
Point-of-Care Assays to Trichomonas vaginalis Diagnosis: The Road So Far

 , ,
, ,  and
and 
Abstract
1. Introduction
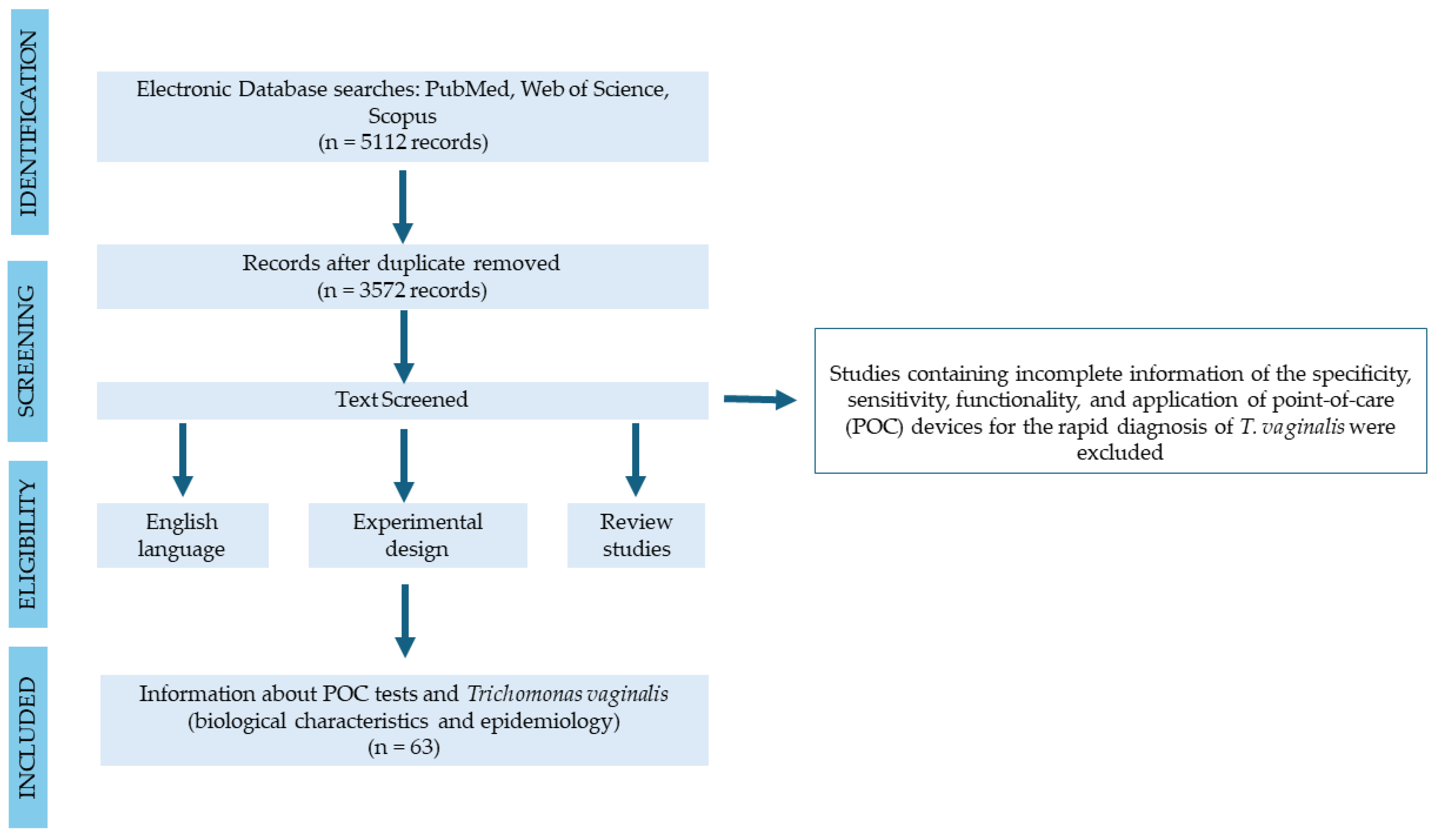
2. Materials and Methods
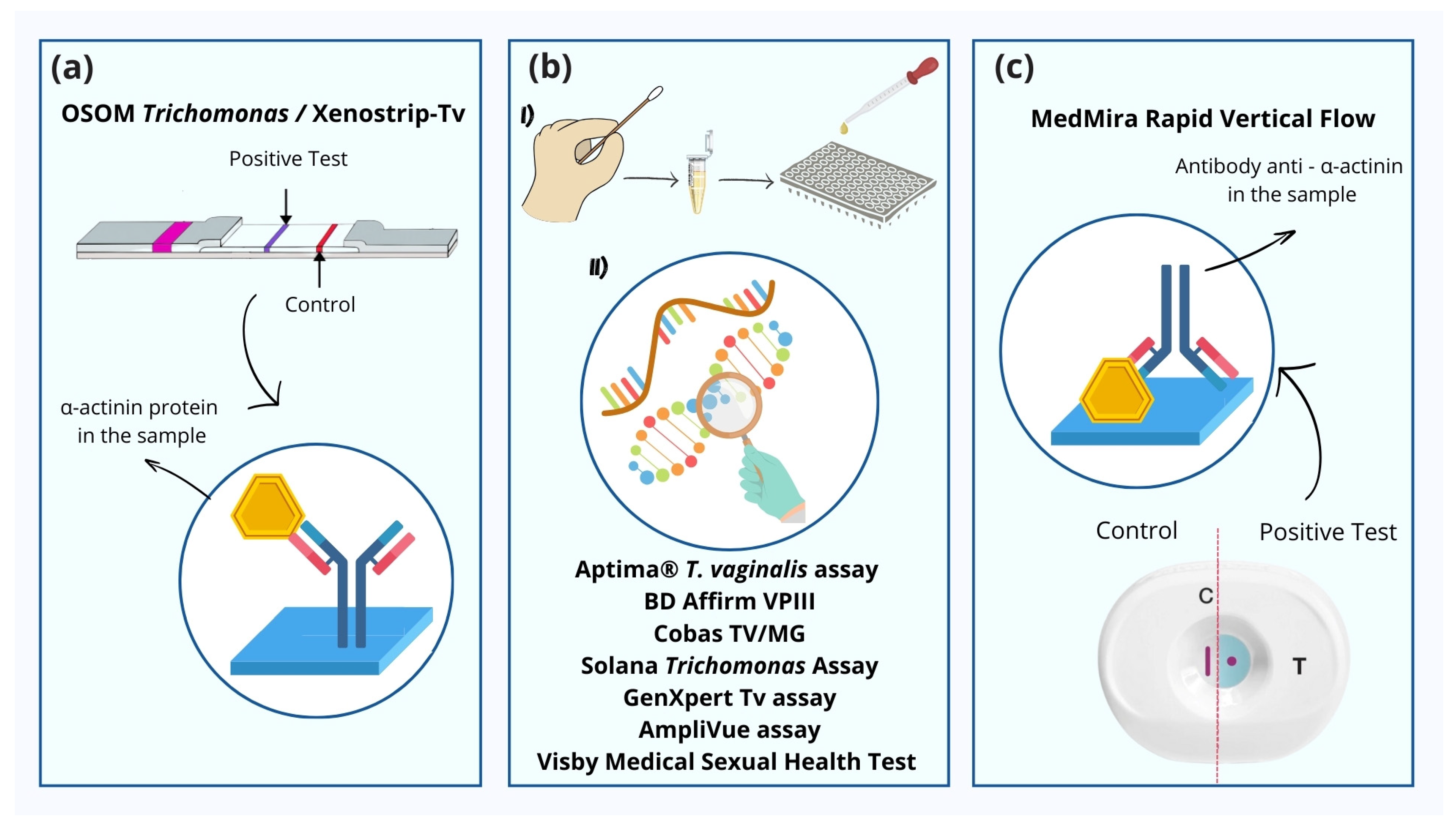
3. Types of POCs for Trichomoniasis
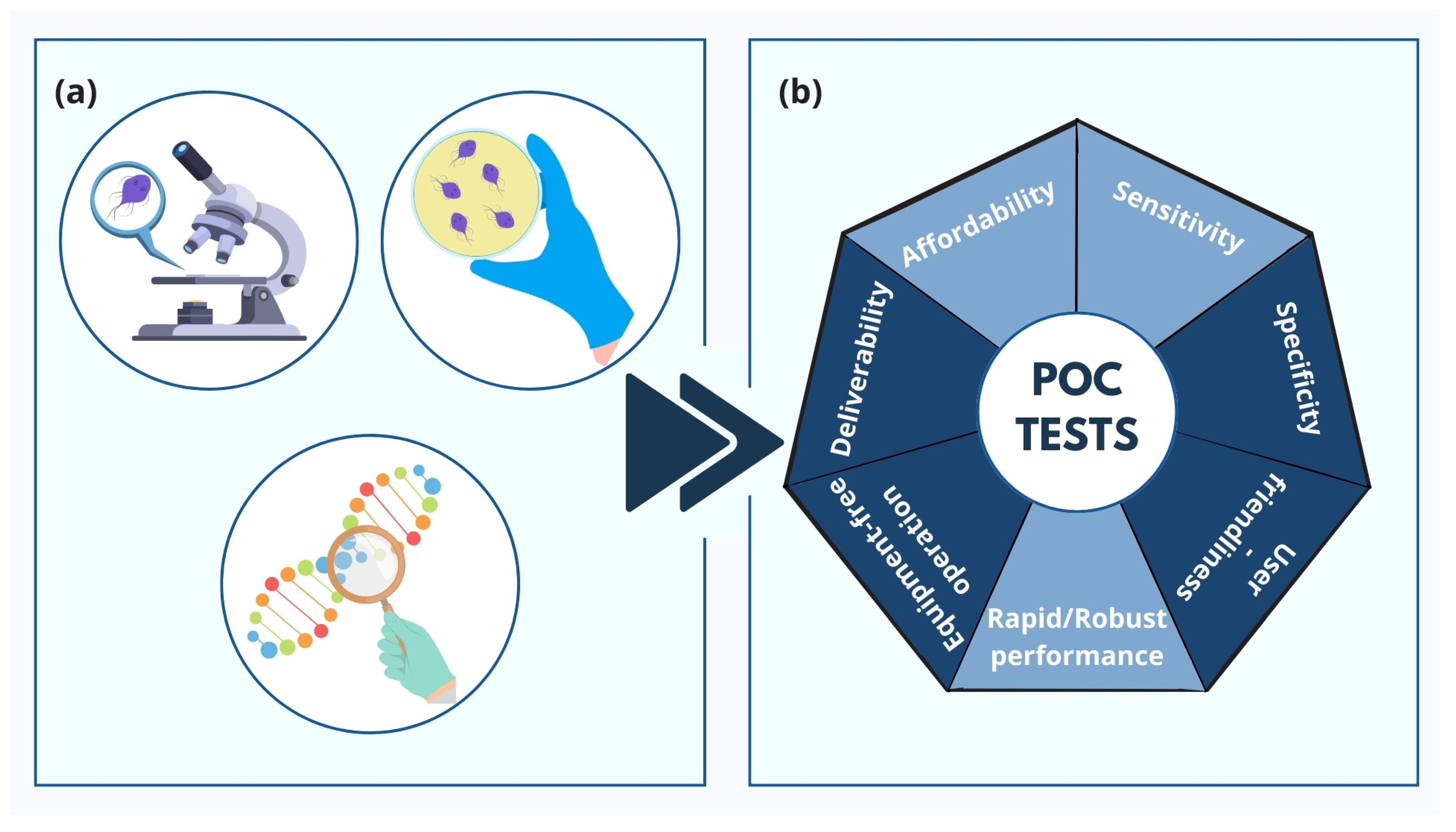
4. Discussion
5. Conclusions
6. Future Directions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Rowley, J.; Vander Hoorn, S.; Korenromp, E.; Low, N.; Unemo, M.; Abu-Raddad, L.J.; Chico, R.M.; Smolak, A.; Newman, L.; Gottlieb, S.; et al. Chlamydia, gonorrhoea, trichomoniasis and syphilis: Global prevalence and incidence estimates, 2016. Bull. World Health Organ. 2019, 97, 548–562. [Google Scholar] [CrossRef] [PubMed]
- Adamson, P.C.; Loeffelholz, M.J.; Klausner, J.D. Point-of-care testing for sexually transmitted infections: A review of recent developments. Arch. Pathol. Lab. Med. 2020, 144, 1344–1351. [Google Scholar] [CrossRef] [PubMed]
