
Historical Perspective and Current State Review: Advancing Lifelong Learning and Continuing Professional Education in Nutrition and Dietetics to Expand Opportunities, Equity, Access, and Future Transformations



Highlights
Abstract
:1. Introduction
2. Methods
3. Findings
3.1. Historical Review and Recent Advances in Nutrition and Dietetics CPE
| Practice Point: The Academy of Nutrition and Dietetics’ focus on lifelong learning and the framework of the Commission on Dietetic Registration (CDR) for continuing professional education (CPE) have continued to evolve and advance. Self-reflection is fundamental to the nutrition and dietetics professional development process, and a reflective learning approach can yield increased and deeper learning. Interprofessional practice benefits high-quality care delivery and interprofessional continuing education (IPCE) can fulfill the CDR’s recertification requirements. |
3.2. Review of the Joint Accreditation for Interprofessional Continuing Education’s Development and IPCE Standards
- The organization’s education structure and processes were designed by and for the healthcare team and have been in place for at least the past 18 months;
- At least 25% of all the educational activities delivered by the organization during the past 18 months were interprofessional, and the organization can demonstrate an integrated planning process (i.e., the process includes input from two or more health professions who represent the targeted healthcare team to address identified practice gaps);
- An integrated planning process that includes healthcare professionals from two or more professions.
- An integrated planning process that includes healthcare professionals who are reflective of the target audience members the activity is designed to address.
- An intent to achieve outcome(s) that reflect a change in skills, strategy, or performance of the healthcare team and/or patient outcomes.
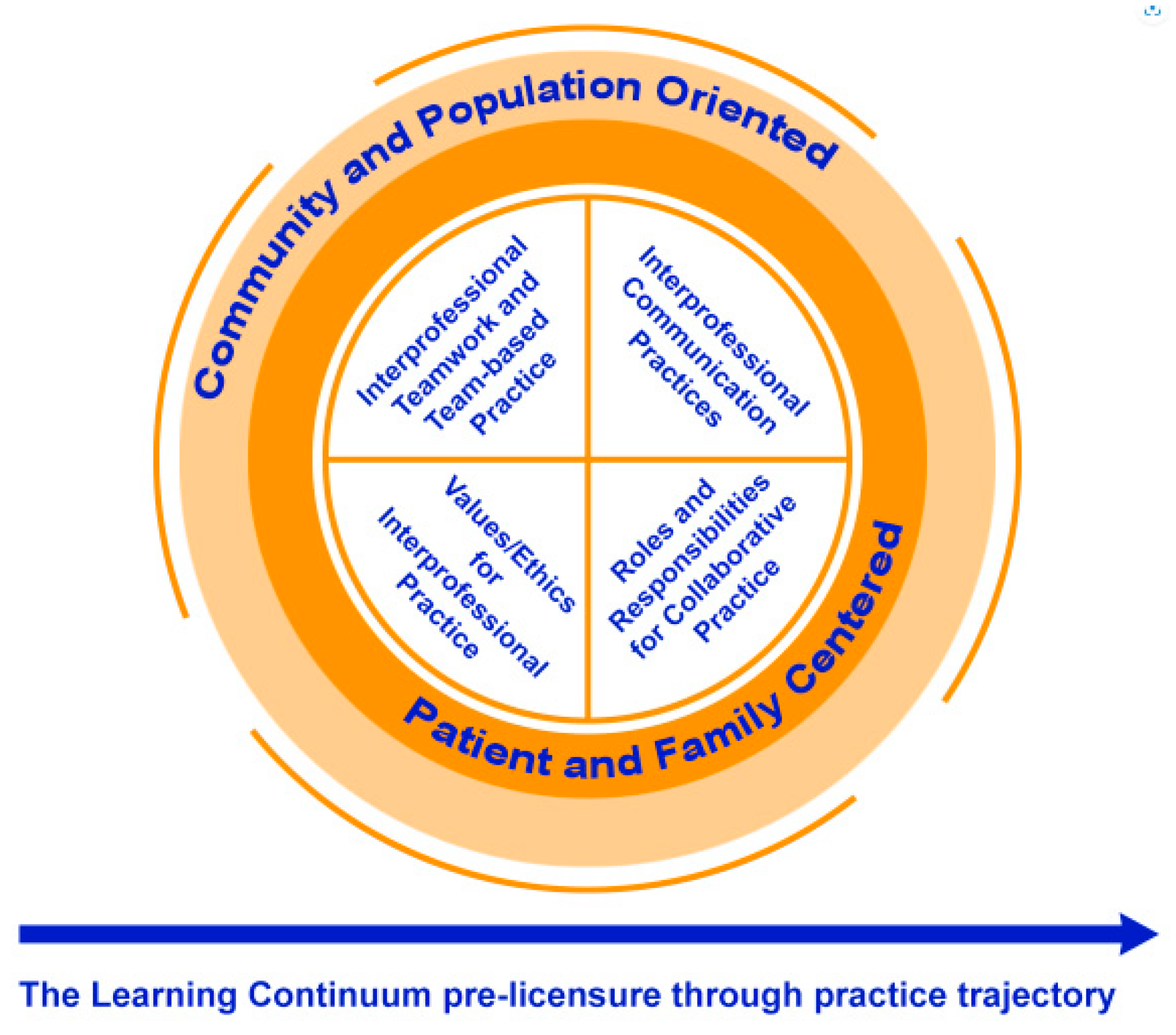
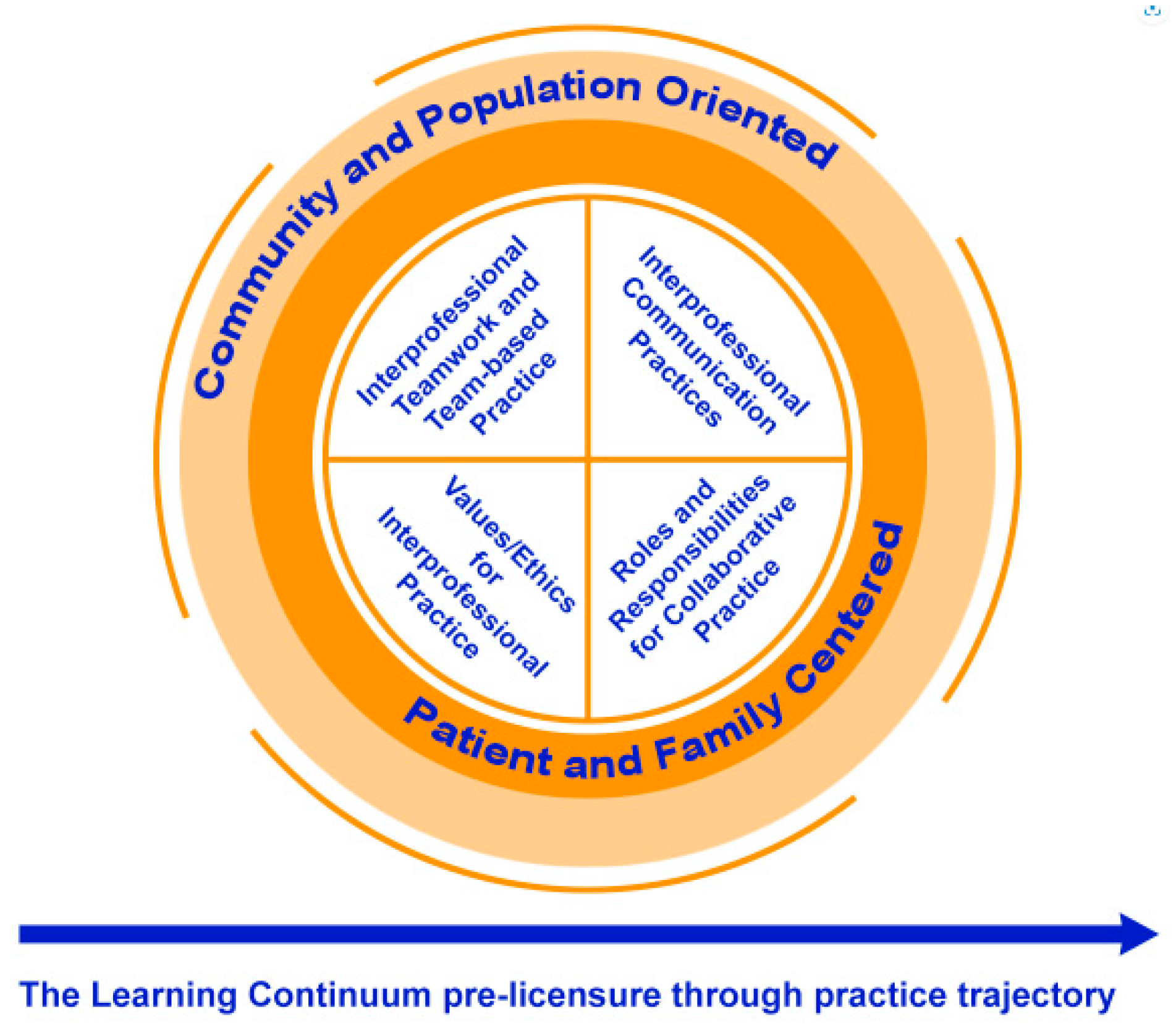
- Reflection of one or more of the interprofessional competencies to include values/ethics, roles/responsibilities, interprofessional communication, and/or teams/teamwork.
