Abstract
Peer Victimization (PV) or being bullied in childhood/adolescence has been associated with several negative outcomes in mental health conditions beyond the time of its occurrence. However, its possible association with personality disorders has been slightly explored. In the present study we have compared the frequency of DSM IV personality disorders among adult patients with (N = 28) or without (N = 418) a reported history of PV. For this purpose, axis II was evaluated with the Self-Report Checklist for Preliminary Items for Major Categories, whereas self-esteem and self-assessment of functioning were evaluated with single questions. Patients with PV history have met the diagnostic criteria of the avoidant (60.7% vs. 12.2%), depressive (28.5% vs. 5.2%) and paranoid (17.9% vs. 5%) personality disorders more frequently than patients without history of PV. Moreover, these patients with antecedents of being bullied have also reported lower self-esteem (2 vs. 3) and in the assessment of social functioning (4 vs. 5). Our study indicated that there is a clear association between PV and avoidant, depressive and paranoid personality patterns. These results suggest that the stress related with the experience of PV threatens a basic psychobiological need such as social acceptance with implications for the beginning of long-term dysfunctional personality trajectories.
1. Introduction
The experience of Peer Victimization (PV) or being bullied is a form of childhood victimization that can be defined as aggressive behavior or intentional harm-doing by peers that happens repeatedly and involves an imbalance of power [1]. PV can have many manifestations, from direct physical harm to verbal taunts and threats; to exclusion, humiliation and rumor spreading and electronic harassment [2]. Approximately, 7–9% of the total school population might have suffered from bullying with some regularity at a particular time of their lives [3]. According to Nansel and colleagues [4] an average of 11% of children reported being victims of bullying. What is more, in the World Health Organization (WHO) report [5] rates ranged between 2–33% at ages of 10, 13 and 15 years in 43 countries. On the other hand, 14% of students reported being bullied in the 2019 status report Bullying in the United States Schools [6]. These data reflect the great magnitude of the problem.
Nonetheless, PV has been considered as a normal interactive pattern among youths and so not harmful [7] even though there are several studies showing that being bullied contributes to children’s symptoms of distress and early mental health problems developing [8]. Moreover, it has been concluded that victims of bullying suffer from a variety of feelings of psychological distress that include anxiety, social anxiety, depression, loneliness and negative feelings about themselves [9]. There is also evidence of its implication in somatic symptoms and health problems through its impact in the neuroendocrine system and related inflammatory processes [10].
The impact of PV during childhood/adolescence in mental health is not circumscribed to the context of its occurrence. Both cross-sectional and follow-up research indicate that is associated also with internalizing disorders such as anxiety, depression, somatization, low self-esteem or suicidal ideation and behavior in adulthood [3,11,12,13,14,15,16]. There is some evidence that indicate that this association could be higher than other forms of maltreatment [17]. Despite the fact that, as developmental psychopathology predicts [18], the impact of this type of experience may be mediated and/or moderated by several environmental and psychobiological factors [19,20,21,22,23,24], the outcome in adulthood has been related with the intensity or degree of bullying during childhood, meaning that more frequent, more severe or more chronical bullying resulted in a worse outcome [25]. Nonetheless, additional work is needed on this field to test whether being bullied contributes to other psychopathological outcomes in adulthood [8].
Despite its relevance in the origin of diverse mental health problems and its association with maladaptive personality traits such as being overly sensitive to critic evaluation, introversion, submissive and passive behavior and low self-esteem in child and adolescent victims [25], there is a notable lack of research on its association with personality disorders in adulthood even though these traits can have long-term continuity. Only a few investigations provide enough data that reflect the role of PV in childhood/adolescence and the borderline personality disorder in adults [26,27,28,29].
Personality disorders can be defined as a group of mental disorders characterized by deeply ingrained maladaptive patterns of inner experience and behavior that lead to significant distress or impairment in social, occupational and in other important areas of functioning. These disorders are usually recognizable by adolescence and may last during all life of the patients that suffer from them.
Theorists and clinicians in the field of personality disorders have highlighted the link between PV and the development of maladaptive personality disorders [30,31]. Therefore, PV might be on the origin of dysfunctional cognitive-affective schemas about the self and others [32] and, in a related way, biases in the social information processing [33]. Thus, the social pain that implies humiliation, rejection and devaluation by peers might leave an emotional scar that, unlike physical pain, lasts over time with negative consequences in the life trajectories at a personal and social level [34] On the other hand, the developmental period (middle childhood and adolescence), chronicity and the meaning of PV experience (thwart of the basic need of acceptance and belonging) could be understood as a class of toxic stress with potential neurobiological repercussions [35].
Based on all above mentioned, the objective of the study was to verify if there are differences between the two groups of patients (with or without reported antecedents of chronic PV along their childhood/adolescence) in the frequency and types of DSM IV personality disorders. Thus, we hypothesize that chronic PV may be associated with: (1) higher Structured Clinical Interview for DSM IV Axis II Personality disorders Questionnaire (SCID II-Q) scores and frequency of personality disorders with a high component of social anxiety and distrust as are the avoidant and paranoid personality disorders; (2) lower self-esteem, and (3) worse perception of social functioning.
2. Materials and Methods
2.1. Subjects
In our study we counted a total sample size of N = 446 patients, from whom twenty-eight patients (N = 28) reported being bullied during childhood/adolescence (history of PV) and N = 418 were considered as clinical controls (without history of PV).
2.2. Procedure
Recruitment took place between 2013 to 2015. Patients who began psychological treatment in a mental health unit were requested for participation and were given a written informed consent. The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board (or Ethics Committee) of Galicia Health Research Institute (IIS Galicia Sur, protocol code 2013/530). Inclusion criteria included patients between 18 and 50 years and that had at least completed the obligatory secondary education. Patients with neurological damage or intellectual disability were excluded from the study. Personal background data such as questions about the occurrence of PV throughout childhood/adolescence and other type of adversities were asked at the first clinical interview. Patients completed the Structured Clinical Interview for DSM IV Personality Disorders Questionnaire (SCID II-Q) at the end of the first clinical interview. Subsequently, the answers to the SCID II-Q were reviewed in consultation with the patients and compliance or not of the DSM-IV diagnostic criteria for each of the personality disorders was determined.
2.3. Instruments
Clinical interview for experiences of adversity in childhood-adolescence. In addition to other forms of adversity in childhood/adolescence (up to 17 years old), one of the areas explored was school experience. In this context, PV was defined as the repeated occurrence over prolonged periods of time of either verbal aggression (in form of insults, nicknames or threats) or physical aggression by other classmates. All these patients reported specific examples of these type of experience that had repeatedly occurred over long periods of time.
