
Knowledge, Attitude, and Practices of Food Hygiene among Mothers from Rural Communities in Malawi

 , , , , , , , and
, , , , , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Study Population
2.3. Sample Size Determination and Sampling Procedure
2.4. Data Collection Instrument and Method
2.5. Determination of Knowledge, Attitude, and Practice Regarding Food Safety and FBDs
2.6. Statistical Analysis
3. Results
3.1. Socio-Demographic Characteristics of the Mothers
3.2. Knowledge Regarding BVP and Molds/Mycotoxins
3.3. Attitude of the Mothers Regarding BVPs and Moulds/Mycotoxins
3.4. Practices Regarding BVPs and Molds/Mycotoxins
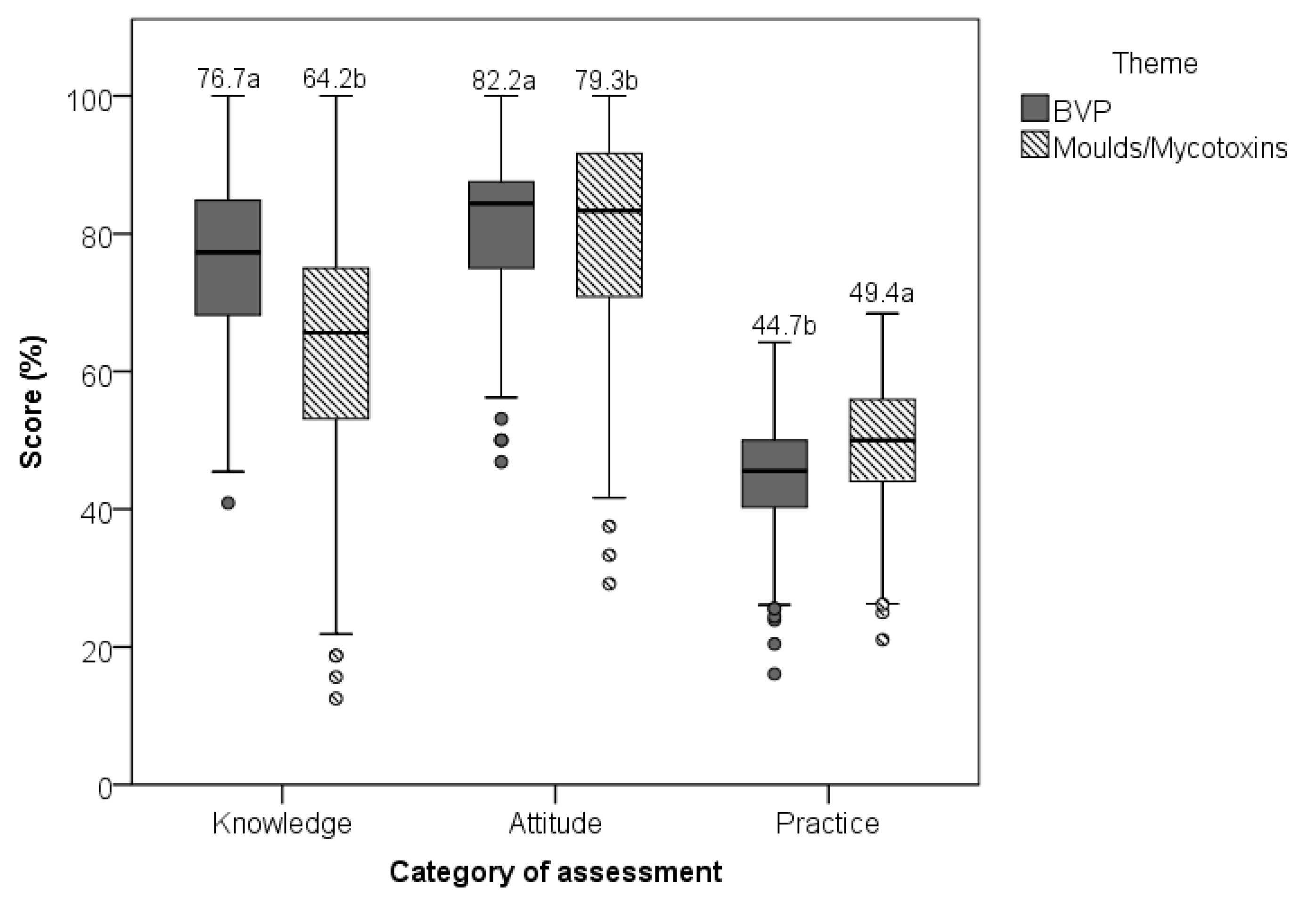
3.5. Overall Assessment of KAP of Mothers Regarding BVPs and Molds/Mycotoxins
3.6. Determinants for Mothers’ Practices Related to BVPs and Molds/Mycotoxins
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Havelaar, A.H.; Kirk, M.D.; Torgerson, P.R.; Gibb, H.J.; Hald, T.; Lake, R.J.; World Health Organization Foodborne Disease Burden Epidemiology Reference Group. World Health Organization Global Estimates and Regional Comparisons of the Burden of Foodborne Disease in 2010. PLoS Med. 2015, 12, e1001923. [Google Scholar] [CrossRef] [PubMed]
- Pires, S.M.; Devleesschauwer, B. Estimates of global disease burden associated with foodborne pathogens. In Foodborne Infections and Intoxications; Academic Press: Cambridge, MA, USA, 2021; pp. 3–17. [Google Scholar]
- WHO. WHO Steps up Action to Improve Food Safety and Protect People from Disease. 7 June 2021. Available online: https://www.who.int/news/item/07-06-2021-who-steps-up-action-to-improve-food-safety-and-protect-people-from-disease (accessed on 22 January 2024).