- Taheri, M.; Ghasemikhah, R. Clinical Manifestation and Epidemiological Finding of Trichomonas vaginalis Infection in Unusual Areas of Body in Neonates: A Systematic Review. Iran. J. Public Health 2022, 51, 1201–1209. [Google Scholar] [CrossRef] [PubMed]
- Kissinger, P. Trichomonas vaginalis: A review of epidemiologic, clinical and treatment issues. BMC Infect. Dis. 2015, 15, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Hezarjaribi, H.Z.; Saberi, R.; Fakhar, M.; Sadeghian, N. Is There Any Relationship between Trichomonas vaginalis Infection and Male Urethritis Risk? A Systematic Review and Meta-Analysis. Interdiscip. Perspect. Infect. Dis. 2022, 2022, 8359859. [Google Scholar] [CrossRef] [PubMed]
- Workowski, K.A.; Bolan, G.A. Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm. Rep. 2015, 64, 1–137. [Google Scholar]
- Nye, M.B.; Schwebke, J.R.; Body, B.A. Comparison of APTIMA Trichomonas vaginalis transcription-mediated amplification to wet mount microscopy, culture, and polymerase chain reaction for diagnosis of trichomoniasis in men and women. Am. J. Obstet. Gynecol. 2009, 200, 188.e1–188.e7. [Google Scholar] [CrossRef]