Structured Clinical Interview of DSM IV Personality Disorders (SCID II) [36]. The assessment of axis II psychopathology was based on the response of the subject to the SCID II-Q questionnaire [37]. The SCID II-Q includes items of all the criteria of the DSM IV personality disorders. For example, “do you often worry about being criticized or rejected in social situations?” in the avoidant personality disorder scale or “do you find that it is best not confide in others because they will use it against you?” in the paranoid personality disorder scale. All the questions are answered dichotomously (yes or not). There is evidence about the internal consistency of the SCID II-Q scales. For example, in one study in made in a large sample size [38] the Kuder-Richardson coefficient for the avoidant personality disorder scale was 0.70 and 0.73 for the paranoid personality disorder scale. After completion of the SCID II-Q, the affirmative questions on each of the personality disorder scales were reviewed with the patient, using the SCID II interview protocol [36], in order to assess the presence or absence of the reported characteristic.
Self-esteem was assessed with a single question “Do you feel you are a person worth at least on an equal basis with others?” employing a 5-point Likert-like scale. The five possible answers were: very much, much, moderate, a little and none.
Self-assessment of functioning evaluated three areas (general mood, social relationships and daily work or school) with a single question “How well you feel you are currently functioning in each of the three areas listed below”. A 10-point Likert-like scale was used with a minimum of “1” meaning “Barely able to function” and a maximum of “10” meaning “excellent functioning”.
2.4. Statistical Analysis
Regarding hypothesis 1, continuous variables (personality disorders scales of the SCID II-Q) were first assessed for normality (Kolmogorov-Smirnov if N > 50 or Shapiro-Wilk if N < 50) and variance homogeneity (Levene test). Continuing with hypothesis 1, we then compared both groups using parametric Student’s t test. Dichotomous variables from hypothesis 1 (axis I DSM IV diagnosis, axis II DSM IV diagnosis) were compared by X2 test. Finally, in order to test hypothesis 2 and 3, we used the U Mann-Whitney test with ordinal variables (self-esteem and self-assessment of functioning). All statistical analysis were made in Graph Pad Prism 7.1.1. and are reported in APA style.
3. Results
3.1. Sociodemographic Characteristics of Patients
Descriptive sociodemographic characteristics of the two groups of patients are shown in Table 1. Basically, there were no statistical differences in terms of sex distribution, marital status, nor in academic formation between both groups.

Table 1.
Sociodemographic characteristics of patients in our study.
However, both groups were statistically different in terms of age (t(445) = 3.47, p < 0.001, Table 1). From our perspective this difference is not biasing our conclusions since it is reduced to a 5 years difference.
3.2. Axis I Disorders
The most frequent axis I disorder diagnosed was depression (PV patients 50% vs. non-PV patients 38.6%, Table 2 [X2 (1, 445) = 0.98, p = 0.32]) that includes major depression and dysthymic disorder. The second most frequent were anxiety disorders (PV patients 25% vs. non-PV patients 37.4%, Table 2 [X2 (1, 445) = 1.74, p = 0.18]) which included generalized anxiety disorder, panic disorder with or without agoraphobia and phobias. On the other hand, adjustment disorders were significantly more frequent in patients without history of PV (PV patients 3.6% vs. non-PV patients 20.6%, Table 2 [X2 (1, 445) = 4–85, p ≤ 0.005]). This included anxiety and/or depressive symptoms. On the contrary, patients with a history of PV were more likely to meet diagnostic criteria for obsessive-compulsive disorder than in patients without PV history (PV patients 17.9% vs. non-PV patients 4.5%, Table 2 [X2 (1, 445) = 9.09, p ≤ 0.005]).
Table 2.
Frequency of Axis I disorders diagnosed in patients from our study.
Both groups were similar in the report of another childhood adversity such as physical and emotional maltreatment or witnessing domestic violence [data not shown].
3.3. Structured Clinical Interview of DSM IV (R) Axis II Personality Disorders Questionnaire (SCID II-Q)
The mean scores of the SCID II-Q are shown in Table 3. The group of patients with a history of PV had significantly higher scores than the group of patients without a PV past of the avoidant [t (440) = 4.29, p ≤ 0.001], depressive [t (439) = 3.33, p ≤ 0.001], paranoid [t (441) = 2.93, p ≤ 0.005] and borderline personality patterns [t (436) = 2.08, p = 0.037].
Table 3.
Average scores of the SCID Q-II personality scales.
Moreover, patients with history of PV were more likely to meet the diagnostic criteria for avoidant (X2 (1, N = 445) = 47.6, p ≤ 0.001), depressive (X2 (1, N = 445) = 22.6, p ≤ 0.001) and paranoid personality disorders (X2 (1, N = 445) = 7.8, p ≤ 0.005). These diagnostics were made by using the SCID II protocol interview (Table 4).
Table 4.
Frequency of SCID II personality disorders.
3.4. Self-Esteem and Social Support
Finally, patients with a history of PV reported lower self-esteem (2 vs. 3) (U = 7477.5, p ≤ 0.001) and worst self-assessment of social relationships (4 vs. 5) (U = 6249, p ≤ 0.05) (Table 5). What is more, it was significantly more difficult for the group of PV patients to answer “yes” (52% vs. 74.4%, p ≤ 0.05) to the question “Do you have a close friend who is supportive and someone you can confide in during difficult times?”.
Table 5.
Median score of self-esteem and self-assessment of functioning.
4. Discussion
Research on the psychopathological repercussions of PV in childhood/adolescence indicates a significant impact on psychological well-being. Thus, it has been observed that those patients exposed to this type of experience are more likely to present psychological symptoms such as anxiety, somatization and low self-esteem [7,8,9,10].
On the other hand, although there are cross-sectional and follow-up studies than have documented the long-term psychological impact of PV [3,11,12,13,14,15,16], only a few offer results on its possible role in personality dysfunction [27,28,29]. Previous studies were mainly focused on the borderline pattern. Therefore, the main goal in the present study was to examine the association of PV experience with all the dysfunctional personality patterns. To the best of our knowledge no previous studies have been conducted with this broader framework.
The main finding of the present research is that patients with antecedents of chronic PV during childhood/adolescence are statistically more likely to meet the diagnostic criteria for three of the DSM IV personality disorders: the avoidant, paranoid and depressive.
We now proceed to discuss these associations, their possible psychological and neurobiological mechanisms, practical implications and future perspectives.
4.1. The Impact of PV in the Long-Term Personality Dysfunction
Nearly 30 years ago, Olweus (1993) [3] wondered if the experience of being victimized over long periods of time leave certain scars on the adult personality. This question is not surprising insofar as the chronic occurrence of PV situations can be understood as a kind of toxic stress that thwarted a basic human need such as social belonging [39].
In our study, the avoidant personality disorder was the one with the strongest association and, thus, in contrast with the clinical control group, more than half of the patients with a history PV (12.2% vs. 60.7%, respectively) met the clinical criteria for the avoidant personality disorder. This result has not come as a surprise since bullying actually implies an aversive interpersonal circumstance that is chronically maintained and that in many cases can be in the basis of social anxieties with attitudes of interpersonal withdrawal, expectations of rejection and, in many cases, personal attributions for its occurrence [40,41,42]. Moreover, patients that had suffered from PV reported having a trusting friendship less frequently and rated their current social functioning more unfavorably which is consistent with the avoidant personality disorder. In addition, although the clearest association was with this personality pattern, the history of being bullied was also associated with a higher frequency of presenting other types of personality disorders such as paranoid and depressive.