- Oduoye, M.O.; Akilimali, A.; Karim, K.A.; Moradeyo, A.A.; Abdullahi, Z.Z.; Muzata, D.; Christopher, G.U.; Chipinga, J.; Simiyu, B.W.; Isiko, I. Diseases Transmitted to Humans through Foodborne Microbes in the Global South. In Food Safety and Quality in the Global South; Springer Nature: Singapore, 2024; pp. 561–597. [Google Scholar]
- Kirk, M.D.; Pires, S.M.; Black, R.E.; Caipo, M.; Crump, J.A.; Devleesschauwer, B.; Döpfer, D.; Fazil, A.; Fischer-Walker, C.L.; Angulo, F.J. World Health Organization estimates of the global and regional disease burden of 22 foodborne bacterial, protozoal, and viral diseases, 2010: A data synthesis. PLoS Med. 2015, 12, e1001921. [Google Scholar]
- Gruber-Dorninger, C.; Jenkins, T.; Schatzmayr, G. Global mycotoxin occurrence in feed: A ten-year survey. Toxins 2019, 11, 375. [Google Scholar] [CrossRef] [PubMed]
- Matumba, L.; Namaumbo, S.; Ngoma, T.; Meleke, N.; De Boevre, M.; Logrieco, A.F.; De Saeger, S. Five keys to prevention and control of mycotoxins in grains: A proposal. Glob. Food Secur. 2001, 30, 100562. [Google Scholar] [CrossRef]
- Matumba, L.; Van Poucke, C.; Njumbe Ediage, E.; De Saeger, S. Keeping mycotoxins away from the food: Does the existence of regulations have any impact in Africa? Crit. Rev. Food Sci. Nutr. 2017, 57, 1584–1592. [Google Scholar] [CrossRef]
- Redmond, E.C.; Griffith, C.J. The importance of hygiene in the domestic kitchen: Implications for preparation and storage of food and infant formula. Perspect. Public Health 2009, 129, 69–76. [Google Scholar] [CrossRef]
- Byrd-Bredbenner, C.; Berning, J.; Martin-Biggers, J.; Quick, V. Food safety in home kitchens: A synthesis of the literature. Int. J. Environ. Res. Public Health 2013, 10, 4060–4085. [Google Scholar] [CrossRef]
- World Health Organization. Five Keys to Safer Food Manual; WHO: Geneve, Switzerland, 2012. Available online: https://www.who.int/publications/i/item/five-keys-to-safer-food-manual (accessed on 8 November 2023).