- Van Gerwen, O.T.; Muzny, C.A. Recent advances in the epidemiology, diagnosis, and management of Trichomonas vaginalis infection. F1000Research 2019, 8, 1666. [Google Scholar] [CrossRef]
- Kissinger, P.J.; A Gaydos, C.; Seña, A.C.; McClelland, R.S.; Soper, D.; Secor, W.E.; Legendre, D.; A Workowski, K.; A Muzny, C. Diagnosis and management of Trichomonas vaginalis: Summary of evidence reviewed for the 2021 Centers for Disease Control and Prevention sexually transmitted infections treatment guidelines. Clin. Infect. Dis. 2022, 74, S152–S161. [Google Scholar] [CrossRef]
- Nucleic Acid Based Tests. Available online: https://www.fda.gov/medical-devices/in-vitro-diagnostics/nucleic-acid-based-tests#microbial (accessed on 29 April 2024).
- Florkowski, C.; Don-Wauchope, A.; Gimenez, N.; Rodriguez-Capote, K.; Wils, J.; Zemlin, A. Point-of-care testing (POCT) and evidence-based laboratory medicine (EBLM)—Does it leverage any advantage in clinical decision making? Crit. Rev. Clin. Lab. Sci. 2017, 54, 471–494. [Google Scholar] [CrossRef]
- Tsai, W.W.; Nash, D.B.; Seamonds, B.; Weir, G.J. Point-of-care versus central laboratory testing: An economic analysis in an academic medical center. Clin. Ther. 1994, 16, 898. [Google Scholar] [PubMed]
- Lundberg, G.D. Acting on significant laboratory results. JAMA 1981, 245, 1762–1763. [Google Scholar] [CrossRef] [PubMed]
- Cristillo, A.D.; Bristow, C.C.; Peeling, R.; Van Der Pol, B.; de Cortina, S.H.; Dimov, I.K.; Pai, N.P.; Shin, D.J.; Chiu, R.Y.; Klapperich, C.; et al. Point-of-care sexually transmitted infection diagnostics: Proceedings of the STAR sexually transmitted infection—clinical trial group programmatic meeting. Sex. Transm. Dis. 2017, 44, 211. [Google Scholar] [CrossRef] [PubMed]
- Point-Of-Care Diagnostic Tests (POCTs) for Sexually Transmitted Infections (STIs). Available online: https://www.who.int/teams/sexual-and-reproductive-health-and-research-(srh)/areas-of-work/sexual-health/sexually-transmitted-infections/point-of-care-tests (accessed on 17 August 2023).
