
Development and Feasibility Test of a Theory- and Evidence-Based Multicomponent Intervention to Reduce Student Smoking at Danish Vocational Schools

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Setting
2.2. Sources of Data
2.2.1. Qualitative Data from Fieldwork in VET Schools
2.2.2. Workshops with Students
2.2.3. Workshop with Stakeholders
2.2.4. Literature
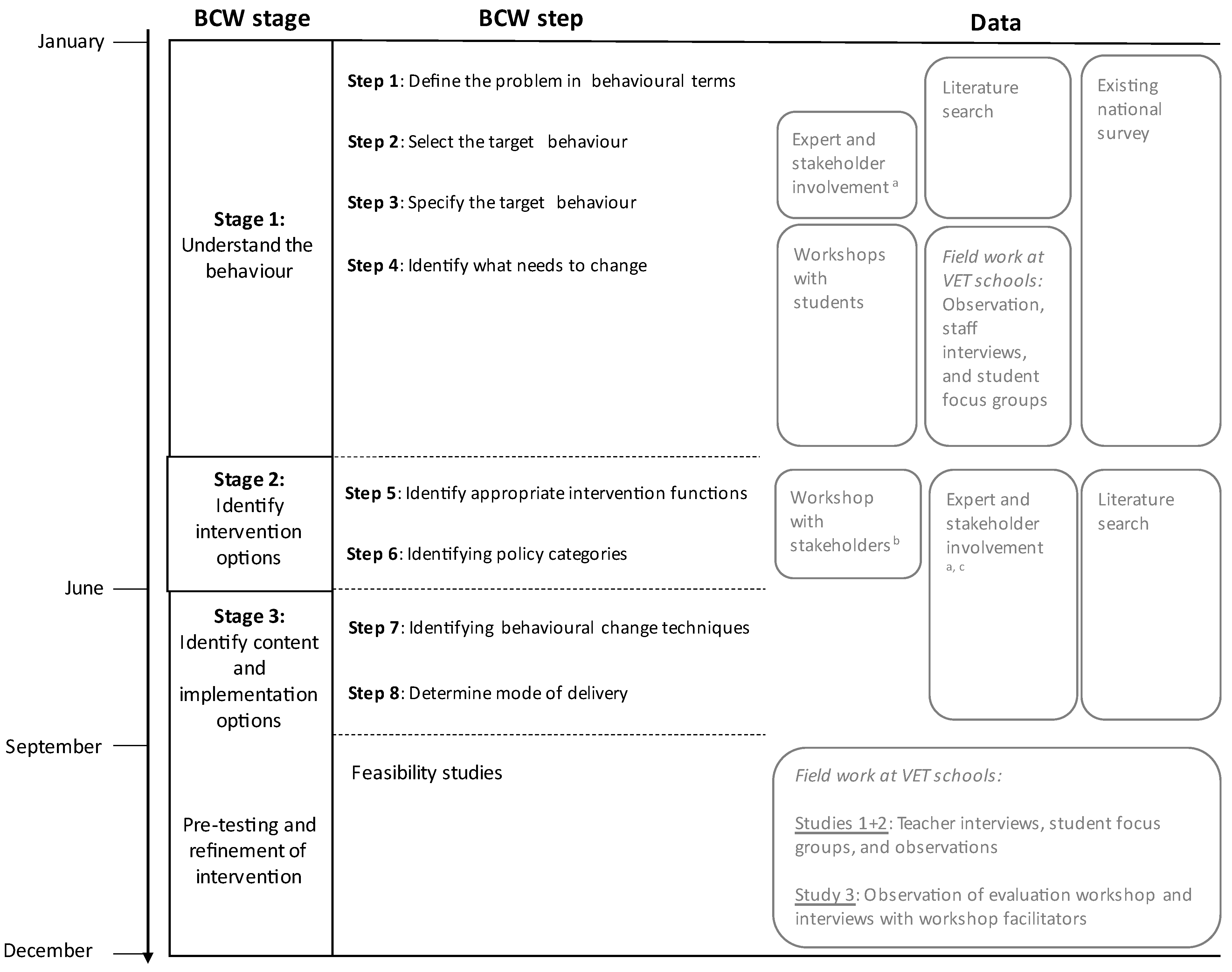
3. Overview of the Development Process (BCW Steps)
3.1. Step 1: Define the Problem
3.2. Steps 2 and 3: Select and Specify the Target Behaviour
3.3. Step 4: Identify What Needs to Change
- Psychological capability: knowledge or psychological skills, strength or stamina to engage in the necessary mental processes;
- Physical capability: physical skills, strength or stamina;
- Physical opportunity: opportunity afforded by the environment involving time, resources, locations, cues, physical ‘affordability’;
- Social opportunity: opportunity afforded by interpersonal influences, social cues, and cultural norms that influence the way we think about things;
- Reflective motivation: reflective processes are cognitive processes such as goals and explicit attitudes and beliefs;
- Automatic motivation: automatic processes occur spontaneously without conscious control and are often based on affective associations related to seeking pleasure or avoiding displeasure.