- Davis, T.P.; Wetzel, C.; Avilan, E.H.; de Mendoza Lopes, C.; Chase, R.P.; Winch, P.J.; Perry, H.B. Reducing child global undernutrition at scale in Sofala Province, Mozambique, using Care Group Volunteers to communicate health messages to mothers. Glob. Health Sci. Pract. 2013, 1, 35–51. [Google Scholar] [CrossRef]
- Geresomo, N.C.; Mbuthia, E.K.; Matofari, J.W.; Mwangwela, A.M. Targeting caregivers with context specific behavior change training increased uptake of recommended hygiene practices during food preparation and complementary feeding in Dedza district of Central Malawi. Ecol. Food Nutr. 2018, 57, 301–313. [Google Scholar] [CrossRef]
- Coates, J.; Swindale, A.; Bilinsky, P. Household Food Insecurity Access Scale (HFIAS) for Measurement of Food Access: Indicator Guide, 3rd ed.; Academy for Educational Development: Washington, DC, USA, 2007. [Google Scholar]
- Demberere, T.; Chidziya, T.; Ncozana, T.; Manyeruke, N. Knowledge and practices regarding water, sanitation and hygiene (WASH) among mothers of under-fives in Mawabeni, Umzingwane District of Zimbabwe. Phys. Chem. Earth Part A/B/C 2016, 92, 119–124. [Google Scholar] [CrossRef]
- Todd, E.C.; Michaels, B.S.; Holah, J.; Smith, D.; Greig, J.D.; Bartleson, C.A. Outbreaks where food workers have been implicated in the spread of foodborne disease. Part 10. Alcohol-based antiseptics for hand disinfection and a comparison of their effectiveness with soaps. J. Food Prot. 2010, 73, 2128–2140. [Google Scholar] [CrossRef] [PubMed]
- Burton, M.; Cobb, E.; Donachie, P.; Judah, G.; Curtis, V.; Schmidt, W.P. The effect of handwashing with water or soap on bacterial contamination of hands. Int. J. Environ. Res. Public Health 2011, 8, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Luby, S.P.; Agboatwalla, M.; Feikin, D.R.; Painter, J.; Billhimer, W.; Altaf, A.; Hoekstra, R.M. Effect of handwashing on child health: A randomised controlled trial. Lancet 2005, 366, 225–233. [Google Scholar] [CrossRef] [PubMed]
- Luby, S.P.; Halder, A.K.; Huda, T.; Unicomb, L.; Johnston, R.B. The effect of handwashing at recommended times with water alone and with soap on child diarrhea in rural Bangladesh: An observational study. PLoS Med. 2011, 8, e1001052. [Google Scholar] [CrossRef]
- Lokossou, Y.U.A.; Tambe, A.B.; Azandjèmè, C.; Mbhenyane, X. Socio-cultural beliefs influence feeding practices of mothers and their children in Grand Popo, Benin. J. Health Popul. Nutr. 2021, 40, 33. [Google Scholar] [CrossRef]
- Napier, A.D.; Ancarno, C.; Butler, B.; Calabrese, J.; Chater, A.; Chatterjee, H.; Guesnet, F.; Horne, R.; Jacyna, S.; Jadhav, S.; et al. Culture and health. Lancet 2014, 384, 1607–1639. [Google Scholar] [CrossRef]
- Magamba, K.; Matumba, L.; Matita, G.; Gama, A.P.; Singano, L.; Monjerezi, M.; Njoroge, S.M. Aflatoxin risk management in commercial groundnut products in Malawi (Sub-Saharan Africa): A call for a more socially responsible industry. J. Consum. Prot. Food Saf. 2017, 12, 309–316. [Google Scholar] [CrossRef]
- Liao, Q.; Cowling, B.J.; Lam, W.W.T.; Fielding, R. The influence of social-cognitive factors on personal hygiene practices to protect against influenzas: Using modelling to compare avian A/H5N1 and 2009 pandemic A/H1N1 influenzas in Hong Kong. Int. J. Behav. Med. 2011, 18, 93–104. [Google Scholar] [CrossRef]