- Toskin, I.; Murtagh, M.; Peeling, R.W.; Blondeel, K.; Cordero, J.; Kiarie, J. Advancing prevention of sexually transmitted infections through point-of-care testing: Target product profiles and landscape analysis. Sex. Transm. Infect. 2017, 93, S69–S80. [Google Scholar] [CrossRef]
- de Cortina, S.H.; Bristow, C.C.; Davey, D.J.; Klausner, J.D. A systematic review of point of care testing for Chlamydia trachomatis, Neisseria gonorrhoeae, and Trichomonas vaginalis. Infect. Dis. Obstet. Gynecol. 2016, 2016, 4386127. [Google Scholar] [CrossRef]
- Gelbart, S.M.; Thomason, J.L.; Osypowski, P.J.; Kellett, A.V.; A James, J.; Broekhuizen, F.F. Growth of Trichomonas vaginalis in commercial culture media. J. Clin. Microbiol. 1990, 28, 962–964. [Google Scholar] [CrossRef]
- Van Gerwen, O.T.; Camino, A.F.; Sharma, J.; Kissinger, P.J.; A Muzny, C. Epidemiology, natural history, diagnosis, and treatment of Trichomonas vaginalis in men. Clin. Infect. Dis. 2021, 73, 1119–1124. [Google Scholar] [CrossRef]
- Gubala, V.; Harris, L.F.; Ricco, A.J.; Tan, M.X.; Williams, D.E. Point of care diagnostics: Status and future. Anal. Chem. 2012, 84, 487–515. [Google Scholar] [CrossRef] [PubMed]
- Hobbs, M.M.; Seña, A.C. Modern diagnosis of Trichomonas vaginalis infection. Sex. Transm. Infect. 2013, 89, 434–438. [Google Scholar] [CrossRef]
- Hegazy, M.M.; El-Tantawy, N.L.; Soliman, M.M.; El-Sadeek, E.S.; El-Nagar, H.S. Performance of rapid immunochromatographic assay in the diagnosis of Trichomoniasis vaginalis. Diagn. Microbiol. Infect. Dis. 2012, 74, 49–53. [Google Scholar] [CrossRef]
- Khatoon, R.; Jahan, N.; Ahmad, S.; Khan, H.; Rabbani, T. Comparison of four diagnostic techniques for detection of Trichomonas vaginalis infection in females attending tertiary care hospital of North India. Indian J. Pathol. Microbiol. 2015, 58, 36. [Google Scholar] [CrossRef]
- Madhivanan, P.; Li, T.; Trammell, S.; Desai, C.; Srinivas, V.; Arun, A.; Klausner, J.D.; Krupp, K. Performance of the OSOM Trichomonas Rapid Test for diagnosis of Trichomonas vaginalis infection among women in Mysore, India. Sex. Health 2013, 10, 320–324. [Google Scholar] [CrossRef] [PubMed]
- Campbell, L.; Woods, V.; Lloyd, T.; Elsayed, S.; Church, D.L. Evaluation of the OSOM trichomonas rapid test versus wet preparation examination for detection of Trichomonas vaginalis vaginitis in specimens from women with a low prevalence of infection. J. Clin. Microbiol. 2008, 46, 3467–3469. [Google Scholar] [CrossRef] [PubMed]
- Sheele, J.M.; Crandall, C.J.; Arko, B.L.; Vallabhaneni, M.; Dunn, C.T.; Chang, B.F.; Fann, P.; Bigach, M. The OSOM® Trichomonas Test is unable to accurately diagnose Trichomonas vaginalis from urine in men. Am. J. Emerg. Med. 2019, 37, 1002–1003. [Google Scholar] [CrossRef]
- Huppert, J.S.; Hesse, E.; Kim, G.; Kim, M.; Agreda, P.; Quinn, N.; Gaydos, C. Adolescent women can perform a point-of-care test for trichomoniasis as accurately as clinicians. Sex. Transm. Infect. 2010, 86, 514–519. [Google Scholar] [CrossRef] [PubMed]
- Pillay, A.; Lewis, J.; Ballard, R.C. Evaluation of Xenostrip-Tv, a rapid diagnostic test for Trichomonas vaginalis infection. J. Clin. Microbiol. 2004, 42, 3853–3856. [Google Scholar] [CrossRef]
- Gaydos, C.A.; Klausner, J.D.; Pai, N.P.; Kelly, H.; Coltart, C.; Peeling, R.W. Rapid and point-of-care tests for the diagnosis of Trichomonas vaginalis in women and men. Sex. Transm. Infect. 2017, 93, S31–S35. [Google Scholar] [CrossRef] [PubMed]
- Morris, S.R.; Bristow, C.C.; Wierzbicki, M.R.; Sarno, M.; Asbel, L.; French, A.; A Gaydos, C.; Hazan, L.; Mena, L.; Madhivanan, P.; et al. Performance of a single-use, rapid, point-of-care PCR device for the detection of Neisseria gonorrhoeae, Chlamydia trachomatis and Trichomonas vaginalis. Lancet Infect. Dis. 2021, 21, 668. [Google Scholar] [CrossRef]