In the present study, PV was associated with significantly higher scores in the SCID II-Q paranoid personality scale and in the percentage of patients that accomplished the DSM IV diagnostic criteria for the paranoid personality disorder. Regarding this personality pattern, is relevant that research indicates the presence of hostile attributional biases in children who have suffered abuse [43]. And there is some evidence of the association between bullying victimization and hostile expectations, suspiciousness and ideas of reference among youths [44] and with rejection sensitivity [45]. Sensitivity to anger cues and biases in social information processing could be precursors of the paranoid orientation observed with increased frequency in the group of patients with antecedents of PV in our study. It could be said that being bullied could induce a cognitive vulnerability with negative schemas about the self, others and the world with implications in the development of paranoid ideation. As Schafer and colleagues [46] said, besides vivid and persistent memories, many of the adults with personal antecedents of PV feel that the experience had long-term effects on them, such as lack of trust in relationships.
On the other hand, results are very consistent with the rejection sensitivity model [47] which predicts that the experience of rejection, such as being a victim of bullying, is involved in perceptions and expectations of rejection in interpersonal relationships. Thus, the person becomes vigilant, meticulously scanning the environment for any possible rejection cues and preparing to act defensively once cues of rejection are detected.
We have also found that patients who had reported PV obtained a higher score in the SCID II-Q scale of depressive personality disorder (included in appendix B of the DSM IV) and more often met the diagnostic DSM IV criteria for this disorder. This reflects the pervasiveness of the depressive experience in this group of patients. There is evidence that major life events involving social rejection are strongly associated with the onset of depression. For example, Slavish and colleagues [48] propose a psychobiological model of depression that highlights that social rejection events activate brain regions involved in processing negative affect and rejection-related distress. They also elicit negative self-referential cognitions (e.g., “I’m undesirable”, “other people don’t like me”) and related self-conscious emotions (e.g., shame, humiliation). The experience of PV, as a class of social rejection, can be involved in the onset of this depressive orientation. It is important to highlight that, as in other studies [46], PV is associated with lower general self-esteem, an important characteristic of depressive disorders. The devaluated self-perception not only is reflected in a specific scale of self-esteem but also in the fact that the practical totality of the patients with a history of PV (27/28) reported feelings of self-depreciation and culpability in the present moment in the specific item of the Depression scale of the Structured Clinical Interview for DSM IV Axis I Disorders. It could be said that one of the consequences of being bullied in the time of its occurrence is the state of poor self-esteem [49] and it might become a lifelong trait.
Taken together, the picture that emerges implies in a significant number of patients, in addition to social anxiety and avoidant behavior, a depressive orientation with a tendency to self-devaluation and negative affectivity, as well as mistrust in the intentions of others and a tendency to make attributions of hostility or rejection in social interactions. These three clusters of traits (avoidant, paranoid, and depressive) would be considered to be closely intertwined. For example, Troop-Gordon and colleagues [50] found, in their longitudinal study, that PV was associated to maladaptive coping responses such as withdrawal from peer activities and even stay at home from school as a means of preventing further harassment and that this coping responses were associated to depressive symptoms in the follow-up.
There is also recent empirical evidence [51] in the general population of Spain which states that interpersonal sensitivity is one of the main factors that make up the dimension of paranoid beliefs, along with distrust and ideas of persecution. This factor is made up of four of the seven items of the SCID II-Q avoidance pattern scale used in the present study. Furthermore, results from the study conducted by Contreras and colleagues [51] suggested the possible role of loneliness in mediating the observed relationship between paranoia, depression and anxiety. Additionally, a recent study [52] finds that avoidant personality traits are associated with a magnification of depressive symptoms in university students who are victims of PV. The results of these studies are consistent with our results. Thus, the greater intensity of depressive traits in the patients with a history of PV may be derived from the experience of loneliness reflected in the avoidance pattern. Additionally, the frequent report among these patients of a lack of a trustworthy friend in whom to confide in times of distress is consistent with the mentioned heightened loneliness experience.
On the other hand, in the present study 11 of the 28 patients (39.28%) that reported PV alluded to it as the worst circumstance of their lives. This fact suggest that chronic PV is an important element in long-term psychological maladjustment as reflected in the high frequency of personality disorders in this group. This is consistent with a recent clinical approach that considers that the impact of this type of chronically maintained experience can be understood within the interpersonal trauma framework [53].
4.2. Peer Victimization: Toxic Stress, Allostatic Load and Epigenetics
Arguably, PV and related experiences such as rejection and ostracism interfere with something that is instinctively human, such as the search for a social place within the peer group and to fulfill a fundamental need to belong [35,39,54]. As children grow up, they spend more time with peers and peer interactions take an increased importance for socialization but it also become a substantial source of stress [55]. Given the importance of peer relationships, it would be surprising if experiencing negative peer attitudes and behaviors during prolonged periods of time had no effect on an individual development from a social and socio-cognitive perspective [46]. Moreover, there is evidence that the social pain associated with this type of experience can be associated with the activation of the same neural network that are involved in physical pain [56]. The activation of these neural regions serves as a neural alarm system or “sociometer” alerting individuals to a discrepancy between their desired social state (social acceptance) and their current social condition (social rejection) [57]. On the other hand, social pain can be relived more intensely than physical pain [33]. Consequently, it is not unexpected that social pain can have neurobiological consequences as other forms of maltreatment [35,58]. So, research in neuroscience suggest that PV can cause significant social pain which can jeopardize the individual capacity for effective functioning rather than “building character” [35].
Toxic stress can be defined as a strong, frequent, and/or prolonged activation of the body´s stress response system [59] and is implicated in Allostatic load, a process in which the body accrues damage over time impairing its capacity to maintain and restore homeostasis in the face of future challenges [55]. There is research evidence about the impact of serious and chronic circumstances during development (such as physical, emotional and sexual abuse, emotional and physical neglect and witnessing intrafamilial violence) on the structure, function and connectivity of diverse brain regions (anterior cingulate cortex, corpus callosum, amygdala, insula, hippocampus and prefrontal cortex) [60]. The impact on these neural regions and networks, that participate in functions as social cognition, self-awareness or emotional regulation, may be important in vulnerability to physical and mental health problems along life [35].
Chronic PV can be seen as a form of toxic stress. Indeed, Vaillancourt and colleagues [19] indicate that PV is associated with: (a) changes in the neuroendocrine stress response system; (b) increased inflammation; and (c) epigenetic alterations such as DNA methylation. The authors highlight that these biological changes are consistent with what is known about the negative effects of chronic and/or extreme stress on health and well-being. For example, Copeland and colleagues [61] found that being bullied predicted long term greater increases in C-reactive protein (CRP), a marker of lower grade inflammation, a mechanism by which PV may get under the skin to affect adult health functioning, even many years later. There is also evidence about the role of PV in the sensitization of neural structures involved in the processing of social information [62]. For example, Swartz, Carranza and Knodt [63] found that that higher amygdala activity to fearful and/or angry faces is predicted by higher PV. McIver and colleagues [64] associated PV with increased neural response to social exclusion in an experimental task (Cyberball paradigm) in the left amygdala, left inferior frontal operculum, and right fusiform gyrus. And Rudolph and colleagues [57] found a heightened response of neural structures of the neural social network (dorsal and subgenual anterior cingulate cortex and anterior insula) in the experimental task of social exclusion (Cyberball paradigm) among girls with chronic experience of PV.
