1. Introduction
The main risk factor for severe forms of coronavirus infection is age. There are different approaches to determine the individual age. Calendar age is the number of years lived. Biological age can be determined by compiles biological indicators including telomerase activity, telomere length and the degree of DNA and histone modifications (epigenetic clock), or by the appearance of aging biomarkers [
1,
2,
3,
4], according to the fragility index [
5,
6], and by estimation of the physiological parameters of the body [
7,
8]. While, subjective age [
9], psychological age [
10] are the measures of subjective assessment of person’s life path.
Most authors associate the occurrence of severe forms of COVID-19 disease with calendar age [
11]. According to data from China, older people, especially people with serious underlying medical conditions, have a higher risk of serious illness and death associated with COVID-19 than younger people [
12]. Cases of COVID-19 between February 12 and March 16, 2020 and the severity of the disease (hospitalisation, admission to the intensive care unit (ICU) and death) by age group were analysed in the United States. Overall, 31% of cases, 45% of hospitalisations, 53% of ICU admissions and 80% of COVID-19-related deaths were registered in adults aged 65 and over. The highest percentage of severe outcomes was noted among people aged 85 years and older [
13]. A possible reason for this is the weakening of immunity in older age groups [
14].
However, some authors suggest that the severity of the disease is rather more strongly associated with the biological age measured by the glycan or epigenetic clock [
15,
16,
17]. American researchers studied biological age indicators of 347,751 participants from a large community cohort in the United Kingdom (UK Biobank), collected between 2006 and 2010, they also studied disease diagnoses (up to 2017), mortality data (up to 2020) and UK national COVID-19 test results (till 31 May 2020). They showed that accelerated aging 10–14 years prior to the COVID-19 pandemic onset was associated with a positive test (OR = 1.15 for 5-year acceleration, 95% C: 1.08–1.21,
p = 3.2 × 10
−6) and all-cause mortality with a confirmed COVID-19 test (OR = 1.25, 5-year acceleration, 95% Di: 1.09–1.44,
p = 0.002) after adjusting for demographic data, including current chronological age, and pre-existing diseases or conditions [
18]. However, when DNA methylation methods are used to assess biological age, the effect is less frequent. For example, using four different age predictors, the authors did not observe accelerated aging in the global DNA methylation profiles of blood samples from nine COVID-19 patients with severe symptoms. Predictions correlated well with chronological age, while COVID-19 patients even tended to be predicted younger than expected [
19].
Research is also underway on the correlation between the severity of COVID-19 and selected biomarkers of aging, including those of the senility index. For example, concomitant cardiovascular diseases in patients with COVID-19 are associated with high mortality risk [
20]. COVID-19 can induce the appearance of biomarkers of aging and impair cardiovascular diseases, including myocardial damage, arrhythmias, acute coronary syndrome, and venous thromboembolism [
21,
22].
We found no specific studies linking the risk of severe COVID-19 with psychological age. However, the impact of the consequences of the COVID-19 pandemic on the subjective perception of time has been noted [
23].
The purpose of this investigation is to study the effect of biopsychological age indicators on the risk of COVID-19 disease and on the probability of death in the Russian Federation during the 2020 epidemic.
2. Methods
1. Biological age (BA) determination according to V. P. Voitenko [
2] (also detailed in [
10,
24]). Calculation is based on the indicators of the cardiovascular system (blood pressure), the state of the respiratory system (breath holding on inhale), the musculoskeletal system and the equilibrium system (static balancing with closed eyes), metabolism (body weight) and psychological indicators (subjective assessment of health).
2. Expected biological age (EBA) for different age groups. This indicator is considered the statistical norm of biological age within a specific age group. It is being used to assess the relative aging index.
3. The relative biological ageing (RBA) index: the difference between biological age and expected biological age (BA-EBA), allows to assess how much an individual is older than their statistical age norm in terms of their health status. Negative values indicate individual youthfulness, while positive values show individual ageing in comparison with statistical norm. This is the main indicator used to assess the dynamics of relative aging.
