to bring her in every year on her ‘no-thumb anniversary’. Those follow-up appointments have been scheduled annually.

Figure 8.
Case Study 3 30 Days after Initial Visit.

Figure 9.
Case Study 3 40+ Days After Initial Visit.

Figure 10.
Case Study 3 3 Months After Initial Visit.
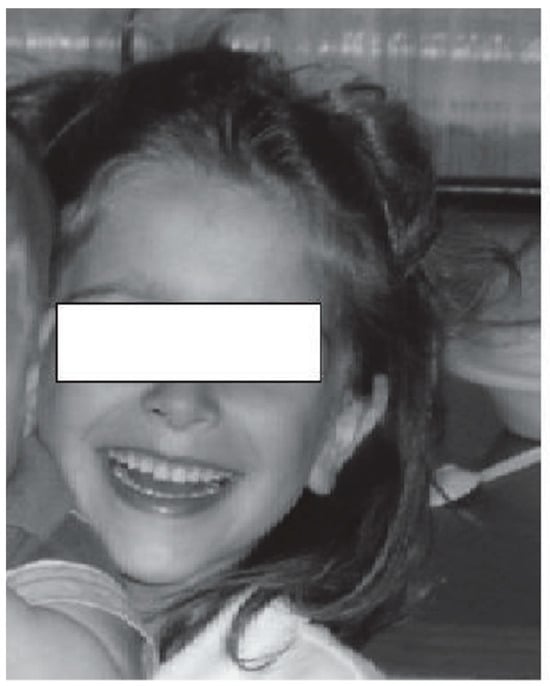
Figure 11.
Case Study 3 15 Months After Initial Visit.
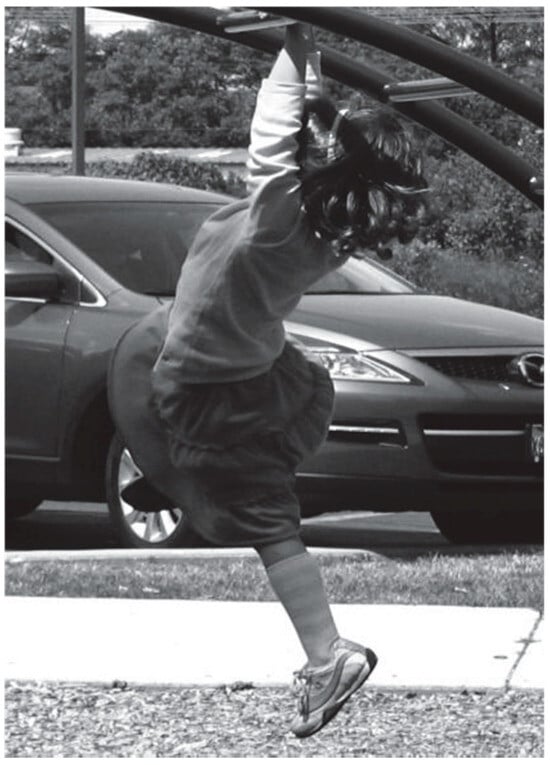
Figure 12.
Case Study 3 16+ Months After Initial Visit.
Discussion Case Study 3: The clinician in the preceding three case studies did not directly treat the hair pulling behavior. Only the thumb-sucking habit was addressed. The client in case study 3 was referred by her pediatric dentist for her digit habit. The hair pulling cessation was an added benefit of treatment.
Case Study #4: Thumb-sucking Elimination with Concurrent Hair Pulling Behavior Elimination Via a Positive Approach
Male, age 10 presented with a moderate to severe history of concomitant daytime and nocturnal thumb-sucking and daytime and sleep inducing hair pulling. The habit had persisted for several years and was well-ingrained. His parents related that they were most concerned with the hair pulling behavior. The child, however, was more motivated by his desire to eradicate the thumb-sucking, and most likely considered any coincidental eradication of the hair pulling a benefit. He presented with an extremely short and ‘socially acceptable’ male-oriented hair cut (‘buzz cut’), in the presence of a possible unilaterally elevated hairline. (Fig. 13, 15) He was referred by his family dentist. The dentist, according to the family, was concerned about the bite, noting the presence of an overjet, inappropriate and highly protrusive rest position of the tongue, and tongue thrust behavior. Teasing had taken place in school, including ridicule and embarrassment in the classroom from multiple peers as the child experienced many episodes of subconscious thumb entry into the oral cavity throughout the day. According to his personal report, he had become anxious about attending school, constantly fearful that the thumb would sneak in at an inopportune time only to be viewed by his classmates giving them more opportunity to taunt him. In addition, it was beginning to effect his schoolwork, as well as his socialization, according to his family.