Epigenetics is a field of enormous transcendence for Psychiatry and clinical Psychology [65,66,67]. Epigenetic mechanisms could underlie the relationship between childhood adversity, such as PV, and vulnerability to stress and psychopathology. Thus, the neurobiological research on the consequences of environmental stressful conditions during development, since the seminal research by Weaber and colleagues [68], has incorporated epigenetic data [69]. Several studies have found epigenetic modifications associated to PV [70,71]. However, other two studies [69,72] only found limited and weak evidence of epigenetic modifications associated to PV. The complexity of research on the potential epigenetic mechanisms in the association between PV and psychopathological outcomes is highlighted by Marzi and colleagues [72]. For example, exposure-related methylation signatures may be concentrated only among the subset of victimized individuals who develop stress-related disorders or could be enhanced by risk factors or mitigated by protective factors.
4.3. Psychological Processes That Link PV and Dysfunctional Personality Traits
Psychological factors involved in PV should not be understood as a separate influence of the neurobiological factors. For example, Rudolph and colleagues [57] found evidence of an indirect pathway, through avoidance motivation, between heightened neural sensitivity in an experimental social exclusion task and internalized psychopathology (symptoms of depression and social anxiety) among girls with experience of chronic PV. The avoidance motivation could be understood as a psychological sensitivity to aversive social cues as reflected in a drive to avoid negative judgments, peer disapproval and loss of social status. Similarly, Guroglu and Veenstra [33] remarked that chronically rejected children and adolescents with heightened neural sensitivity to exclusion may not only experience more adverse reactions to actual peer rejection but also show hypervigilance to potential social threats and a tendency to avoid the possibility of future rejection. Therefore, accumulating negative experiences in the peer context might further strengthen heightened neural responses to these adverse interactions.
The experience of PV may be involved in the development of cognitive schemas with perceptions of the self as worthless and unlovable, the world as hostile, as well as a negative perception of the future [32]. As Slavish [54] stated, these schemas play critical roles in structuring attitudes, expectations, beliefs and behaviors across life span. On the other hand, dysfunctional coping strategies (such as ruminative thoughts, emotional numbness or inaction) in the context of PV are associated with depressive symptoms in the follow up and these types of dysfunctional strategies have continuity along time [50]. The characteristic way of coping of interpersonal stress may goes beyond childhood and emerge as a long-lasting trait in the adulthood as can be seen in the dysfunctional personality patterns of the group of patients with antecedents of PV in our study. It is important to highlight that the social support and bonding has a significant effect in the modulation of stress [73,74]. The poor social functioning, mistrust and avoidance behaviors may be important mediators of the long-term difficulties in coping with stress and, in consequence, in the vulnerability to psychopathology.
However, as proposed by developmental psychopathology [18], not only genetic and neurobiological factors [19,20], but also other circumstances in life, can modulate the impact of adversity on development [21,22]. For example, Teicher and colleagues [60] proposed the hypothesis that certain polymorphisms may together determine how malleable an individual is to both negative and positive experiences and called it phenotypic plasticity. As a matter of fact, the temperamental trait of Behavioral Inhibition is an important predictor of social anxiety [23,24]. On the other hand, Ttofi and colleagues [75] reported that having a good performance at school and social skills, coming from a stable (undisrupted) family, being attached to parents and having prosocial friends seem to interrupt the continuity from school bullying perpetration and victimization to later maladjustment problems.
Despite the fact that is probable that many who have gone through this type of experience show resilience and do not get into paths of dysfunctional functioning, the high frequency of personality disorders in this study with a clinical sample of patients in treatment in a mental health center, suggest also that for many it may be a circumstance of special relevance to understand the origin of life trajectories with chronic difficulties as reflected in personality disorders. As Teicher [58] said in relation to the experience of maltreatment in childhood, for patients with a history of PV this experience could be seen as a wound that time does not heal.
It may be said, in summary, that the adverse psychological outcomes related with the experience of PV are implicated in altered cognitive and emotional processes and their related neural and behavioral functioning. These processes could be conceived, more than discrete states, as conforming patterns of functioning with continuity along life as can be seen in the personality disorders. Adaptive inflexibility, tendency to be involved in vicious circles and tenuous stability in the face of stress [30] of these dysfunctional patterns may have important implications for the physical and mental health. Figure 1 shows the main psychological impact of PV during adulthood and the possible long-term neurobiological alterations such as cognitive alterations and molecular changes that may have some peripheral impact that could be traced as biomarkers. Further research is needed to shed some light into this field.
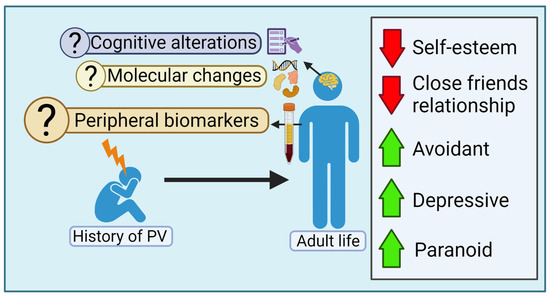
Figure 1.
The possible long-term neurobiological and psychological impact of Peer Victimization.
Building on an increased body of evidence, the Center for Disease Control and Prevention has proposed that child abuse and neglect be defined as a public health issue with lifelong consequences [76]. Thus, the design and implementation of approaches to both the prevention and treatment of toxic stress and its consequences, beginning in the early years must be a key priority [59]. PV, as a form of toxic stress with lifelong consequences, also should be considered a public health issue. There is evidence of effective school based anti-bullying programs [77,78] and, as Olweus [3] indicated thirty years ago, based in the immediate and long-term emotional repercussion of PV, it is urgent for school authorities and parents to intervene against bully/victim problems not only to stop current suffering of the victims but also to prevent its frequent long term psychopathological sequelae.
4.4. Limitations and Future Perspective
The study has several limitations that we should point out:
In first place, its cross-sectional design does not allow the establishment of causal links among being bullied and the clinical manifestations of personality dysfunction. For example, patients with antecedents of PV could also have higher social anxiety and be easier targets of bullying. This shared vulnerability is captured in the concept of “evocative genotype-environmental correlation” that refers to genetic influences in individual differences in exposure to certain environments [79]. However, the results of one study with twins reflects that along the shared vulnerability, there are an environmental impact of bullying victimization on child social and separation anxiety and in adult suicidal ideation that cannot be accounted for by genetic background or shared environmental factors [80].