4. Subjective psychological age (PA), according to K.A. Abulkhanova and T.N. Berezina [
10]. The test subjects were asked to evaluate their age at the 100-point scale (from 0 to 100), where 0 points are the age of a newborn baby, and 100 points—a person who has already achieved everything and will not be able to achieve more. The method is described in detail here [
10].
5. The relative psychological ageing (RPA) index: psychological age minus calendar age (PA-CA). Negative values indicate the person’s perception to be younger than their calendar age. Positive values indicate that the person considers themselves more mature, wise, and successful than other people at that age.
6. COVID-19 severity scale. 0 points—the disease is absent. 1 point—a mild form of the disease, the presence of certain symptoms (positive PCR smear). 2 points—the average severity of the disease (hospitalisation). 3 points—severe degree of the disease (staying in the ICU and/or mechanical ventilation). 4 points—lethal outcome (cause of death—COVID-19).
7. Quarantine compliance scale. 0 points—did not comply at all. 1 point—minimum compliance (“just leave me alone”). 2 points—met the basic requirements when outside. 3 points—met all the requirements when outside, 4 points—complete self-isolation, did not leave home, limited contacts.
3. Statistical Analysis. One-Way Analysis of Variance (ANOVA), Regression Analysis (Linear Regression)
Sample. Total 447 people aged 35-70 years (306 women) included in the database of the longitudinal study of the retirement reform in Russia. Among them: (1) working adults—239 people (155 women, average age = 47.7; and 84 men, average age = 51.9), examined at the place of work or study; (2) retiree with chronic diseases (risk group)—208 people (151 women, average age = 64.7; and 57 men, average age = 66.8). The survey was carried out in the outpatient hospital (polyclinic). Testing was carried out in mid-2020 (the indicators of biopsychological age were measured) and at the end of 2020 (the number of cases, the severity of the disease and its outcome were assessed).
4. Results
At the first stage, we studied the disease dynamics in the working group and the risk group. The peak of the first wave of incidence in Russia occurred in the 2nd half of 2020. In the first half of the year, there were only 0.4% of cases in the working group, reaching 31% by the end of 2020. Interestingly, over the entire observation period, there were no cases in the risk group. We assume that the representatives of the risk group more strictly observed quarantine measures (3.5–3.8 points versus 2.0–2.3 working group). Respondents from the risk group, who tended to stay at home, practically without leaving their place of residence, had limited communication, and contacted health workers by phone or were seen by doctor at home. Adult workers led more active lifestyles, went to work, and provided livelihoods for families, including at-risk retirement parents.