A positive behavior modification approach for thumb-sucking elimination commonly utilized by certified orofacial myologists was then initiated. Although very motivated to cease sucking, the child struggled to eliminate his thumb-sucking behavior and the hair pulling in the initial portion of the program. This may have been due to sporadic parental compliance with the complete program. Without parental participation in a behavior modification approach to oral habit elimination, one cannot expect ease of cessation or long term success. Parental participation and consistency is essential to success.
The client did achieve complete dual cessation the vast majority of days, with minor slips occurring on a sporadic basis, which were directly related to the inconsistencies present when the full dynamics of the program were not in place. (Fig. 14, 16) He was observed five times within a 60 day period to follow up. At that time, the parents had reported that they had not followed the specific tasks assigned for the home program at his last visit, but despite this, they indicated that the client had not displayed any sucking or pulling behaviors in almost a month. The parents were advised that they needed to continue implementing the follow-up home program. The process of habit reversal can take an extended amount of time. He was to report back weekly on his continued progress. Upon a follow up call two months later, it was reported that the hair pulling, although of a mild nature, and only as he was falling asleep, had returned. No thumb sucking, however, was present.
Figure 13.
Case Study 4 Initial Visit.
Figure 14.
Case Study 4 30 Days After Initial Visit.
Figure 15.
Case Study 4 Initial Visit.

Figure 16.
Case Study 4 30 Days After Initial Visit.
The client was advised to consult with their referral source and return to the orofacial myologist’s office to follow up with his oral habit. The parent declined the suggested follow up visit due to a rigorous work schedule.
Discussion Case Study 4: Based on experience, this author has found that when a parent is challenged in their monitoring and participation in a behavior modification program of this intensity, the result is predictable. The program on some level will fail. Thus, one may conclude that the outcome of hair vs. thumb for this client might be deemed a ‘long term failure with a short term success.’ An invested clinician would not be completely satisfied with the results for this client. However, a clinician in this type of circumstance can only guide. They can never force nor expect every individual client or their family to comply completely. The family, as a unit, must be of the mind-set that they are willing to make the time commitment necessary, and understand that there will be necessary sacrifices if they are to enhance the greatest chance of complete long term success.
Clinicians understand the importance of such consistency. They follow up with the child and family regularly, and provide continued support. It is prudent to never take anyone into a habit elimination program that the clinician does not feel can succeed, unless a pediatrician or dentist consults and requests otherwise. Some orofacial myologists believe that it is ultimately up to the referral source to provide an interested clinician with an indisputable reason why that individual must be given the opportunity to participate in the elimination process and hopefully be motivated further to meet his or her maximum potential to succeed. Could one have predicted that this client would succeed-at eradicating the thumb habit? Yes...he was highly motivated...to cease the THUMB habit. Using that justification, the pre-judgement of an individual possessing adequate motivation towards their primary habit could actually be right on target. In addition, despite a lack of full parental support, the desire to eradicate the thumb was very great on the part of the boy. That in itself was justification enough to put a plan into place. As eluded to earlier, via Friman and Schmitt, (1989) that treatment may be recommended if a child requests help in quitting or if some emotional sequelae or physical concern appears imminent. This child displayed a strong desire to ‘quit’ the thumb, and there was, according to the referral source, the concern of what may be considered ‘physical and emotional sequelae’. Thus, despite the ultimate struggle for full compliance, according to Friman and Schmitt, (1989) this child would have been determined to be a suitable candidate for a habit elimination program.
Under these circumstances, one might conclude the clinician did their job. The clinician was successful with the child regarding the thumb habit which was the target for treatment.
