Abstract
Background/Objective: High-risk Human papillomavirus (hrHPV) is the leading cause of premalignant lesions and cervical cancer (CC), affecting disproportionally women living with HIV. Mozambique is among the countries with a heavy triple-burden of HIV, hrHPV infections and CC which accounts for more than 5300 new cases and 3800 deaths each year. In this study, we assessed the age-specific distribution and factors associated with hrHPV and cervical lesions among HIV-positive and -negative women from HPV-ISI (HPV Innovative Screening Initiative) study in Maputo, Mozambique. Methods: This cross-sectional study included 1248 non-pregnant women aged ≥18 years who attended CC screening at the DREAM Sant’Egídio Health Centre between July 2021 and April 2022. Screening involved visual inspection with acetic acid (VIA) and high-risk HPV DNA testing. Sociodemographic, lifestyle, and reproductive data were collected through a routine questionnaire. Logistic regression assessed associations between risk factors and hrHPV infection or cervical lesions. Age-specific hrHPV prevalence, partial HPV16/18 genotyping, and abnormal cytology rates were further analyzed by HIV status. Results: The mean age of participants was 43.0 ± 8.6 years. Overall hrHPV prevalence was 28.0%, being higher among HIV-positive women (46.8%) than HIV-negative women (23.8%). Non-16/18 hrHPV genotypes predominated across all age groups. VIA positivity was 11.1%, most frequently involving less than 75% of the cervical area and was more common among younger women (30–45 years) and those living with HIV. Increasing age was associated with lower odds of hrHPV infection (OR = 0.98, 95% CI: 0.97–1.00; p = 0.017), as was higher parity (≥3 deliveries vs. nulliparity: OR = 0.58, 95% CI: 0.36–0.94; p = 0.029). Contraceptive use (OR = 1.65, 95% CI: 1.15–2.38; p = 0.007) and a partially or non-visible squamocolumnar junction (SCJ) (OR = 2.88, 95% CI: 1.74–4.79; p < 0.001) were associated with higher odds of VIA positivity. Conclusions: hrHPV infection and cervical lesions were more frequent in younger and HIV-positive women, highlighting the need for strengthened targeted screening within HIV care services in Mozambique.
1. Introduction
Human papillomavirus (HPV) is one of the most common sexually transmitted infection (STI) worldwide [1,2]. Infections with HPV have a high negative impact on women social life in Sub-Saharan Africa, as they are responsible for a significant proportion (ranging from 20% to 26%), of all cancers diagnosed [3], mainly cervical cancer (CC)—the most common female cancer and leading cause of morbidity and mortality in the region [4,5].
Genital infection with HPV is substantial high during the individual’s lifetime, with an estimated risk of 60–84.6% among sexually active women; however, without necessarily developing any symptoms [1,6]. Most (80–90%) of these infections are cleared spontaneously within 12–24 months; some, particularly by oncogenic types—well known as high-risk HPV (hrHPV), persist and induce the development of premalignant lesions and CC over time [5,7,8]. To date, the hrHPV include fifteen genotypes (HPV 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 68, 73, and 82), classified as oncogenic, and three genotypes (HPV 26, 53, and 66), considered probably carcinogenic [9,10].
The worldwide prevalence of HPV infection in women with no cervical abnormalities is 11–12%, with higher age-standardized rates in sub-Saharan Africa (24%), compared to other region (16–21%) [1,2]. Immunodeficiency is a major determinant of HPV infection and CC risk [11]. Women living with HIV face a disproportionately high burden, including increased acquisition of HPV, higher frequency of multiple infections, and greater likelihood of persistent hrHPV infection, resulting in a six-fold increased risk of premalignant lesions and CC [11,12,13]. On the other hand, the exposure and acquisition of HPV infection relay primarily on sexual lifestyle-related factors, including early age of sexual debut, the number of lifetime sexual partners, history of STIs, and others. In addition to these, other factors such as smoking, diet/malnutrition, parity, use of hormonal contraceptives, alcohol consumption, and concomitant STIs (specially Chlamydia trachomatis, Neisseria gonorrhoeae, Mycoplasma spp., and Herpes virus), have been associated, beyond the acquisition of the infection, with a higher probability of hrHPV persistence, and further development of premalignant lesions and CC [14,15,16]. Additionally, an older age, lower socioeconomic and educational status [17,18,19] have also been associated with an increased risk of disease in HPV-seropositive women.
Mozambique is among the countries with a heavy burden of HPV infection, HIV, and cervical cancer [11,20]. The prevalence of HPV infection among Mozambican women is alarmingly high, with studies indicating significant rates of hrHPV (HPV 16, 18, 31, 33, 35, 45, 51, 52, and 58), either among women with normal cytology [1] or among those diagnosed with cervical precancerous lesions and cancer; varying from 20% to 75.9% [21,22,23,24,25,26]. Every year, more than 5300 cervical cancer new cases and more than 3800 deaths are registered [20], affecting particularly women living with HIV/AIDS [27,28]. It is estimated that in the general population, around 8.6% of Mozambican women of reproductive age (>18 years old) have had a cervical hrHPV infection at some point in their lives, with HPV types 16 and 18 accounting for over 51.0% of invasive CC cases [20,29].
In the overall picture of HPV infection and CC incidence in Mozambique, the key contributing factors include the high rates of HIV infection (between 15.1 and 26.6%) among sexually active women or those of reproductive age [30,31], and the strikingly low availability and uptake of annual cervical cancer screening [28,32]. Meanwhile, although the prevalence and distribution of HPV genotypes in Mozambique have been considerably elucidated, little is known about age-related differences and the sociodemographic, lifestyle, and gynecological factors associated with hrHPV infection and cervical lesions within the context of HIV care in the country.
Knowledge of risk factors, combined with early detection of high-risk HPV infection and precancerous lesions, provides essential information for identifying at-risk populations and preventing CC [7,33,34]. In this study, we present the age-specific distribution and factors associated with high-risk HPV infection and cervical lesions, stratified by HIV status, among Mozambican women. The objective was to identify determinants of hrHPV infection and cervical abnormalities to inform the implementation of HPV-based screening programs in Mozambique [28,35,36].
2. Material and Methods
2.1. Study Design, Participants and Ethical Approval
This is a cross-sectional study in which we analyzed data of 1248 women aged over 18 years who were recruited and screened for hrHPV during a larger research project named HPV innovative screening approach (HPV-ISI), conducted at the DREAM Sant’Egidio health centre in Zimpeto, Maputo, Mozambique [26]. The DREAM Sant’Egidio health centre is an HIV-focused primary care facility affiliated with the DREAM program, a health initiative run by the Community of Sant’Egidio across 11 African countries and providing care to over 500,000 patients. The program implements multiple health projects in sub-Saharan Africa and is actively engaged in laboratory research [26,37,38,39,40,41]. At the DREAM Sant’Egidio health centre, cervical cancer (CC) screening is routinely conducted for women from both urban and rural settings, using a combined visual inspection with acetic acid (VIA)-hrHPV testing approach.
