INTRODUCTION
Since the moment of birth nasal respiration is an elementary vital situation for human beings. The alteration of respiratory standards and the acquisition of vicarious mouth breathing is a functional adaptation that results in modifications in not only the organs and apparatus directly involved but also in corporeal dynamics as a whole.
Vicarious mouth breathing, as an adaptive function of the Stomatognathic System brings about structural alterations that allow its installation and functionality. These alterations are accompanied by a myofunctional imbalance that may cause changes in stomatognathic functions and in the corporeal axis.
Angle (
1907) studied mouth breathing and made the following remarks:
“Mouth breathing is, of the several causes of malocclusion, the strongest, the most constant and the one that has the most varied results … causing asymmetric development of muscles as well as of the bones of the nose, and of the upper and lower jaws and also a disorganization of the functions of the lips, cheeks and tongue … The consequences of mouth breathing are always reflected on the face. The nose is small, short and has straight wings; the cheeks are pale and low; the mouth is constantly open; the upper lip is short and the jaw, placed backwards is underdeveloped and its length is shorter than the average, probably because of muscular unbalanced pressures.”
Having a better understanding of corporeal development (Beziers 1994; Rolf 1990; Rocabado 1979; Akerman 1997) it is possible to compare the probable consequences determined by improper respiration. This knowledge creates the possibility of developing preventive treatments aimed at a better quality of life and, as a result, more complete health.
The objective of this paper is to analyze, by means of pictures taken from the frontal, dorsal and sagittal planes, the relationship between mouth breathing and postural alterations of children aged 5 to 10 and to compare the results with those of children of the same age that have nasal respiration.
REVIEW OF RESEARCH
Nasal respiration is the physiological respiration of human beings. Besides the functional and anatomic integrity of the respiratory tract, nasal respiration requires that no obstruction be present which prevents the passage of air. The presence of any kind of obstruction brings forth the conditions necessary for mouth breathing.
The characterization of a syndrome involving signs and symptoms resulting from mouth breathing is based upon a series of research studies performed mainly by orthodontists and otorhinolaryngologysts. They analyzed alterations of the teeth and of the upper and lower jaws, craniofacial growth and development and the consequences caused by the hypertrophy of palatine tonsils, and pharyngeal tonsils, hypertrophy of turbinated bones, rhinitis or by the habit of breathing through the mouth.
According to
Kimmelman (
1989) nasal resistance is a main factor for physiological respiration because the feeling of freedom created by nasal respiration, paradoxically only takes place when there is some resistance. On the other hand nasal obstruction is quite uncomfortable. Because of the activity of the nasal valve, the resistance to the air may change, creating the sensation that the person is breathing normally. However, if the resistance is too strong or too weak, a sensation of nasal obstruction is created. In persons suffering from mouth breathing, nasal resistance diminishes, which is something quite uncomfortable for most people.
During our life, corporeal posture keeps straightening while the respiratory systems, sensory, dental etc., foster the anatomic adaptation of the body in relation to the neck. The trunk and the neck muscles have a significant role in the equilibrium of the head, if there is any interference in this equilibrium; the posture of the head is affected (
Rolf, 1990).
In medical literature there are some authors who relate corporeal posture and mouth breathing.
Ricketts (
1968), quoting a “Forum About Tonsils and Adenoids Problems...” showed the importance of the size of the nasopharynx in relation to the presence of adenoidal tissue. If it is deep the soft palate will lean properly; if it were shallow the soft palate would be in an abrupt acute angle in relation to the spina nasalis posterior. Under these conditions, mainly in tall and thin persons, the tongue would not occupy the proper position; the soft palate would be more backwards and upwards thus obstructing the nasopharynx. To permit the passage of air the soft palate could have a downward tendency and so the tongue would be in a more anterior and lower position within the mouth as a consequence of the functional requirements of the soft palate.
The same author pointed out that the tongue placed in a more forward position, was frequently seen in those cases in which the nasopharynx was obstructed by the pharyngeal tonsil. The tongue would be in that anterior position because of the condition of the nasopharynx and respiration would be a factor leading to dental malocclusion by means of the position of tongue and, probably, even of the jaw. The eruption of teeth would be related to the muscular activity on one side of the teeth by the tongue and on the other side of the teeth by the cheek.
Ricketts also commented on the high frequency of the collateral effects of the palatine and pharyngeal tonsils and related them to the Respiratory Obstruction Syndrome. Some of the characteristics of this syndrome are: a long face; crossed unilateral or bilateral bites or open bites because of tongue forward projection; short lips and teeth projected forward and bilateral constriction of the jaw that may be associated to a jaw deflection which leads to a functional crossed bite. In some cases the head is rotated on the cervical axis attempting to increase the passage of air.
Freunthaller (
1975) mentioned the importance of the examination by the rhinologist to define the causes of mouth breathing by means of rhinoscopy. Freunthaller believed that a person suffering from mouth breathing has a functional deviation of mouth, facial and postural muscles which leads to the improper development of the masticatory apparatus, which points to malocclusion.
Solow and Kreiborg (
1977) analyzed 120 persons through cephalometry and suggested that the connection between nasal aerial obstruction and facial alteration results in the lengthening of the soft facial tissue, thus changing craniofacial morphology. According to the authors, nasal obstruction leads to a change of the posture of the head, which in turn, affects dentofacial development.