3.4. Steps 5 and 6: Identify Intervention Functions and Policy Categories
3.5. Step 7: Identify Content (Behaviour Change Techniques)
3.6. Step 8: Identify Implementation Options (Mode of Delivery)
- Study 1: We pre-tested the class-based intervention components at two VET schools in the Capital Region of Denmark. We collected feedback through two focus group interviews with a total of fifteen students (age range 15–19 years; 65% women) and six semi-structured interviews with teachers, by discussing their experiences with the tested components. Moreover, we conducted two days of observations to observe how the intervention components worked in practice.
- Study 2: Smoking cessation support delivered by the national Quitline was discussed among students from a third VET school in the Capital Region of Denmark. We held two focus group interviews with a total of ten students (age range 16–18 years), which focused on students’ acceptability of the Quitline approach.
- Study 3: A comprehensive school tobacco policy ‘smoke-free-school-day’ was implemented at a large VET school in the Region of Southern Denmark with support from the Danish Cancer Society. Feedback on process was achieved through an evaluation workshop at the VET school, which was facilitated by the Danish Cancer Society. We observed the workshop and interviewed two facilitators from the Danish Cancer Society, who assisted with the implementation of the policy and facilitated the workshop.
4. Results
4.1. Step 1: Identification of the Problem
4.2. Steps 2 and 3: Specification of the Target Behaviour
4.3. Step 4: COM-B Analysis: Identification of What Needs to Change
4.3.1. Psychological Capability
4.3.2. Physical Capability
4.3.3. Physical Opportunity
“Due to the legislation regarding young people under the age of 18, smoking has been relocated [from the school premises] to public roads. Smoking is not allowed on school premises. But luckily you can still go outside to smoke. But besides that, I don’t have any impression that anything is being done here.”
4.3.4. Social Opportunity
“It is frustrating that it is easy to socialize if you smoke. Enrolling in a new school, the non-smokers stand in each corner, and don’t know where to go. It is much easier to get new friends, if you are a smoker, when you enrol in a new school.”
“There is social pressure, i.e., if you have a dominant group in class that you look up to, it affects whether you smoke or not, because you want to be part of that group.”
4.3.5. Reflective Motivation
4.3.6. Automatic Motivation
4.4. Steps 5 and 6: Identification of Intervention Functions and Policy Categories
4.5. Step 7: Identification of Behaviour Change Techniques (BCTs)
4.6. Step 8: Identification of the Mode of Delivery
4.6.1. School Environmental Component: School Tobacco Policy
4.6.2. Class-Based Component: Walk and Talks
4.6.3. Class-Based Component: Quit and Win Competition Based on Measurements of Carbon Monoxide Levels
4.6.4. Individual-Based Component: Access to Smoking Cessation Support
5. Feasibility Testing and Subsequent Intervention Refinement
5.1. Smoke-Free School Tobacco Policy
“... they interpreted the smoke-free school time differently, i.e., when does the school open (is that when you meet in the morning or do we uphold official hours?) and likewise, when a lecture ends, is the school closed then? It may be [closed] even if you’re doing group work [in the evening].”
5.2. Class-Based Component: Walk and Talks
“It didn’t go very well when we walked around by ourselves, because then we’d just talk, like half a minute per question, and then we went back up [to the classroom]. But when for example you [a researcher] went along, then we would talk a lot about it, and more and more questions would come up, and then we would actually talk more about it [the assigned topic].”
“I find it really ironic, that when we are going to do a non-smoking thing, then why does half of the class light up cigarettes, it’s because no one is checking up on us. […] So, I think it should be more structured.”
5.3. Class-Based Component: Quit and Win Competition
“If someone told me ‘you won’t get anything if you do this’, then I wouldn’t do anything. Because today, you have to get something to do something. So, if someone told me that ‘you won’t get anything if you do this [stop/reduce smoking]’, then there wouldn’t be any benefits to gain from it.”
“I mean even though there wasn’t a competition about a bowling trip, I still think it could be fun to see if your CO levels went down. And to sort of see if there was any change. That would be a challenge to yourself, to see how much you could get the number down.”