This case study has been included to stress the point that this child had a strong desire to eradicate the thumb habit but a limited desire to eradicate the hair pulling. In fact, the parent was far more concerned in this aspect of hair pulling than the young man. The boy’s indifference towards the hair pulling, either as a result of having little influence his social life or peers, or simply because short hair is acceptable to a boy, and thus, did not motivate him to quit his hair pulling habit.
The fact that the thumb was so significant a social factor for him, was the boy’s main motivation. He had no strong desire to stop hair pulling, and perhaps, absolutely no desire or motivational reason to quit the hair pulling. It is conceivable that he was quite happy with his short hair. The hair pulling significantly lessened despite a lack of desire on his part to work on this hair pulling behavior, as a result of his desire to work on the thumb, and thus is an excellent example of how the following could be postulated. The cessation of his hair pulling was a result of eradicating the thumb habit.
This client did not seek advice with the end goal of eradicating a trichotillomania habit. The client and his family were seeking advice to eliminate a thumb-sucking habit. If the extinction, or in this case the reduction of the secondary habit coincidentally follows, as the research cited in this article has suggested it often does, it may be considered a positive unexpected outcome.
Both the client and the parents were pleased with the outcome for digit habit cessation. They were also pleased with the reduction in the secondary habit of hair pulling as an effect of eradicating the thumb-sucking. Yes, the parent may have preferred to see total cessation of the secondary habit. However, a consistently implemented home monitoring program was not implemented. One cannot expect complete success when incomplete effort is put forth. In this or similar situations, clinicians may feel compelled or obligated to continue to revisit this client. In essence, full eradication of both habits was not achieved.
However, this client was successful with thumb habit cessation, and that is what this particular clinician felt comfortable addressing. Providing treatment only for the trichotillomania without a concomitant digit habit is not something which certified orofacial myologists would be addressing. This particular clinician felt their role was to specifically address an ‘oral habit’, and not the ‘hair pulling’, per se. Eradication of the secondary habit as a result of the thumb habit cessation is a finding in many cases, and often is not the initial aspect that many COMs would primarily address. However, from this certified orofacial myologist’s perspective, the outcome with this client was successful. The oral habit was successfully addressed.
Experienced clinicians understand that if there is partial compliance by the client and/or the parents toward a particular goal, you are likely to end up with a partial result. In this instance, the client outcomes were what reasonable expectations would have dictated.
DISCUSSION
It is interesting to note that in the case studies of the females presented above who displayed concomitant hair-pulling and thumb-sucking, motivation appeared to be driven by their physical appearance, despite all three girls being younger in age than the boy highlighted above. Children as young as 4 months show similarity with adults in the ‘aesthetic perception of attractiveness’. Infant facial esthetic preference was not based on the vertical symmetry of the face.
Facial symmetry is often postulated to be a standard of physical facial attractiveness. This was confirmed by Samuels, Butterworth, Roberts, Graupner, and Hole (1994). In this study, it was determined that babies chose to glance longer at attractive/normal faces rather than unattractive faces. No matter what age the infant was, this held true.
This preference for attractiveness by young infants was confirmed yet again, as well, by Ramsey, Langlois, Hoss, Rubensten, and Griffin (2004). In this research addressing the human stereotyping of attractiveness, Ramsey et al investigated whether or not 6-month-old infants could categorize female faces into two categories - attractive or unattractive. Results confirmed that the 6-month-olds could and did indeed categorize feminine faces into the categories of attractive versus unattractive female faces.
Ruiz, Conde, and Torres, (2005), confirmed this finding with older children. They determined for a group of subjects age 8, 12, and 13, that physical attractiveness appeared a desirable characteristic for each age group. The study encompassed older children, but considering the results by Ruiz et al., (2005) and Ramsey et al., (2004), preference for attractiveness actually begins much younger in life, and well within the age range for the case studies on the three girls presented previously.
Shame and embarrassment often co-exist with hair pulling habits. This is supported by Bohne (2005), in their review of the literature. In the three female trich-thumb-sucking case studies above, it appeared that the girls experienced shame and embarrassment as a result of their habit, and their desire to cover their scalps suggested a deeper concern on how their appearance might be viewed publicly if their habit was ‘out there for all to see.’
