Repeated Tongue and Hand Strength Measurements in Normal Adults and Individuals with Parkinson’s Disease

Abstract
:INTRODUCTION
METHOD
Participants
IOPI Apparatus
Procedure
RESULTS
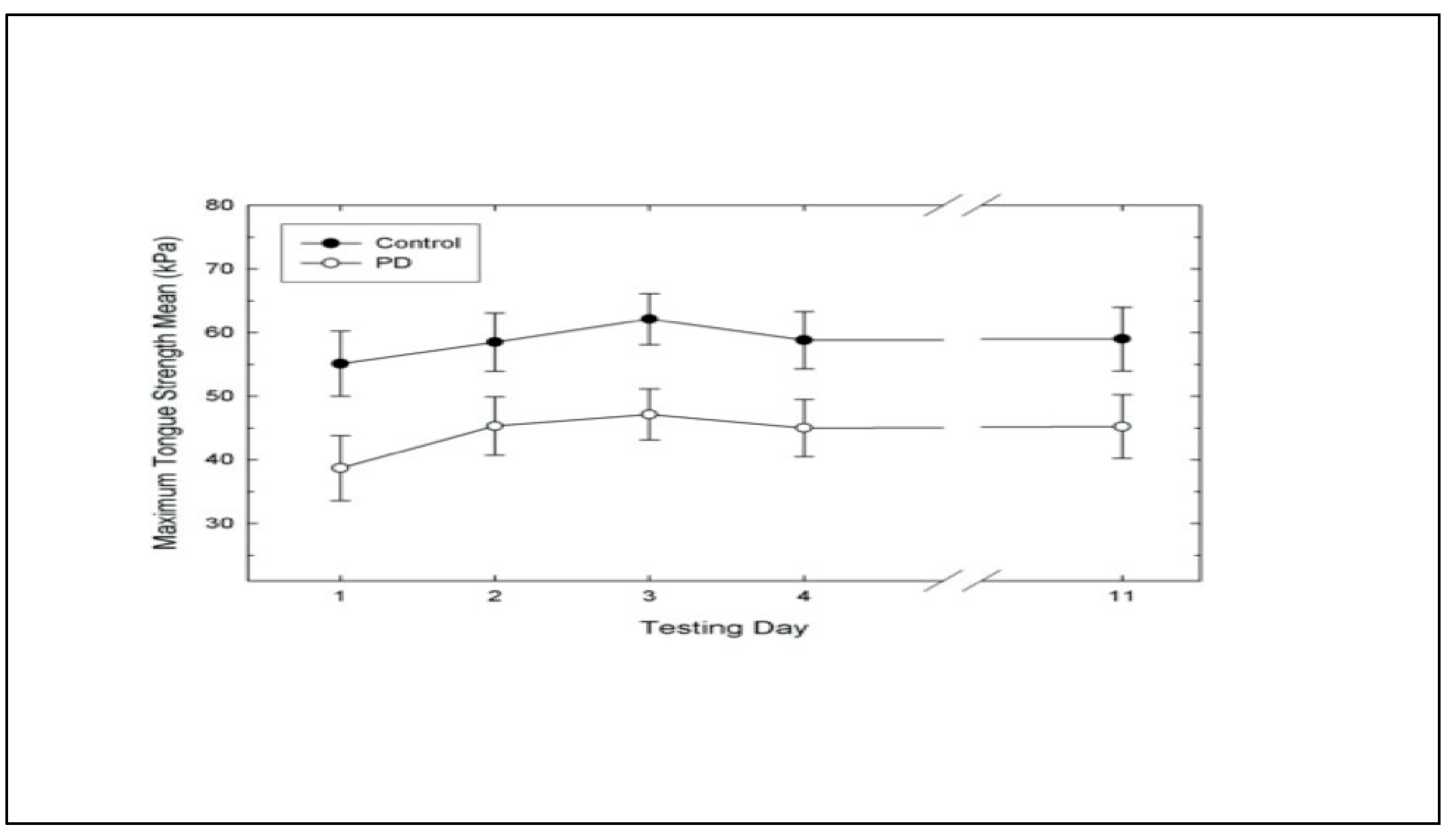
Tongue Strength Measurement
Hand Strength Measurement
Correlation Analyses of Hand Size and Hand Strength Measurement
DISCUSSION

{kind=link}
| Tongue | Day 1 | Day 2 | Day 3 | Day 4 | Day 5 | M | SD |
| PD Group | |||||||
| M | 38.7 | 45.3 | 47.1 | 45 | 45.2 | 44.26 | 13.27 |
| SD | 13.15 | 13.55 | 11.42 | 12.89 | 16.12 | ||
| Control Group | |||||||
| M | 55.1 | 58.5 | 62.1 | 58.8 | 59 | 58.7 | 15.26 |
| SD | 18.86 | 14.65 | 13.62 | 15.59 | 15.57 | ||
| Hand | Day 1 | Day 2 | Day 3 | Day 4 | Day 5 | M | SD |
| PD Group | |||||||
| M | 105.9 | 106.1 | 110.5 | 109.2 | 111.7 | 108.68 | 33.01 |
| SD | 32.93 | 28.93 | 38.55 | 31.62 | 38.67 | ||
| Control | |||||||
| Group | |||||||
| M | 133.2 | 139.3 | 136.9 | 134.2 | 137.5 | 136.34 | 22.65 |
| SD | 25.62 | 25.27 | 24.03 | 23.71 | 18.09 |
| Variable Tongue | F | df | p | ES |
|---|---|---|---|---|
| Group by Day | .21 | 4, 72 | .9312 | .1476 |
| Group | 5.64 | 1, 18 | .0288 | .2225 |
| Day | 4.09 | 4, 72 | .0048 | .1825 |
| Hand | ||||
| Group by Day | .4 | 4, 72 | .8053 | .0095 |
| Group | 5.15 | 1, 18 | .0358 | .2387 |
| Day | .5 | 4, 72 | .7363 | .1833 |
CONCLUSIONS
Future Research
References
- Baum, B. J., and L. Bodner. 1983. Aging and oral motor function; evidence for altered performance among older persons. Journal of Dental Restoration 62: 2–6. [Google Scholar] [CrossRef] [PubMed]
- Butler, M. 1997. Hand strength: A comparative study. New Zealand Journal of Occupational Therapy 48, 1: 5–12. [Google Scholar]
- Calne, D. B., D. G. Shaw, A. S. D. Spiers, and G. M. Stern. 1970. Swallowing in Parkinsonism. British Journal of Radiology 43: 456–457. [Google Scholar] [CrossRef] [PubMed]
- Capriotti, V. P., W. M. Sherman, and D. R. Lamb. 1999. Reliability of power output during intermittent high-intensity cycling. Medical Science of Sports Exercise 31, 6: 913–915. [Google Scholar] [CrossRef]
- Clark, H. M., P.A. Henson, W. D. Barber, J. A. G. Stierwalt, and M. Sherrill. 2003. Relationships among subjective and objective measures of tongue strength and oral phase swallowing impairment. American Journal of Speech-Language Pathology 12: 40–50. [Google Scholar] [CrossRef] [PubMed]
- Crosby, C. A., M. A. Wehbe, and B. Mawr. 1994. Hand strength: Normative values. Journal of Hand Surgery 19A: 665–670. [Google Scholar] [CrossRef]
- Crow, H. C., and J. A. Ship. 1996. Tongue strength and endurance in different aged individuals. Journal of Gerontology: Medical Sciences 51, 5: M247–M250. [Google Scholar] [CrossRef]
- DePaul, R., and B. R. Brooks. 1993. Multiple orofacial indices in amyotrophic lateral sclerosis. Journal of Speech and Hearing Research 36: 1158–1167. [Google Scholar] [CrossRef]
- Desrosiers, J., G. Bravo, R. Hebert, and E. Dutil. 1995. Normative data for hand strength of elderly men and women. The American Journal of Occupational Therapy 49, 7: 637–644. [Google Scholar] [CrossRef]