In second place, other limitation is the retrospective self-report of the experiences of peer victimization, although there is evidence that when reporting situations from childhood, most adults are accurate and stable in their recollections [81].
A third limitation is that most of the study subjects were women which reflect the greater ease with which women with psychological problems seek mental health treatment for them. This fact could limit the generalizability of the results. On the other hand, the generalizability of the results also is limited to patients in psychological treatment.
A fourth limitation is that age is significantly different between groups. From our perspective, 5 years on average would not affect to the main conclusion of the present study.
A fifth limitation is that the environment context of the patients in the group with a history of PV could be differ significantly. Thus, several patients suffer also another concurrent adversity as emotional and physical maltreatment in their home. However, there are not differences in the frequency of these another adversity in comparison with the clinical control group.
Finally, the definition of PV or bullying victimization also is different of the definition used in other studies. For example, in a study in Spain [82] all the university subjects that reported at least one experience of bullying victimization in the last 12 months were classified as bully victims. On the contrary, in the present study we decide only include as victims of PV those patients with repeated experiences of being bullied during long periods of time. Therefore, the experience of these patients represents the more serious forms of PV.
The association between PV and adult avoidant, depressive and paranoid personality traits and disorders found in the present study reflect the penetrant repercussions of this type of experience. A circumstance that thwarts the psychobiological need of social belonginess. However, future studies must test if these associations are present in the general population and not only in individuals with axis I psychopathology that seek treatment. In future studies will be of special interest, also, investigate specific characteristics of the experience of PV (such as, psychological, cyberbullying, physical bullying), intensity of the experience (frequency of the episodes and duration), developmental period in which occur, and risk and protective environmental/contextual, genetic/epigenetic and neurobiological factors that might modulate and/or mediate the impact of PV in long-term maladaptive outcomes.
5. Conclusions
As McDougall and Vaillancourt remarks [14], few topics in developmental and educational psychology have united researchers, parents, teachers and health professionals in such a profound way than the study of PV to the extent that it can be considered an extremely difficult life experience with lasting and serious negative repercussions. The results of the present study support the hypothesis that PV in childhood/adolescence may be an important antecedent in personality dysfunction as reflected in pervasive social anxiety, interpersonal sensitivity and paranoid thought, low self-esteem and emotional distress. These experiences, found in the context of being bullied [25], may have long-term continuity and be important in the subjective ill-being and in seeking psychological treatment [83]. In this, regardless of the theoretical framework (e.g., psychodynamic, cognitive-behavioral, experiential), a basic requirement is the case conceptualization or clinical formulation. The remote history of bullying may have a prominent place in the clinical formulation and, thus, it should be taken into account in the orientation of the treatment [28].
In short, research findings on the association between PV in childhood and/or adolescence and long-term psychological symptoms and personality dysfunction have important policy implications. It constitutes a public health problem since it might be behind the origin of psychopathological life trajectories that culminate in adult personality pathology and so deep efforts should be made in schools in order to take actions against this common behavior. The available evidence indicates that bullying is a risk factor of mental health problems potentially modifiable. Thus, together with the clinical understanding that allow us to offer adequate treatment to those who suffer psychopathological sequelae derived from their history of PV, bullying prevention interventions should become a priority for universal primary prevention in mental health [54,78].
Author Contributions
Conceptualization: R.F.-M. and R.C.A.-B.; methodology: R.F.-M.; validation: R.F.-M.; formal analysis: R.F.-M., C.F.-P., D.P.-R. and A.S.-B.; investigation: R.F.-M. and C.F.-P.; resources: J.M.O.D. and R.C.A.-B.; data curation: R.F.-M., D.P.-R., C.V.G., S.T.-C. and J.M.P.-G.; writing—original draft preparation: R.F.-M.; writing—review and editing: R.F.-M., C.F.-P., D.P.-R., A.S.-B., C.V.G., S.T.-C., J.M.P.-G., J.M.O.D. and R.C.A.-B.; supervision: R.F.-M., J.M.O.D. and R.C.A.-B.; project administration, R.F.-M.; funding acquisition: R.C.A.-B. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Instituto de Salud Carlos III (ISCIII)—PI18/01311—Cofinanciado (Co-funded) Unión Europea/FEDER to R.C.A.-B. Both C.F.-P. and D.P.R. are supported by “Investigo Program” predoctoral contracts from Xunta de Galicia.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board (or Ethics Committee) of Galicia Sur Health Research Institute (IIS Galicia Sur) (protocol code 2013/530).
Informed Consent Statement
Written informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Not applicable.
Acknowledgments
The authors would like to thank Galicia Sur Health Research Institute and the Área Sanitaria de Vigo for their support.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Menesini, E.; Salmivalli, C. Bullying in schools: The state of knowledge and effective interventions. Psychol. Health Med. 2017, 22 (Suppl. S1), 240–253. [Google Scholar] [CrossRef] [PubMed]
- Hymel, S.; Swerer, S.M. Four decades of research on school bullying. Am. Psychol. 2015, 70, 293–299. [Google Scholar] [CrossRef]
- Olweus, D. Victimization by Peers: Antecedents and Long-Term Outcomes. In Social Withdrawal, Inhibition and Shyness in Childhood; Rubin, K.H., Aserdorf, J.B., Eds.; Earlbaum: Hilldale, NJ, USA, 1993; pp. 315–341. [Google Scholar]
- Nansel, T.R.; Craig, W.; Overpeck, M.D.; Saluja, G.; Ruan, J. Cross-national consistency in the relationships between bullying behaviors and psychosocial adjustment. Arch. Pedriatr. Adolesc. Med. 2004, 158, 730–736. [Google Scholar] [CrossRef]
- Currie, C.; Zanotti, C.; Morgan, A.; Currie, D.; de Looze, M.; Roberts, C.; Samdal, O.; Smith, O.R.; Barnekow, V. Social Determinants of Health and Well-Being among Young People. Health Behaviour in School-Aged Children (HCSC) Study: International Report from the 2009/2010 Survey; WHO Regional Office for Europe: Copenhagen, Denmark, 2012; (Health Policy for Children and Adolescents, No. 6); Available online: https://www.euro.who.int/__data/assets/pdf_file/0007/167281/E96444_part1.pdf (accessed on 18 December 2022).
- Luxemberg, H.; Limber, S.P.; Olweus, D. Bullying in U.S. Schools: 2019 Status Report; Hazelden Publishing: Center City, MN, USA, 2019; Available online: https://olweus.sites.clemson.edu/documents/Status%20Report_2019.pdf (accessed on 18 December 2022).