- Martin, K.; Chikwari, C.D.; Dauya, E.; Mackworth-Young, C.R.S.; Bath, D.; Tucker, J.; Simms, V.; Bandason, T.; Ndowa, F.; Katsidzira, L.; et al. Investigating point-of-care diagnostics for sexually transmitted infections and antimicrobial resistance in antenatal care in Zimbabwe (IPSAZ): Protocol for a mixed-methods study. BMJ Open 2023, 13, e070889. [Google Scholar] [CrossRef]
- Gaydos, C.; Schwebke, J.; Dombrowski, J.; Marrazzo, J.; Coleman, J.; Silver, B.; Barnes, M.; Crane, L.; Fine, P. Clinical performance of the Solana® Point-of-Care Trichomonas assay from clinician-collected vaginal swabs and urine specimens from symptomatic and asymptomatic women. Expert Rev. Mol. Diagn. 2017, 17, 303–306. [Google Scholar] [CrossRef]
- Gaydos, C.A.D.; Hobbs, M.; Marrazzo, J.; Schwebke, J.; Coleman, J.S.; Masek, B.M.; Dize, L.; Jang, D.B.; Li, J.B.; Chernesky, M. Rapid diagnosis of Trichomonas vaginalis by testing vaginal swabs in an isothermal Helicase-Dependent AmpliVue assay. Sex. Transm. Dis. 2016, 43, 369–373. [Google Scholar] [CrossRef] [PubMed]
- Dessai, F.; Nyirenda, M.; Sebitloane, M.; Abbai, N. Diagnostic evaluation of the BD Affirm VPIII assay as a point-of-care test for the diagnosis of bacterial vaginosis, trichomoniasis and candidiasis. Int. J. STD AIDS 2020, 31, 303–311. [Google Scholar] [CrossRef]
- Taylor, S.; Rucki, A.; Lockamy, E.; Wolfe, D.; Streck, N.; Uribe, G.; Cammarata, C.; Diodene, D.; Cooper, C.K.; Vaughan, L.; et al. Validation of a New High-Throughput BD COR System Using the BD CTGCTV2 Assay. J. Mol. Diagn. 2022, 24, 485–493. [Google Scholar] [CrossRef]
- Van Der Pol, B.; Torres-Chavolla, E.; Kodsi, S.; Cooper, C.K.; Davis, T.E.; Fife, K.H.; Taylor, S.N.; Augenbraun, M.H.M.; Gaydos, C.A.M. Clinical performance of the BD CTGCTV2 assay for the BD MAX System for detection of Chlamydia trachomatis, Neisseria gonorrhoeae, and Trichomonas vaginalis infections. J. Sex. Transm. Dis. 2021, 48, 134–140. [Google Scholar] [CrossRef] [PubMed]
- Marlowe, E.M.; Gohl, P.; Steidle, M.; Arcenas, R.; Bier, C. Trichomonas vaginalis detection in female specimens with cobas® TV/MG for use on the cobas® 6800/8800 Systems. Eur. J. Microbiol. Immunol. 2019, 9, 42–45. [Google Scholar] [CrossRef]
- Alderete, J.F.; Chan, H. Point-of-Care Diagnostic for Trichomonas vaginalis, the Most Prevalent, Non-Viral Sexually Transmitted Infection. Pathogens 2023, 12, 77. [Google Scholar] [CrossRef]
- Riegler, A.N.; Larsen, N.; Amerson-Brown, M.H. Point-of-Care Testing for Sexually Transmitted Infections. Clin. Lab. Med. 2023, 43, 189–207. [Google Scholar] [CrossRef]
- World Health Organization. Point-of-Care Tests for Sexually Transmitted Infections: Target Product Profiles; World Health Organization: Geneva, Switzerland, 2023. [Google Scholar]
- Land, K.J.; Boeras, D.I.; Chen, X.-S.; Ramsay, A.R.; Peeling, R.W. REASSURED diagnostics to inform disease control strategies, strengthen health systems and improve patient outcomes. Nat. Microbiol. 2019, 4, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Harding-Esch, E.; Cousins, E.; Chow, S.-L.; Phillips, L.; Hall, C.; Cooper, N.; Fuller, S.; Nori, A.; Patel, R.; Thomas-William, S.; et al. A 30-min nucleic acid amplification point-of-care test for genital Chlamydia trachomatis infection in women: A prospective, multi-center study of diagnostic accuracy. EBioMedicine 2018, 28, 120–127. [Google Scholar] [CrossRef]
- Gettinger, J.; Van Wagoner, N.; Daniels, B.; Boutwell, A.; Van Der Pol, B. Patients are willing to wait for rapid sexually transmitted infection results in a university student health clinic. Sex. Trans. Dis. 2020, 47, 67–69. [Google Scholar] [CrossRef]
- Soin, N.; Fishlock, S.J.; Kelsey, C.; Smith, S. Triboelectric effect enabled self-powered, point-of-care diagnostics: Opportunities for developing assured and reassured devices. Micromachines. 2021, 12, 337. [Google Scholar] [CrossRef] [PubMed]
- Technical Consultation on Point-of-Care Tests for Sexually Transmitted Infections. Available online: https://www.who.int/reproductivehealth/POTC-TPPs-2016.pdf (accessed on 20 August 2023).