Subtelny (
1980) considered nasal respiration as the proper utilization of the nasal and nasopharyngeal tract and believed that the increase in development of the structures contained in these anatomic areas as well as that of the adenoidal tissue of the nasopharynx and of the nasal turbinated bones could prevent the passage of air along the nasorespiratory channel. If the nasal obstruction were large enough as to prevent nasal respiration, it could result in an adaptation to mouth breathing. This type of respiration would cause the postural adaptation of the structures of the head and of the area of the neck which would lead to undesirable consequences in inter maxillomandibular relations and in the development of occlusion.
Joseph (
1982) mentioned that a disorder in growth balance in both the lymphoid tissue of nasopharynx and of the nasopharynx area could lead to mouth breathing which would have consequences on the face and on dentition. He pointed out that, after the cause of the obstruction had been removed and nasal respiration was restored, malformations were reduced and looks and health became normal. Joseph considered the following as the effects of mouth breathing: adenoid facies; increased inferior facial height; increased mandibular plane angle and a more open gonion angle; a more forward position of the tongue; atypical deglutition; narrower superior arches with anterior open bite; alteration of the posture of the head and gingival hyperplasia.
Aragao (
1991) described the corporeal posture of children suffering from mouth breathing. He said that their neck is forwardly projected; the neck and scapulae muscles are affected causing an abnormal posture; shoulders are rounded; and their chests are sunken. Muscular malfunctioning results in short and quick respiration. The movement of the diaphragm is altered, abdominal muscles become flaccid and arms and legs adopt a new position in relation to gravity.
Sa Filho (
1994) described a series of characteristics of patients suffering from mouth breathing. Of the characteristics studied, he considered the following alterations: dentomaxillo-facial (muscular and of the skeleton), otorhinolaryngologycal, physiology of the digestive apparatus, of general metabolism and of the ocular apparatus. He made a detailed description of the alteration in the skeleton and musculothorax which includes: (1) thorax carenatum; (2) thorax excavatum; (3) plane thorax; (4) emphysematous thorax; (5) inspiratory thorax; (6) shoulders in a forward and fallen position; (7) winged scapulae; (8) rachidial alterations; (9) kyphosis; (10) scoliosis; (11) lordosis; (12) pelvic asymmetries; (13) hypotonicity; (14) improper muscular work; (15) protruding abdomen; (16) flat feet.
Vig and collaborators (1980) studied the relation between nasal aerial obstruction and postural alteration in 30 persons. They closed the nostrils of the subjects for an hour and a half and found an anterior-vertical increase of the extension of the head during that term. That study proved that nasal obstruction results in a progressive lengthening of the neck.
Kumar and collaborators (1995) performed cephalometric research focusing on the relation between the hyoid bone and the first cervical vertebra (atlas) in people suffering from mouth breathing. They studied 29 patients (17 boys and 12 girls), aged 10 to 14 who were examined through a cephalometric analysis and later compared with 23 subjects (11 boys and 12 girls) who had nasal respiration. The assessment performed in both groups was based on clinic record and evaluation. This research indicated that those affected by mouth breathing have an extended head posture causing a clear increase of the distance between the occipital and the dorsal arch of the first cervical vertebra.
Farah and Tanaka (
1997) conducted research in order to characterize the posture and the mobility of cervical column and the trunk of people suffering from oral myofunctional alterations. They studied 26 persons aged 14 to 29, of both sexes. Patients were assessed in relation to the mobility of their cervical column and their trunk and to the position of their heads. Photos as per a customized method recorded posture. This research proved that patients with oral myofacial alterations suffer from head protraction, diminution of the tibia-tarsal angle, hyperextension of the knee and forwardimpelled pelvis as well as diminution of the cervical and trunk mobility.
Saboya (
1987) found a significant percentage of alteration in the posture of the head, in relation to the sagittal axis resulting in changes of equilibrium. Such axis is described in physiotheraputical literature (
Rolf, 1990) as the position in which the ear of the person is aligned with his/her shoulder. A lack of harmony between the tongue, the lips, the palate and the jaw is generally associated with a lack harmony and flexibility of the head and neck.
METHOD
Subjects
The 5 to 10 year old age range was chosen with the purpose of highlighting that group of children who more frequently consult a SpeechLanguage-Pathologist due to mouth breathing.
The age limit of 10 was established to avoid the mistake of including in the analysis contingent alterations inherent to puberty growth and the lower limit was established because at this age the problem is almost nonexistent as practically no child 5 years old ever goes to the SpeechLanguage-Pathology clinic because of respiratory alteration.
The groups were formed by recruiting 50 (fifty) children for the Mouth Breathing Group (MBG) at Speech-Language-Pathology and
Odontological clinics. The children had, at least, two of the following problems: Open anterior bite
Everted or flaccid lips
Broadened base of the nose
Circles under the eyes
Tongue anterior projection
Facial flaccidity
Identified patients suffering from visual deficiency, auditory deficiency, orthopedic and neurological alterations were excluded (through summary anamnesis), from the study.
To form the Control Group (CG) children of the same age range were selected from private schools which constitute an incidental sample of this population. The selection criterion was adopted using middle-high socio-economical standard. Thus, to constitute the CG, 30 (thirty) children aged 5 to 10 were chosen who presented the following characteristics:
Nasal respiration
No visual alterations
No orthopedic devices (braces, corrective footwear, etc.)
No neurological alterations
No orthodontic devices.