- Smith, P.K.; Brain, P. Bullying in schools: Lessons from two decades of research. Aggress. Behav. 2000, 26, 1–9. [Google Scholar] [CrossRef]
- Arsaneault, L.; Bowes, L.; Shakoor, S. Bullying victimization in youths and mental health problems: ‘Much ado about nothing’? Psychol. Med. 2010, 40, 717–729. [Google Scholar] [CrossRef] [PubMed]
- Hawker, D.S.L.; Boulton, M.J. Twenty years’ research on peer victimization and psychosocial maladjustment: A meta-analytic review of cross-sectional studies. J. Child Psychol. Psychiatry Allied Discip. 2000, 41, 441–455. Available online: https://pubmed.ncbi.nlm.nih.gov/10836674/ (accessed on 18 December 2022). [CrossRef]
- Arana, A.A.; Boyd, E.Q.; Guarneri-White, M. The impact of social and physical peer victimization on systemic inflammation in adolescence. Merril Palmer Q. 2018, 64, 12–40. Available online: https://www.muse.jhu.edu/article/705184 (accessed on 18 December 2022). [CrossRef]
- Sourander, A.; Jensen, P.; Ronning, J.A.; Niemela, S.; Helenius, H.; Sillamäki, L.; Kumpulainen, K.; Piha, J.; Tamminen, T.; Moilanen, I.; et al. What is the early adulthood outcome of boys who bully or are bullied in childhood? The finnish “from a boy to a man” study. Pediatrics 2007, 120, 397–404. [Google Scholar] [CrossRef]
- Takizawa, R.; Maughan, B.; Arsenault, L. Adult health outcomes of childhood bullying victimization: Evidence from a five-decade longitudinal british birth cohort. Am. J. Psychiatry 2014, 171, 777–784. [Google Scholar] [CrossRef]
- Klomek, A.B.; Sourander, A.; Elonheimo, H. Bullying by peers in childhood and effects on psychopathology, suicidality and criminality in adulthood. Lancet Psychiatry 2015, 2, 930–941. [Google Scholar] [CrossRef]
- McDougall, P.; Vaillancourt, T. Long-term adult outcomes of peer victimization in childhood and adolescence. Am. Psychol. 2015, 70, 300–310. [Google Scholar] [CrossRef] [PubMed]
- Moore, S.E.; Norman, R.E.; Suetani, S.; Thomas, H.J.; Sly, P.D.; Scott, J.G. Consequences of bullying victimization in childhood and adolescence: A systematic review and meta-analysis. World J. Psychiatry 2017, 7, 60–76. [Google Scholar] [CrossRef] [PubMed]
- Copeland, W.; Wolke, D.; Angold, A.; Costello, J. Adult psychiatric outcomes of bullying and being bullied by peers in childhood and adolescence. JAMA Psychiatry 2013, 70, 419–426. [Google Scholar] [CrossRef] [PubMed]
- Lereya, S.T.; Copeland, W.E.; Costello, E.J.; Wolke, D. Adult mental health consequences of peer bullying and maltreatment in childhood: Two cohorts in two countries. Lancet Psychiatry 2015, 2, 524–531. [Google Scholar] [CrossRef] [PubMed]
- Cicchetti, D.; Rogosch, F.A. Equifinality and multifinality in developmental psychopathology. Dev. Psychopathol. 1996, 8, 597–600. [Google Scholar] [CrossRef]
- Vaillancourt, T.; Sanderson, C.; Arnold, P.; McDougall, P. The Neurobiology of Peer Victimization: Longitudinal Links to Health, Genetic Risk, and Epigenetic Mechanisms. In Handbook of Bullying Prevention: A Life Course Perspective; Bradshaw, C., Ed.; NASW Press: Cary, NC, USA, 2017; pp. 35–47. [Google Scholar]
- Caspi, A.; McClay, J.; Moffitt, T.E.; Mill, J.; Martin, J.; Craig, I.W.; Taylor, A.; Poulton, R. Role of genotype in the cycle of violence in maltreated children. Science 2002, 297, 851–854. [Google Scholar] [CrossRef]
- Hodges, E.V.E.; Boivin, M.; Vitaro, F.; Bukowski, W.M. The power of friendship: Protection against an escalating cycle of peer victimization. Dev. Psychol. 1999, 35, 94–101. [Google Scholar] [CrossRef]
- Fitzpatrick, S.; Bussey, K. The role of perceived friendship self-efficacy as a protective factor against the negative effects of social victimization. Soc. Dev. 2014, 23, 41–60. [Google Scholar] [CrossRef]
- Clauss, J.A.; Blackford, J.U. Behavioral inhibition and risk for development social anxiety disorder: A meta-analytic study. J. Am. Acad. Child Adolesc. Psychiatry 2012, 51, 1066–1075. [Google Scholar] [CrossRef]
- Caouette, J.D.; Guyer, A.E. Gaining insight into adolescent vulnerability for social anxiety from developmental cognitive neuroscience. Dev. Cogn. Neurosci. 2014, 8, 65–76. [Google Scholar] [CrossRef]
- Wolke, D.; Lereya, S.T. Long term effects of bullying. Arch. Dis. Child. 2015, 100, 879–885. [Google Scholar] [CrossRef] [PubMed]
- Kasen, S.; Johnson, J.G.; Chen, H.; Crawford, T.N. School Climate and Change in Personality Disorder Symptom Trajectories Related to Bullying: A Prospective Study. In Bullying in North American Schools; Espalage, D.L., Swearer, S.M., Eds.; Routledge: New York, NY, USA, 2010. [Google Scholar]
- Sansone, R.A.; Lam, C.; Wiederman, M.W. Being bullied in childhood: Correlations with borderline personality in adulthood. Compr. Psychiatry 2010, 51, 458–461. [Google Scholar] [CrossRef] [PubMed]
- Erazo, M.B.; Krygsman, A.L.; Vallancourt, T. The cumulative effects of bullying victimization in childhood and adolescence on borderline personality disorder symptoms in emerging adulthood. Int. J. Bullying Prev. 2022. [Google Scholar] [CrossRef]
- Antila, H.; Arola, R.; Hakko, H.; Riala, K.; Riipinen, P.; Kantjärvi, L. Bullying involvement in relation to personality disorders: A prospective follow-up of 508 inpatient adolescents. Eur. Child Adolesc. Psychiatry 2017, 26, 779–789. [Google Scholar] [CrossRef]
- Millon, T. Trastornos de la Personalidad: Más Allá del DSM IV; Masson: Barcelona, Spain, 1998. [Google Scholar]
- Young, J. Cognitive Therapy for Personality Disorders: A Schema-Focused Approach; Professional Resource Press: Sarasota, FL, USA, 1994. [Google Scholar]
- Sweerer, S.M.; Hymel, S. Understanding the psychology of bullying: Moving toward a social-ecological diathesis stress model. Am. Psychol. 2015, 70, 344–353. [Google Scholar] [CrossRef]
- Guroglu, B.; Veenstra, R. Neural underpinnings of peer experiences and interactions: A review of social neuroscience research. Merril Palmer Q. 2021, 67, 416–456. [Google Scholar] [CrossRef]
- Chen, Z.; Williams, K.D.; Fitness, J.; Newton, N.C. When hurt will not heal. Exploring the capacity to relive social and physical pain. Psychol. Sci. 2008, 19, 789–795. [Google Scholar] [CrossRef]
- Lupien, S.J.; Juster, R.P.; Raymond, C.; Marín, M.F. The effects of chronic stress on the human brain: From neurotoxicity, to vulnerability, to opportunity. Front. Neuroendocrinol. 2018, 49, 91–105. [Google Scholar] [CrossRef]
- First, M.B.; Gibbon, M.; Spitzer, R.L.; Williams, J.B.; Benjamin, L.S. Entrevista Clínica Estructurada Para Los Trastornos de la Personalidad del eje II del DSM-IV (SCID-II); Masson: Barcelona, Spain, 1999. [Google Scholar]
- First, M.B.; Gibbon, M.; Spitzer, R.L.; Williams, J.B.; Benjamin, L.S. SCID-II Personality Questionnaire; American Psychiatric Press: Washington, DC, USA, 1997. [Google Scholar]
- Campo-Arias, A.; Díaz-Martínez, L.A.; Barros-Bermúdez, J.A. Consistencia interna del cuestionario autoadministado de la Entrevista Clínica Estructurada para Trastornos del Eje II del DSM IV. Rev. Colomb. Psiquiat. 2008, 37, 378–384. Available online: http://www.redalyc.org/articulo.oa?id=80611205008 (accessed on 11 December 2022).