The HPV-ISI research project was conducted between July 2021 and May 2022 and evaluated the feasibility of hrHPV DNA testing compared to the VIA screen-and-treat approach (VIA was used as a screen and not as a triage for hrHPV-positive women) [26], preceding the launch of the national pilot program of hrHPV screening, triage and/or treatment in Mozambique, introduced in 2023 [42].
Figure 1 illustrates the flow diagram of women screened and included in the study analysis. The initial dataset comprised 1323 women (participants) aged over 18 years who were voluntarily recruited from DREAM HIV care centers and from referrals originating from other public health facilities within the Maputo region. Participants were not randomly selected, nor were they sampled to obtain similar numbers of HIV-positive [+] and HIV-negative [+] women. Instead, women were consecutively enrolled as they presented for routine services, and the final sample reflects the natural distribution of HIV status among service users during the study period. Of the 1323 women screened for hrHPV, we excluded 75 records due to missing outcome data and incomplete key variables (Table 1), yielding a final sample of 1248 participants for this analysis. The inclusion criteria were: (1) women aged ≥18 years with documented genital hrHPV and VIA results; and (2) not currently pregnant. The exclusion criteria were: (1) missing data in more than three study variables (Table 1); and (2) indeterminate or invalid hrHPV results. All participants provided written informed consent. Ethical approval was obtained from the Mozambican National Ethics Committee (ref. 688/CNBS/20) and from the Institutional Health Bioethics Committee of the Faculty of Medicine, Eduardo Mondlane University, and Maputo Central Hospital (ref. CIBS FM&HCM/019/2023). All data were anonymized using numerical codes prior to database creation.
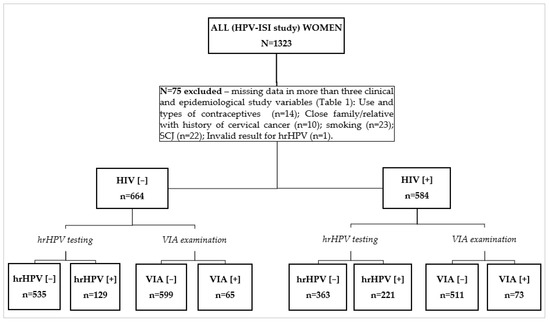
Figure 1.
Consort flow diagram of women screened and included in the study analysis. HIV—human immunodeficiency virus; SCJ—squamocolumnar junction; VIA—visual inspection with acetic acid; hrHPV—high-risk human Papilomavirus; [−] Negative results; [+] Positive results.

Table 1.
Participants data and variables analyzed in this study.
2.2. Data Collection, Samples and Screening Tests
In this study, the outcome variables of interest were hrHPV and VIA cervical screening results of the participants. We considered as potential factors, the variables (Table 1) found to be related to testing hrHPV and VIA positive [+] in previous studies or otherwise biologically plausible.
In summary, to obtain the data used in this study, all participants responded to a brief routine structured questionnaire that included questions on sociodemographic information, lifestyle, sexual and reproductive behavior, and clinical data (Table 1). After the brief questionnaire, a cervical sample was collected and placed into a 20 mL Liquid Media (Roche Cell Collection Medium), which was then sent to the local Molecular laboratory for hrHPV-DNA testing. After sampling for HPV testing women were screened with the current national recommendations based on VIA [43]. For all VIA [+] cases, a digital colposcopy (DC) was performed for lesion confirmation. Cryotherapy was subsequently performed on-site if VIA tested positive with lesions < 75% of the cervix, and women with confirmed major lesions were referred for biopsy.
The hrHPV testing was performed using the Cobas HPV DNA test, in the Cobas 4800 system (Roche Molecular Systems, Pleasanton, CA, USA). The Cobas® 4800 HPV DNA test is a qualitative assay that allows the detection of 14 hrHPV types by polymerase chain reaction (PCR) and nucleic acid hybridization, giving a partial genotyping by separately identifying HPV16 and HPV18, and 12 other hrHPV types (including HPV types 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, and 68) “pooled” in the same channel. The assay utilizes a human beta-globin gene as internal control to assess the quality of the sampling and the efficiency of the PCR amplification. If internal control was not amplified, samples were referred as invalid. Only samples with a valid test result on Cobas 4800 were included in the analysis of this study.
2.3. Statistical Analyses
Data were analyzed using STATA 15.1 (StataCorp LP, College Station, TX, USA, 2017). Descriptive analyses, including means and standard deviations (SD), were performed for continuous variables, and the number and percentages for categorical variables. The detection results of hrHPV by participant’s characteristics were stratified according to HIV status and by VIA results. An independent-samples t test was used to assess the statistical differences in continuous variables across different hrHPV and VIA groups, within each HIV stratum. Chi-square tests assessed the association of categorical variables with hrHPV and VIA results, according to HIV status. Variables with frequency of less than 5 values were evaluated with Fisher’s exact test. Statistically significant (p < 0.05) variables for hrHPV and VIA results were considered for univariate binary logistic regression to estimate crude odds ratios (ORs). Analyses were conducted for the overall sample and stratified by HIV status (HIV-positive and HIV-negative).
3. Results
3.1. Characteristics of Participants
Characteristic of study population (N = 1248) analyzed in this study are shown in Table 2. The majority (84.3%) were recruited within the study site—DREAM Sant’Egidio health centre, while smaller proportions were referred from DREAM centers, Machava (10.9%), Consolata/Criança (3.7%) and Matola-II (0.9%), and other health facilities external to the DREAM program (0.2%).
Table 2.
Characteristics of study population in the HPV-ISI study (Maputo, Mozambique).
The mean age of the participants was 43.0 ± 8.6 years (range: 18–72 years). The age group with the largest proportion of participants was 30–45 years (16.3%), with 41–45 years being the most represented sub-group within this range. Regarding screening history, nearly three-quarters (74%) were screened for the first time, in comparison to other screening types. The mean age at sexual debut was 17.5 ± 2.4 years, with over half (53.4%) reporting initiation at ≤17 years. Most women were multiparous: 77.1% had ≥3 pregnancies and 63.4% had ≥3 deliveries, while nulligravidity and nulliparity were relatively small (4.2% and 6.2%, respectively).
Concerning reproductive and lifestyle characteristics, 32.9% reported irregular menstrual cycles, and 29.9% used contraceptives, mainly oral pills (9.4%), implants (6.7%), and injectables (6.1%). Family history of cervical cancer was uncommon (1.2%), and smoking was virtually absent (0.1%). A small proportion reported prior STIs or vaginal discharge (7.9%). Gynecological examination showed abnormalities in 8.1% of cases, while the SCJ was visible in 92.4%. VIA testing yielded 11.1% positive results, with most lesions involving <75% of the cervix. The prevalence of hrHPV infection was 28%.
