
The Budget Impact of Adopting Oral Pre-Exposure Prophylaxis for HIV Prevention: A Rapid Review

 ,
,  , , and
, , and
Abstract
1. Introduction
2. Methodology
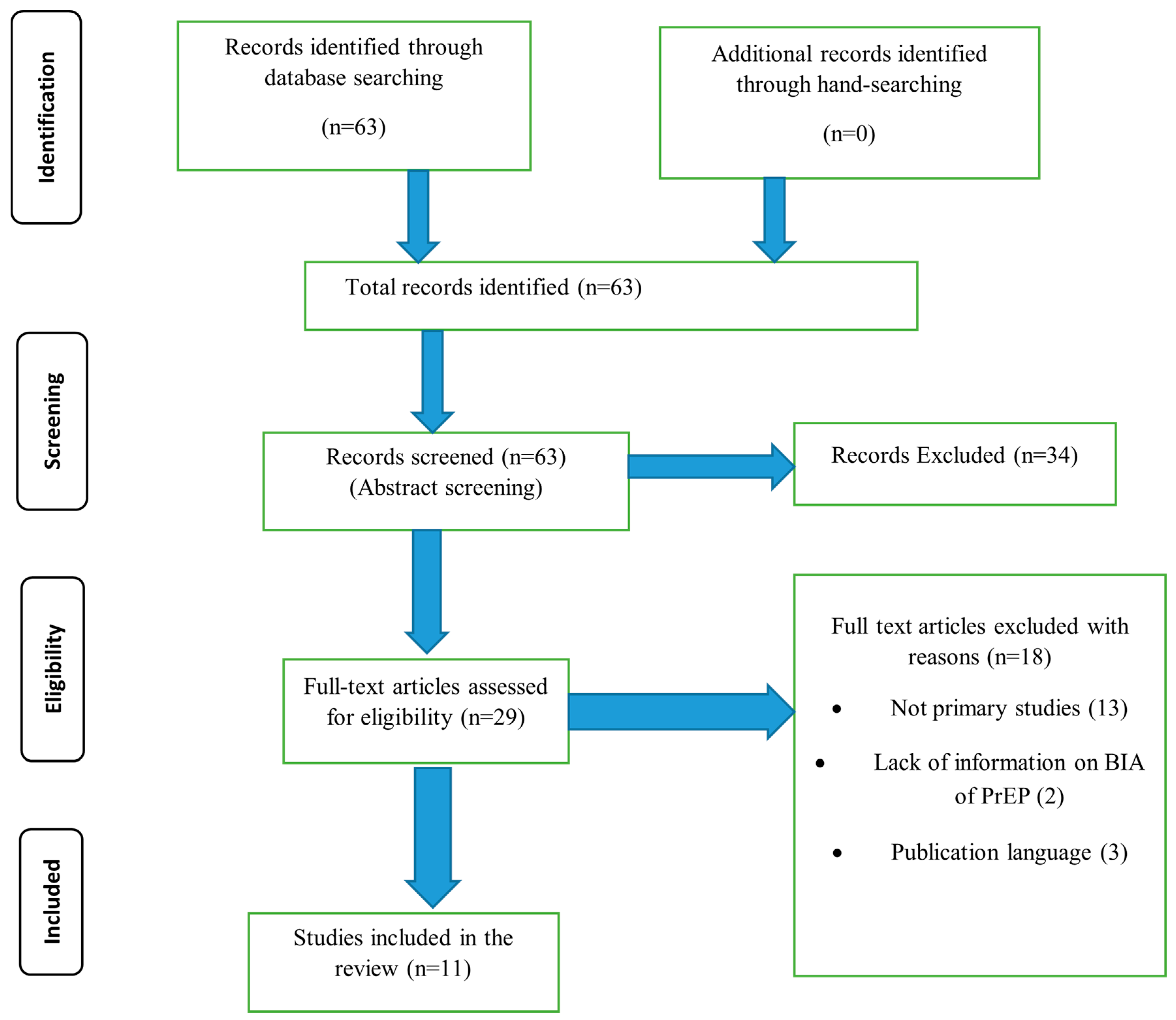
2.1. Information Sources and Literature Search
2.2. Participants
2.3. Study Selection and Inclusion Criteria
2.4. Screening and Data Abstraction Process
2.5. Quality of the Selected Studies
2.6. Data Synthesis
3. Results
3.1. Characteristics of the Included Studies
3.2. Study Findings
3.2.1. Study Perspective
3.2.2. Target Population
3.2.3. Time Horizon
3.2.4. Costing and Resource Utilisation
3.2.5. Sensitivity Analysis
3.2.6. Discounting
3.2.7. Summary of Conclusions from the Studies
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- The Joint United Nations Programme on HIV/AIDS (UNAIDS). The Path That Ends AIDS: Unaids Global AIDS Update 2023. 2023. Available online: https://www.unaids.org/en/resources/documents/2023/global-aids-update-2023 (accessed on 5 October 2023).