According to Bohne, Keuthen, and Wilhelm, (2005), sufferers of hair pulling often fail to want to admit the self-inflicted nature of their physical damage. One may postulate their shame might be appearance-driven in nature. How their appearance was perceived by others seemed socially significant to them. Each expressed this concern, embarrassment, or shame in their own unique way i.e., two of the girls habitually insisted on altering their clothing or apparel in an effort to camouflage their habit behavior to the world, and the third girl was motivated by the hope of being able to alter her hair appearance so that she could wear her hair covering in the presence of a full head of hair in the future when others would be looking on within a rather large and socially significant group dynamic.
In essence, all three girls appeared motivated to seek help with the end goal of hair pulling as a major factor, rather than the thumb being the primary motivator, despite their age. However, in the case of the boy, the opposite held true. Most of the ‘teasing’ the boy experienced occurred because of the thumb habit and peer pressure. That is what motivated him to want to participate in the cessation program, and that was his driving force to succeed. (He ultimately did succeed at achieving his initial personal goal for eradicating the thumb habit). One might postulate that society views attractive hair in women as an asset to be cherished, and these girls, despite their age, may have somehow identified with the inherent or perceived value or benefit. Mayo Clinic.com confirms that ‘Hair is often associated with beauty and vitality. That’s why trichotillomania — also called hair-pulling disorder, trich, or pulling — can be so emotionally painful for people with the condition.’
On this topic of attractiveness, Rieger, Gygaz, Linsenmeier, Siler-Knogl, Moskowitz, and Bailey, (2009), explored a similar issue of femininity in girls. Results suggested that both young boys and girls equate attractiveness with femininity. The older a girl becomes, the more childhood femininity may be viewed as related to attractiveness by both boys and girls. The older the child becomes, the relationship between female attractiveness and femininity appears to strengthen. It appears that both sex and maturity of the individual may play a role on the impact of femininity on female attractiveness. In essence, the older a girl is, the more apt she is to equate femininity with attractiveness. The boys, however, did not equate masculinity as strongly with attractiveness as they aged. Perhaps the girls in these case studies innately understood that a boy with short hair is socially acceptable...but not a girl’s.
Abelson and Paluszny, (1978) compared childrens’ ability to determine gender identity using the Michigan Gender Identity Test (MGIT). Included in their study were 36 normal children and 52 children experiencing developmental or emotional challenges. Subjects in both groups were shown various photos of children, including themselves, wearing gender specific clothing and depicting gender specific hairstyles. The goal was to determine if the challenged subjects could tell the difference between male and female in a manner similar to that of the normal children based on stereotypical appearance of children depicted.
A correlation was found between mental age and ability to recognize a specific gender based on this test. In addition to their results, the importance to this author is that Abelson and Paluszny (1978) felt that collecting data on gender identity using hairstyle and clothing for the basis of their research indicates that hairstyle and clothing are critical elements for gender identification.
Zosuls, Ruble, Tamis-Lemonda, Shrout, Bornstein, and Greulich, (2009), explored the relation between gender labeling and gender-type play was examined in 82 children, prior to age five years. Researchers conducted parental telephone interviews regarding their child’s language at 9-21 months, and play in these children via videotape and parental home visits at 17 and 21 months. They concluded that the average age children underwent a ‘developmental transition’ regarding gender labeling at 19 months. In addition, girls were shown to begin gender labeling significantly earlier than boys.
CONCLUSIONS
In conclusion, more ongoing research needs to be conducted in the area of concomitant habits. Future exploration in large scale studies might include: how often do concomitant habit eradication occur; does peer pressure play a significant role in outcome success; how are family dynamics related in dual cessation; or does age play a factor in success rates of concomitant oral habits. COM’s are capable of being an integral part of this equation. They have the access to the clients, the knowledge base, the ability to implement a successful strategy on primary oral habits, the passion for the task, and the desire to share their knowledge. COMs have the true obligation to make this knowledge known.
(Postscript by the author: I truly believe it is history in the making. And, I believe this article in itself has made a little piece of that history happen today. I may also add: Thank goodness, we have this forum in which to share it!)