- An opportunity for learners to learn with, from, and about each other.
- Activity evaluations that seek to determine:
- ○
- Changes in skills, strategy, performance of one’s role or contribution as a member of the healthcare team; and/or
- ○
- Impact on the healthcare team; and/or
- ○
- Impact on patient outcomes [32]”.
| Practice Point: In 2020, the Commission on Dietetic Registration (CDR) joined the Joint Accreditation for Interprofessional Continuing Education organization (Joint Accreditation). Joint-accredited organizations have the advantage of being able to offer interprofessional continuing education (ICPE) for up to 10 different professions. To become joint-accredited, organizations must meet specific criteria, including that their ICPE complies with the Accreditation Council for Continuing Medical Education (ACCME) Standards for Integrity and Independence in Accredited Continuing Education. |
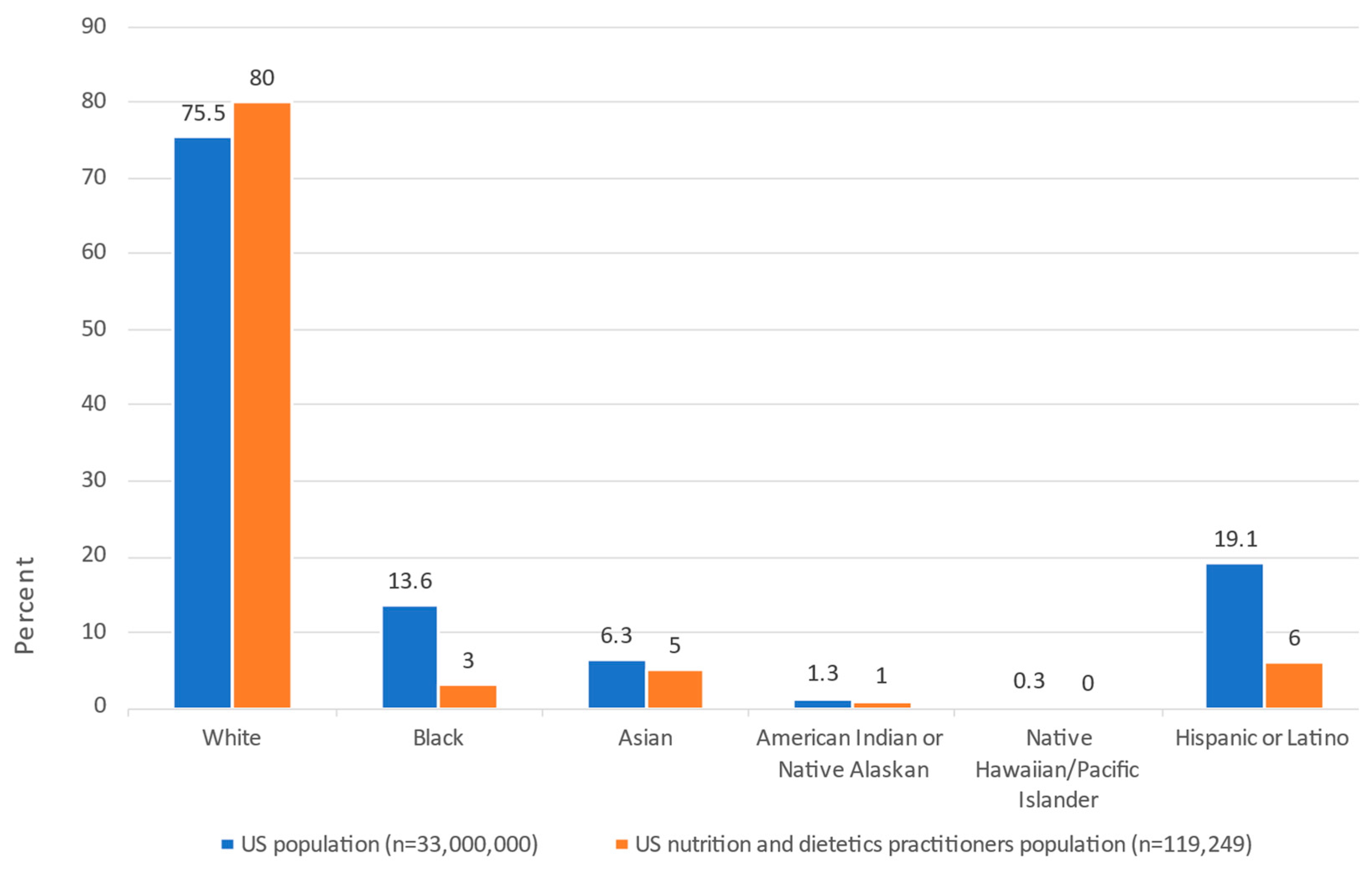
3.3. Current State Review of the CDR and Academy’s Strategies for Building a More Diverse Practitioner Pipeline and Opportunities to Support CPE Access and Equity
| Practice Point: As the US population becomes more diverse, it is critical that nutrition and dietetics recruitment and continuing professional education (CPE) continue to intentionally foster inclusion, diversity, equity, and access (IDEA). The new policies of the Commission on Dietetics Registration (CDR) require prior-approved CPE activities to be conducted with a comprehensive IDEA lens. These steps are important to advance the nutrition and dietetics profession and the development of CPE, as well as to help reduce health disparities. |
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AAPA | American Academy of Physician Associates |
| Academy | Academy of Nutrition and Dietetics |
| ACCME | Accreditation Council for Continuing Medical Education |
| ACEND | Accreditation Council for Education in Nutrition and Dietetics |
| ACPE | Accreditation Council for Pharmacy Education |
| ADA CERP | American Dental Association’s Continuing Education Recognition Program |
| ANCC | American Nurses Credentialing Center |
| APA | American Psychological Association |
| ARBO | Association of Regulatory Boards of Optometry |
| ASWB | Association of Social Work Boards |
| BOC | Board of Certification for the Athletic Trainer |
| CDR | Commission on Dietetic Registration |