- Dworkin, J. P. 1980. Tongue force in normals and in dysarthric patients with amyotrophic lateral sclerosis. Journal of Speech and Hearing Research 23: 828–837. [Google Scholar] [CrossRef]
- Dworkin, J. P. 1991. Edited by D. K. Marshall. Motor Speech Disorders: A treatment guide. St. Louis: Mosby-Year Book, Inc.: 220. [Google Scholar]
- Everett, P. W., and F. D. Sills. 1952. Relationship of grip strength to stature, somato-type components and anthropometric measurements of the hand. Research Quarterly 23: 1610166. [Google Scholar]
- Fiebert, I. M., K. E. Roach, T. Armstrong, D. W. Mandel, and M. Donohue. 1995. Dynamometric hand strength assessment of subjects sixty years and older. Physical & Occupational Therapy in Geriatrics 13, 4: 27–40. [Google Scholar]
- Folstein, M., S. Folstein, and P. McHugh. 1975. Mini-mental state: a practical method for grading the cognitive state of patients for the clinician. Journal of Psychiatric Research 12: 189–198. [Google Scholar] [CrossRef] [PubMed]
- Gentil, M., S. Perrin, C. Tournier, and P. Pollak. 1999. Lip, tongue, and forefinger force control in Parkinson's disease. Clinical Linguistics and Phonetics 13, 1: 45–54. [Google Scholar]
- Goldman, R., and M. Fristoe. 2000. Goldman Fristoe-2 Test of Articulation. In Circle pines. Minnesota: American Guidance Service, Inc. [Google Scholar]
- Goodglass, H., and E. Kaplan. 1972. The assessment of aphasia and related disorders. Philadelphia: Lea & Febriger. [Google Scholar]
- Hamilton, A., R. Balnave, and R. Adams. 1994. Grip strength testing reliability. Journal of Hand Therapy 7: 163–170. [Google Scholar] [CrossRef]
- Hanten, W. P., W. Chen, A. A. Austin, R. E. Brooks, H. Carter, C. A. Law, M. K. Morgan, D. J. Sanders, C. A. Swan, and A. L. Vanderslice. 1999. Maximum hand strength in normal subjects from 20 to 64 years of age. Journal of the American Society of Hand Therapists 12, 3: 193–200. [Google Scholar] [CrossRef]
- Horowitz, B., R. Tollin, and G. Cassidy. 1997. Hand strength: Collection of Normative data with community dwelling elders. Physical and Occupational Therapy in Geriatrics 15, 1: 53–64. [Google Scholar]
- Innes, E. 1999. Hand literature. Australian Occupational Therapy Journal 46: 120–140. [Google Scholar] [CrossRef]
- Kellor, M., J. Frost, N. Silverberg, I. Iversen, and R. Cummings. 1971. Hand strength and dexterity: Norms for clinical use. American Journal of Occupational Therapy 25: 77–83. [Google Scholar]
- Langmore, S. E., and M. E. Lehman. 1994. Physiologic deficits in the orofacial system underlying dysarthria in amyotrophic lateral sclerosis. Journal of Speech and Hearing Research 37: 28–37. [Google Scholar] [CrossRef]
- Logemann, J. A. 1998. Evaluation and treatment of swallowing disorders, 2nd Ed. ed. Austin, Texas: Pro-Ed, Inc., pp. 334–336. [Google Scholar]
- Martin, J. C., D. Diedrich, and E. F. Coyle. 2000. Time course of learning to produce maximum cycling power. International Journal of Sports Medicine 21, 7: 485–487. [Google Scholar] [CrossRef]