REFERENCES
- Abelson, G., and M. Paluszny. 1978. Gender identity in a group of retarded children. Journal of Autism and Child Schizophrenia 8: 403–411. [Google Scholar] [CrossRef]
- Abelson, J.F. 2005. Sequence Variants in SLITRK1 Are Associated with Tourette’s Syndrome. Science 310: 317–20. [Google Scholar] [CrossRef]
- Altman, K., C. Grahs, and P. Friman. 1982. Treatment of unobserved trichotillomania by attention-reflection and punishment of an apparent covarian. Journal of Behavioral Therapy and Experimental Psychiatry 13: 337–4. [Google Scholar] [CrossRef] [PubMed]
- Bohne, A., N. Keuthen, and S. Wilhelm. 2005. Pathological hairpullling, skin picking, and nailbiting. Annals of Clinical Psychiatry 17: 227–32. [Google Scholar] [CrossRef] [PubMed]
- Bruce, T.O., L.W. Barwick, and H.H. Wright. 2005. Diagnosis and management of trichotillomania in children and adolescents. Paediatric Drugs 7: 365–76. [Google Scholar] [CrossRef]
- Christenson, G., and S. S.J. Crow. 1996. The characterization and treatment of trichotillomania. Journal of Clinical Psychiatry 57: 42–49. [Google Scholar] [PubMed]
- Crow, S.J. 1996. The characterization and treatment of trichotillomania. Journal of Clinical Psychiatry 57: 42–49. [Google Scholar]
- Coulson, S. 2009. IAOM Clinical Convention, Clinician’s Roundtable, San Diego, Calif. USA.
- Enos, S., and T. Plante. 2001. Trichotillomania. An overview and guide to understanding. Journal of Psychosocial Nursing and Mental Health Services 39: 8–10. [Google Scholar] [CrossRef]
- Friman, P.C., and G. Hove. 1987. Apparent covariation between child habit disorders: effects of successful treatment for thumb sucking on untargeted chronic hair-pulling. Journal of Applied Behavior Analysis 20: 421–5. [Google Scholar] [CrossRef]
- Friman, P.C., and B.D. Schmitt. 1989. Thumb sucking: pediatricians’ guidelines. Clinical Pediatrics 28: 438–40. [Google Scholar] [CrossRef]
- Grant, J.E., and B.L. Odlaug. 2009. Update on pathological skin picking. Current Psychiatry Reports 11: 283–8. [Google Scholar] [CrossRef] [PubMed]
- Green, S.E. 1998. That little thumb can do an awful lot of damage. In Pamphlet. Chicago. Il: Independent. [Google Scholar]
- Klicpera, B.G., and C. Klicpera. 2001. Victimization by peers as a developmental risk factor. Zeitschrift für Kinder und Jugendpsychiatrie und Psychotherapie 29: 99–111. [Google Scholar] [PubMed]
- Knell, S.M., and D.J. Moore. 1988. Childhood trichotillomania treated indirectly by punishing thumb-sucking. Journal of Behavioral Therapy and Experimental Psychiatry 19: 305–10. [Google Scholar] [CrossRef] [PubMed]
- Mansueto, C., P. Ninan, B. Rothbaum, E. Reeve, and M. Lu. 2002. Trichotillomania and its Treatment in Children and Adolescents: Pulling Hair : A Guide for Clinicians/A publication of the Scientific Advisory Board of the Trichotillomania Learning Center. Retrieved Oct. 29, 2009 from trich.org. Jan. website: www.trich.org/dnld/Child_Clinicians_Guide_v08.pdf.
- Staff, Mayo Clinic. 2009. Trichotillomania (hair-pulling disorder): definition, symptoms, causes, risk factors, and complications. Retrieved Oct. 26, 2009 from MayoClinic.com. website: http://www.mayoclinic.com/health/trichotillomania/DS00895 http://www.mayoclinic.com/health/trichotillomania/DS00895/DSECTION=symptoms http://www.mayoclinic.com/health/trichotillomania/DS00895/DSECTION=causes http://www.mayoclinic.com/health/trichotillomania/DS00895/DSECTION=risk%2Dfactors http://www.mayoclinic.com/health/trichotillomania/DS00895/DSECTION=complications.