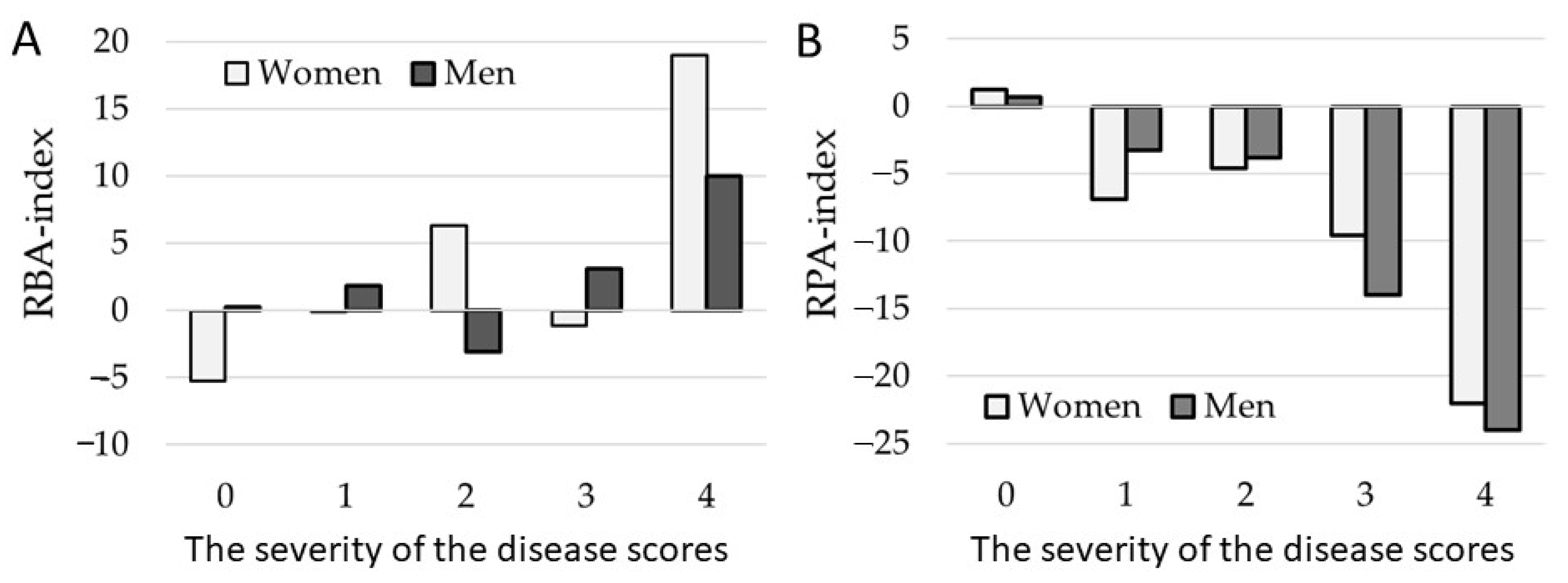
Figure 1A shows the relative biological aging (RBA) indicators. The RBA index associates with the risk of severe forms of COVID-19, both in men (F = 1.7104,
p = 0.17150) and in women (F = 1.980,
p = 0.002). The increase of the relative psychological aging (RPA) index, on the contrary, reduces the risk of severe forms of COVID-19, both in men (F = 2.222,
p = 0.007) and in women (F = 1.837,
p = 0.004), (
Figure 1B).
Assessing the influence of various age indicators on the onset of the disease and on the risk of patients’ death (in the group of working adults), we found that the calendar age in the range of 35–70 years affects the onset of the disease and the possibility of death only at the trend level (
p = 0.1) (
Table 1). The absolute biological and psychological age did not affect the rate of the disease, however, with an increase of biological age, the likelihood of death increases. It is the relative indicators (RBA, RPA), showing how much the person is older or younger than their age standard, that had a particularly strong influence (
Figure 1). The older the person is (biological age relative to the peer standard, RBA), the higher the likelihood of the disease onset (
p = 0.05) and the probability of patient’s death (
p < 0.001). And vice versa, the younger the person considers themselves to be psychologically in relation to their calendar age (RPA indicator), the higher the likelihood of the disease onset (
p = 0.059) and the probability of patients’ death (
p = 0.00001) (
Figure 1B,
Table 1).
5. Discussion
The main risk factor for coronavirus infection is considered to be age, as well as concomitant age-related diseases such as diabetes mellitus [
25], obesity [
26], and impaired blood coagulation [
27]. Our study shows that the risk of contracting COVID-19 is affected by quarantine measures. Older people at risk observed quarantine more strictly than middle-aged people, so the incidence in older people was lower. The ability to strictly observe quarantine in the elderly was due to the fact that they were retired and did not work [
28]. The occurrence of the disease is influenced by both the biological and psychological age of a person. Biological age characterizes the state of the body, all systems of its organs. Not surprisingly, biological age affects disease resistance. While the impact on the severity of the disease of psychological age, which reflects a person’s subjective assessment of his life path, is an interesting phenomenon.