| COPE | Council on Optometric Practitioner Education |
| CPE | Continuing Professional Education |
| DEI | diversity, equity, and inclusion |
| DPD | Didactic Program in Dietetics |
| HBCUs | historically Black colleges and universities |
| IDEA | inclusion, diversity, equity, and access |
| IPCE | interprofessional continuing education |
| ISPP | Individualized Supervised Practice Pathway |
| JAC | Joint Accreditation Criteria |
| Joint Accreditation | Joint Accreditation for Interprofessional Continuing Education |
| MIG | Member Interest Group |
| NOBIDAN | National Organization of Blacks in Dietetics and Nutrition |
| PDP | Professional Development Portfolio |
| RISA | Research, International, and Scientific Affairs |
| RDN | registered dietitian nutritionist |
| US | United States |
References
- Stein, K.; Rops, M. The Commission on Dietetic Registration: Ahead of the trends for a competent 21st century workforce. J. Acad. Nutr. Diet. 2016, 116, 1981–1997.e7. [Google Scholar] [CrossRef] [PubMed]
- Chernoff, R. President’s page: A little knowledge. J. Am. Diet. Assoc. 1996, 96, 1053. [Google Scholar] [CrossRef]
- Puckett, R.P. Education and the dietetics profession. J. Am. Diet. Assoc. 1997, 97, 252–253. [Google Scholar] [CrossRef] [PubMed]
- Fitz, P. President’s Page: Lifelong learning is the key to success. J. Acad. Nutr. Diet. 1997, 97, 1014. [Google Scholar]
- Monsen, E.R. Lifelong learning expands career horizons. J. Am. Diet. Assoc. 1999, 99, 522. [Google Scholar] [CrossRef]
- Monsen, E.R. Becoming an active learner--and teacher--for life. J. Am. Diet. Assoc. 2000, 100, 154. [Google Scholar] [CrossRef]
- Touger-Decker, R. Developing a continuum for lifelong learning in dietetics. Top. Clin. Nutr. 2002, 17, 1. [Google Scholar] [CrossRef]
- Gilbride, J.A. The challenges and rewards of life-long learning. J. Am. Diet. Assoc. 2006, 106, 1933. [Google Scholar] [CrossRef]
- Yadrick, M.M. Accountability for lifelong learning. J. Am. Diet. Assoc. 2009, 109, 203. [Google Scholar] [CrossRef]
- Bergman, E.A. Lifelong learning advances us—One and all. J. Acad. Nutr. Diet. 2012, 112, 1518. [Google Scholar] [CrossRef]
- Duyff, R.L. The Value of lifelong learning: Key element in professional career development. J. Acad. Nutr. Diet. 1999, 99, 538–543. [Google Scholar] [CrossRef]