To analyze the results, the MBG was divided into 5 (five) age sub-groups; consisting of 10 (ten) children suffering from mouth breathing. The CG consisted of 6 (six) children in each sub-group). The sub-groups were divided as follows: from 5-0 to 6-0 years old; from 6-1 to 70 years old; from 7-1 to 8-0; from 8-1 to 9-0 years old and from 9-1 to 10-0 years old.
Procedure
All of the children were analyzed by means of pictures taken from three positions: frontal, lateral and DORSAL, as proposed by
Rolf (
1990). From those positions it was possible to perform a proper examination of postural
alterations. The photos were taken with a POLAROID camera, SPECTRA 2 model, and using a HIGH GRID DEFINITION film. This film, which was previously squared, allows the observed subject to be adjusted in relation to the ground and to the vertical plane. Using this technique it was possible for an immediate analysis of the pictures to be made and to rephotograph if necessary. To enhance the quality of the analysis, colored pictures were used.
The camera was placed on a tripod, 1 meter from the ground and 2 meters from a constant background. The children were placed 20 cm from the wall standing on a spot marked on the floor. They were standing but not leaning against the wall, without crossing their feet or hands and without resting their hands on their waist thus avoiding any alterations in posture. They were asked to look at a place far away (their eyes lost in the horizon) in their most natural way.
The following criteria was defined for analysis of the pictures of the children of both groups, MBG and CG:
Frontal pictures: the plane of the shoulders was analyzed in relation to the ground. In this way it was possible to analyze the posture of the shoulders in relation to the frontal plane; the result may be symmetric or asymmetric. These results are presented as FRONTAL.
Lateral pictures: the plane of the head is analyzed in relation to the neck. In this way it is possible to observe the posture of the head in relation to the Sagittal plane; the result may be anterior, posterior or normal (the head is in the body axis). These results are presented as SAGITTAL.
Dorsal pictures: scapulae are analyzed in relation to the body axis. In this way it is possible to observe the posture of the scapulae in relation to the horizontal plane; the result may be symmetric or asymmetric. These results are presented as DORSAL.
To obtain a more effective analysis for each segment examined, the following characteristics were observed for each plane:
Frontal plane: the right and the left sides of the body were compared and shoulders, face and head asymmetry were observed.
Sagittal plane: anterior or posterior displacement of the head and the position of the cervical spinal column in relation to the shoulders were observed.
Dorsal plane: scapulae, elbows and waist line asymmetry were observed.
Based on the review of research, the purpose of this paper was to verify if children suffering from mouth breathing do or do not present postural alterations as a result of oral respiration and to compare the results with those children who have nasal respiration.
Other situations could also result in postural alterations in children and to ensure that the children of the research did not present postural alterations resulting from other etiologies different from mouth breathing, children affected by hearing, visual or neurological alterations or from orthopedic problems as these may cause postural alterations, were excluded from the sample Groups (MBG) and CG.
To analyze statistically (The conclusions presented in this article are derived from statistical analysis based on several variables. The tables presented are a summary of the greater analysis, and I believe represent the conclusions that were drawn. If there is an interest in more detailed statistical information please contact me.) the collected data, two methods were used: FISHER and KAPPA. Fisher’s method verifies the relation between two qualitatively measurable characteristics. Under Fisher’s methodology, a value less than or equal to .05 is understood to be a significant difference. Larger than .05, it is understood that there is no significant difference.
In this study, Fisher’s methodology was aplied to determine if there is a relationship between sex and posture and to determine if there is a relationship between types of posture (frontal, sagittal and dorsal) and the groupings studied (age groups and sex). The results obtained demonstrated values less than .05 indicating statistical relevance.
Kappa’s methodology is applied when assessing the grade of concordance between two information groups of data. If a value of z (k) is greater than 1.64, then a concordance is sifnificant to 5%. In this study the level of concordance was 5%.
Kappa’s methodology was applied to determine the relationship between the types of posture studied. For example, the methodology was used to analyze the relationship between Frontal and Dorsal postures among the age group 5 to 8 years within the control group. The values obtained were greater than 1.64, indicating their statistical relevance.
The first step was to verify whether differences exist in the postures studied (Frontal, Sagittal and Dorsal) for male and female children. For this purpose MBG and CG groups were evenly divided by sex.
The next step was to verify if there were differences in the postures analyzed, in relation to age as a consequence of normal growth. Groups MBG and CG were divided in five age ranges (5-0 to 6-0 years; 6-1 to 7-0 years; 7-1 to 8-0 years; 8-1 to 9-0 years; 9-1 to 10-0 years).
Having finished with the statistical analysis [The conclusions presented in this article are derived from statistical analysis based on several variables. The tables presented are a summary of the greater analysis, and I believe represent the conclusions that were drawn. If there is an interest in more detailed statistical information please contact me.] it was necessary to create a new grouping of homogeneous population which became the subject of our research from then on. These groups were: Age range: 5-0 to 8-0 years and Age Range: 8-1 to 10-0 years.