“That you started out measuring the CO levels (…) it was very good that you started with that. Because then all the smokers could start out seeing, that it really has an effect on us, that we’re smoking.”
“Well, I think that it’s a cool concept. That it’s a bit of competition, you think you want to be better than the others or something silly like ‘we’re gonna take them down’ (laughing), I think that’s cool. But I can’t do much because I don’t smoke, so I can’t really be that person that helps.”
5.4. Individual-Based Component: Access to Smoking Cessation Support
“If I was determined to quit, I think it would be helpful. But it depends on yourself. If I had decided ‘Okay, I need to quit now’ then I believe it could help me, that it could give me that extra boost. And if you did it together with a group.”
6. Final Intervention
7. Discussion
8. Future Directions
9. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Reitsma, M.B.; Kendrick, P.J.; Ababneh, E.; Abbafati, C.; Abbasi-Kangevari, M.; Abdoli, A.; Abedi, A.; Abhilash, E.S.; Abila, D.B.; Aboyans, V.; et al. Spatial, temporal, and demographic patterns in prevalence of smoking tobacco use and attributable disease burden in 204 countries and territories, 1990–2019: A systematic analysis from the Global Burden of Disease Study 2019. Lancet 2021, 397, 2337–2360. [Google Scholar] [CrossRef] [PubMed]
- National Center for Chronic Disease Prevention and Health Promotion. Reports of the Surgeon General. In Preventing Tobacco Use among Youth and Young Adults: A Report of the Surgeon General; Centers for Disease Control and Prevention (US): Atlanta, GA, USA, 2012. [Google Scholar]
- Barrington-Trimis, J.L.; Braymiller, J.L.; Unger, J.B.; McConnell, R.; Stokes, A.; Leventhal, A.M.; Sargent, J.D.; Samet, J.M.; Goodwin, R.D. Trends in the Age of Cigarette Smoking Initiation among Young Adults in the US from 2002 to 2018. JAMA Netw. Open 2020, 3, e2019022. [Google Scholar] [CrossRef] [PubMed]
- Prokhorov, A.V.; Winickoff, J.P.; Ahluwalia, J.S.; Ossip-Klein, D.; Tanski, S.; Lando, H.A.; Moolchan, E.T.; Muramoto, M.; Klein, J.D.; Weitzman, M.; et al. Youth Tobacco Use: A Global Perspective for Child Health Care Clinicians. Pediatrics 2006, 118, e890–e903. [Google Scholar] [CrossRef]
- World Health Organization Regional Office for Europe. European Tobacco Use: Trends Report 2019; World Health Organization Regional Office for Europe: Copenhagen, Denmark, 2019. [Google Scholar]
- Sussman, S.; Arriaza, B.; Grigsby, T.J. Alcohol, Tobacco, and Other Drug Misuse Prevention and Cessation Programming for Alternative High School Youth: A Review. J. Sch. Health 2014, 84, 748–758. [Google Scholar] [CrossRef] [PubMed]
- Ringgaard, L.; Heinze, C.; Andersen, N.; Hansen, G.; Hjort, A.; Klinker, C. UNG19—Sundhed Og Trivsel På Erhvervsuddannelser 2019 [YOUTH19—Health and Well-Being at Vocational Schools 2019]; Steno Diabetes Centre Copenhagen, Danish Heart Foundation, and Danish Cancer Society: Copenhagen, Denmark, 2020. [Google Scholar]
- Pisinger, V.S.C.; Thorsted, A.; Jezek, A.H.; Jørgensen, A.; Christensen, A.I.; Tolstrup, J.S.; Thygesen, L.C. The Danish National Youth Study 2019: Study design and participant characteristics. Scand. J. Public Health 2022, 50, 323–332. [Google Scholar] [CrossRef]
- Pisinger, V.; Mikkelsen, S.S.; Bendtsen, P.; Egan, K.K.; Tolstrup, J.S. The Danish National Youth Study 2014: Study design, population characteristics and non-response analysis. Scand. J. Public Health 2020, 48, 224–232. [Google Scholar] [CrossRef]
- Teng, A.; Blakely, T.; Atkinson, J.; Kalėdienė, R.; Leinsalu, M.; Martikainen, P.T.; Rychtaříková, J.; Mackenbach, J.P. Changing social inequalities in smoking, obesity and cause-specific mortality: Cross-national comparisons using compass typology. PLoS ONE 2020, 15, e0232971. [Google Scholar] [CrossRef]