3.2. Distribution of hrHPV and VIA Results by Participants Characteristics and According to HIV Status
Table 3 and Table 4 summarize the bivariate association analyses comparing sociodemographic, reproductive, behavioral, and clinical characteristics according to hrHPV status and VIA results, stratified by HIV status: HIV-positive [+] and HIV-negative [−]. Women with hrHPV positivity [+] (Table 3) were slightly younger than those who tested negative [−] (mean age 42.0 vs. 43.3 years, p = 0.013), a difference that was particularly evident among HIV [−] women (p < 0.001). Stratification by age groups showed higher hrHPV prevalence among women aged 30–45 years (16.5%) and ≥46 years (9.9%), compared to those ≤29 years (1.7%). Screening history also influenced hrHPV detection, with first-time attendees more frequently hrHPV [+] than those at follow-up (p = 0.038).
Table 3.
Bivariate association analyses between participants’ characteristics and hrHPV status among all women and stratified by HIV status.
Table 4.
Bivariate association analyses between participants’ characteristics and VIA results among all women and stratified by HIV status.
Reproductive history revealed significant associations. Women with hrHPV [+] were more likely to be nulligravida (p = 0.038) or have had one to two deliveries (p = 0.046), particularly among HIV [−] participants (p = 0.013 and p = 0.017, respectively). In contrast, age at sexual debut, number of pregnancies, contraceptive use, menstrual regularity, and family history of cervical cancer did not show significant associations with hrHPV. Finally, gynecological abnormalities of the vagina or uterus were more common in hrHPV [+] women (3.1% vs. 5.0%, p = 0.020), while visibility of the squamocolumnar junction and prior STI history were not significantly related (Table 3).
Regarding the VIA results, women with VIA-positive [+] results were significantly younger than VIA-negative [−] women (mean age 38.9 vs. 43.5 years, p < 0.001). This trend was consistent across both HIV [+] and HIV [−] groups. The highest VIA [+] was observed among women aged 30–45 years, while those ≥46 years were more often VIA [−] (p < 0.001). Screening type showed no significant differences, although most VIA [+] cases were detected during first-time screening (Table 4).
Reproductive factors showed mixed associations. VIA [+] women had slightly fewer pregnancies and deliveries on average, but only parity was marginally associated, with nulliparous women less likely to test VIA [+] (p = 0.036). Age at sexual debut, family history of CC, and reported STI/vaginal discharge were not significantly related to VIA results (Table 4). Contraceptive use showed an interesting pattern: women not using contraceptives had higher VIA [+] compared to users, particularly among HIV [−] women (p = 0.007). Menstrual cycle regularity, smoking history, and gynecological findings of the vagina/uterus were not significant predictors. However, visibility of the SCJ was strongly associated with VIA results, especially among HIV [+] women (p < 0.001).
3.3. Overall Prevalence of hrHPV Types According to HIV Status and Its Age-Specific Distribution
Figure 2 and Figure 3 show the distribution of hrHPV types (HPV-16, HPV-18, and non-16/18 types) in single and multiple infections according to HIV status and age groups, respectively. Among HIV [−] women, hrHPV types other than HPV-16/18 were most common (17.0%), mainly as single infections (14.2%) and less as multiple (2.8%). HPV-16 and HPV-18 were less frequent, up to 3.6% and 2.0%, respectively. In HIV [+] women, hrHPV prevalence was higher, especially non-16/18 types (31.8%), with 23.8% single and 8.0% multiple infections. HPV-16 (9.4%) and HPV-18 (5.6%) were also more frequent than in HIV [−] (Figure 2).
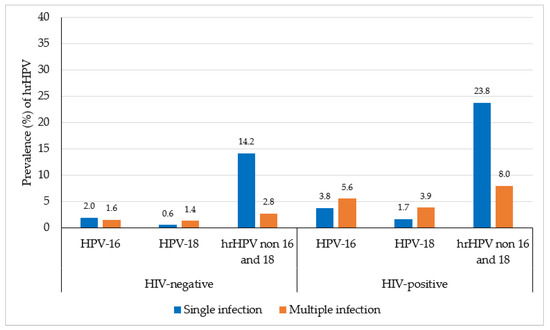
Figure 2.
Distribution of high-risk HPV detection (relative frequencies) in single and multiple infection, according to HIV status. Bar graph colors: single (blue), multiple (orange).
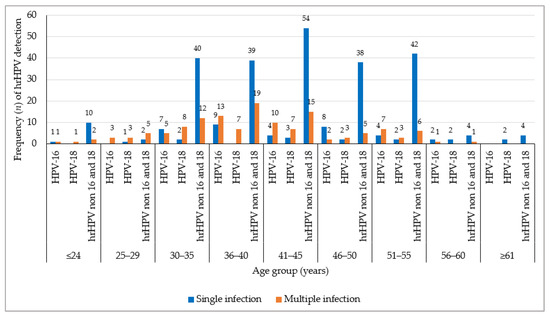
Figure 3.
Age-specific distribution of high-risk HPV detection (absolute frequencies) in single and multiple infections among all hrHPV-positive women (n = 350). Multiple infection refers to co-infection with two or three detected genotypes (HPV-16, HPV-18 and Other hrHPV). Bar colors: single infection (blue), multiple infection (orange).
The distribution of hrHPV types across different age groups (Figure 3), shows peaks among women aged 30–45 years, particularly at 41–45 years. Single infections predominated across all age groups. Non-16/18 hrHPV types accounted for most infections, both single and multiple, whereas HPV-16 and HPV-18 were less frequent and mainly detected as single infections. Multiple hrHPV infections were more common in women aged 30–45 years and declined with increasing age. HrHPV detection was markedly lower in women aged ≥ 56 years.
3.4. Overall Prevalence of Cervical Lesions According to HIV Status and Its Age-Specific Distribution
Figure 4 shows the distribution of cervical lesions—frequency of VIA-positive [+] lesions (<75% and ≥75% of the cervix) across age groups, stratified by HIV status. Among HIV [−] women, VIA [+] < 75% were identified in 59 cases (8.9% of the total), with the highest frequency in the 30–35-year age group (17 cases, 2.6%). Larger lesions (≥75%) were rare, occurring in only 6 cases (0.9%). In HIV [+] women, VIA [+] < 75% were slightly more frequent (66 cases, 11.3%), with a peak in the 36–40-year age group (26 cases, 4.5%). Larger lesions (≥75%) were also more common among HIV [+] women (7 cases, 1.2%) compared with HIV [−] women. Overall, VIA positivity was concentrated among women aged 30–45 years, with both lesion types (<75% and ≥75% of the cervix) more frequent in HIV [+] participants, highlighting the combined influence of age and HIV status on cervical lesion burden.
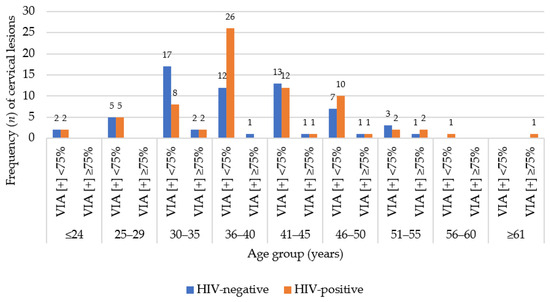
Figure 4.