RESULTS
Analyzing the pictures, the following results were obtained:
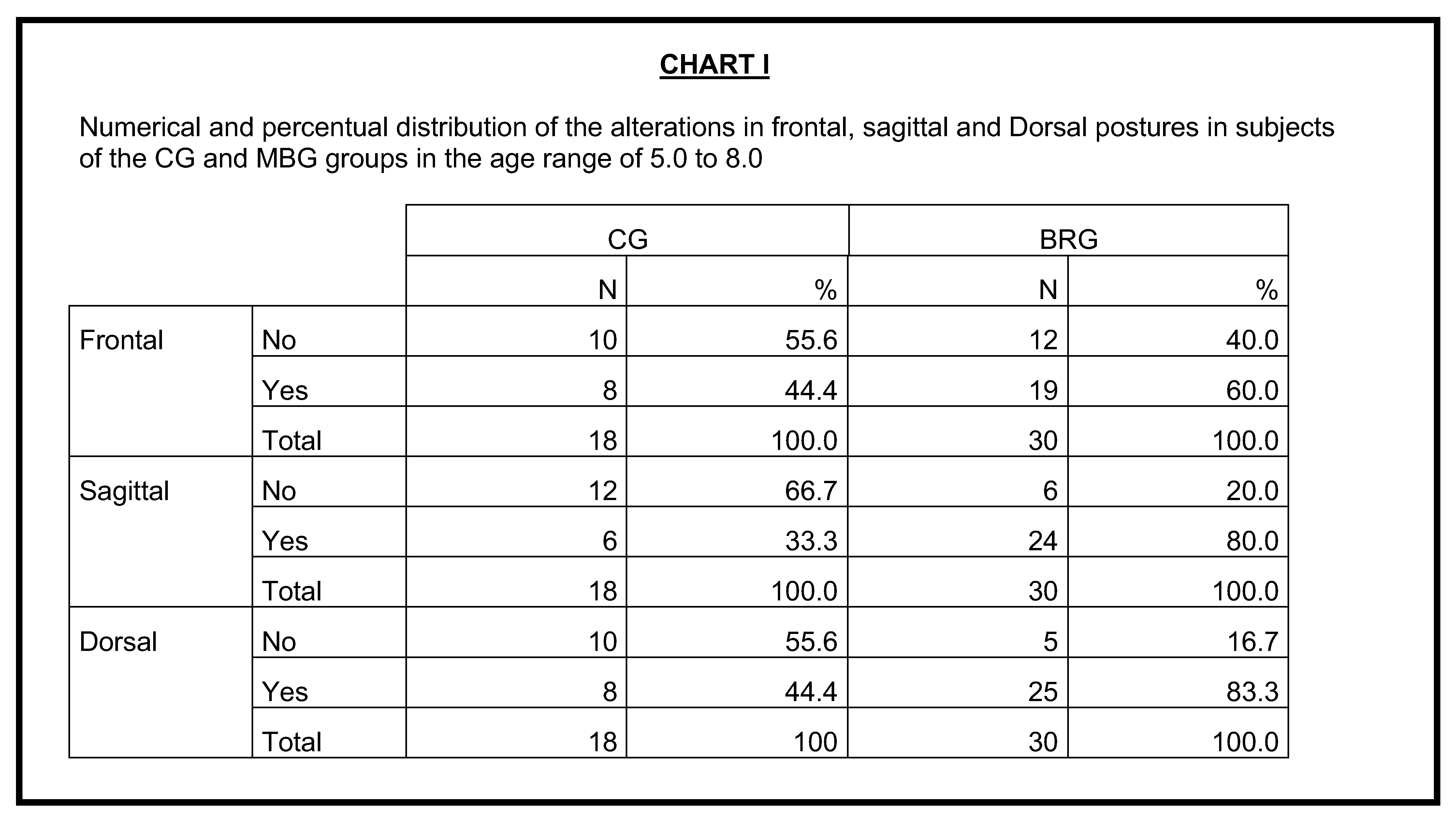
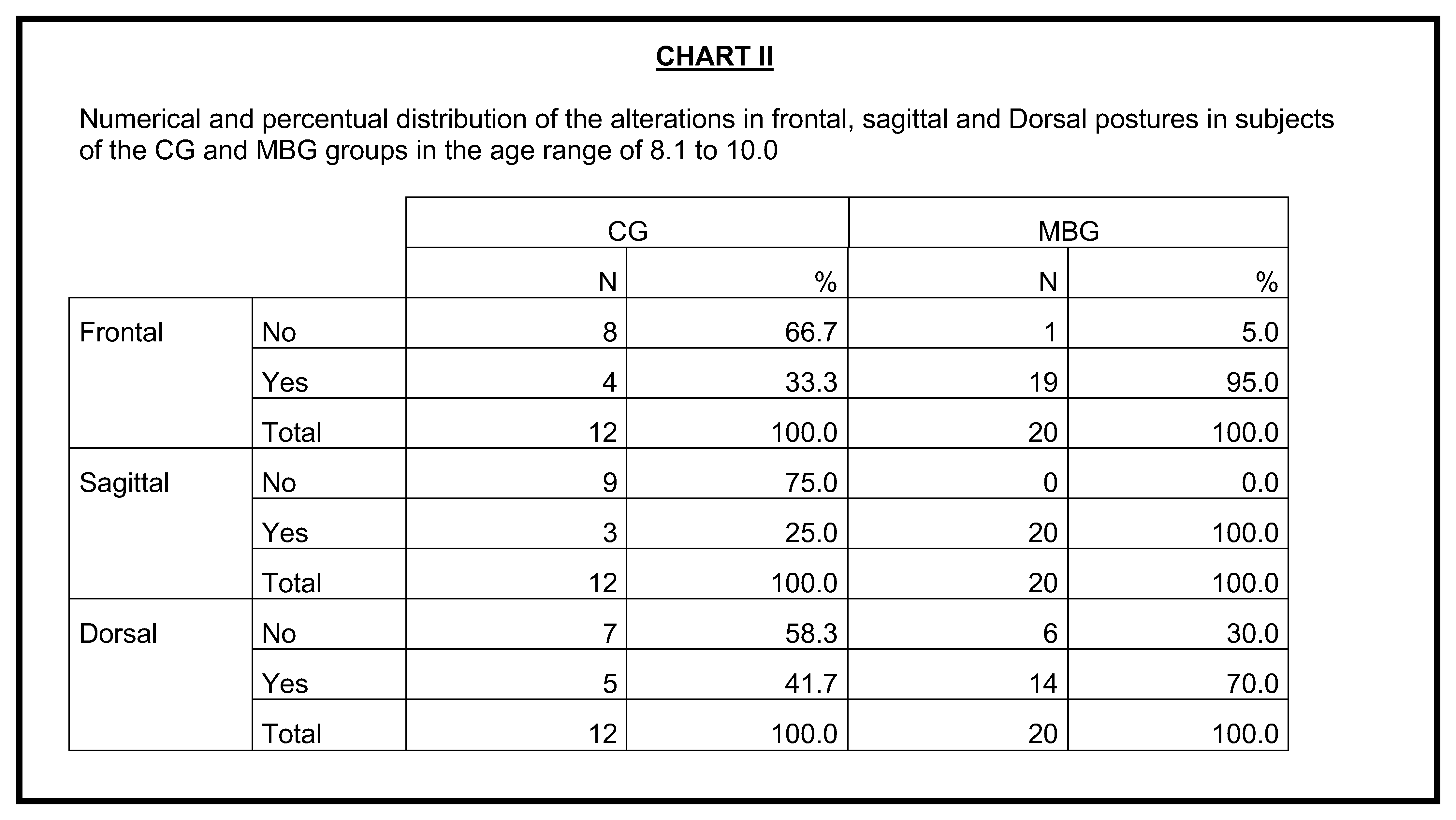
Frontal posture: the statistical results of this study show that the frequency of alterations in FRONTAL posture in CG is statistically the same as the frequency of alterations in MBG for the age range of 5-0 to 8-0 but for the age range 8-1 to 10-0 CG ‘s frequency is lower.
Sagittal posture: the statistical results of this study provide evidence that for the age ranges 5-0 to 8-0 and 8-1 to 9-0 the frequency of alterations in this posture is lower in CG.
Sagittal posture: the statistical results of this study demonstrate that the number of alterations in CG is lower than that of the MBG for age range of 5-0 to 8-0 years however it is the same for the age range 8-1 to 10-0 years
These results can be seen in Charts I and II.
![Ijom 26 00002 g001]()
![Ijom 26 00002 g002]()