- Villanti, A.C.; Niaura, R.S.; Abrams, D.B.; Mermelstein, R. Preventing Smoking Progression in Young Adults: The Concept of Prevescalation. Prev. Sci. 2019, 20, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Peirson, L.; Ali, M.U.; Kenny, M.; Raina, P.; Sherifali, D. Interventions for prevention and treatment of tobacco smoking in school-aged children and adolescents: A systematic review and meta-analysis. Prev. Med. 2016, 85, 20–31. [Google Scholar] [CrossRef]
- Poole, R.; Carver, H.; Anagnostou, D.; Edwards, A.; Moore, G.; Smith, P.; Wood, F.; Brain, K. Tobacco use, smoking identities and pathways into and out of smoking among young adults: A meta-ethnography. Subst. Abus. Treat. Prev. Policy 2022, 17, 24. [Google Scholar] [CrossRef]
- Vallata, A.; O’Loughlin, J.; Cengelli, S.; Alla, F. Predictors of Cigarette Smoking Cessation in Adolescents: A Systematic Review. J. Adolesc. Health 2021, 68, 649–657. [Google Scholar] [CrossRef] [PubMed]
- Jones, G. Youth; Polity: Cambridge, UK, 2009. [Google Scholar]
- Andersen, S.; Rod, M.; Ersbøll, A.; Stock, C.; Johansen, C.; Holmberg, T.; Zinckernagel, L.; Ingholt, L.; Sørensen, B.; Tolstrup, J. Effects of a settings-based intervention to promote student wellbeing and reduce smoking in vocational schools: A non-randomized controlled study. Soc. Sci. Med. 2016, 161, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Ingholt, L.; Sørensen, B.; Andersen, S.; Zinckernagel, L.; Friis-Holmberg, T.; Frank, V.; Stock, C.; Tjørnhøj-Thomsen, T.; Rod, M. How can we strengthen students’ social relations in order to reduce school dropout? An intervention development study within four Danish vocational schools. BMC Public Health 2015, 15, 502. [Google Scholar] [CrossRef]
- Andersen, S.; Pisinger, V.; Rod, M.H.; Tolstrup, J. Associations of school tobacco policies and legislation with youth smoking: A cross-sectional study of Danish vocational high schools. BMJ Open 2019, 9, e028357. [Google Scholar] [CrossRef]
- Jarlstrup, N.S.; Juel, K.; Pisinger, C.H.; Grønbæk, M.; Holm, S.; Andersen, S. International Approaches to Tobacco Use Cessation Programs and Policy in Adolescents and Young Adults: Denmark. Curr. Addict. Rep. 2018, 5, 42–53. [Google Scholar] [CrossRef]
- Coppo, A.; Galanti, M.R.; Giordano, L.; Buscemi, D.; Bremberg, S.; Faggiano, F. School policies for preventing smoking among young people. Cochrane Database Syst. Rev. 2014, 10, CD009990. [Google Scholar] [CrossRef]
- Hill, S.; Amos, A.; Clifford, D.; Platt, S. Impact of tobacco control interventions on socioeconomic inequalities in smoking: Review of the evidence. Tob. Control 2014, 23, e89–e97. [Google Scholar] [CrossRef]
- Fanshawe, T.R.; Halliwell, W.; Lindson, N.; Aveyard, P.; Livingstone-Banks, J.; Hartmann-Boyce, J. Tobacco cessation interventions for young people. Cochrane Database Syst. Rev. 2017, 11, CD003289. [Google Scholar] [CrossRef]
- Skivington, K.; Matthews, L.; Simpson, S.A.; Craig, P.; Baird, J.; Blazeby, J.M.; Boyd, K.A.; Craig, N.; French, D.P.; McIntosh, E.; et al. A new framework for developing and evaluating complex interventions: Update of Medical Research Council guidance. BMJ 2021, 374, n2061. [Google Scholar] [CrossRef]
- Michie, S.; van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef]
- Michie, S.; Atkins, L.; West, R. The Behaviour Change Wheel: A Guide to Designing Interventions; Silverback Publishing: Great Britain, UK, 2014. [Google Scholar]
- Cowdell, F.; Dyson, J. How is the theoretical domains framework applied to developing health behaviour interventions? A systematic search and narrative synthesis. BMC Public Health 2019, 19, 1180. [Google Scholar] [CrossRef] [PubMed]
- Cane, J.; O’Connor, D.; Michie, S. Validation of the theoretical domains framework for use in behaviour change and implementation research. Implement. Sci. 2012, 7, 37. [Google Scholar] [CrossRef]
- Ryan, R.M.; Deci, E.L. Intrinsic and extrinsic motivation from a self-determination theory perspective: Definitions, theory, practices, and future directions. Contemp. Educ. Psychol. 2020, 61, 101860. [Google Scholar] [CrossRef]
- Ryan, R.M.; Deci, E.L. Intrinsic and Extrinsic Motivations: Classic Definitions and New Directions. Contemp. Educ. Psychol. 2000, 25, 54–67. [Google Scholar] [CrossRef] [PubMed]