- Mathiowetz, V., K. Weber, G. Volland, and N. Kashman. 1984. Reliability and validity of hand strength and pinch strength evaluations. The Journal of Hand Surgery 9A: 222–226. [Google Scholar] [CrossRef]
- Marieb, E. N. 1992. The appendicular skeleton. In Human anatomy laboratory manual. Redwood City, California: The Benjamin/Cummings Publishing Company, Inc. [Google Scholar]
- Metter, E. J., and W. R. Hanson. 1986. Clinical and acoustic variability in hypokinetic dysarthria. Journal of Communication Disorders 19: 347–366. [Google Scholar] [CrossRef] [PubMed]
- Morrison, E. B., S. Rigrodsky, and E. D. Mysak. 1970. Parkinson’s disease: Speech disorder and released infantile oroneuromotor activity. Journal of Speech and Hearing Research 13: 655–666. [Google Scholar] [CrossRef]
- Robin, D. A., A. Goel, L. B. Somodi, and E. S. Luschei. 1992. Tongue strength and endurance: Relation to highly skilled movements. Journal of Speech and Hearing Research 35: 1239–1245. [Google Scholar] [CrossRef] [PubMed]
- Robin, D. A., L. B. Somodi, and E. S. Luschei. 1991. Edited by C. A. Moore, K. M. Yorkston and D. R. Beukelman. Measurement of strength and endurance in normal and articulation disordered subjects. In Dysarthria and apraxia of speech: Perspectives on management. Baltimore: Paul H. Brookes, pp. 173–184. [Google Scholar]
- Robbins, J., J. W. Hamilton, G. L. Lof, and G. B. Kempster. 1992. Oropharyngeal swallowing in normal adults of different ages. Gastroenterology 103: 823–829. [Google Scholar] [CrossRef]
- Robbins, J., R. Levine, J. Wood, E. B. Roecker, and E. Luschei. 1995. Age effects on lingual pressure generation as a risk factor for dysphagia. Journal of Gerontology: Medical Sciences 50A: M257–M262. [Google Scholar] [CrossRef]
- Schmidt, R., and J. Toews. 1970. Grip strength as measured by the Jamar Dynamometer. Archives of Physical Medicine and Rehabilitation 51: 321–327. [Google Scholar]
- Shiffman, L. M. 1992. Effects of aging on adult hand function. The American Journal of Occupational Therapy 46, 9: 785–792. [Google Scholar] [CrossRef]
- St. Louis, K. O, and D. M. Ruscello. 1987. Oral speech mechanism screening examination-revised. Austin, Texas: Pro-Ed. [Google Scholar]
- Solomon, N. P., D. A. Robin, D. M. Lorell, R. L. Rodnitzky, and E. S. Luschei. 1994. Edited by J. A. Till, K. M. Yorkston and D. R. Beukelman. Tongue function testing in Parkinson's Disease. In Motor speech disorders. Baltimore: Paul H. Brookes Publishing Co, pp. 147–160. [Google Scholar]
- Solomon, N. P., D. M. Lorell, D. A. Robin, R. L. Rodnitzky, and E. S. Luschei. 1995. Tongue strength and endurance in mild to moderate Parkinson's disease. Journal of Medical Speech-Language Pathology 3: 15–26. [Google Scholar]
- Solomon, N. P., D. A. Robin, and E. S. Luschei. 2000. Strength, endurance, and stability of the tongue and hand in Parkinson's Disease. Journal of Speech, Language, and Hearing Research 43, 1: 256–267. [Google Scholar] [CrossRef]