It was possible to observe through the results and the analysis of the pictures, that most of the children in the MBG and 8-1 years and older have their head axis out of alignment in relation to their shoulders. Children suffering from mouth breathing change the posture of their heads, probably to adapt the pharyngeal angle to facilitate the intake of air through their mouth, trying to obtain a better superior aerial flux. The change of the head axis also alters the position of the mandibular resting posture, the occlusive contacts and the optical and bipupilar plans. It is possible, that after these changes, adaptive movements of the body appear in order to obtain a more comfortable posture and balance.
From the above, it can be understood that children suffering from mouth breathing alter their physiological functioning of respiration and that the posture of the head undergoes transformations. As a consequence, the relationship of the head and neck and of the neck and trunk may also be altered.
Therefore, we can state that those children exhibiting nasal respiration, alignment of a straight corporeal axis takes place naturally in the three planes (FRONTAL/SAGITTAL/DORSAL). This physiological phenomenon would be hindered when vicarious mouth breathing is needed in the Sagittal plane mainly influenced by head projection.
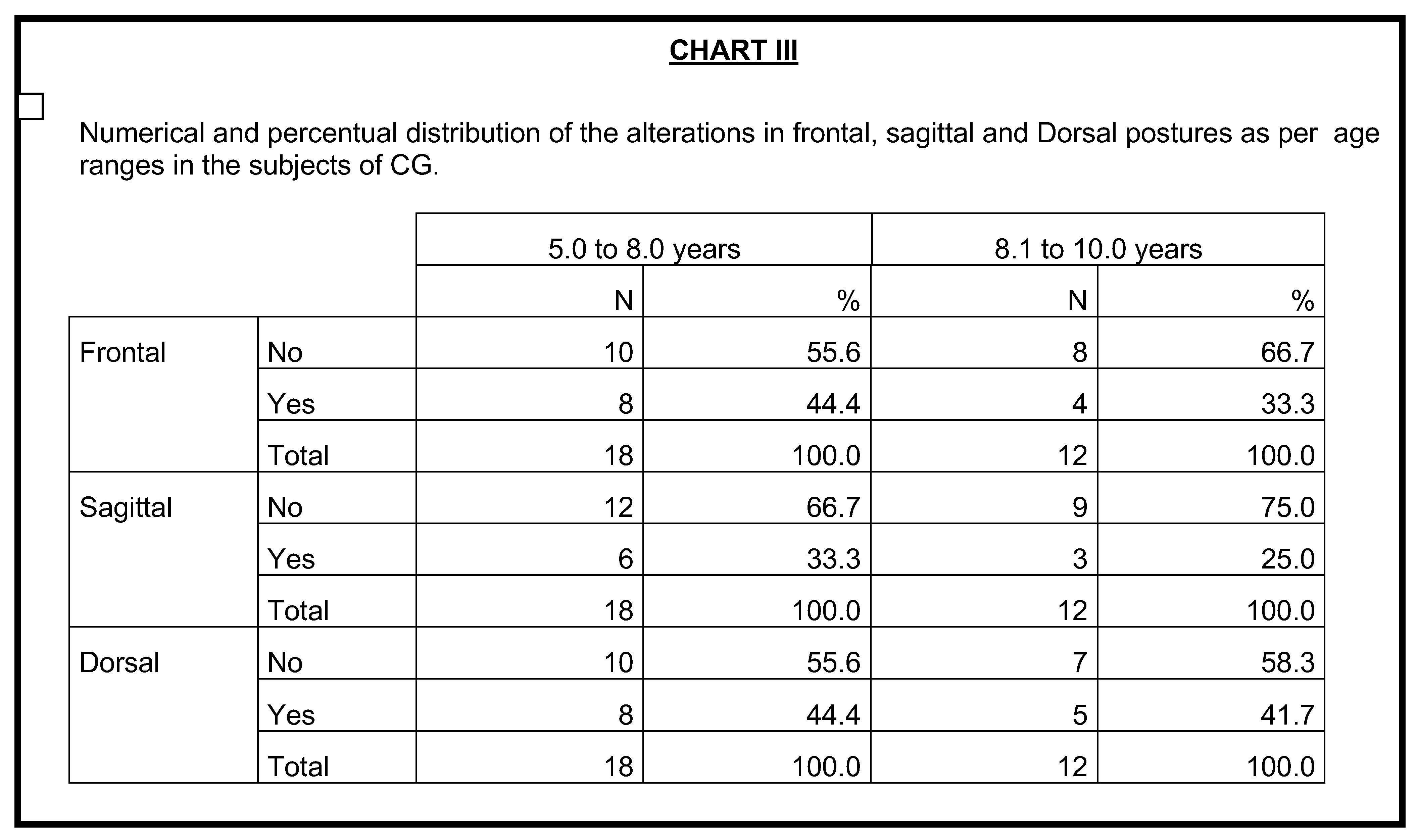
We also verified whether, as time passes, there is a change in the corporeal behavior of children and if there are any differences between CG and MBG. In the CG, the number of alterations found in the postures studied in the 5-0 to 8-0 age range was the same as the number of alterations in the same postures in the 8-1 to 100 age range.
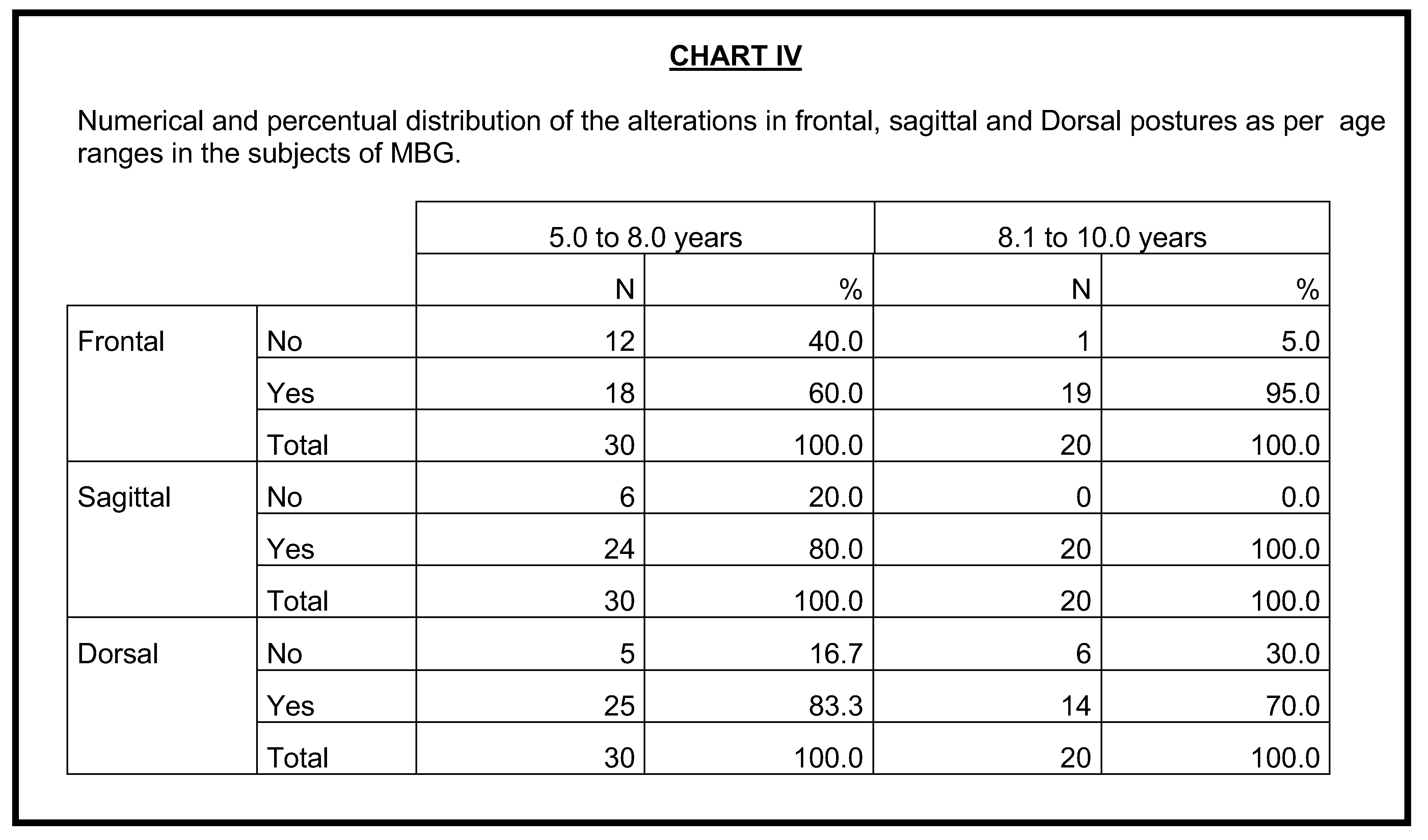
In relation to the MBG the number of alterations found in FRONTAL posture in the age range 5-0 to 8-0 years was lower than the number of alterations in the same posture as in the age range 8-1 to 10-0 years. In relation to SAGITTAL and DORSAL postures, the number of alterations in the age range from 5-0 to 8-0 years was statistically the same as those in the age range from 8-1 to 10-0 years.