- Ntoumanis, N.; Ng, J.Y.Y.; Prestwich, A.; Quested, E.; Hancox, J.E.; Thøgersen-Ntoumani, C.; Deci, E.L.; Ryan, R.M.; Lonsdale, C.; Williams, G.C. A meta-analysis of self-determination theory-informed intervention studies in the health domain: Effects on motivation, health behavior, physical, and psychological health. Health Psychol. Rev. 2021, 15, 214–244. [Google Scholar] [CrossRef]
- Williams, G.C.; Patrick, H.; Niemiec, C.P.; Ryan, R.M.; Deci, E.L.; Lavigne, H.M. The smoker’s health project: A self-determination theory intervention to facilitate maintenance of tobacco abstinence. Contemp. Clin. Trials 2011, 32, 535–543. [Google Scholar] [CrossRef]
- Craig, P.; Dieppe, P.; Macintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Developing and evaluating complex interventions: The new Medical Research Council guidance. Int. J. Nurs. Stud. 2013, 50, 587–592. [Google Scholar] [CrossRef]
- Campbell, M.; Fitzpatrick, R.; Haines, A.; Kinmonth, A.L.; Sandercock, P.; Spiegelhalter, D.; Tyrer, P. Framework for design and evaluation of complex interventions to improve health. BMJ Br. Med. J. 2000, 321, 694–696. [Google Scholar] [CrossRef]
- Michie, S.; Hyder, N.; Walia, A.; West, R. Development of a taxonomy of behaviour change techniques used in individual behavioural support for smoking cessation. Addict. Behav. 2011, 36, 315–319. [Google Scholar] [CrossRef]
- Elffers, L.; Oort, F.J.; Karsten, S. Making the connection: The role of social and academic school experiences in students’ emotional engagement with school in post-secondary vocational education. Learn. Individ. Differ. 2012, 22, 242–250. [Google Scholar] [CrossRef]
- Rod, M.H.; Ingholt, L.; Bang Sørensen, B.; Tjørnhøj-Thomsen, T. The spirit of the intervention: Reflections on social effectiveness in public health intervention research. Crit. Public Health 2014, 24, 296–307. [Google Scholar] [CrossRef]
- Jones, L.; Somekh, B. Observation. In Theory and Methods in Social Research, 2nd ed.; Somekh, B., Lewin, C., Eds.; SAGE Publications Ltd.: London, UK, 2011; pp. 131–138. [Google Scholar]
- Hastrup, K.; Rubow, C.; Tjørnhøj-Thomsen, T. Kulturanalyse—Kort Fortalt; Samfundslitteratur: Frederiksberg, Denmark, 2011. [Google Scholar]
- Stewart, D.W.; Shamdasani, P.N.; Rook, D.W. Focus Groups: Theory and Practice, 2nd ed.; SAGE Publications, Ltd.: Thousand Oaks, CA, USA, 2007. [Google Scholar] [CrossRef]
- Halkier, B. Focus groups as social enactments: Integrating interaction and content in the analysis of focus group data. Qual. Res. 2010, 10, 71–89. [Google Scholar] [CrossRef]
- Malterud, K. Systematic text condensation: A strategy for qualitative analysis. Scand. J. Public Health 2012, 40, 795–805. [Google Scholar] [CrossRef] [PubMed]
- Andersen, S.; Riis, N.; Nygart, V.; Hansen, G.; Pisinger, C. Rygning På Erhvervsskoler: Det Skal Være Federe at Være Ikkeryger [Smoking at Vocational Schools: It Should Be More Cool Not to Smoke]; Vidensråd for Forebyggelse: Copenhagen, Denmark, 2018. [Google Scholar]
- Begh, R.; Lindson-Hawley, N.; Aveyard, P. Does reduced smoking if you can’t stop make any difference? BMC Med. 2015, 13, 257. [Google Scholar] [CrossRef]
- Coban, F.R.; Kunst, A.E.; Van Stralen, M.M.; Richter, M.; Rathmann, K.; Perelman, J.; Alves, J.; Federico, B.; Rimpelä, A.; Lorant, V.; et al. Nicotine dependence among adolescents in the European Union: How many and who are affected? J. Public Health 2018, 41, 447–455. [Google Scholar] [CrossRef]
- Solberg, L.I.; Boyle, R.G.; McCarty, M.; Asche, S.E.; Thoele, M.J. Young adult smokers: Are they different? Am. J. Manag. Care 2007, 13, 626. [Google Scholar]
- McCarthy, M.; Siahpush, M.; Shaikh, R.A.; Sikora Kessler, A.; Tibbits, M. Social Disparities in Unaided Quit Attempts among Daily Current and Former Smokers: Results from the 2010–2011 Tobacco Use Supplement to the Current Population Survey. Nicotine Tob. Res. 2016, 18, 1705–1710. [Google Scholar] [CrossRef] [PubMed]