- Baumeister, R.; Leary, M.R. The need to belong: Desire for interpersonal attachments as a fundamental human motivation. Psychol. Bull. 1995, 117, 497–529. Available online: https://pubmed.ncbi.nlm.nih.gov/7777651/ (accessed on 18 December 2022). [CrossRef]
- Graham, S.; Junoven, J. Self-blame and peer victimization in middle school: An attibutional analysis. Dev. Psychol. 1998, 34, 587–599. [Google Scholar] [CrossRef] [PubMed]
- Negi, R. Cognitive processes of victims of bullying. Int. J. Bullying Prev. 2021, 3, 1–13. [Google Scholar] [CrossRef]
- Calderero, M.; Salazar, I.C.; Caballo, V.E. Una revisión de las relaciones entre el acoso escolar y la ansiedad social. Behav. Psychol. 2011, 19, 393–419. Available online: https://www.behavioralpsycho.com/wp-content/uploads/2019/08/08.Calderero_19-2oa.pdf (accessed on 18 December 2022).
- Keil, V.; Price, J.M. Social information-processing patterns of maltreated children in two social domains. J. Appl. Dev. Psychol. 2009, 30, 43–52. [Google Scholar] [CrossRef]
- Ziv, Y.; Leibovich, I.; Shechtman, Z. Bullying victimization in early adolescence: Relations to social information processing patterns. Aggress. Behav. 2013, 39, 482–492. [Google Scholar] [CrossRef] [PubMed]
- Butler, J.C.; Doherty, M.S.; Potter, R.M. Social antecedents and consequences of interpersonal rejection sensitivity. Personal. Individ. Differ. 2007, 43, 1376–1385. [Google Scholar] [CrossRef]
- Schäfer, M.; Korno, S.; Smith, P.K.; Hunter, S.C.; Mora-Merchán, A.; Singer, M.; van der Meulen, K. Lonely in the crowd: Recollections of bullying. Br. J. Dev. Psychol. 2004, 22, 379–394. [Google Scholar] [CrossRef]
- Levy, S.R.; Ayduk, O.; Downey, G. The Role of Rejection Sensitivity in People’s Relationships with Significant Others and Valued Social Groups. In Interpersonal Rejection; Leary, M., Ed.; Oxford University Press: Oxford, UK, 2001; pp. 251–289. [Google Scholar]
- Slavisch, G.M.; O’Donovan, A.; Epel, E.; Kennedy, M. Black sheep get the blues: A psychobiological model of social rejection and depression. Neurosci. Biobehav. Rev. 2010, 35, 39–45. [Google Scholar] [CrossRef]
- Muñoz-Prieto, M.M. Incidencia del Acoso Escolar en Alumnos de 4° y 6° de Educación Primaria en Colegios de la Ciudad de Vigo. Ph.D. Thesis, Universidad de Salamanca, Salamanca, Spain, 2009. [Google Scholar]
- Troop-Gordon, W.; Rudolph, K.D.; Sugimura, N.; Little, T.D. Peer victimization in middle childhood impedes adaptive responses to stress: A pathway to depressive symptoms. J. Clin. Child Adolesc. Psychol. 2014, 44, 432–445. [Google Scholar] [CrossRef]
- Contreras, A.; Valiente, C.; Vázquez, C.; Trucharte, A.; Peinado, V.; Varese, F.; Bentall, R. The network structure of paranoia dimensions and its mental health correlates in the general population: The core role of loneliness. Schizophr. Res. 2022, 246, 65–73. [Google Scholar] [CrossRef]
- Xu, Y.M.; Pu, S.S.; Li, Y.; Zhong, B.L. Possible Avoidant Personality Disorder Magnifies the Association Between Bullying Victimization and Depressive Symptoms Among Chinese University Freshmen. Front. Psychiatry 2022, 13, 822185. [Google Scholar] [CrossRef]
- Idsoe, T.; Vallancourt, T.; Dyregrov, A.; Hagen, K.A.; Ogden, T.; Naerde, A. Bullying victimization and trauma. Front. Psychiatry 2021, 11, 480353. [Google Scholar] [CrossRef] [PubMed]
- Slavich, G.M. Social Safety Theory: A biologically based evolutionary perspective on life stress, health and behavior. Annu. Rev. Clin. Psychol. 2020, 16, 265–295. [Google Scholar] [CrossRef] [PubMed]
- Zárate-Garza, P.P.; Biggs, B.K.; Croarkin, P.; Morath, B.; Leffler, J.; Cuéllar-Barboza, A.; Tye, S. How well do we understand the long-term health implications of childhood bullying? Harv. Rev. Psychiatry 2017, 25, 89–95. [Google Scholar] [CrossRef]
- Eisenberger, N.I.; Lieberman, M.D.; Williams, K.D. Does rejection hurt? An fMRI study of social exclusion. Science 2003, 302, 290–292. [Google Scholar] [CrossRef] [PubMed]
- Rudolph, K.D.; Miernicki, M.E.; Troop-Gordon, W.; Davis, M.; Telzer, E.H. Adding insult to injury: Neural sensitivity to social exclusion is associated with internalizing symptoms in chronically peer victimized girls. Soc. Cogn. Neurosci. 2016, 11, 829–842. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Teicher, M.H. Scars that won’t heal: The neurobiology of child abuse. Sci. Am. 2002, 286, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Shonkoff, J.P.; Boyce, T.; McEwen, B.S. Neuroscience, molecular biology and the childhood roots of health disparities: Building a new framework for health promotion and disease prevention. JAMA 2009, 301, 2252–2259. [Google Scholar] [CrossRef]
- Teicher, M.H.; Samson, J.A.; Anderson, C.M.; Ohashi, K. The effects of childhood maltreatment on brain structure, function and connectivity. Nat. Rev. Neurosci. 2016, 17, 152–666. [Google Scholar] [CrossRef]
- Copeland, W.E.; Wolke, D.; Lereya, S.T.; Shanahan, L.; Worthman, C.; Costello, E.J. Childhood bullying involvement predicts low grade systemic inflammation into adulthood. Proc. Natl. Acad. Sci. USA 2014, 111, 7570–7575. [Google Scholar] [CrossRef] [PubMed]
- Ke, T.; De Simoni, S.; Barker, E.; Smith, P. The association between peer-victimization and structural and functional brain outcomes: A systematic review. JCCP Adv. 2022, 2, e12081. [Google Scholar] [CrossRef]