In addition to these results, although not significant from a statistical point of view, the percentage of alterations are lower in the Age range from 8-1 to 10-0 years in all postures.
On the other hand, in the MBG the opposite happened for FRONTAL and SAGITTAL postures. By analyzing these postures, the percentages of alterations found were higher in the 8-1 to 10-0 age range. This increase is statically significant for the FRONTAL position and represents an important tendency to SAGITTAL position. It is only for the DORSAL position that that percentage of MBG behaves in the same way for the CG.
Based on the results of the CG the data point out that, as children grow, there is an evolution of their FRONTAL, SAGITTAL, and DORSAL postures. This development does not appear to take place with children of the MBG and thus it is possible to infer that to keep an adequate corporeal axis, nasal respiration is necessary.
The results above may be observed in Charts III and IV.
![Ijom 26 00002 g003]()
![Ijom 26 00002 g004]()
DISCUSSION
Beziers and Hunsinger (
1994) show the importance of four basic functions of the body in relation to the development of motor coordination. They are: rolling, straightening, twisting and tension. In relation to the development of the trunk and the head, it is necessary to consider the following: head rolling is a very complex movement that starts at the lip muscles and coordinates all the muscles of deglutition; the hyoidic motor center, allowing the balance of the head in a forward direction thus opening at the back the space between the two first cervical vertebrae. This movement represents a small leaning of the head during anterior flexion.
In relation to straightening, the muscles of the posterior part of the trunk—the extensor muscles of the back—may be considered a kind of spring. The flexion-extension process ensures harmony and the antero-posterior balance of the body. In the case of lack of harmony between the flexor and extensor muscles the trunk adopts an incorrect position.
In 1996, Beziers and Hunsinger pointed out that mouth breathing led to alterations in the flexion process, as it did not allow the creation of a space between the two first cervical vertebrae, thus resulting in a diminution of the space in that area and, as a consequence, a more forwarded position of the head.
Denys-Struyf (
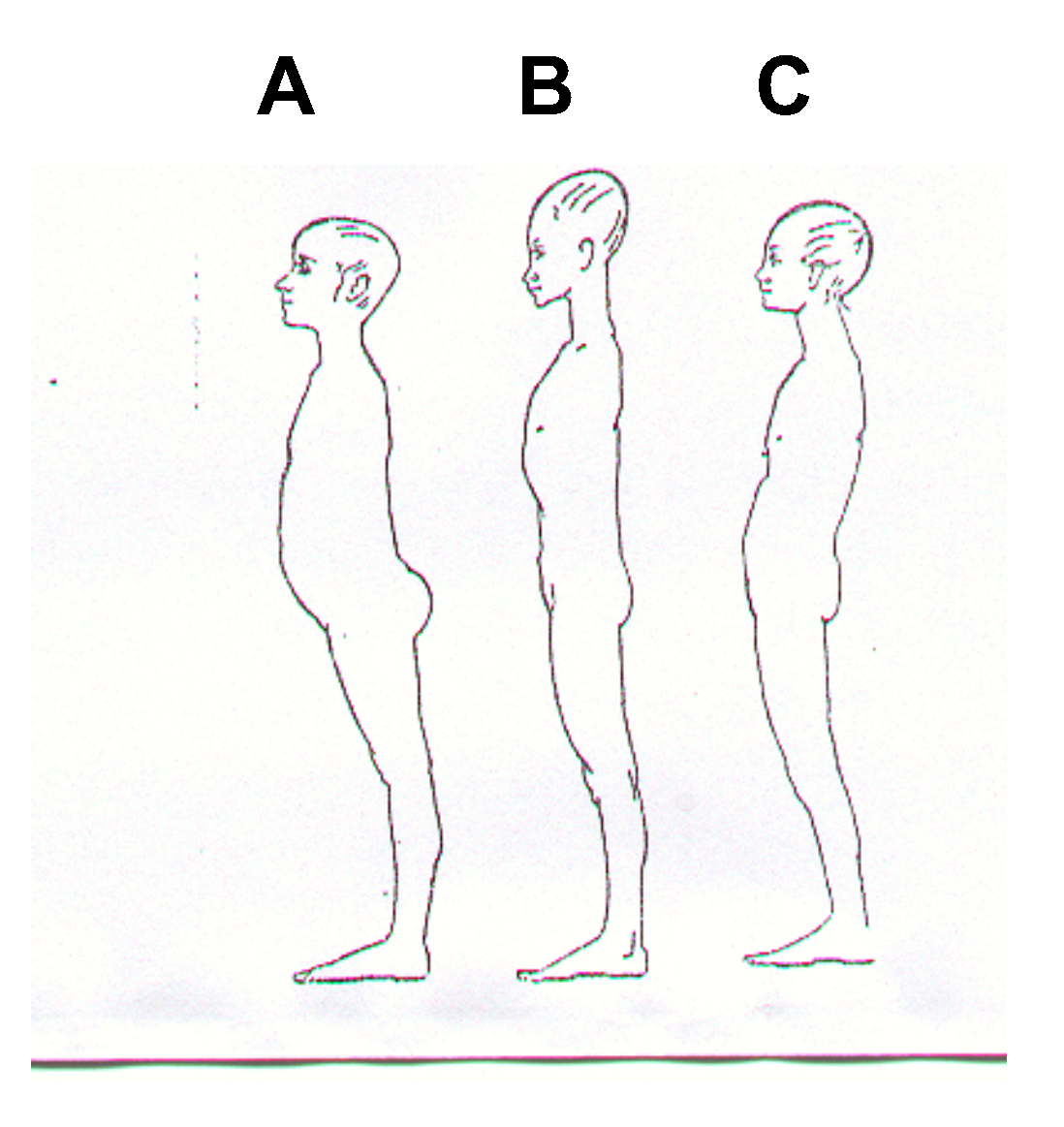
1995), considered the corporeal axis and its lack of harmony, and believed that the balance of a standing man was the consequence of the activity of three masses: cephalic, thoracic and pelvic. The observation of a person starts by his/her expression in a standing position and mainly by observing the ways he/she adapts to find the balance in his/her natural standing position. The corporeal expression forms considered as most important are associated to the forms adopted to ensure the balance of the body in a standing position in the SAGITTAL axis. We have different gestures and attitudes, but our static posture is mainly characterized by how we choose a kind of balance. In picture (1) we can see in (C) the corporeal axis in equilibrium and in the lateral pictures, the adjustment to a new standard of balance leading to forwarded postures (a) or backwarded postures (B).
![Ijom 26 00002 g005]()
Rocabado-Seaton (
1979) considered the importance of the relation between the skull, the cervical column and the Stomatogtonatic System. The author stated that the straight stability of the skull (orthostatic) was very important, as there was a delicate equilibrium of the skull upon the occipital region. The equilibrium of the lowest part of the skull depends on the masticatory muscles and on the muscles of the supra and infra-hyoidic region. The analysis of Stomatognatic System cannot be separated from its relationship with the structures of the head and of the neck, which should be assessed as a whole and have an integral treatment.