- Pereboom, M.T.; Manniën, J.; Spelten, E.R.; Schellevis, F.G.; Hutton, E.K. Observational study to assess pregnant women’s knowledge and behaviour to prevent toxoplasmosis, listeriosis and cytomegalovirus. BMC Pregnancy Childbirth 2013, 13, 98. [Google Scholar] [CrossRef]
- Bloomfield, S.; Ackerley, L. Developing better understanding of hygiene is key to developing hygiene behaviour change in home and everyday life settings. Perspect. Public Health 2023, 22, 17579139231163734. [Google Scholar] [CrossRef]
- Matumba, L.; Monjerezi, M.; Kankwamba, H.; Njoroge, S.M.C.; Ndilowe, P.; Kabuli, H.; Kambewa, D.; Njapau, H. Knowledge, attitude, and practices concerning presence of molds in foods among members of the general public in Malawi. Mycotoxin Res. 2016, 32, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Martey, E.; Al-Hassan, R.M.; Kuwornu, J.K. Commercialization of smallholder agriculture in Ghana: A Tobit regression analysis. Afr. J. Agric. Res. 2012, 7, 2131–2141. [Google Scholar]
- Grace, D. Food safety in low- and middle-income countries. Int. J. Environ. Res. Public Health 2015, 12, 10490–10507. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Item | n (%) | |
|---|---|---|
| Age group of respondents | Under 25 | 177 (33.9) |
| 26–35 | 174 (33.3) | |
| 36–45 | 108 (20.7) | |
| Above 46 | 63 (12.1) | |
| Respondent’s household status | Household head | 155 (29.7) |
| Spouse | 345 (66.1) | |
| Child | 21 (4.2) | |
| Education of respondent | No formal education | 76 (14.6) |
| Attempted primary school | 394(75.5) | |
| Attempted secondary school | 52 (10.0) | |
| Role of the respondents in the village | Ordinary member | 434 (83.1) |
| Lead farmer | 4 (0.8) | |
| Local leader | 10 (1.9) | |
| Care group member | 29 (5.6) | |
| Care group promoter | 31 (5.9) | |
| Cluster leader | 14 (2.7) | |
| Household membership | 1–4 | 228 (43.7) |
| 5–7 | 230 (44.1) | |
| 8+ | 64 (12.3) | |
| Household food insecurity access score | Secure (0–1) | 91 (17.4) |
| Mildly food insecure (2–7) | 111 (21.3) | |
| Moderately food insecure (8–14) | 139 (26.6) | |
| Severely food insecure (15–27) | 181 (34.7) | |
| Main material for house walls | Leaves, tree poles, bamboo | 12 (2.3) |
| Mud and poles or stones | 148 (28.4) | |
| Mud bricks | 101 (19.3) | |
| Baked or burnt bricks | 254 (48.7) | |
| Concrete, cement, stone | 7 (1.3) | |
| Main material for floor | Earth | 448 (85.8) |
| Cement | 74 (14.2) | |
| Main material for roof | Grass, leaves, bamboo | 294 (56.3) |
| Galvanized metal sheets/iron sheets | 228 (43.7) | |
| Toilet | Unproved simple pit latrine | 417 (79.9) |
| Improved simple pit latrine | 56 (10.7) | |
| No toilet | 49 (9.4) | |
| Toilet with drop hole cover | 212 (40.6) | |
| Toilet with a functional tip-tap/hand-washing facility | 63 (12.1) | |
| Have a kitchen | 316 (60.5) | |
| Kitchen with a proper door | 112 (21.5) | |
| Spend 30+ min to obtain domestic water and come back during the dry season | 61 (11.7) | |
| Spend 30+ min to obtain domestic water and come back during the rainy season | 54 (10.1) | |
| Houses with non-leaking roof | 220 (42.1) | |
| Keep livestock in the kitchen/household | 156 (29.9) | |
| Have a refuse pit | 141 (27.0) | |
| Knowledge Aspect | n (%) |
|---|---|
| Unaware that hand washing without soap is insufficient to eliminate BVP, even when performed over an extended duration | 172 (33) |
| Believed that the safety of water could be determined by its visual appearance | 322 (61.7) |
| Mothers were uninformed about the health risks associated with consuming milk directly from an animal | 263 (50.4) |