- Academy of Nutrition and Dietetics. Eat Right Pro: Committee for Lifelong Learning. Available online: https://www.eatrightpro.org/leadership/governance/academy-committees/committee-for-lifelong-learning (accessed on 8 August 2023).
- Commission on Dietetic Registration. About CDR. Available online: https://www.cdrnet.org/about (accessed on 8 August 2023).
- Joint Accreditation Interprofessional Continuing Education. Commission on Dietetic Registration Joins Joint Accreditation. Available online: https://jointaccreditation.org/news/commission-dietetic-registration-joins-joint-accreditation/ (accessed on 8 August 2023).
- Commission on Dietetic Registration. Credentialing Tips: Phase-Out-CDR CPE Accredited Provider Program. Available online: https://admin.cdrnet.org/vault/2459/web/Credentialing%20Tips-Phase-Out-CDR%20CPE%20Accredited%20Provider%20Program%20Feb%202022.pdf (accessed on 8 August 2023).
- Shanley, E.R. Recruiting and preparing the next generation of practitioners. J. Acad. Nutr. Diet. 2022, 122, 2203–2204. [Google Scholar] [CrossRef]
- Academy of Nutrition and Dietetics. Eat Right Pro: Inclusion, Diversity, Equity, and Access. Available online: https://www.eatrightpro.org/about-us/our-work/inclusion-diversity-equity-and-access (accessed on 8 August 2023).
- Goals of the Lifetime Education of the Dietitian. Committee on Goals of Education for Dietetics, Dietetic Internship Council, the American Dietetic Association. J. Am. Diet. Assoc. 1969, 54, 91–93. [CrossRef]
- American Dietetic Association. A new look at the profession of dietetics. Final report of the American Dietetic Association Foundation 1984 Study Commission on Dietetics: Summary and recommendations. J. Am. Diet. Assoc. 1984, 84, 1052–1063. [Google Scholar] [CrossRef]
- Commission on Dietetic Registration. Professional Development Portfolio Guide with Essential Practice Competencies. 2018. Available online: https://www.cdrnet.org/vault/2459/web/files/PDP%20Guide%202018.pdf (accessed on 8 August 2023).
- Worsfold, L.; Grant, B.L.; Barnhill, G.C. The essential practice competencies for the Commission on Dietetic Registration’s credentialed nutrition and dietetics practitioners. J. Acad. Nutr. Diet. 2015, 115, 978–984. [Google Scholar] [CrossRef]
- Commission on Dietetic Registration. Professional Development Portfolio Guide with Essential Practice Competencies. 2020. Available online: https://www.cdrnet.org/vault/2459/web/CDR%20PDP%20Guide%20June%202%202023%20thru%20May%202029_v2_FINAL.pdf (accessed on 8 August 2023).