Age-specific distribution of cervical lesions (absolute frequencies of VIA positivity classes, among all n = 138 cases: n = 125 for lesions < 75% and n = 13 for lesions ≥ 75%), according to HIV status. Bar colors: HIV-negative [−] (blue), HIV-positive [+] (orange).
3.5. Factors Associated with hrHPV Prevalence and Cervical Lesions
A logistic regression analysis evaluating factors associated with hrHPV infection, stratified by HIV status, showed that increasing age was associated with lower odds of hrHPV infection (OR = 0.98, p = 0.017), corresponding to an approximately 2% decrease in the odds of hrHPV per additional year of age. This association was more pronounced among HIV [−] (OR = 0.96, p < 0.001), indicating lower odds of hrHPV with increasing age, and was not statistically significant among HIV [+] women. Compared with women aged ≤29 years, those aged ≥46 years had significantly lower odds of hrHPV infection overall (OR = 0.56, p = 0.046) and among HIV [−] women (OR = 0.28, p < 0.001).
Similarly, higher parity was associated with lower odds of hrHPV infection. Women with ≥3 pregnancies (OR = 0.48, p = 0.012) or ≥3 deliveries (OR = 0.58, p = 0.029) had lower odds of hrHPV infection, particularly among HIV [−] women. No statistically significant associations between age or parity and hrHPV infection were observed among HIV [+] women (Table 5).
Table 5.
Logistic regression analysis for the association between hrHPV results with predictor variables, according to HIV status.
Regarding factors associated with cervical lesions, logistic regression analysis (Table 6) showed that increasing age was associated with lower odds of VIA positivity. Each additional year of age was associated with reduced odds of a VIA-positive result (OR = 0.94, p < 0.001). Compared with women aged ≤ 29 years, those aged 30–45 years and ≥46 years had substantially lower odds of VIA positivity, particularly among HIV [+] women (OR = 0.11 and OR = 0.06, respectively; both p < 0.001). Number of deliveries was not significantly associated with VIA positivity.
Table 6.
Logistic regression analysis for the association between VIA results with predictor variables, according to HIV status.
Contraceptive use was associated with higher odds of VIA positivity overall (OR = 1.65, p = 0.007), with a stronger association observed among HIV [−] women (OR = 2.09, p = 0.005). In addition, a partially or non-visible squamocolumnar junction (SCJ) was strongly associated with higher odds of VIA positivity, especially among HIV [+] women (OR = 4.64, p < 0.001) (Table 6).
4. Discussion
Cervical cancer (CC) ranks as the most frequent cancer in Mozambique among women of all ages in 2022, accounting for about 20.5% of female cancer cases, according to GLOBOCAN estimates [44,45]. It also remains the leading cause of cancer mortality among Mozambican women [20,45]. High-risk (hr) HPV (persistent) infection is well known as prerequisite factor for the modification of the squamous epithelium and progression to premalignant lesions and CC over time [5,7,8].
This study provides important insights into the epidemiology of hrHPV infection and cervical premalignant lesions among women in Mozambique, with particular focus on its age-specific distribution and the associated risk factors, by HIV status. Our findings highlight critical epidemiological patterns that can inform prevention strategies, including screening, integration with HIV services and vaccination.
The mean age of participants (43.0 ± 8.6 years) reflects the typical profile of women attending screening in Mozambique and other sub-Saharan African and worldwide countries, where uptake peaks in mid-adult life [35,46,47,48]. Nearly three-quarters of women were undergoing screening for the first time, pointing to major gaps in awareness and access. This is consistent with earlier studies in Maputo and Nampula, where first-time screening rates exceeded 60% [22,23]. Such low coverage continues to undermine timely prevention [46,47].
The overall hrHPV prevalence of 28% aligns with prior studies from Mozambique, which reported values between 20% and 75.9% depending on HIV status and age [21,22,23,24,25,49]. Comparable prevalence has been described in sub-Saharan African countries [13], including Nigeria, Rwanda, and Burkina Faso [50,51,52]. Unlike high-income settings, where hrHPV prevalence declines after age 30 [53,54], our data show higher positivity in older ages, particularly 30–45 and ≥46 years. This supports evidence that HPV is more frequent in African women, influenced by HIV, reproductive history, and limited access to continuous screening [54,55,56].
HIV was strongly associated with hrHPV infection. HIV-positive [+] women had higher hrHPV prevalence (31.8%) and more frequent multiple infections than HIV-negative [−] counterparts. The crude odds of hrHPV infection were higher in HIV-positive women (OR = 1.99; 95% CI: 1.0–3.9), although this association did not reach statistical significance (p = 0.082). These findings are consistent with systematic reviews in Sub-Saharan Africa reporting higher pooled prevalence of any HPV or hrHPV/multiple infections among HIV [+] women, compared to HIV [−] women; OR = 4.68 (0.71–30.76) [13] and, OR = 3.22 (3.00–3.42) and OR = 3.71 (2.39–5.75), p < 0.001, respectively [12]. Other studies from Mozambique, Zimbabwe, and Kenya also reported that HIV coinfection was linked to broader hrHPV type distribution and reduced viral clearance [56,57,58].
Although HPV-16 and 18 remain oncogenically important, non-16/18 hrHPV types predominated in both groups, especially among HIV [+] women, and were concentrated in women of reproductive and early peri-menopausal age. These patterns mirror findings from African cohorts [13], including Maputo–Mozambique [14,21,23,58] and Burkina Faso [52], underscoring the need for screening and vaccination strategies beyond HPV-16/18. Vaccines targeting only HPV-16/18 may provide partial/limited preventive protection to CC, whereas the nonavalent vaccine could offer broader coverage, although access remains limited. The borderline difference in hrHPV prevalence between HIV [+] and HIV [−] women may reflect sample size constraints and suggests that additional factors—such as reproductive history, genital tract inflammation, and sexual behavior—play an important role in infection risk.
Among the factors assessed, age was associated with hrHPV infection. Logistic regression indicated that each additional year of age slightly reduced the odds of hrHPV, with a stronger effect observed in HIV-negative women. This aligns with findings from several sub-Saharan African countries [13], including South Africa and Nigeria [50,59], where hrHPV declined after midlife, likely reflecting cumulative immune clearance. Conversely, HIV [+] women may sustain hrHPV well into older ages due to immunosuppression and coinfections, underlining the need for differentiated screening strategies.
Reproductive history also influenced hrHPV prevalence. Nulligravida women and those with 1–2 deliveries had higher hrHPV positivity, whereas women with three or more deliveries showed lower odds of infection. This partly contrasts with global data linking high parity to CC [60]. Similar paradoxical findings in Rwanda [51] and Brazil [61] suggest that immune adaptations during multiple pregnancies may enhance viral clearance. Understanding these mechanisms will require more detailed longitudinal studies.