- Heinz, A.J.; Kassel, J.D.; Berbaum, M.; Mermelstein, R. Adolescents’ expectancies for smoking to regulate affect predict smoking behavior and nicotine dependence over time. Drug Alcohol Depend. 2010, 111, 128–135. [Google Scholar] [CrossRef]
- Bader, P.; Travis, H.E.; Skinner, H.A. Knowledge synthesis of smoking cessation among employed and unemployed young adults. Am. J. Public Health 2007, 97, 1434–1443. [Google Scholar] [CrossRef]
- Matkin, W.; Ordóñez-Mena, J.M.; Hartmann-Boyce, J. Telephone counselling for smoking cessation. Cochrane Database Syst. Rev. 2019, 5, CD002850. [Google Scholar] [CrossRef]
- Pbert, L.; Druker, S.; DiFranza, J.R.; Gorak, D.; Reed, G.; Magner, R.; Sheetz, A.H.; Osganian, S. Effectiveness of a School Nurse–Delivered Smoking-Cessation Intervention for Adolescents. Pediatrics 2011, 128, 926–936. [Google Scholar] [CrossRef] [PubMed]
- Stead, L.F.; Perera, R.; Lancaster, T. A systematic review of interventions for smokers who contact quitlines. Tob. Control 2007, 16, i3–i8. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014, 348, g1687. [Google Scholar] [CrossRef] [PubMed]
- Kuipers, M.A.G.; de Korte, R.; Soto, V.E.; Richter, M.; Moor, I.; Rimpelä, A.H.; Perelman, J.; Federico, B.; Kunst, A.E.; Lorant, V. School smoking policies and educational inequalities in smoking behaviour of adolescents aged 14–17 years in Europe. J. Epidemiol. Community Health 2016, 70, 132–139. [Google Scholar] [CrossRef] [PubMed]
- Mélard, N.; Grard, A.; Robert, P.-O.; Kuipers, M.A.G.; Schreuders, M.; Rimpelä, A.H.; Leão, T.; Hoffmann, L.; Richter, M.; Kunst, A.E.; et al. School tobacco policies and adolescent smoking in six European cities in 2013 and 2016: A school-level longitudinal study. Prev. Med. 2020, 138, 106142. [Google Scholar] [CrossRef]
- Evans-Whipp, T.; Beyers, J.M.; Lloyd, S.; Lafazia, A.N.; Toumbourou, J.W.; Arthur, M.W.; Catalano, R.F. A review of school drug policies and their impact on youth substance use. Health Promot. Int. 2004, 19, 227–234. [Google Scholar] [CrossRef]
- Schreuders, M.; Nuyts, P.A.W.; van den Putte, B.; Kunst, A.E. Understanding the impact of school tobacco policies on adolescent smoking behaviour: A realist review. Soc. Sci. Med. 2017, 183, 19–27. [Google Scholar] [CrossRef]
- Schreuders, M.; van den Putte, B.; Kunst, A.E. Smoke-free school policies in Europe: Challenges for the future. Prev. Med. 2020, 138, 106130. [Google Scholar] [CrossRef]
- Wells, J.; Barlow, J.; Stewart-Brown, S. A systematic review of universal approaches to mental health promotion in schools. Health Educ. 2003, 103, 197–220. [Google Scholar] [CrossRef]
- Clarke, A.M. Implementing Universal and Targeted Mental Health Promotion Interventions in Schools. In Implementing Mental Health Promotion; Barry, M.M., Clarke, A.M., Petersen, I., Jenkins, R., Eds.; Springer International Publishing: Cham, Switzerland, 2019; pp. 341–385. [Google Scholar]
- Villanti, A.C.; West, J.C.; Klemperer, E.M.; Graham, A.L.; Mays, D.; Mermelstein, R.J.; Higgins, S.T. Smoking-Cessation Interventions for U.S. Young Adults: Updated Systematic Review. Am. J. Prev. Med. 2020, 59, 123–136. [Google Scholar] [CrossRef]
- Suls, J.M.; Luger, T.M.; Curry, S.J.; Mermelstein, R.J.; Sporer, A.K.; An, L.C. Efficacy of Smoking-Cessation Interventions for Young Adults: A Meta-Analysis. Am. J. Prev. Med. 2012, 42, 655–662. [Google Scholar] [CrossRef] [PubMed]
- Duncan, E.; O’Cathain, A.; Rousseau, N.; Croot, L.; Sworn, K.; Turner, K.M.; Yardley, L.; Hoddinott, P. Guidance for reporting intervention development studies in health research (GUIDED): An evidence-based consensus study. BMJ Open 2020, 10, e033516. [Google Scholar] [CrossRef] [PubMed]
- O’Cathain, A.; Croot, L.; Sworn, K.; Duncan, E.; Rousseau, N.; Turner, K.; Yardley, L.; Hoddinott, P. Taxonomy of approaches to developing interventions to improve health: A systematic methods overview. Pilot Feasibility Stud. 2019, 5, 41. [Google Scholar] [CrossRef] [PubMed]
- Bartholomew, L.; Parcel, G.; Kok, G.; Gottlieb, N.; Fernandez, M. Planning Health Promotion Programmes. An Intervention Mapping Approach; Jossey Bass: San Francisco, CA, USA, 2011. [Google Scholar]