- Davies, S. Embracing reflective practice. Educ. Prim. Care 2012, 23, 9–12. [Google Scholar] [CrossRef] [PubMed]
- Fragkos, K.C. Reflective practice in healthcare education: An umbrella review. Educ. Sci. 2016, 6, 27. [Google Scholar] [CrossRef]
- World Health Organization. Framework for Action on Interprofessional Education & Collaborative Practice. Available online: https://www.who.int/publications-detail-redirect/framework-for-action-on-interprofessional-education-collaborative-practice (accessed on 8 August 2023).
- Continuing Education, Professional Development, and Lifelong Learning for the 21st Century Health Care Workforce. Available online: https://www.hrsa.gov/sites/default/files/hrsa/advisory-committees/community-based-linkages/reports/eleventh-2011.pdf (accessed on 8 August 2023).
- The University of Texas Austin Center for Health Interprofessional Practice and Education. Framework for Action on Interprofessional Education & Collaborative Practice. Core Competencies for Interprofessional Collaborative Practice. Available online: https://healthipe.utexas.edu/core-competencies-interprofessional-collaborative-practice-0 (accessed on 8 August 2023).
- Regnier, K.; Chappell, K.; Travlos, D.V. The role and rise of interprofessional continuing education. J. Med. Regul. 2019, 105, 6–13. [Google Scholar] [CrossRef]
- Gordon, B.; Weeden, A. The interprofessional practice learning needs of nutrition and dietetics students. J. Acad. Nutr. Diet. 2023, 123, 386–398. [Google Scholar] [CrossRef]
- Commission on Dietetic Registration. CDR CPEU Prior Approval Program Provider Policy Manual. Available online: https://www.cdrnet.org/vault/2459/web/CDR%20CPEU%20Prior%20Approval%20Program%20Provider%20Policy%20Manual.pdf (accessed on 8 August 2023).
- Accreditation Council for Continuing Medical Education. Standards for Integrity and Independence in Accredited Continuing Education Released December 2020. Available online: https://accme.org/sites/default/files/2021-06/884_20210624_New%20Standards%20Standalone%20Package.pdf (accessed on 8 August 2023).
- Joint Accreditation Interprofessional Continuing Education. Joint Accreditation Framework Advancing Healthcare Education by the Team, for the Team. Available online: https://jointaccreditation.org/wp-content/uploads/2023/02/816_20230130_ja_framework.pdf (accessed on 8 August 2023).
- Regnier, K.; Travlos, D.V.; Pace, D.; Powell, S.; Hunt, A. Leading change together: Supporting collaborative practice through Joint Accreditation for Interprofessional Continuing Education. J. Eur. CME 2022, 11, 2146372. [Google Scholar] [CrossRef]
- Chappell, K.; Regnier, K.; Travlos, D.V. Leading by example: The role of accreditors in promoting interprofessional collaborative practice. J. Interprof. Care 2018, 32, 404–406. [Google Scholar] [CrossRef] [PubMed]
- Joint Accreditation Interprofessional Continuing Education. Accrediting Organizations for ICPE for Healthcare. Available online: https://jointaccreditation.org/joint-accreditation/accrediting-organizations/ (accessed on 7 August 2023).
- Joint Accreditation Interprofessional Continuing Education. 2022 Joint Accreditation Data Report: Touchstones of Strength and Progress in Accredited Continuing Education for Healthcare Teams. Available online: www.jointaccreditation.org/reports/2022-data-report (accessed on 8 August 2023).
- Joint Accreditation Interprofessional Continuing Education. Joint Accreditation Criteria. Available online: https://jointaccreditation.org/accreditation-process/requirements/criteria/ (accessed on 8 August 2023).
- Joint Accreditation Interprofessional Continuing Education. Accreditation Process Eligibility. Available online: https://jointaccreditation.org/accreditation-process/eligibility/ (accessed on 8 August 2023).