- WHO. Consolidated Guidelines on HIV Prevention, Diagnosis, and Care for Key Populations. 2016. Available online: http://apps.who.int/iris/bitstream/handle/10665/246200/9789241511124-eng.pdf?sequence=8 (accessed on 10 September 2023).
- Bekker, L.G.; Beyrer, C.; Quinn, T.C. Behavioral and Biomedical Combination Strategies for HIV Prevention. Cold Spring Harb. Perspect. Med. 2012, 2, a007435. [Google Scholar] [CrossRef]
- Sipe, T.A.; Barham, T.L.; Johnson, W.D.; Joseph, H.A.; Tungol-Ashmon, M.L.; O’leary, A. Structural Interventions in HIV Prevention: A Taxonomy and Descriptive Systematic Review. AIDS Behav. 2017, 21, 3366–3430. [Google Scholar] [CrossRef]
- Hodges-Mameletzis, I.; Dalal, S.; Msimanga-Radebe, B.; Rodolph, M.; Baggaley, R. Going global: The adoption of the World Health Organization’s enabling recommendation on oral pre-exposure prophylaxis for HIV. Sex Health 2018, 15, 489–500. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global PrEP Network Highlight-March 2021. 2021. Available online: https://www.who.int/news-room/feature-stories/detail/global-data-shows-increasing-prep-use-and-widespread-adoption-of-who-prep-recommendations (accessed on 26 December 2024).
- Pretorius, C.; Schnure, M.; Dent, J.; Glaubius, R.; Mahiane, G.; Hamilton, M.; Reidy, M.; Matse, S.; Njeuhmeli, E.; Castor, D.; et al. Modelling impact and cost-effectiveness of oral pre-exposure prophylaxis in 13 low-resource countries. J. Int. AIDS Soc. 2020, 23, e25451. [Google Scholar] [CrossRef] [PubMed]
- Leelahavarong, P. Budget impact analysis. J. Med. Assoc. Thail. 2014, 97 (Suppl. S5), S65–S71. [Google Scholar]
- Garattini, L.; van de Vooren, K. Budget impact analysis in economic evaluation: A proposal for a clearer definition. Eur. J. Health Econ. 2011, 12, 499–502. [Google Scholar] [CrossRef]
- Carvalho, N.; Jit, M.; Cox, S.; Yoong, J.; Hutubessy, R.C.W. Capturing Budget Impact Considerations Within Economic Evaluations: A Systematic Review of Economic Evaluations of Rotavirus Vaccine in Low- and Middle-Income Countries and a Proposed Assessment Framework. Pharmacoeconomics 2018, 36, 79–90. [Google Scholar] [CrossRef]
- van de Vijver, D.A.M.C.; Richter, A.-K.; Boucher, C.A.B.; Gunsenheimer-Bartmeyer, B.; Kollan, C.; E Nichols, B.; Spinner, C.D.; Wasem, J.; Schewe, K.; Neumann, A. Cost-effectiveness and budget effect of pre-exposure prophylaxis for HIV-1 prevention in Germany from 2018 to 2058. Eurosurveillance 2019, 24, 1800398. [Google Scholar] [PubMed]
- Vermeersch, S.; Callens, S.; De Wit, S.; Goffard, J.-C.; Laga, M.; Van Beckhoven, D.; Annemans, L. Health and budget impact of combined HIV prevention—First results of the BELHIVPREV model. Acta Clin. Belg. 2018, 73, 54–67. [Google Scholar] [CrossRef] [PubMed]
- Cambiano, V.; Miners, A.; Dunn, D.; McCormack, S.; Ong, K.J.; Gill, O.N.; Nardone, A.; Desai, M.; Field, N.; Hart, G.; et al. Cost-effectiveness of pre-exposure prophylaxis for HIV prevention in men who have sex with men in the UK: A modelling study and health economic evaluation. Lancet Infect. Dis. 2018, 18, 85–94. [Google Scholar] [CrossRef]
- Ong, K.J.; Desai, S.; Field, N.; Desai, M.; Nardone, A.; van Hoek, A.J.; Gill, O.N. Economic evaluation of HIV pre-exposure prophylaxis among men-who-have-sex-with-men in England in 2016. Eurosurveillance 2017, 22, 15–24. [Google Scholar] [CrossRef]
- Alvis-Zakzuk, N.; Tolosa-Pérez, N.; Buitrago, G.; Moreno, C.A.; Sotomayor, M.C.; De La Hoz, F. Budget impact of pre-exposure prophylaxis (PrEP) strategy for the prevention of HIV in Colombia, 2019–2020. Value Health 2020, 23 (Suppl. S1), S174. [Google Scholar]