{kind=link}
| Observations | Student Focus Groups (Number of Students) | School Staff Interviews | Workshops | |
|---|---|---|---|---|
| BCW stage 1: | ||||
| School 1 | 5 days | 1 (7) | 3 | |
| School 2 | 4 days | 1 (7) | 1 | |
| School 3 | 4 days | 1 (4) | 1 | |
| School 4 | 3 days | 1 (2) | 1 | |
| School 5–6 | 4 a | |||
| School 7–9 | 1 b | |||
| Feasibility studies: | ||||
| School 10 | 1 day | 1 (7) | 3 | |
| School 11 | 1 day | 1 (8) | 3 | |
| School 12 | 2 (10) | |||
| School 13 | 1 c |
| COM-B | TDF | What Needs to Change | Intervention Functions (Policy Category) | BCW Techniques (BCW no.) | Intervention Elements |
|---|---|---|---|---|---|
| Psychological Capability | Knowledge | Students need to know how to receive smoking cessation support, and what are the benefits of the counselling | Education (C) | Instruction on how to perform a behaviour (4.1) | Information about the national Quitline in the edutainment session, and on posters. |
| Knowledge | Students need to know about the impact of nicotine dependence | Education (C) | Information about antecedents (4.2), Information about health consequences (5.1) | Information in the edutainment session and the teaching material. | |
| Behaviour regulation | Students need to improve their self-regulatory ability and monitor their effort | Enablement Education Persuasion (C, E, S) | Biofeedback (2.6), Social support (unspecified) (3.1), Behavioural practice/rehearsal (8.1) | Class-based competition with carbon monoxide breath readings. | |
| Physical Capability | Skills | Students with nicotine dependence/craving need to be physically capable of not smoking | Education Enablement (S) | Instruction on how to perform a behaviour (4.1) Behaviour substitution (8.2) | Advice by/talks with staff who have been trained on the staff course. The national Quitline service adapted to VET students. |
| Physical Opportunity | Environmental context and resources | Students need to have access to smoking cessation services and support at school | Enablement Environmental restructuring (E) | Instruction on how to perform a behaviour (4.1) | Information in the edutainment session and posters at school on how to contact the national Quitline. Staff trained in having dialogue with students. |
| Environmental context and resources | Schools need to make smoking more difficult on school premise and close to the school | Restriction (R) | Restructuring the social environment (12.2.) | Implementation of a comprehensive school tobacco policy, where students, staff, and visitors are not allowed to smoke during school. | |
| Social Opportunity | Social influences | Students need a supportive social environment at school and to alter the perception that smoking is the social norm, or not feel obligated to adhere to the perceived norm. | Enablement Environmental restructuring Modelling (C, E) | Social support (unspecified) (3.1.), Demonstration of the behaviour (6.1), Social comparison (6.2), Information about others’ approval (6.3), Habit transformation (8.3) | School tobacco policy and quit-and-win competition: experiencing others who do not want to initiate smoking or want to quit. The teaching material: correcting misperceptions of overestimation of smoking prevalence; student involvement in class ethos and creating social activities in breaks. |
| Reflective motivation | Social role and identity | Students need to minimise their perception of smoking as part of their social engagement at school and their identity as being young | Education Persuasion (C, E) | Identification of self as a role model (13.1), Framing/reframing (13.2) | The teaching material: for example, discussing the responsibility of being a role model for younger students; how smoking is influenced by, e.g., family, friends, school, legislation, the tobacco industry |
| Beliefs about consequences | Students need to have fewer positive beliefs about the psychological and social benefits of smoking | Education Persuasion (C, E) | Information about social and environmental consequences (5.3) Information about emotional consequences (5.6) | The teaching material: addressing beliefs about benefits of smoking. | |