As our study has shown, the risk of severity of COVID-19 is associated not by absolute values of biological or psychological age, but rather by relative indicators. The main risk factor for a person is a significant increase in his biological age over the calendar age, with a significant decrease in psychological age relative to the calendar age. We suggest that if people consider themselves younger than they are, they tend to underestimate the danger of infection. Perhaps, they are more prone to risky behavior. Previously, it was shown that the mismatch of biological and psychological ages is a dangerous indicator and may be associated with the effects of stress, due to retirement [
24] or professional circumstances [
29].
6. Conclusions
Compliance with quarantine measures is an effective way to prevent COVID-19 spread. Not a single case of COVID-19 infection was detected in the risk group in Russia (retirees with severe chronic diseases) whose representatives observed strict self-isolation measures. In the group of working adults, the disease was registered in 31% of the surveyed (2% of deaths) in 2020.
The probability of contracting COVID-19 in working adults in Russia aged 35–70 years was most influenced by the individual relative biological age: the higher the RBA index, the higher the risk of infection (p = 0.05), and the probability of death (p < 0.001). The relative psychological age had an inverse effect on the risk of infection: the higher the RPA index, the lower the risk of infection (p = 0.06) and the risk of death (p < 0.001). Calendar age also increased the risk of infection and the risk of death at a trend level below the validity level.
The most dangerous is the combination of an increase of the RBA index and an underestimation of the RPA index. In this case, the risk of severe forms of the disease increases, up to a lethal outcome.
7. Recommendations
A predictive model based on regression analysis has been developed to predict the risk of severe forms of COVID-19 in terms of relative biological and psychological ages.
All addends are significant (p < 0.01). The model describes empirical data with validity F (2.236) = 13.137, p < 0.001, R = 0.316. The risk index values correspond to those described in the method for the disease severity estimation (see methods number 6).
The model can predict the risks of severe COVID-19. It can be implemented both for further clinical trials on an expanded sample and as a mobile application for individual use. The necessary techniques for assessing the indicators of biological and psychological age are described in our early works [
10,
30].
Author Contributions
Conceptualization, T.N.B. and S.A.R.; methodology, T.N.B.; software, S.A.R.; validation, T.N.B., S.A.R.; formal analysis, T.N.B.; investigation, S.A.R.; resources, T.N.B.; data curation, T.N.B.; writing—original draft preparation, T.N.B.; writing—review and editing, S.A.R.; visualization, S.A.R.; supervision, T.N.B.; project administration, T.N.B.; funding acquisition, T.N.B. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by Russian Science Foundation, No. 22-18-00150.
Data Availability Statement
Not applicable.
Acknowledgments
The authors are grateful to the researchers who took part in the collection of empirical material: A.M. Zinatullina, A.A. Kalaeva, G.V. Fatyanova. Natalia Rybtsov for useful cements.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Lara, J.; Cooper, R.; Nissan, J.; Ginty, A.T.; Khaw, K.-T.; Deary, I.J.; Lord, J.M.; Kuh, D.; Mathers, J.C. A proposed panel of biomarkers of healthy ageing. BMC Med. 2015, 13, 222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Voitenko, V.P.; Tokar, A.V. The assessment of biological age and sex differences of human aging. Exp. Aging Res. 1983, 9, 239–244. [Google Scholar] [CrossRef] [PubMed]