- Kazemian, P.; Costantini, S.; Kumarasamy, N.; Paltiel, A.D.; Mayer, K.H.; Chandhiok, N.; Walensky, R.P.; A Freedberg, K. The Cost-effectiveness of Human Immunodeficiency Virus (HIV) Preexposure Prophylaxis and HIV Testing Strategies in High-risk Groups in India. Clin. Infect. Dis. 2020, 70, 633–642. [Google Scholar] [CrossRef] [PubMed]
- Reyes-Urueña, J.; Campbell, C.; Diez, E.; Ortún, V.; Casabona, J. Can we afford to offer pre-exposure prophylaxis to MSM in Catalonia? Cost-effectiveness analysis and budget impact assessment. AIDS Care 2017, 30, 784–792. [Google Scholar] [CrossRef] [PubMed]
- Walensky, R.P.; Park, J.-E.; Wood, R.; Freedberg, K.A.; Scott, C.A.; Bekker, L.-G.; Losina, E.; Mayer, K.H.; Seage, G.R.; Paltiel, A.D. The Cost-effectiveness of Pre-Exposure Prophylaxis for HIV Infection in South African Women. Clin. Infect. Dis. 2012, 54, 1504–1513. [Google Scholar] [CrossRef]
- Juusola, J.; Brandeau, M.; Owens, D.; Bendavid, E. The Cost-Effectiveness of Preexposure Prophylaxis for HIV Prevention in Men Who Have Sex with Men in the United States. Ann. Intern. Med. 2012, 156, 541–550. [Google Scholar] [CrossRef] [PubMed]
- Schneider, K.; Gray, R.T.; Wilson, D.P. A cost-effectiveness analysis of HIV preexposure prophylaxis for men who have sex with men in Australia. Clin. Infect. Dis. 2014, 58, 1027–1034. [Google Scholar] [CrossRef]
- Moyo, E.; Barham, L.; Mhango, M.; Musuka, G.; Dzinamarira, T. Estimating the budget impact of adopting tenofovir/emtricitabine for pre-exposure prophylaxis of HIV in the public health sector in Namibia (2021–2023). J. Infect. Public Health 2022, 15, 1147–1155. [Google Scholar] [CrossRef] [PubMed]
- Sittimart, M.; Rattanavipapong, W.; Mirelman, A.J.; Hung, T.M.; Dabak, S.; Downey, L.E.; Jit, M.; Teerawattananon, Y.; Turner, H.C. An overview of the perspectives used in health economic evaluations. Cost Eff. Resour. Alloc. 2024, 22, 41. [Google Scholar] [CrossRef] [PubMed]
- Gomez, G.B.; Borquez, A.; Case, K.K.; Wheelock, A.; Vassall, A.; Hankins, C. The Cost and Impact of Scaling Up Pre-exposure Prophylaxis for HIV Prevention: A Systematic Review of Cost-Effectiveness Modelling Studies. PLoS Med. 2013, 10, e1001401. [Google Scholar] [CrossRef]
- Sullivan, S.D.; Mauskopf, J.A.; Augustovski, F.; Caro, J.J.; Lee, K.M.; Minchin, M.; Orlewska, E.; Penna, P.; Barrios, J.-M.R.; Shau, W.-Y. Budget impact analysis-principles of good practice: Report of the ISPOR 2012 Budget Impact Analysis Good Practice II Task Force. Value Health 2014, 17, 5–14. [Google Scholar] [CrossRef] [PubMed]
- Cunnama, L.; Sinanovic, E.; Ramma, L.; Foster, N.; Berrie, L.; Stevens, W.; Molapo, S.; Marokane, P.; McCarthy, K.; Churchyard, G.; et al. Using Top-down and Bottom-up Costing Approaches in LMICs: The Case for Using Both to Assess the Incremental Costs of New Technologies at Scale. Health Econ. 2016, 25 (Suppl. S1), 53–66. [Google Scholar] [CrossRef] [PubMed]
- Potter, S.; Davies, C.; Davies, G.; Rice, C.; Hollingworth, W. The use of micro-costing in economic analyses of surgical interventions: A systematic review. Health Econ Rev. 2020, 10, 3. [Google Scholar] [CrossRef] [PubMed]
- Roberts, D.A.; Barnabas, R.V.; Abuna, F.; Lagat, H.; Kinuthia, J.; Pintye, J.; Bochner, A.F.; Forsythe, S.; Gomez, G.B.; Baeten, J.M.; et al. The role of costing in the introduction and scale-up of HIV pre-exposure prophylaxis: Evidence from integrating PrEP into routine maternal and child health and family planning clinics in western Kenya. J. Int. AIDS Soc. 2019, 22, e25296. [Google Scholar] [CrossRef] [PubMed]