| Beliefs about capabilities | Students need to correct their belief that they can quit at any time without assistance | Education Persuasion (C, E) | Framing/reframing (13.2) | Edutainment session and teaching material: smoking reframed as an addiction, not a choice. | |
| Intentions | Students need to increase awareness of the negative effect of smoking on their body and be encouraged to reduce smoking | Incentivisation (C, S) | Biofeedback (2.6) | Monitor the students carbon monoxide levels twice. | |
| Goals | Students need to have a vision of what they achieve by reducing smoking | Education Training (S) | Goal setting (behaviour) (1.1.), Goal setting (outcome) (1.3.) | By participating in the competition, the students want to reduce own level of carbon monoxide. | |
| Automatic motivation | Reinforcement | Students need to change their perception of smoking as a habit in their daily school life | Environmental restructuring Restriction (E, R) | Restructuring the physical environment (12.1), Restructuring the social environment (12.2), Behavioural practice/rehearsal (8.1), Habit formation (8.3) | School tobacco policy: encouraging habit formation, changing the habit during breaks, commitment not to smoke during school, creating fear of being caught for violating the policy. |
| Reinforcement | Students need to have a tangible encouragement to reduce smoking | Incentivisation (S) | Incentive (outcome) (10.8), reward (outcome) (10.10) | Competition and the prize: rehearsal, creating expectation of rewards, celebrating wins. | |
| Emotion | Some students experience that they need smoking to cope with stressful situations. | Education Persuasion (E) | Social support (emotional) (3.3.), Information about emotional consequences (5.6), Reduce negative emotions (11.2), Framing/reframing (13.2) | Support from staff. The teaching material: discussing beliefs about psychological benefits of smoking and how to tackle stress. |
| Checklist Item | Item Description |
|---|---|
| Name | Focus: a school-based multicomponent intervention focusing on reducing smoking in the school environment for vocational education and training (VET). |
| Why | Danish VET schools have a high number of students who smoke. |
| What a |
|
| Who provided |
|
| Where | The intervention itself occurred in school during school hours. The staff course took place at the University of Southern Denmark. |
| When and how much |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andersen, S.; Holt, D.H.; Vinther, J.L.; Danielsen, D.; Jakobsen, G.S.; Holmberg, T.; Jensen, M.P.; Pisinger, C.; Krølner, R.F. Development and Feasibility Test of a Theory- and Evidence-Based Multicomponent Intervention to Reduce Student Smoking at Danish Vocational Schools. Youth 2023, 3, 715-736. https://doi.org/10.3390/youth3020047
Andersen S, Holt DH, Vinther JL, Danielsen D, Jakobsen GS, Holmberg T, Jensen MP, Pisinger C, Krølner RF. Development and Feasibility Test of a Theory- and Evidence-Based Multicomponent Intervention to Reduce Student Smoking at Danish Vocational Schools. Youth. 2023; 3(2):715-736. https://doi.org/10.3390/youth3020047
Chicago/Turabian StyleAndersen, Susan, Ditte H. Holt, Johan L. Vinther, Dina Danielsen, Gitte S. Jakobsen, Teresa Holmberg, Marie P. Jensen, Charlotta Pisinger, and Rikke F. Krølner. 2023. "Development and Feasibility Test of a Theory- and Evidence-Based Multicomponent Intervention to Reduce Student Smoking at Danish Vocational Schools" Youth 3, no. 2: 715-736. https://doi.org/10.3390/youth3020047
APA StyleAndersen, S., Holt, D. H., Vinther, J. L., Danielsen, D., Jakobsen, G. S., Holmberg, T., Jensen, M. P., Pisinger, C., & Krølner, R. F. (2023). Development and Feasibility Test of a Theory- and Evidence-Based Multicomponent Intervention to Reduce Student Smoking at Danish Vocational Schools. Youth, 3(2), 715-736. https://doi.org/10.3390/youth3020047