Akerman (
1997) stated that children of up to 7 or 8 years of age did not have complete function of their abdominal muscles, which are not fully developed at that age, but would begin to mature at that age. Abdominal muscles are responsible for the stability of the sternum, the ribs and the spinal column, thus aiding respiration and speech.
Between 5 and 8 years of age sudden growth activities takes place that cause disorganization in the body of children who, little by little, reorganize their posture in space, if typical development takes place. As the abdominal muscles have not yet finished their development, the trunk does not receive the proper activity of those muscles and so they do not allow the lowering of ribs which move forward to compensate for the lack of abdominal activity.
Children, therefore, end up adapting themselves to a new compensatory posture. With these data we can imagine that the superior part of the trunk receives less support causing a disorganized posture with a protruding abdomen, winged scapulae and asymmetric shoulders.
In the case of children older than 8 years of age, the findings of our research are different, as an improvement of posture in CG can be observed, thus improving their corporeal characteristics, which did not improve in MBG group. Therefore, children present an improvement in their posture as they grow up which is jeopardized by mouth breathing.
CONCLUSIONS AND RECOMMENDATIONS
Based on the findings of this research, it was verified that children of 5-0 to 8-0 years demonstrating either mouth breathing or nasal respiration present postural alterations. However, children older than 8 years with nasal respiration improve their posture as they grow up while children suffering from mouth breathing keep the disorganized corporeal standard consistent with postures found in younger children.
In this way it seems that it is inadequate to use the word pathological to define the postural alterations of children having oral respiration until they are 8 years old. However, if that respiratory standard persists beyond that age, it could cause structural alterations in the corporeal axis of these children when compared to children having normal respiration.
Postural alterations take place in the same way in both sexes. Children of up to 8-0 do not show any statistical differences between the postural alteration of those having nasal respiration and those who suffer from mouth breathing.
However, from 8-0 onwards the frequency of alterations is statistically larger in the group of children who demonstrate mouth breathing than that of the children who have nasal respiration. Children having nasal respiration present a better corporeal harmony than the children who suffer from mouth breathing.
The speech-language-pathologist has a very important role in children aged 5-0 to 8-0 who present with mouth breathing difficulties. The therapist may be able to suggest interventions to prevent the development of serious postural problems, which could lead to further rehabilitation difficulties.
Picture control, especially those of the SAGITTAL plane, has proven to be efficient both for diagnostic and follow-up processes. The photos must be taken every two months to observe and evaluate progress of myofunctional therapy.
The utilization of pictures has proven to be an efficient method of characterizing postural alterations. Picture documentation should be included in Speech-Language-Pathologist practice. The Sagittal plane is the one that affords the most information regarding postural alterations.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}