- Attema, A.E.; Brouwer, W.B.F.; Claxton, K. Discounting in Economic Evaluations. Pharmacoeconomics 2018, 36, 745–758. [Google Scholar] [CrossRef]
- Kelley, C.F.; Acevedo-Quiñones, M.; Agwu, A.L.; Avihingsanon, A.; Benson, P.; Blumenthal, J.; Brinson, C.; Brites, C.; Cahn, P.; Cantos, V.D.; et al. Twice-Yearly Lenacapavir for HIV Prevention in Men and Gender-Diverse Persons. N. Engl. J. Med. 2024. online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Yamey, G.; Machingaidze, S. Lenacapavir: A giant step forward in HIV prevention-but a missed opportunity for achieving equity and access. BMJ 2024, 387, q2254. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Reference | van de Vijver et al. (2019) | Vermeersch et al. (2018) | Cambiano et al. (2018) | Ong et al. (2017) | Alvis-Zakzuk et al. (2020) | Kazemianet al. (2020) | Reyes-Uruena et al. (2017) | Walensky et al. (2012) | Juusola et al. (2012) | Schneider et al. (2014) | Moyo et al. (2022) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| [11] | [12] | [13] | [14] | [15] | [16] | [17] | [18] | [19] | [20] | [21] | |
| Perspective given | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Eligible population given | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Current intervention described | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Coverage of PrEP given | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Cost of introducing PrEP | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Time horizon given | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Discounting decision explained | Y | N | Y | Y | N | Y | Y | Y | Y | Y | Y |
| Model Type given | Y | Y | Y | Y | Y | Y | N | Y | Y | Y | Y |
| Data sources provided | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Budget impact calculated | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Validity of model determined | N | Y | N | Y | N | Y | N | N | N | Y | Y |
| Sensitivity analysis performed | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Conclusions and limitations discussed | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Authors | Setting, Perspective and Time Horizon | Methodology | Patient Population | Types of Costs Included | Sensitivity Analysis | Findings |
|---|---|---|---|---|---|---|
| van de Vijver et al. (2019) [11] | Germany, Healthcare payer over 40 years. | CEA and BIA conducted using a Dutch mathematical model with parameter from the Germany HIV epidemic. | MSM. | Annual costs of drugs determined using micro-costing. | Both univariate and multivariate performed. | 1. Cost saving at generic price of PrEP after a period of at least 10 years. 2. Expected to save EUR 5.1 billion in HIV care costs over a 40 year period. 3. Reduction in the price of ART will increase the time for cost savings to be realised. |
| Vermeersch et al. (2018) [12] | Belgium, Pharmaceutical healthcare budget holder over 15 years. | CEA and BIA conducted using a predictive model that estimated the annual number of new HIV diagnosis and the total number of HIV patients in medical follow-up. | Whole population. | Pharmaceutical costs of ART and PrEP. | Univariate performed. | 1. Breakeven situation expected after 10 years. 2. Cost savings expected to range from EUR 1.9 to EUR 33.7 million annually from the 10th year to the 15th year. 3. Impact most sensitive to cost of ART. 4. Even with a 30% increase in ART costs by 2030, annual cost savings of EUR 22 million would be realised. |