VIA results add further perspective. Overall, 11.1% of women were VIA-positive [+], with slightly higher prevalence among HIV [+] women (11.3% vs. 8.9%). Larger lesions (≥75% of the cervix) were also more frequent in HIV [+] women. These findings are consistent with reports from other African countries, where HIV infection is recognized as an important factor associated with VIA positivity [56] and CC, with an attributable fraction of 20.4% (vs. 1.3% and 1.1%, respectively, in the rest of the world) [60]. Yet, logistic regression revealed that contraceptive use was associated with higher odds of VIA positivity, particularly among HIV [−] women, while parity and prior STI history were not significant predictors. This contrasts with studies from Nigeria and Burkina Faso, where contraceptive use was not significantly associated with hrHPV infection [52,55], and with an Ethiopian study identifying high parity and a history of STIs as associated with VIA positivity (adjusted OR = 2.1, 95% CI: 1.3–4.0; adjusted OR = 1.9, 95% CI: 1.1–3.5, respectively) [62]. Possible explanations include hormonal influences on cervical epithelium or residual confounding by sexual behavior in our sample. Importantly, VIA positivity was strongly associated with poor SCJ visibility, especially in HIV [+] women, confirming that VIA performance declines when the transformation zone is not fully visible [14,63]. This reinforces WHO recommendations to prioritize HPV DNA testing, with VIA limited to triage where feasible.
Our findings on HPV type distribution highlight a regional pattern. HPV-16 and 18 were detected in 9.4% and 5.6% of HIV [+] women, respectively, compared with 3.6% and 2.0% in HIV [−] women. Although modest, these rates are clinically relevant, as HPV-16 and 18 account for most CC cases globally [14]. However, the predominance of other hrHPV types indicates that current vaccines alone will not eliminate CC in Mozambique. Expanded use of the nonavalent vaccine could further increase coverage against the spectrum of circulating hrHPV types.
Behavioral characteristics also influenced observed associations. The mean sexual debut age (17.5 years) and high multiparity reflect sociocultural patterns consistent with other studies from Africa and Mozambique [13,21,22,50]. Earlier sexual debut increases lifetime exposure to HPV [1], while genital tract abnormalities were more frequent in hrHPV-positive women, suggesting that local inflammation and STIs may facilitate persistence [41,64]. Notably, smoking—a key risk factor in other regions [48,65]—was virtually absent in our cohort, limiting its contribution. This underscores the context-specific nature of HPV epidemiology in Africa.
This study contributes to understanding the interplay of HIV, hrHPV, and cervical lesions in a high-burden setting. While our cross-sectional design limits causal inference, the findings reinforce that HIV [+] women are disproportionately affected by hrHPV and cervical abnormalities, especially from non-16/18 types. VIA alone may be inadequate for this group, given anatomical and immunological challenges. Broader vaccine coverage, HPV testing, and integrated HIV–HPV strategies are urgently needed. If scaled up effectively, these interventions could accelerate progress toward WHO’s CC elimination targets in Mozambique and similar settings.
5. Conclusions
This study revealed a 28% prevalence of high-risk HPV (hrHPV) among women in Maputo, with higher rates and multiple infections in HIV-positive [+] participants. Non-16/18 hrHPV types predominated across all ages, particularly among women aged 30–45 years. Younger age, lower parity, and HIV infection were key factors associated with hrHPV positivity, while older age and higher parity showed protective effects. VIA-positive [+] lesions were more frequent in younger and HIV [+] women.
Author Contributions
A.S. and C.N. conceived the idea and had a full role in the conceptualization and design of the study, formal analysis, draft writing, and revision of the manuscript. N.C., C.M. and J.S. (Júlia Sebastião) participated in the selection of study population, collection of clinical materials, gynecological examination, and patient care. J.S. (Júlia Sebastião) and Z.S. carried out HPV genotyping analyses. S.C., F.C., J.S. (Jahit Sacarlal) and M.C.B. participated in the draft writing, analysis of the results, and revision of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Mozambican National ethical committee (ref. 688/CNBS/20) (approval date: 2 December 2020) and from the Institutional Health Bioethics Committee of the Faculty of Medicine, Eduardo Mondlane University, and Maputo Central Hospital (ref. CIBS FM&HCM/019/2023) (approval date: 26 March 2024).
Informed Consent Statement
Informed consent was obtained from all participants involved in the study.
Data Availability Statement
The data that support the findings made in this study can be made available from the corresponding author, A.S., on request.
Acknowledgments
The co-authors played an invaluable role in the completion of this work. We thank the patients, nurses, and other DREAM Program staff in Mozambique who participated in the HPV-ISI study, as well as the DREAM Program administration for allowing the use of the data for this study. During the preparation of this manuscript, the authors used Grammarly version 14.1256.0 for spelling revision.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Bruni, L.; Diaz, M.; Castellsagué, X.; Ferrer, E.; Bosch, F.X.; De Sanjosé, S. Cervical human papillomavirus prevalence in 5 continents: Meta-analysis of 1 million women with normal cytological findings. J. Infect. Dis. 2010, 202, 1789–1799. [Google Scholar] [CrossRef]
- Bruni, L.; Albero, G.; Serrano, B.; Mena, M.; Collado, J.J.; Gómez, D.; Muñoz, J.; Bosch, F.X.; de Sanjosé, S. ICO/IARC Information Centre on HPV and Cancer (HPV Information Centre). Human Papillomavirus and Related Diseases in the World. Summary Report. 2023. Available online: https://hpvcentre.net/statistics/reports/XWX.pdf (accessed on 9 May 2025).