- Moulton, J.; Dickerson, P. Implementing the standards for integrity and independence in accredited nursing continuing professional development. J. Contin. Educ. Nurs. 2022, 53, 52–54. [Google Scholar] [CrossRef] [PubMed]
- Wong, L.; Arndt, R.; Katz, A.R.; Loos, J.R.; Masaki, K.; Tokumaru, S.; Davis, K.F. Transforming the future of health care today with interprofessional education. Hawaii J. Health Soc. Welf. 2023, 82, 16–18. [Google Scholar]
- Joint Accreditation Interprofessional Continuing Education. Improving Healthcare with Interprofessional Continuing Education (IPCE). Available online: https://jointaccreditation.org/ (accessed on 8 August 2023).
- Joint Accreditation Interprofessional Continuing Education. 2022 Joint Accreditation Leadership Summit Climbing Higher with IPCE. Available online: https://jointaccreditation.org/wp-content/uploads/2023/02/2022-Joint-Accreditation-Leadership-Summit_Climbing-Higher-with-IPCE.pdf (accessed on 8 August 2023).
- Agic, B.; Fruitman, H.; Maharaj, A.; Taylor, J.; Ashraf, A.; Henderson, J.; Ronda, N.; McKenzie, K.; Soklaridis, S.; Sockalingam, S. Advancing curriculum development and design in health professions education: A health equity and inclusion framework for education programs. J. Contin. Educ. Health Prof. 2022. [Google Scholar] [CrossRef] [PubMed]
- American Psychological Association. What Does Diversity Mean as an Approved Sponsor? Available online: https://www.apa.org/ed/sponsor/resources/diversity.pdf (accessed on 8 August 2023).
- U.S. Census Bureau. The Chance That Two People Chosen at Random Are of Different Race or Ethnicity Groups Has Increased Since. 2010. Available online: https://www.census.gov/library/stories/2021/08/2020-united-states-population-more-racially-ethnically-diverse-than-2010.html (accessed on 9 August 2023).
- Biden-Harris Administration National Strategy on Hunger, Nutrition and Health. Available online: https://www.whitehouse.gov/wp-content/uploads/2022/09/White-House-National-Strategy-on-Hunger-Nutrition-and-Health-FINAL.pdf (accessed on 8 August 2023).
- Taub-Dix, B. Diversifying Dietetics. Todays Dietit. 2020, 22, 4. [Google Scholar]
- U.S. Census Bureau QuickFacts: United States. Available online: https://www.census.gov/quickfacts/fact/table/US/PST045222 (accessed on 8 August 2023).
- Rogers, D. Report on the Academy/Commission on Dietetic Registration 2020 Needs Satisfaction Survey. J. Acad. Nutr. Diet. 2021, 121, 134–138. [Google Scholar] [CrossRef]
- Reeves, R.V.; Smith, F. Black and Hispanic Americans at Higher Risk of Hypertension, Diabetes, Obesity: Time to Fix Our Broken Food System. Available online: https://www.brookings.edu/articles/black-and-hispanic-americans-at-higher-risk-of-hypertension-diabetes-obesity-time-to-fix-our-broken-food-system/ (accessed on 8 September 2023).
- Johnson-Askew, W.L.; Gordon, L.; Sockalingam, S. Practice paper of the American Dietetic Association: Addressing racial and ethnic health disparities. J. Am. Diet. Assoc. 2011, 111, 446–456. [Google Scholar] [CrossRef]
- Institute of Medicine (US). Committee on Understanding and Eliminating Racial and Ethnic Disparities in Health Care Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care; Smedley, B.D., Stith, A.Y., Nelson, A.R., Eds.; National Academies Press (US): Washington, DC, USA, 2003. [Google Scholar]
- Stein, K. The Educational pipeline and diversity in dietetics. J. Acad. Nutr. Diet. 2013, 113, S13–S19. [Google Scholar] [CrossRef]
- Burt, K.G.; Delgado, K.; Chen, M.; Paul, R. Strategies and recommendations to increase diversity in dietetics. J. Acad. Nutr. Diet. 2019, 119, 733–738. [Google Scholar] [CrossRef]
- Academy of Nutrition and Dietetics. Eat Right Pro: Academy Strategic Plan. Available online: https://www.eatrightpro.org/about-us/our-work/academy-strategic-plan (accessed on 7 September 2023).