| Cambiano et al. (2018) [13] | United Kingdom, Health service provider (NHS) over 80 years. | CEA and BIA performed using dynamic individual-based simulation model calibrated to MSM HIV epidemic. | MSM. | Costs of ART and PrEP drugs, laboratory tests, consultation costs, and counselling costs. | Univariate and probabilistic sensitivity analysis (PSA) performed. | 1. Increase in total HIV care costs for the first 20 years. 2. Budget impact favourable after 20 years of adoption of PrEP. 3. Cost savings of GDP 1 billion on HIV care over the 80 years. |
| Ong et al. (2017) [14] | United Kingdom, Health service provider (NHS) over 10 years. | CEA and BIA performed using a static decision analytic model. | MSM. | Costs of ART and PrEP drugs, laboratory tests, consultation costs, and counselling costs. | Univariate and scenario analysis performed. | 1. Budget impact unfavourable over the 10 years. 2. Breakeven point of year 1 investment on PrEP with cumulative HIV care costs would be reached after 23 years if PrEP effectiveness was 86% and after 33 years if PrEP effectiveness was 64%. 3. If PrEP drug costs reduced by 90%, breakeven of year 1 investment would happen by the 5th year at 86% effectiveness and 6th year at 64% effectiveness. 4. Reduction in HIV drug costs would increase the time to breakeven of year 1 investment. |
| Alvis-Zakzuk et al. (2020) [15] | Colombia, health system perspective over 3 years. | BIA model adapted from one developed by Fiocruz in Brazil was used. | MSM and TGW. | PrEP programme costs | Univariate and scenario analysis were performed. | 1. PrEP was found to be cost-saving for the health system. 2. Among MSM, cost savings of COP 47 billion would be made in year 1, COP 20 billion in year 2, and COP 11 billion in year 3 at PrEP coverage of 80%. 3. Among TGW, cost savings of COP 3.3 billion would be made in year 1, COP 2.1 billion in year 2, and COP 8.1 billion in year 3 at PrEP coverage of 80%. |
| Kazemianet al. (2020) [16] | India, societal perspective over 15 years. | CEA and BIA were performed using the Cost-effectiveness of Preventing AIDS Complications-International (CEPAC-I) model. | MSM and PWID. | All costs related to HIV care, whether incurred by the health system, individuals, or society at large. | Univariate performed. | 1. PrEP with one time or 6 months testing were found not to be cost-saving both at 5 years and at 15 years. 2. Over a 5-year time horizon, one-time tests increased expenditures for MSM by USD 55 million while 6 months of testing resulted in additional costs of USD 708 million. 3. Over a 5-year time horizon, one-time testing increased expenditure for PWID by USD 21 million and 6 months testing by USD 218 million. 4. Over 15 years, PrEP with 6 months testing increased the HIV care budget by USD 1.67 billion among MSM and USD 387 million among PWID. |
| Reyes-Uruena et al. (2017) [17] | Spain, health service perspective over one year. | CEA and BIA were performed, although the model used was not specified. | MSM. | Direct medical costs, laboratory costs, and indirect medical costs. | Univariate performed on price of Truvada, HIV incidence, and PrEP effectiveness. | 1. The results show that PrEP was not cost-saving in one year. 2. Daily dosing of PrEP could be cost saving in 20 years if the cost of Truvada was reduced by 80% or HIV incidence was greater than 3%. 3. About EUR 50 million additional costs to the budget would be required per year if on-demand PrEP were adopted, and EUR 80 million per year if daily PrEP were adopted. |