- Lekoane, B.K.M.; Mashamba-Thompson, T.P.; Ginindza, T.G. Mapping evidence on the distribution of human papillomavirus-related cancers in sub-Saharan Africa: Scoping review protocol. Syst. Rev. 2017, 6, 229. [Google Scholar] [CrossRef] [PubMed]
- Mboumba Bouassa, R.S.; Prazuck, T.; Lethu, T.; Jenabian, M.A.; Meye, J.F.; Bélec, L. Cervical cancer in sub-Saharan Africa: A preventable noncommunicable disease. Expert. Rev. Anti Infect. Ther. 2017, 15, 613–627. [Google Scholar] [CrossRef] [PubMed]
- de Martel, C.; Plummer, M.; Vignat, J.; Franceschi, S. Worldwide burden of cancer attributable to HPV by site, country and HPV type. Int. J. Cancer 2017, 141, 664–670. [Google Scholar] [CrossRef] [PubMed]
- Chesson, H.W.; Dunne, E.F.; Hariri, S.; Markowitz, L.E. The estimated lifetime probability of acquiring human papillomavirus in the United States. Sex. Transm. Dis. 2014, 41, 660–664. [Google Scholar] [CrossRef]
- Sudenga, S.L.; Shrestha, S. Key considerations and current perspectives of epidemiological studies on human papillomavirus persistence, the intermediate phenotype to cervical cancer. Int. J. Infect. Dis. 2013, 17, e216–e220. [Google Scholar] [CrossRef]
- Walboomers, J.M.M.; Jacobs, M.V.; Manos, M.M.; Bosch, F.X.; Kummer, J.A.; Shah, K.V.; Snijders, P.J.; Peto, J.; Meijer, C.J.; Muñoz, N. Human papillomavirus is a necessary cause of invasive cervical cancer worldwide. J. Pathol. 1999, 189, 12–19. [Google Scholar] [CrossRef]
- Muñoz, N.; Bosch, F.X.; de Sanjosé, S.; Herrero, R.; Castellsagué, X.; Shah, K.V.; Snijders, P.J.; Meijer, C.J.; International Agency for Research on Cancer Multicenter Cervical Cancer Study Group. Epidemiologic Classification of Human Papillomavirus Types Associated with Cervical Cancer. N. Engl. J. Med. 2003, 348, 518–527. [Google Scholar] [CrossRef]
- Arbyn, M.; Tommasino, M.; Depuydt, C.; Dillner, J. Are 20 human papillomavirus types causing cervical cancer? J. Pathol. 2014, 234, 431–435. [Google Scholar] [CrossRef]
- Stelzle, D.; Tanaka, L.F.; Lee, K.K.; Ibrahim Khalil, A.; Baussano, I.; Shah, A.S.V.; McAllister, D.A.; Gottlieb, S.L.; Klug, S.J.; Winkler, A.S.; et al. Estimates of the global burden of cervical cancer associated with HIV. Lancet Glob. Health 2021, 9, e161–e169. [Google Scholar] [CrossRef]
- Okoye, J.O.; Ofodile, C.A.; Adeleke, O.K.; Obioma, O. Prevalence of high-risk HPV genotypes in sub-Saharan Africa according to HIV status: A 20-year systematic review. Epidemiol. Health 2021, 43, e2021039. [Google Scholar] [CrossRef]
- Tchouaket, M.C.T.; Ka’e, A.C.; Semengue, E.N.J.; Sosso, S.M.; Simo, R.K.; Yagai, B.; Nka, A.D.; Chenwi, C.A.; Abba, A.; Fainguem, N.; et al. Variability of High-Risk Human Papillomavirus and Associated Factors among Women in Sub-Saharan Africa: A Systematic Review and Meta-Analysis. Pathogens 2023, 12, 1032. [Google Scholar] [CrossRef] [PubMed]
- Castellsagué, X. Natural history and epidemiology of HPV infection and cervical cancer. Gynecol. Oncol. 2008, 110, S4–S7. [Google Scholar] [CrossRef]
- Panatto, D.; Amicizia, D.; Trucchi, C.; Casabona, F.; Lai, P.L.; Bonanni, P.; Boccalini, S.; Bechini, A.; Tiscione, E.; Zotti, C.M.; et al. Sexual behaviour and risk factors for the acquisition of human papillomavirus infections in young people in Italy: Suggestions for future vaccination policies. BMC Public Health 2012, 12, 623. [Google Scholar] [CrossRef] [PubMed]
- Schiffman, M.; Wentzensen, N. Human Papillomavirus Infection and the Multistage Carcinogenesis of Cervical Cancer. Cancer Epidemiol. Biomark. Prev. 2013, 22, 553–560. [Google Scholar] [CrossRef]
- Lee, M.; Park, E.C.; Chang, H.S.; Kwon, J.A.; Yoo, K.B.; Kim, T.H. Socioeconomic disparity in cervical cancer screening among Korean women: 1998–2010. BMC Public Health 2013, 13, 553. [Google Scholar] [CrossRef]
- Broberg, G.; Wang, J.; Östberg, A.L.; Adolfsson, A.; Nemes, S.; Sparén, P.; Strander, B. Socio-economic and demographic determinants affecting participation in the Swedish cervical screening program: A population-based case-control study. PLoS ONE 2018, 13, e0190171. [Google Scholar] [CrossRef]
- Akinyemiju, T.; Ogunsina, K.; Sakhuja, S.; Ogbhodo, V.; Braithwaite, D. Life-course socioeconomic status and breast and cervical cancer screening: Analysis of the WHO’s Study on Global Ageing and Adult Health (SAGE). BMJ Open 2016, 6, e012753. [Google Scholar] [CrossRef]
- Bruni, L.; Albero, G.; Serrano, B.; Mena, M.; Collado, J.J.; Gómez, D.; Muñoz, J.; Bosch, F.X.; de Sanjosé, S. ICO/IARC Information Centre on HPV and Cancer (HPV Information Centre). Human Papillomavirus and Related Diseases in Mozambique. Summary Report. 2023. Available online: https://hpvcentre.net/statistics/reports/MOZ.pdf (accessed on 9 May 2025).