- Mspennylane, Lizzie, Daniela, Delilah, C.C. Lemons, Teenage Trichster. 2009. What it feels like. [Web log messages].Retrieved Oct. 30 from. October 30. website blog: www.trichotillomaniaBlog.com/PullingOutHair/.
- Meunier, S.A., D.F. Tolin, and M. Franklin. 2009. Affective and sensory correlates of hair pulling in pediatric trichotillomania. Behavior Modification 33: 396–407. [Google Scholar] [CrossRef]
- Moore, N.L. 2002. Suffer the little children: fixed intraoral habit appliances for treating childhood thumbsucking habits: a critical review of the literature. International Journal of Orofacial Myology 28: 6–38. [Google Scholar] [CrossRef]
- Odlaug, B.L., and J.E. Grant. 1994. Trichotillomania and pathological skin picking: clinical comparison with an examination of comorbidity. Journal of Abnormal Child Psychology 22: 79–97. [Google Scholar]
- Ramsey, J.L., J.H. Langlois, R.A. Hoss, A.J. Rubenstein, and A.M. Griffin. 2004. Origins of a stereoype: categorization of facial attractiveness by 6-month old infants. Developmental Science 7: 201–211. [Google Scholar]
- Rieger G., Gygaz, L., J.A. Linsenmeier, A. Siler-Knogl, D.A Moskowitz, and J.M. Bailey. 2009. Sex typicality and attractiveness in childhood and adulthood: assessing their relationships from videos. Archives of Sexual Behaviour, Epub ahead of print. Northwestern University. [Google Scholar]
- Ruiz, C., E. Conde, and E. Torres. 2005. Importance of facial physical attractiveness of audiovisual model. Developmental Science 101: 229–243. [Google Scholar]
- Samuels, C.A., G. Butterworth, T. Roberts, L. Graupner, and G. Hole. 1994. Facial aesthetics: babies prefer attractiveness to symmetry. Perception 23: 823–31. [Google Scholar] [CrossRef]
- Shusterman, A., L. Feld, L. Baer, and N. Keuthen. 2009. Affective regulation in trichotillomania:Evidence from a large-scale internet survey. Behaviour Research and Therapy 47: 637–44. [Google Scholar] [CrossRef]
- Stillman, A.A., Z. Krsnik, J. Sun, M.R. Rasin, M.W. State, N. Sestan, and A. Louvi. 2009. Developmentally regulated and evolutionarily conserved expression of SLITRK1 in brain circuits implicated in Tourette syndrome. Journal of Comparative Neurology 1: 21–37. [Google Scholar] [CrossRef] [PubMed]
- Trich.org. 2009. Trichotillomania and its Treatment in Children and Adolescents. [Google Scholar]
- Hair Pulling: A Guide for Clinicians/A publication of the Scientific Advisory Board of the Trichotillomania Learning Center.
- Troster, H. 1994. Prevalence and functions of stereotyped behaviors in nonhandicapped children in residential care. Journal of Abnormal Child Psychology 22: 79–97. [Google Scholar] [CrossRef]
- Van Norman, R.A. 1997. Digit-sucking: a review of the literature, clinical observations and treatment recommendations. International Journal of Orofacial Myology 12: 14–34. [Google Scholar] [CrossRef]
- Van Norman, R.A. 2001. Thumb or finger sucking: growth, development and help with a positive approach. Pamphlet, NE: Independent. [Google Scholar]
- Watson, T.S., J.H. Flegle, and K.D. Allen. 1992. A thermoplastic thumb post for the treatment of thumb-sucking. American Journal of Occupational Therapy 46: 552–4. [Google Scholar]
- Watson, T.S., and K.D. Allen. 1993. Elimination of thumb-sucking as a treatment for severe trichotillomania. Journal of the American Academy of Child and Adolescent Psychiatry 32: 830–34. [Google Scholar] [CrossRef]
- Zosuls, K.M., D.N. Ruble, C.S. Tamis-Lemonda, P.E. Shrout, M.H. Bornstein, and F.K. Greulich. 2009. The acquisition of gender labels in infancy: implications for gender-typed play. Developmental Psychology 45: 688–701. [Google Scholar] [CrossRef]
© 2009 by the author. 2009 Shari Green