- Patel, E.U.; A Gaydos, C.; Packman, Z.R.; Quinn, T.C.; Tobian, A.A.R. Prevalence and correlates of Trichomonas vaginalis infection among men and women in the United States. Clin. Infect. Dis. 2018, 67, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Khatib, N.; Bradbury, C.; Chalker, V.; Koh, G.; Smit, E.; Wilson, S.; Watson, J. Prevalence of Trichomonas vaginalis, Mycoplasma genitalium and Ureaplasma urealyticum in men with urethritis attending an urban sexual health clinic. Int. J. STD AIDS 2015, 26, 388–392. [Google Scholar] [CrossRef] [PubMed]
- Gift, T.L.; Pate, M.S.M.; Hook, E.W.I.; Kassler, W.J. The rapid test paradox: When fewer cases detected lead to more cases treated: A decision analysis of tests for Chlamydia trachomatis. Sex. Transm. Dis. 1999, 26, 232–240. [Google Scholar] [CrossRef] [PubMed]
- Huntington, S.E.; Burns, R.M.; Harding-Esch, E.; Harvey, M.J.; Hill-Tout, R.; Fuller, S.S.; Adams, E.J.; Sadiq, S.T. Modelling-based evaluation of the costs, benefits and cost-effectiveness of multipathogen point-of-care tests for sexually transmitted infections in symptomatic genitourinary medicine clinic attendees. BMJ Open 2018, 8, e020394. [Google Scholar] [CrossRef] [PubMed]
- Vickerman, P. Sensitivity requirements for the point of care diagnosis of Chlamydia trachomatis and Neisseria gonorrhoeae in women. Sex. Transm. Infect. 2003, 79, 363–367. [Google Scholar] [CrossRef] [PubMed]
- Sadeghi, M.; Sadeghi, S.; Naghib, S.M.; Garshasbi, H.R. A Comprehensive Review on Electrochemical Nano Biosensors for Precise Detection of Blood-Based Oncomarkers in Breast Cancer. Biosensors 2023, 13, 481. [Google Scholar] [CrossRef]
- Gong, Z.; Huang, Y.; Hu, X.; Zhang, J.; Chen, Q.; Chen, H. Recent progress in electrochemical nano-biosensors for detection of pesticides and mycotoxins in foods. Biosensors 2023, 13, 140. [Google Scholar] [CrossRef] [PubMed]
- Abdelhamied, N.; Abdelrahman, F.; El-Shibiny, A.; Hassan, R.Y.A. Bacteriophage-based nano-biosensors for the fast impedimetric determination of pathogens in food samples. Sci. Rep. 2023, 13, 3498. [Google Scholar] [CrossRef] [PubMed]
- Ahangari, A.; Mahmoodi, P.; Mohammadzadeh, A. Advanced nano biosensors for rapid detection of zoonotic bacteria. Biotechnol. Bioeng. 2023, 120, 41–56. [Google Scholar] [CrossRef]
- Choi, H.K.; Yoon, J. Nanotechnology-assisted biosensors for the detection of viral nucleic acids: An Overview. Biosensors 2023, 13, 208. [Google Scholar] [CrossRef]
- Habimana, J.D.; Ji, J.; Sun, X. Minireview: Trends in optical-based biosensors for point-of-care bacterial pathogen detection for food safety and clinical diagnostics. Anal. Lett. 2018, 51, 2933–2966. [Google Scholar] [CrossRef]
- Bai, D.-P.; Lin, X.-Y.; Huang, Y.-F.; Zhang, X.-F. Theranostics aspects of various nanoparticles in veterinary medicine. Int. J. Mol. Sci. 2018, 19, 3299. [Google Scholar] [CrossRef]
- Mittal, S.; Kaur, H.; Gautam, N.; Mantha, A.K. Biosensors for breast cancer diagnosis: A review of bioreceptors, biotransducers and signal amplification strategies. Biosens. Bioelectron. 2017, 88, 217–231. [Google Scholar] [CrossRef] [PubMed]