| Walensky et al. (2012) [18] | South Africa, ministry of health perspective over 20 years. | CEA and BIA were performed using the CEPAC-I model. | Heterosexual women. | Direct medical and laboratory costs of PrEP and HIV care costs. | Univariate and multi-way performed. | 1. PrEP would not result in cost savings within the 20 year period. 2. However, reducing the total PrEP programme costs by 50%, having an annual HIV incidence rate above 5%, and having PrEP effectiveness above 50% would result in cost savings. 3. To achieve coverage of half the women population in the country would require USD 6 billion over 5 years. 4. Targeting women at highest risk and/or those most likely to adhere to PrEP would give the highest returns on the investment and would be cost-saving. |
| Juusola et al. (2012) [19] | United States of America, societal perspective over 20 years. | CEA and BIA were performed using a dynamic model of HIV transmission and progression. | MSM between 13 and 64 years of age. | All costs related to HIV care, whether incurred by the health system, individuals, or society at large. | Univariate and multivariate were performed. | 1. Not cost saving if used in the MSM general population. 2. Affordability in high-risk MSM was uncertain. Additional costs of USD 95 million required over 20 years with 20% PrEP coverage of the general MSM population. |
| Schneider et al. (2014) [20] | New South Wales (NSW), Australia, healthcare service provider over 10 years. | CEA and BIA performed using a stochastic agent-based model of HIV transmission and progression. | MSM. | Direct medical costs. | Univariate performed. | 1. Additional cost of AUD 316–AUD 952 million would be required over 10 years if PrEP were used in 10–30% of MSM in NSW. 2. Cost savings could be achieved if prices of PrEP drugs were similar to ART drugs and only 15% of MSM in discordant regular partnerships were targeted. |
| Moyo et al. (2022) [21] | Namibia, ministry of health perspective over 3 years. | BIA performed using a country-specific model. | All people in the population who are likely to acquire HIV. | Direct medical and laboratory costs of PrEP and HIV care costs. | Univariate and scenario analyses performed. | 1. Additional costs on HIV care were expected to reduce by 3.3%, 4.3%, and 5.4% in 2021, 2022, and 2023, respectively. 2. A 1% increase in cost savings was expected to be realised annually from 2022 3. If HIV care costs were increased by 10%, cost savings would increase by 3.5% in 2021 and 2022 and 3.4% in 2023. 4. If PrEP expenses were reduced by 10%, cost savings would increase by 3.8% in 2021 and 2023 and 3.9% in 2022. 5. Targeting people at high risk may be more cost-saving. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moyo, E.; Moyo, P.; Barham, L.; Mangoya, D.; Mhango, M.; Dzinamarira, T. The Budget Impact of Adopting Oral Pre-Exposure Prophylaxis for HIV Prevention: A Rapid Review. Venereology 2025, 4, 2. https://doi.org/10.3390/venereology4010002
Moyo E, Moyo P, Barham L, Mangoya D, Mhango M, Dzinamarira T. The Budget Impact of Adopting Oral Pre-Exposure Prophylaxis for HIV Prevention: A Rapid Review. Venereology. 2025; 4(1):2. https://doi.org/10.3390/venereology4010002
Chicago/Turabian StyleMoyo, Enos, Perseverance Moyo, Leela Barham, Derek Mangoya, Malizgani Mhango, and Tafadzwa Dzinamarira. 2025. "The Budget Impact of Adopting Oral Pre-Exposure Prophylaxis for HIV Prevention: A Rapid Review" Venereology 4, no. 1: 2. https://doi.org/10.3390/venereology4010002
APA StyleMoyo, E., Moyo, P., Barham, L., Mangoya, D., Mhango, M., & Dzinamarira, T. (2025). The Budget Impact of Adopting Oral Pre-Exposure Prophylaxis for HIV Prevention: A Rapid Review. Venereology, 4(1), 2. https://doi.org/10.3390/venereology4010002