- Solomon, N. P., K. D. R. Drager, and E. S. Luschei. 2000. Sustaining a Constant Effort by the Tongue and Hand: Effects of Acute Fatigue. Journal of Speech, Language and Hearing Research 45: 613–624. [Google Scholar] [CrossRef] [PubMed]
- Solomon, N. P., and B. Munson. 2004. The effect of jaw position on measures of tongue strength and endurance. Journal of Speech, Language, and Hearing Research 47: 584–594. [Google Scholar] [CrossRef] [PubMed]
- Sonies, B. C., M. Stone, and T. Shawker. 1984. Speech and swallowing in the elderly. Gerontology 3: 115–123. [Google Scholar] [CrossRef] [PubMed]
- Stierwalt, J. A. G., D. A. Robin, N. P. Solomon, A. L. Weiss, and J. E. Max. 1995. Edited by D. A. Robin, K. M. Yorkston and D. R. Beukelman. Tongue strength and endurance: Relation to the speaking ability of children and adolescents following traumatic grain injury. In Disorders of motor speech: Recent advances in assessment, treatment, and clinical characterization. Baltimore: Paul H. Brookes, pp. 243–258. [Google Scholar]
- Thompson, E. C., B. E. Murdoch, and P. D. Stokes. 1995. Tongue function in subjects with upper motor neuron type dysarthria following cerebrovascular accident. Journal of Medical Speech-Language Pathology 3: 27–40. [Google Scholar]
- Tonkovich, J. D., T. J. Latham, and M. W. Rambow. 1982. Dysarthria rehabilitation. Austin, Texas: Pro Ed. [Google Scholar]
- Tracy, J. F., J. A. Logemann, P. J. Kahrilas, P. Jacob, M. Kobara, and C. Krugler. 1989. Preliminary observations on the effects of age on oropharyngeal deglutition. Dysphagia 4: 90–94. [Google Scholar] [CrossRef]
- Weathers, M. 2000. Oral motor abilities in children performing a novel task. Unpublished doctoral dissertation, University of South Carolina, Columbia. [Google Scholar]
© 2008 by the authors. 2008 Carol O’Day, Elaine Frank, Allen Montgomery, Michele Nichols, Hiram McDade
Share and Cite
O'Day, C.; Frank, E.; Montgomery, A.; Nichols, M.; McDade, H. Repeated Tongue and Hand Strength Measurements in Normal Adults and Individuals with Parkinson’s Disease. Int. J. Orofac. Myol. Myofunct. Ther. 2005, 31, 15-25. https://doi.org/10.52010/ijom.2005.31.1.2
O'Day C, Frank E, Montgomery A, Nichols M, McDade H. Repeated Tongue and Hand Strength Measurements in Normal Adults and Individuals with Parkinson’s Disease. International Journal of Orofacial Myology and Myofunctional Therapy. 2005; 31(1):15-25. https://doi.org/10.52010/ijom.2005.31.1.2
Chicago/Turabian StyleO'Day, Carol, Elaine Frank, Allen Montgomery, Michele Nichols, and Hiram McDade. 2005. "Repeated Tongue and Hand Strength Measurements in Normal Adults and Individuals with Parkinson’s Disease" International Journal of Orofacial Myology and Myofunctional Therapy 31, no. 1: 15-25. https://doi.org/10.52010/ijom.2005.31.1.2
APA StyleO'Day, C., Frank, E., Montgomery, A., Nichols, M., & McDade, H. (2005). Repeated Tongue and Hand Strength Measurements in Normal Adults and Individuals with Parkinson’s Disease. International Journal of Orofacial Myology and Myofunctional Therapy, 31(1), 15-25. https://doi.org/10.52010/ijom.2005.31.1.2