- Ellington, A.D.; Szostak, J.W. In vitro selection of RNA molecules that bind specific ligands. Nature 1990, 346, 818–822. [Google Scholar] [CrossRef] [PubMed]
- Robertson, D.L.; Joyce, G.F. Selection in vitro of an RNA enzyme that specifically cleaves single-stranded DNA. Nature 1990, 344, 467–468. [Google Scholar] [CrossRef]
- Tuerk, C.; Gold, L. Systematic evolution of ligands by exponential enrichment: RNA ligands to bacteriophage T4 DNA polymerase. Science 1990, 249, 505–510. [Google Scholar] [CrossRef]
- Stoltenburg, R.; Reinemann, C.; Strehlitz, B. SELEX—A (r) evolutionary method to generate high-affinity nucleic acid ligands. Biomol. Eng. 2007, 24, 381–403. [Google Scholar] [CrossRef]
- Espiritu, C.A.L.; Justo, C.A.C.; Rubio, M.J.; Svobodova, M.; Bashammakh, A.S.; Alyoubi, A.O.; Rivera, W.L.; Rollon, A.P.; O’sullivan, C.K. Aptamer selection against a Trichomonas vaginalis adhesion protein for diagnostic applications. ACS Infect. Dis. 2018, 4, 1306–1315. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| POC Test | Sample | Time to Diagnosis | Sensitivity | Mechanism |
|---|---|---|---|---|
| Mount microscopy | Vaginal and urethral secretions | 10 min | 44–68% | Direct observation of parasites |
| Culture | Vaginal swab and urine | - | Variable | Culture |
| OSOM trichomonas rapid test | Vaginal swab | 10 min | 85–100% | Qualitative immuno-chromatography (antigen detection) |
| Xenostrip-TV | Vaginal swab | 10 min | 98–100% | Immunochromatography |
| Visby Medical Sexual Health Test | Vaginal swab | 30 min | 98.50% | PCR |
| GeneXpert TV assay | Vaginal swab | 30 min | 99.9–100% | PCR |
| Solana trichomonas assay | Vaginal swab | <40 min | 92–100% | DNA presence |
| AmpliVue | Vaginal swab | 45 min | 98–100% | PCR |
| BD Affirm VPIII | Vaginal fluids | 45 min | 91–100% | Molecular probe—acid nucleic identification |
| BD MAX CTG CTV2 | Vaginal swab and urine | - | 100% | PCR |
| Cobas TV/MG | Vaginal swab and urine | - | >95% | PCR |
| MedMira rapid vertical flow (RFV) | Blood or serum | 5 min | 99–100% | Specific antibodies |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borges, A.V.B.e.; Perini, H.F.; Alvin, E.A.; Silva, A.C.A.; da Silva, M.V. Point-of-Care Assays to Trichomonas vaginalis Diagnosis: The Road So Far. Venereology 2024, 3, 107-119. https://doi.org/10.3390/venereology3030009
Borges AVBe, Perini HF, Alvin EA, Silva ACA, da Silva MV. Point-of-Care Assays to Trichomonas vaginalis Diagnosis: The Road So Far. Venereology. 2024; 3(3):107-119. https://doi.org/10.3390/venereology3030009
Chicago/Turabian StyleBorges, Anna Victória Bernardes e, Hugo Felix Perini, Eliete Almeida Alvin, Anielle Christine Almeida Silva, and Marcos Vinicius da Silva. 2024. "Point-of-Care Assays to Trichomonas vaginalis Diagnosis: The Road So Far" Venereology 3, no. 3: 107-119. https://doi.org/10.3390/venereology3030009
APA StyleBorges, A. V. B. e., Perini, H. F., Alvin, E. A., Silva, A. C. A., & da Silva, M. V. (2024). Point-of-Care Assays to Trichomonas vaginalis Diagnosis: The Road So Far. Venereology, 3(3), 107-119. https://doi.org/10.3390/venereology3030009