- Romero Starke, K.; Petereit-Haack, G.; Schubert, M.; Kämpf, D.; Schliebner, A.; JHegewald Seidler, A. The age-related risk of severe outcomes due to covid-19 infection: A rapid review, meta-analysis, and meta-regression. Int. J. Environ. Res. Public Health 2020, 17, 5974. [Google Scholar] [CrossRef] [PubMed]
- Moskalev, A. The challenges of estimating biological age. eLife 2020, 9, e54969. [Google Scholar] [CrossRef]
- Vries, N.M.; de Staal, J.B.; van Ravensberg, C.D.; Hobbelen, J.S.M.; Olde Rikkert, M.G.M.; Nijhuis-van der Sanden, M.W.G. Outcome instruments to measure frailty: A systematic review. Ageing Res. Rev. 2011, 10, 104–114. [Google Scholar] [CrossRef]
- Searle, S.D.; Mitnitski, A.; Gahbauer, E.A.; Gill, T.M.; Rockwood, K. A standard procedure for creating a frailty index. BMC Geriatr. 2008, 8, 24. [Google Scholar] [CrossRef] [Green Version]
- Hertel, J.; Friedrich, N.; Wittfeld, K.; Pietzner, M.; Budde, K.; Van der Auwera, S.; Lohmann, T.; Teumer, A.; Völzke, H.; Nauck, M.; et al. Measuring biological age via metabonomics: The metabolic age score. J. Proteome Res. 2016, 15, 400–410. [Google Scholar] [CrossRef]
- Hamczyk, M.R.; Nevado, R.M.; Barettino, A.; Fuster, V.; Andrés, V. Biological versus chronological aging: Jacc focus seminar. J. Am. Coll. Cardiol. 2020, 75, 919–930. [Google Scholar] [CrossRef]
- Barak, B. Age identity: A cross-cultural global approach. Int. J. Behav. Dev. 2009, 33, 2–11. [Google Scholar] [CrossRef]
- Berezina, T.N.; Rybtsova, N.N.; Rybtsov, S.A. Comparative Dynamics of Individual Ageing Among the Investigative Type of Professionals Living in Russia and Russian Migrants to the EU Countries. Eur. J. Investig. Health Psychol. Educ. 2020, 10, 749–762. [Google Scholar] [CrossRef]
- Tay, M.Z.; Poh, C.M.; Rénia, L.; MacAry, P.A.; Ng, L.F.P. The trinity of covid-19: Immunity, inflammation and intervention. Nat. Rev. Immunol. 2020, 20, 363–374. [Google Scholar] [CrossRef] [PubMed]
- Novel Coronavirus Pneumonia Emergency Response Epidemiology Team. The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19) in China. Chin. J. Epidemiol. 2020, 41, 145–151. [Google Scholar] [CrossRef]
- Bialek, S.; Boundy, E.; Bowen, V.; Chow, N.; Cohn, A.; Dowling, N.; Ellington, S.; Gierke, R.; Hall, A.; MacNeil, J.; et al. Severe Outcomes Among Patients with Coronavirus Disease 2019 (COVID-19)—United States, February 12–March 16, 2020. MMWR. Morb. Mortal. Wkly. Rep. 2020, 69, 343–346. [Google Scholar] [CrossRef]
- Rybtsova, N.; Berezina, T.; Kagansky, A.; Rybtsov, S. Can Blood-Circulating Factors Unveil and Delay Your Biological Aging? Biomedicines 2020, 8, 615. [Google Scholar] [CrossRef] [PubMed]
- Lauc, G.; Sinclair, D. Biomarkers of biological age as predictors of COVID-19 disease severity. Aging 2020, 12, 6490–6491. [Google Scholar] [CrossRef]
- Polidori, M.C.; Sies, H.; Ferrucci, L.; Benzing, T. Covid-19 mortality as a fingerprint of biological age. Ageing Res. Rev. 2021, 67, 101308. [Google Scholar] [CrossRef]
- Lauc, G.; Pezer, M.; Rudan, I.; Campbell, H. Mechanisms of disease: The human n-glycome. Biochim. Biophys. Acta 2016, 1860, 1574–1582. [Google Scholar] [CrossRef] [Green Version]
- Kuo, C.L.; Pilling, L.C.; Atkins, J.L.; Masoli, J.A.; Delgado, J.; Tignanelli, C.; Levine, M.E. COVID-19 Severity Is Predicted by Earlier Evidence of Accelerated Aging. Available online: https://www.medrxiv.org/content/10.1101/2020.07.10.20147777v1.full-text (accessed on 23 January 2021).