- Edna Omar, V.; Orvalho, A.; Nália, I.; Kaliff, M.; Lillsunde-Larsson, G.; Ramqvist, T.; Nilsson, C.; Falk, K.; Nafissa, O.; Ilesh Vindorai, J.; et al. Human papillomavirus prevalence and genotype distribution among young women and men in Maputo city, Mozambique. BMJ Open 2017, 7, e015653. [Google Scholar] [CrossRef] [PubMed]
- Bule, Y.P.; Silva, J.; Carrilho, C.; Campos, C.; Sousa, H.; Tavares, A.; Medeiros, R. Human papillomavirus prevalence and distribution in self-collected samples from female university students in Maputo. Int. J. Gynecol. Obstet. 2020, 149, 237–246. [Google Scholar] [CrossRef]
- Maueia, C.; Murahwa, A.; Manjate, A.; Andersson, S.; Sacarlal, J.; Kenga, D.; Mussá, T.; Williamson, A.L. Identification of the human papillomavirus genotypes, according to the human immunodeficiency virus status in a cohort of women from maputo, Mozambique. Viruses 2022, 14, 24. [Google Scholar] [CrossRef] [PubMed]
- Salcedo, M.P.; Oliveira, C.; Andrade, V.; Mariano, A.A.N.; Changule, D.; Rangeiro, R.; Monteiro, E.C.S.; Baker, E.; Phoolcharoen, N.; Varon, M.L.; et al. The Capulana study: A prospective evaluation of cervical cancer screening using human papillomavirus testing in Mozambique. Int. J. Gynecol. Cancer 2020, 30, 1292–1297. [Google Scholar] [CrossRef]
- Salcedo, M.P.; Lathrop, E.; Osman, N.; Neves, A.; Rangeiro, R.; Mariano, A.A.N.; Nkundabatware, J.C.; Tivir, G.; Carrilho, C.; Monteiro, E.C.S.; et al. The Mulher Study: Cervical cancer screening with primary HPV testing in Mozambique. Int. J. Gynecol. Cancer 2023, 33, 1869–1874. [Google Scholar] [CrossRef]
- Sineque, A.; Catalao, C.; Ceffa, S.; Fonseca, A.M.; Parruque, F.; Guidotti, G.; Massango, C.; Carrilho, C.; Bicho, C.; Rangeiro, R.; et al. Screening approaches for cervical cancer in Mozambique in HIV positive and negative women. Eur. J. Cancer Prev. 2023, 32, 431–437. [Google Scholar] [CrossRef]
- Carrilho, C.; Fontes, F.; Tulsidás, S.; Lorenzoni, C.; Ferro, J.; Brandão, M.; Ferro, A.; Lunet, N. Cancer incidence in Mozambique in 2015–2016: Data from the Maputo Central Hospital Cancer Registry. Eur. J. Cancer Prev. 2019, 28, 373–376. [Google Scholar] [CrossRef]
- Batman, S.; Rangeiro, R.; Monteiro, E.; Changule, D.; Daud, S.; Ribeiro, M.; Tsambe, E.; Bila, C.; Osman, N.; Carrilho, C.; et al. Expanding Cervical Cancer Screening in Mozambique: Challenges Associated with Diagnosing and Treating Cervical Cancer. JCO Glob. Oncol. 2023, 9, e2300139. [Google Scholar] [CrossRef] [PubMed]
- Naucler, P.; Mabota da Costa, F.; da Costa, J.L.; Ljungberg, O.; Bugalho, A.; Dillner, J. Human papillomavirus type-specific risk of cervical cancer in a population with high human immunodeficiency virus prevalence: Case–control study. J. Gen. Virol. 2011, 92, 2784–2791. [Google Scholar] [CrossRef]
- Boothe, M.A.S.; Sathane, I.; Baltazar, C.S.; Chicuecue, N.; Horth, R.; Fazito, E.; Raymond, H.F. Low engagement in HIV services and progress through the treatment cascade among key populations living with HIV in Mozambique: Alarming gaps in knowledge of status. BMC Public Health 2021, 21, 146. [Google Scholar] [CrossRef]
- INS—Instituto Nacional de Saúde. Inquérito Nacional sobre o Impacto do HIV e SIDA (INSIDA 2021): Relatório Final. Maputo. 2023. Available online: http://ins.gov.mz (accessed on 4 October 2025).
- Brandão, M.; Tulsidás, S.; Damasceno, A.; Silva-Matos, C.; Carrilho, C.; Lunet, N. Cervical cancer screening uptake in women aged between 15 and 64 years in Mozambique. Eur. J. Cancer Prev. 2019, 28, 338–343. [Google Scholar] [CrossRef]
- WHO. WHO Guideline for Screening and Treatment of Cervical Pre-Cancer Lesions for Cervical Cancer Prevention, 2nd ed.; World Health Organization: Geneva, Switzerland, 2021; pp. 1–115. [Google Scholar]
- Golia D’Augè, T.; Giannini, A.; Bogani, G.; Di Dio, C.; Laganà, A.S.; Di Donato, V.; Salerno, M.G.; Caserta, D.; Chiantera, V.; Vizza, E.; et al. Prevention, Screening, Treatment and Follow-Up of Gynecological Cancers: State of Art and Future Perspectives. Clin. Exp. Obs. Gynecol. 2023, 50, 160. [Google Scholar] [CrossRef]
- Adams, R.; Botha, M. Cervical cancer prevention in Southern Africa: A review of national cervical cancer screening guidelines in the Southern African development community. J. Cancer Policy. 2024, 40, 100477. [Google Scholar] [CrossRef]
- Correia, D.; Bay, Z.; Wate, A.; Nhanguiombe, H.; Manhica, P.; Bila, E.; Tualufo, S.; Mate, C.; Amado, C.; Lorenzoni, C. Scaling-up Cervical Cancer Services for Women Living with HIV in Mozambique, October 2018–September 2023. 2024. Available online: https://www.medrxiv.org/content/10.1101/2024.11.21.24317677v1 (accessed on 4 November 2025).
- Sant’Egidio Community. Drug Resource Enhancement Against AIDS and Malnutrition—DREAM: Report. Rome. 2011. Available online: https://www.santegidiomadrid.org/wp-content/uploads/2011/03/201103_ReportEN_.pdf (accessed on 1 November 2025).
- DREAM Program. The Disease Relief Through Excellent and Advanced Means (DREAM) Program in Sub-Saharan Africa. Available online: https://www.dream-health.org/?lang=en (accessed on 1 November 2025).
- Leone, M.; Palombi, L.; Guidotti, G.; Ciccacci, F.; Lunghi, R.; Orlando, S.; Nurja, M.A.; Sangare, M.H.; Marazzi, C.M. What headache services in sub-Saharan Africa? The DREAM program as possible model. Cephalalgia 2019, 39, 1339–1340. [Google Scholar] [CrossRef]
- Lio, M.M.S.; Marchetti, I.; Carrilho, C.; Cioni, M.P.; Guidotti, G.; Moscatelli, C.; Taponeco, F.; Walle, E.S.F.; Zimba, I.; Bevilacqua, G. Human papillomavirus (HPV) genotypes among HIV-infected and HIV-uninfected women in Mozambique. Retrovirology 2010, 7, P2. [Google Scholar] [CrossRef]
- Sineque, A.; Ceffa, S.; Parruque, F.; Guidotti, G.; Massango, C.; Sidumo, Z.; Carrilho, C.; Bicho, C.; Rangeiro, R.; Orlando, S.; et al. Impact of STIs on cervical cancer screening: Prevalence of Chlamydia trachomatis and Neisseria gonorrhoeae in visual inspection with acetic acid (VIA) positive women in Mozambique. Int. J. STD AIDS 2024, 35, 1019–1024. [Google Scholar] [CrossRef] [PubMed]
- MISAU. Plano Nacional de Controlo do Cancro 2019–2029; Ministry of Health—MISAU: Maputo, Mozambique, 2019. [Google Scholar]
- Cunha, M.; Matos, C.S.; MISAU. Normas Nacionais para Prevenção do Cancro do Colo Uterino. Maputo. Available online: https://www.iccp-portal.org (accessed on 4 October 2025).
- Bray, F.; Laversanne, M.; Sung, H.; Ferlay, J.; Siegel, R.L.; Soerjomataram, I.; Jemal, A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2024, 74, 229–263. [Google Scholar] [CrossRef]
- Globocan. The Global Cancer Observatory: Fact Sheet—Mozambique. 2024. Available online: https://gco.iarc.who.int/media/globocan/factsheets/populations/508-mozambique-fact-sheet.pdf (accessed on 4 October 2025).
- IARC—The International Agency for Research on Cancer. Cervical Cancer Screening Programme in Five Continents (CanScreen5): Country Fact Sheets. 2020. Available online: https://canscreen5.iarc.fr/?page=countryfactsheetcervix&q=MOZ&rc= (accessed on 4 October 2025).