| Unaware that feces from seemingly healthy-looking infants posed diseases-related risks | 130 (24.9) |
| Unaware that the presence of weeds in a field could contribute to this issue. | 291(55.7) |
| Unaware that drought promotes mold infestation | 245 (47.1) |
| Unaware that late planting promotes mold growth | 238 (45.7) |
| Unaware that late planting and leaving crops in the field for an extended period after attaining physiological maturity and field and storage pests are conditions conducive to mold growth | 128 (24.7) |
| Incorrectly thought that normal heating, e.g., boiling, is capable of destroying mold toxins and making the food safe | 280 (53.7) |
| Incorrectly thought that soaking moldy grains in water for a couple of days would remove mold toxins | 235 (45.0) |
| Unaware that moldy foodstuff has the potential to cause death instantly or within a couple of days or weeks if consumed in large amounts | 293 (56.1) |
| Unaware that moldy foodstuffs have the potential to induce congenital disabilities | 262 (50.2) |
| Unaware that moldy foodstuffs have the potential to affect child growth negatively | 180 (34.5) |
| Unaware that mouldy foodstuffs have the potential to depress one’s immunity | 178 (34.1) |
| Attitude Aspect | n (%) |
|---|---|
| Disagreed that washing hands with soap was wasteful | 479 (91.8) |
| Found it culturally unacceptable to request handwashing with running/pouring water when others used a shared bucket | 155 (29.7) |
| Felt it was unethical to ask for soap for handwashing at someone’s home or in public | 156 (29.9) |
| Believed good hygiene practices were nearly impossible for households with limited resources | 247 (47.3) |
| Found it unethical to dispose of moldy food when others were in need | 142 (27.2) |
| Believed it was prudent to sort and sell the higher-quality portion while consuming the lower-quality fraction | 63 (12.1) |
| Expressed a strong willingness to change inappropriate practices | 518 (99.2) |
| Expressed concerns about the presence of molds in their food | 461 (88.3) |
| Concerned about the potential for associated foodborne diseases | 425 (81.4) |
| Agreed that sorting and removing moldy fractions from their foods was a worthwhile effort | 482 (92.3) |
| Practices | n (%) | |
|---|---|---|
| Inadequate Handwashing Practices | Inconsistent handwashing after using a toilet | 87 (16.7) |
| Inconsistent or no handwashing with soap after using the toilet | 467 (89.5) | |
| Inconsistent handwashing after changing baby nappies | 187 (35.8) | |
| Inconsistent handwashing after disposing of garbage | 353 (67.6) | |
| Inconsistent handwashing before cooking food | 277 (53.1) | |
| Soap usage | Inconsistent or no hand washing with soap after cleaning the house | 514 (98.5) |
| Inconsistent or no hand washing with soap after disposing of garbage | 508 (97.3) | |
| Inconsistent handwashing with soap before cooking food | 498 (95.4) | |
| Inconsistent or no soap usage before eating | 522 (100) | |
| Unhygienic Shared Bucket Usage | Dip shared bucket handwashing | 317 (60.7) |
| Use of a common bucket for various activities (kitchen and non-kitchen) | 168 (32.2) | |
| Unsanitary Utensil and Water Handling | Inconsistent use of soap for washing utensils | |
| Failure to keep drinking water covered | 105 (20.1) | |
| Contaminating drinking water by dipping a cup | 294 (56.3) | |