- Franzen, J.; Nüchtern, S.; Tharmapalan, V.; Vieri, M.; Nikolić, M.; Han, Y.; Wagner, W. Epigenetic Clocks Are Not Accelerated in COVID-19 Patients. Available online: https://www.medrxiv.org/content/10.1101/2020.11.13.20229781v1.full-text (accessed on 23 January 2021).
- Atkins, J.L.; Masoli, J.A.H.; Delgado, J.; Pilling, L.C.; Kuo, C.-L.C.; Kuchel, G.; Melzer, D. Preexisting comorbidities predicting severe COVID-19 in older adults in the UK biobank community cohort. MedRxiv 2020, 11, 2224–2230. [Google Scholar] [CrossRef]
- Nishiga, M.; Wang, D.W.; Han, Y.; Lewis, D.B.; Wu, J.C. COVID-19 and cardiovascular disease: From basic mechanisms to clinical perspectives. Nat. Rev. Cardiol. 2020, 17, 543–558. [Google Scholar] [CrossRef]
- Shinohara, T.; Saida, K.; Tanaka, S.; Murayama, A. Association between frailty and changes in lifestyle and physical or psychological conditions among older adults affected by the coronavirus disease 2019 countermeasures in Japan. Geriatr. Gerontol. Int. 2021, 21, 39–42. [Google Scholar] [CrossRef]
- Maffoni, M.; Torlaschi, V.; Pierobon, A. It’s all a matter of time. Ann. Ig. 2020, 32, 689–690. [Google Scholar] [PubMed]
- Berezina, T.; Rybtsova, N.; Rybtsov, S.; Fatianov, G. Individually-personal factors of pension stress in representatives of the intellectual type of professions. J. Mod. Foreign Psychol. 2020, 9, 8–21. [Google Scholar] [CrossRef]
- McGurnaghan, S.J.; Weir, A.; Bishop, J.; Kennedy, S.; Blackbourn LA, K.; McAllister, D.A.; Hutchinson, S.; Caparrotta, T.M.; Mellor, J.; Jeyam, A.; et al. Risks of and risk factors for covid-19 disease in people with diabetes: A cohort study of the total population of Scotland. Lancet Diabetes Endocrinol. 2021, 9, 82–93. [Google Scholar] [CrossRef]
- Hendren, N.S.; de Lemos, J.A.; Ayers, C.; Das, S.R.; Rao, A.; Carter, S.; Rosenblatt, A.; Walchok, J.; Omar, W.; Khera, R.; et al. Association of body mass index and age with morbidity and mortality in patients hospitalized with COVID-19: Results from the american heart association COVID-19 cardiovascular dis-ease registry. Circulation 2021, 143, 135–144. [Google Scholar] [CrossRef] [PubMed]
- Wolff, D.; Nee, S.; Hickey, N.S.; Marschollek, M. Risk factors for COVID-19 severity and fatality: A structured literature review. Infection 2021, 49, 15–28. [Google Scholar] [CrossRef]
- Zinatullina, A.M.; Melnik, V.P.; Zimina, A.A. Personal factors of biological aging in working and non-working respondents in late maturity period. Int. J. Health Sci. 2021, 5, 639–648. [Google Scholar] [CrossRef]
- Koteneva, A.V.; Berezina, T.N.; Rybtsov, S.A. Religiosity, Spirituality and Biopsychological Age of Professionals in Russia. Eur. J. Investig. Health Psychol. Educ. 2021, 11, 1221–1238. [Google Scholar] [CrossRef]
- Berezina, T. Distribution of biomarkers of aging in people with different personality types (in Russia). E3S Web Conf. 2020, 210, 17028. [Google Scholar] [CrossRef]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).




{kind=link}