- Swartz, J.R.; Carranza, A.F.; Knodt, A.R. Amygdala activity to angry and fearful faces relates to bullying and victimization in adolescents. Soc. Cogn. Affect. Neurosci. 2019, 14, 1027–1035. [Google Scholar] [CrossRef] [PubMed]
- McIver, T.; Bosma, R.L.; Sandre, A.; Goegan, S.; Klassen, J.; Chiarella, J.; Booij, K.; Craig, W. Peer victimization is associated with neural response to social exclusion. Merril Palmer Q. 2018, 64, 135–161. [Google Scholar] [CrossRef]
- González-Pardo, H.; Pérez-Álvarez, M. Epigenetics and its implications for Psychology. Psicothema 2013, 25, 3–12. [Google Scholar] [PubMed]
- Delgado-Morales, R.; Agis-Balboa, R.C. Epigenetic mechanisms during ageing and neurogenesis as novel therapeutic avenues in human brain disorders. Clin. Epigenet. 2017, 9, 67. [Google Scholar] [CrossRef] [PubMed]
- Spuch, C.; Agis-Balboa, R.C. Epigenética en neurociencias. Span. Soc. Biochem. Mol. Biol. SEBB Mag. 2014, 174, 18–21. [Google Scholar]
- Weaber, C.G.; Cervoni, C.; Champagne, F.A.; D’Alessio, A.C.; Sharma, S.; Seckl, J.R.; Dymov, S.; Szyf, M.; Meaney, M.J. Epigenetic programming by maternal behavior. Nat. Neurosci. 2004, 7, 847–854. [Google Scholar] [CrossRef]
- Mulder, R.; Walton, E.; Neumann, A.; Houtepen, L.C.; Felix, J.; Bakermans-Kranenburg, M.J.; Suderman, M.; Tiemeier, H.; van Ijzendoornm, M.; Relton, C.; et al. Epigenomics of being bullied: Changes in DNA following bullying exposure. Epigenetics 2020, 15, 750–764. [Google Scholar] [CrossRef]
- Ouellet-Morin, I.; Wong, C.C.Y.; Danese, A.; Pariante, C.M.; Papadopoulos, A.S.; Mill, L.; Arsenault, L. Increased serotonin transporter gene (SERT) DNA methylation is associated with bullying victimization and blunted cortisol response to stress in childhood: A longitudinal study of discordant monozygotic twins. Psychol. Med. 2013, 43, 1813–1823. [Google Scholar] [CrossRef]
- Efstahopoulos, P.; Anderson, F.; Melas, P.A.; Yang, L.L.; Villaescusa, J.C.; Ruegg, J.; Ekstrom, T.J.; Forsell, Y.; Galanti, M.R.; Lavebratt, C. NR3C1 hypermethylation in depressed and bullied adolescents. Transl. Psychiatry 2018, 8, 121. [Google Scholar] [CrossRef]
- Marzi, S.J.; Sujden, K.; Arsenault, L.; Belsky, D.W.; Burrage, J.; Corcoran, D.L.; Danese, A.; Fisher, H.L.; Hannon, E.; Moffitt, T.E.; et al. Analysis of DNA methylation in young people: Limited evidence for an association between victimization stress and epigenetic variation in blood. Am. J. Psych. 2018, 175, 517–529. [Google Scholar] [CrossRef] [PubMed]
- Cacioppo, S.; Cacioppo, J. Decoding the invisible forces of social connection. Front. Integr. Neurosci. 2012, 6, 51. [Google Scholar] [CrossRef] [PubMed]
- Coan, J.; Sbarra, D.A. Social baseline theory: The social regulation of risk and effort. Curr. Opin. Psychol. 2015, 1, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Ttofi, M.M.; Bowes, L.; Farrington, D.P.; Lösel, P. Protective factors interrumping the continuity from school bullying to later internalizing and externalizing problems: A systematic review of prospective longitudinal studies. J. Sch. Violence 2014, 13, 5–38. [Google Scholar] [CrossRef]
- Middlesbrooks, J.S.; Audage, C.A. The Effects of Childhood Stress on Health across the Lifespan; Centers for Disease Control and Prevention, National Center for Injury Prevention and Control: Atlanta, GA, USA, 2008. Available online: https://stacks.cdc.gov/view/cdc/6978 (accessed on 18 December 2022).
- Ttofi, M.M.; Farrington, D.P. Effectiveness of school-based programs to reduce bullying: A systematic and meta-analytic review. J. Exp. Criminol. 2011, 7, 27–56. [Google Scholar] [CrossRef]
- Fraguas, D.; Díaz-Caneja, C.; Ayora, M.; Durán-Cutlla, M.; Abregú-Crespo, R.; Ezquiaga-Bravo, I.; Martín-Babarro, J.; Arango, C. Assessment of school anti-bullying interventions: A meta-analysis of randomized controlled trials. JAMA Pediatr. 2021, 175, 44–55. [Google Scholar] [CrossRef]
- McEwen, B.S.; Eiland, L.; Hunter, R.G.; Miller, M.M. Stress and anxiety: Structural plasticity and epigenetic regulation as a consequence of stress. Neuropharmacology 2012, 62, 3–12. [Google Scholar] [CrossRef]
- Sildberg, J.L.; Copeland, W.; Linker, J.; Moore, A.; Roberson-Nay, R.; York, T.P. Psychiatric outcomes of bullying victimization: A study of discordant monozygotic twins. Psychol. Med. 2016, 46, 1875–1883. [Google Scholar] [CrossRef]
- Brewin, C.R.; Andrews, B.; Gotlib, I.H. Psychopathology and early experience: A reappraisal of retrospective reports. Psychol. Bull. 1993, 113, 82–89. [Google Scholar] [CrossRef]
- Sánchez, F.C.; Romero, M.F.; Zaragoza, J.N.; Ruiz-Cabello, A.L.; Frantzisko, O.R.; Maldonado, A.L. Prevalence and patterns of traditional bullying victimization and cyber-teasing among college population in Spain. BMC Public Health 2016, 16, 176. [Google Scholar] [CrossRef]
- Masillo, A.; Valmaggia, L.R.; Saba, R.; Brandizzi, M.; Cascio, N.; Telesfro, L.; Venturini, P.; Izzo, A.; Mattioli, M.T.; D’Alerma, M.; et al. Interpersonal sensitivity, bullying victimization and paranoid ideation among help-seeking adolescents and young adults. Early Interv. Psychiatry 2019, 13, 57–63. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).