- Tulsidás, S.; Fontes, F.; Brandão, M.; Lunet, N.; Carrilho, C. Oncology in Mozambique: Overview of the Diagnostic, Treatment, and Research Capacity. Cancers 2023, 15, 1163. [Google Scholar] [CrossRef] [PubMed]
- Saldaña-Rodríguez, P.; Bahena-Román, M.; Delgado-Romero, K.; Madrid-Marina, V.; Torres-Poveda, K. Prevalence and Risk Factors for High-Risk Human Papillomavirus Infection and Cervical Disorders: Baseline Findings from an Human Papillomavirus Cohort Study. Cancer Control 2023, 30, 10732748231202925. [Google Scholar] [CrossRef] [PubMed]
- Pizzol, D.; Putoto, G.; Chhaganlal, K.D. Human papillomavirus (HPV) infection: A Mozambique overview. VirusDisease 2016, 27, 116–122. [Google Scholar] [CrossRef]
- Okunade, K.S.; Nwogu, C.M.; Oluwole, A.A.; Anorlu, R.I. Prevalence and risk factors for genital high-risk human papillomavirus infection among women attending the outpatient clinics of a university teaching hospital in Lagos, Nigeria. Pan Afr. Med. J. 2017, 28, 227. [Google Scholar] [CrossRef]
- Sinayobye, J.D.A.; Sklar, M.; Hoover, D.R.; Shi, Q.; Dusingize, J.C.; Cohen, M.; Mutimura, E.; Asiimwe-Kateera, B.; Castle, P.E.; Strickler, H.; et al. Prevalence and risk factors for High-Risk Human Papillomavirus (hrHPV) infection among HIV-infected and Uninfected Rwandan women: Implications for hrHPV-based screening in Rwanda. Infect. Agent. Cancer 2014, 9, 40. [Google Scholar] [CrossRef]
- Zabre, P.; Sagna, T.; Ouedraogo, R.; Simpore, J. Epidemiological profile of human papillomavirus infections and cervical cancer prevention among sexually active women in Burkina Faso: Literature Review. Med. Res. Arch. 2024, 12, 5883. [Google Scholar] [CrossRef]
- Clarke, M.A.; Risley, C.; Stewart, M.W.; Geisinger, K.R.; Hiser, L.M.; Morgan, J.C.; Owens, K.J.; Ayyalasomayajula, K.; Rives, R.M.; Jannela, A.; et al. Age-specific prevalence of human papillomavirus and abnormal cytology at baseline in a diverse statewide prospective cohort of individuals undergoing cervical cancer screening in Mississippi. Cancer Med. 2021, 10, 8641–8650. [Google Scholar] [CrossRef]
- Osmani, V.; Hörner, L.; Nkurunziza, T.; Rank, S.; Tanaka, L.F.; Klug, S.J. Global prevalence of cervical human papillomavirus in women aged 50 years and older with normal cytology: A systematic review and meta-analysis. Lancet Microbe 2025, 6, 100955. [Google Scholar] [CrossRef] [PubMed]
- Magaji, S.; Aminu, M.; Inabo, H.; Oguntayo, A. Spectrum of high-risk human papillomavirus types in women in Kaduna State, Nigeria. Ann. Afr. Med. 2019, 18, 30–35. [Google Scholar] [CrossRef]
- Kangethe, J.M.; Gichuhi, S.; Odari, E.; Pintye, J.; Mutai, K.; Abdullahi, L.; Maiyo, A.; Mureithi, M.W. Confronting the human papillomavirus–HIV intersection: Cervical cytology implications for Kenyan women living with HIV. S. Afr. J. HIV Med. 2023, 24, 1508. [Google Scholar] [CrossRef]
- Kufa, T.; Mandiriri, A.; Shamu, T.; Dube Mandishora, R.S.; Pascoe, M.J. Prevalence of cervical high-risk human papillomavirus among Zimbabwean women living with HIV. S. Afr. J. HIV Med. 2024, 25, 1633. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, C.M.; Rangeiro, R.; Osman, N.; Baker, E.; Neves, A.; Mariano, A.A.N.; Tivir, G.; Thomas, J.P.; Carns, J.; Andrade, V.; et al. Evaluation of HPV risk groups among women enrolled in the mulher cervical cancer screening study in Mozambique. Infect. Agent. Cancer 2025, 20, 24. [Google Scholar] [CrossRef]
- Tiiti, T.A.; Selabe, S.G.; Bogers, J.; Lebelo, R.L. High prevalence of and factors associated with human papillomavirus infection among women attending a tertiary hospital in Gauteng Province, South Africa. BMC Cancer 2022, 22, 854. [Google Scholar] [CrossRef]
- Ibrahim Khalil, A.; Mpunga, T.; Wei, F.; Baussano, I.; de Martel, C.; Bray, F.; Stelzle, D.; Dryden-Peterson, S.; Jaquet, A.; Horner, M.J.; et al. Age-specific burden of cervical cancer associated with HIV: A global analysis with a focus on sub-Saharan Africa. Int. J. Cancer 2022, 150, 761–772. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues De Oliveira, V.; Vieira, V.C.; Barral, M.F.M.; Döwich, V.; Soares, M.A.; Conçalves, C.V.; Martinez, A.M.B.D. Risk factors and prevalence of HPV infection in patients from Basic Health Units of an University Hospital in southern Brazil Palavras-chave. Rev. Bras. Ginecol. Obs. 2013, 35, 226–232. [Google Scholar]
- Tekalegn, Y.; Aman, R.; Woldeyohannes, D.; Sahiledengle, B.; Degno, S. Determinants of VIA Positivity Among Women Screened for Cervical Precancerous Lesion in Public Hospitals of Oromia Region, Ethiopia: Unmatched Case-Control Study. Int. J. Womens Health 2020, 12, 587–596. [Google Scholar] [CrossRef] [PubMed]
- Desai, V.B.; Wright, J.D.; Gross, C.P.; Lin, H.; Boscoe, F.P.; Hutchison, L.M.; Schwartz, P.E.; Xu, X. Prevalence, characteristics, and risk factors of occult uterine cancer in presumed benign hysterectomy. Am. J. Obs. Gynecol. 2019, 221, 39.e1–39.e14. [Google Scholar] [CrossRef]
- Maueia, C.; Murahwa, A.; Manjate, A.; Sacarlal, J.; Kenga, D.; Unemo, M.; Andersson, S.; Mussá, T.; Williamson, A.L. The relationship between selected sexually transmitted pathogens, HPV and HIV infection status in women presenting with gynaecological symptoms in Maputo City, Mozambique. PLoS ONE 2024, 19, e0307781. [Google Scholar] [CrossRef] [PubMed]
- Yang, D.; Zhang, J.; Cui, X.; Ma, J.; Wang, C.; Piao, H. Status and epidemiological characteristics of high-risk human papillomavirus infection in multiple centers in Shenyang. Front. Microbiol. 2022, 13, 985561. [Google Scholar] [CrossRef] [PubMed]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.