| Unsafe Food Handling Practices | Failure to use separate utensils for raw and cooked food | 218 (41.7) |
| Consuming cooked food after two hours of preparation | 318 (61.0) | |
| Unhealthy Infant Feeding Practices | Inconsistent handwashing before breastfeeding | 85 (16.3) |
| Rare usage of soap for washing infant feeding containers | 483 (92.5) | |
| Cooled porridge in the mouth before feeding babies | 137 (26.2) | |
| Negligent Mould Prevention Practices | Failure to plant with the first good rains | 254 (48.7) |
| Harvesting maize before maturity due to various reasons | 380 (72.8) | |
| Neglecting to check for moldy cobs during harvesting | 202 (38.7) | |
| Drying maize on bare soil | 300 (57.4) | |
| Lack of sorting maize before dehulling | 459 (88.0) | |
| Buying maize with noticeable mold | 518 (99.2) | |
| Factor | Practice Regarding Control of BVP | Practice Regarding Control of Molds/Mycotoxins | |||
|---|---|---|---|---|---|
| Coefficient | Std Error | Coefficient | Std Error | ||
| Mother’s age category (years) | 25 and below (Ref) | - | - | - | - |
| 26–35 | 0.0227 | 0.193 | −0.1452 | 0.199 | |
| 36–45 | 0.1914 | 0.237 | −0.0485 | 0.227 | |
| 46 and above | 0.0951 | 0.298 | −0.0687 | 0.289 | |
| Education level of the mother | No education (Ref) | - | - | - | - |
| Primary school incomplete | 0.2277 | 0.239 | 0.2135 | 0.242 | |
| Primary school complete | 0.1993 | 0.390 | 0.0723 | 0.392 | |
| Did not complete secondary school education | 0.7652 * | 0.361 | 0.4345 | 0.353 | |
| Completed secondary school education | 1.5268 * | 0.626 | 1.1334 | 0.669 | |
| Household headed by a female | −0.3063 | 0.168 | −0.2015 | 0.168 | |
| Number of household members | 0.0254 | 0.401 | 0.8000 * | 0.404 | |
| Household food insecurity access score | −0.0068 | 0.010 | −0.0114 | 0.010 | |
| Knowledge about BVP | 0.0396 * | 0.008 | |||
| Knowledge about molds/mycotoxins | 0.0065 | 0.005 | |||
| Attitude about BVP | 0.0384 * | 0.009 | 0.0362 * | 0.007 | |
| Attitude about molds/mycotoxins | - | - | 0.0362 * | 0.007 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Batch, V.; Kress, M.; Luhanga, E.; Monjerezi, M.; Pfaff, D.; Phiri, H.; Gama, A.P.; Chomanika, K.; Schmidt, A.; Duelken, B.; et al. Knowledge, Attitude, and Practices of Food Hygiene among Mothers from Rural Communities in Malawi. Hygiene 2024, 4, 361-373. https://doi.org/10.3390/hygiene4030028
Batch V, Kress M, Luhanga E, Monjerezi M, Pfaff D, Phiri H, Gama AP, Chomanika K, Schmidt A, Duelken B, et al. Knowledge, Attitude, and Practices of Food Hygiene among Mothers from Rural Communities in Malawi. Hygiene. 2024; 4(3):361-373. https://doi.org/10.3390/hygiene4030028
Chicago/Turabian StyleBatch, Vitowe, Martina Kress, Ezekiel Luhanga, Maurice Monjerezi, Daniel Pfaff, Horace Phiri, Aggrey Pemba Gama, Kelvin Chomanika, Anja Schmidt, Bianca Duelken, and et al. 2024. "Knowledge, Attitude, and Practices of Food Hygiene among Mothers from Rural Communities in Malawi" Hygiene 4, no. 3: 361-373. https://doi.org/10.3390/hygiene4030028
APA StyleBatch, V., Kress, M., Luhanga, E., Monjerezi, M., Pfaff, D., Phiri, H., Gama, A. P., Chomanika, K., Schmidt, A., Duelken, B., Jurisic, I., Mlangeni, A. T., Mikwamba, K., Chiutsi-Phiri, G., Corner, P. L., Kumwenda, S., Kaonga, C., Schwan, S., Kamndaya, M., & Matumba, L. (2024). Knowledge, Attitude, and Practices of Food Hygiene among Mothers from Rural Communities in Malawi. Hygiene, 4(3), 361-373. https://doi.org/10.3390/hygiene4030028