- Commission on Dietetic Registration. 2024 Graduate Degree Requirement-Registration Eligibility. Available online: https://www.cdrnet.org/graduatedegree (accessed on 10 August 2023).
- Academy of Nutrition and Dietetics. Eat Right Pro: Academy Foundation Accepting Scholarship Applications. Available online: https://www.eatrightpro.org/about-us/for-media/press-releases/academy-foundation-accepting-scholarship-applications (accessed on 10 August 2023).
- Cohen, B.; DuBois, S.; Lynch, P.A.; Swami, N.; Noftle, K.; Arensberg, M.B. Use of an artificial intelligence-driven digital platform for reflective learning to support continuing medical and professional education and opportunities for interprofessional education and equitable access. Educ. Sci. 2023, 13, 760. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| ACCME Standard | Case Examples | Applications | Exceptions | Related Policies for the CDR’s Prior Approval Program for Nutrition and Dietetics CPE |
|---|---|---|---|---|
| Standard 1: Ensure content is valid | ||||
| Accredited providers are responsible for ensuring that their education is fair and balanced and that any clinical content presented supports safe, effective patient care. | Discussing new evolving science about a nutrient or a diet-related intervention |
|
|
|
| Standard 2: Prevent commercial bias and marketing in accredited CE | ||||
| Accredited continuing education must protect learners from commercial bias and marketing. | Sharing learners’ contact information with a commercial company |
|
|
|
| Standard 3: Identify, mitigate, and disclose relevant financial relationships | ||||
| The accredited provider is responsible for identifying relevant financial relationships between individuals in control of educational content and ineligible companies and managing these to ensure they do not introduce commercial bias into the education. | Using a corporate speaker |
|
|
|
| Planning for a non-clinical activity |
|
| ||
| Standard 4: Manage commercial support appropriately | ||||
| Accredited providers that choose to accept commercial support (defined as financial or in-kind support from ineligible companies) are responsible for ensuring that the education remains independent of the ineligible company and that the support does not result in commercial bias or commercial influence in the education. | Using a corporate grant |
|
|
|
| Standard 5: Manage ancillary activities offered in conjunction with accredited continuing education | ||||
| Accredited providers are responsible for ensuring that education is separate from marketing by ineligible companies—including advertising, sales, exhibits, and promotion—and from nonaccredited education offered in conjunction with accredited continuing education. | Non-accredited and non-prior-approved continuing education in an exhibit hall |
|
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gonzalez, A.L.; Lynch, P.A.; Dorner, B.; Arensberg, M.B. Historical Perspective and Current State Review: Advancing Lifelong Learning and Continuing Professional Education in Nutrition and Dietetics to Expand Opportunities, Equity, Access, and Future Transformations. Dietetics 2023, 2, 321-333. https://doi.org/10.3390/dietetics2040023
Gonzalez AL, Lynch PA, Dorner B, Arensberg MB. Historical Perspective and Current State Review: Advancing Lifelong Learning and Continuing Professional Education in Nutrition and Dietetics to Expand Opportunities, Equity, Access, and Future Transformations. Dietetics. 2023; 2(4):321-333. https://doi.org/10.3390/dietetics2040023
Chicago/Turabian StyleGonzalez, Andie Lee, Patricia A. Lynch, Becky Dorner, and Mary Beth Arensberg. 2023. "Historical Perspective and Current State Review: Advancing Lifelong Learning and Continuing Professional Education in Nutrition and Dietetics to Expand Opportunities, Equity, Access, and Future Transformations" Dietetics 2, no. 4: 321-333. https://doi.org/10.3390/dietetics2040023
APA StyleGonzalez, A. L., Lynch, P. A., Dorner, B., & Arensberg, M. B. (2023). Historical Perspective and Current State Review: Advancing Lifelong Learning and Continuing Professional Education in Nutrition and Dietetics to Expand Opportunities, Equity, Access, and Future Transformations. Dietetics, 2(4), 321-333. https://doi.org/10.3390/dietetics2040023