
Sustained Virological Response Is the Most Effective in Preventing Hepatocellular Carcinoma Recurrence after Curative Treatment in Hepatitis C Virus-Positive Patients: A Study Using Decision Tree Analysis

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
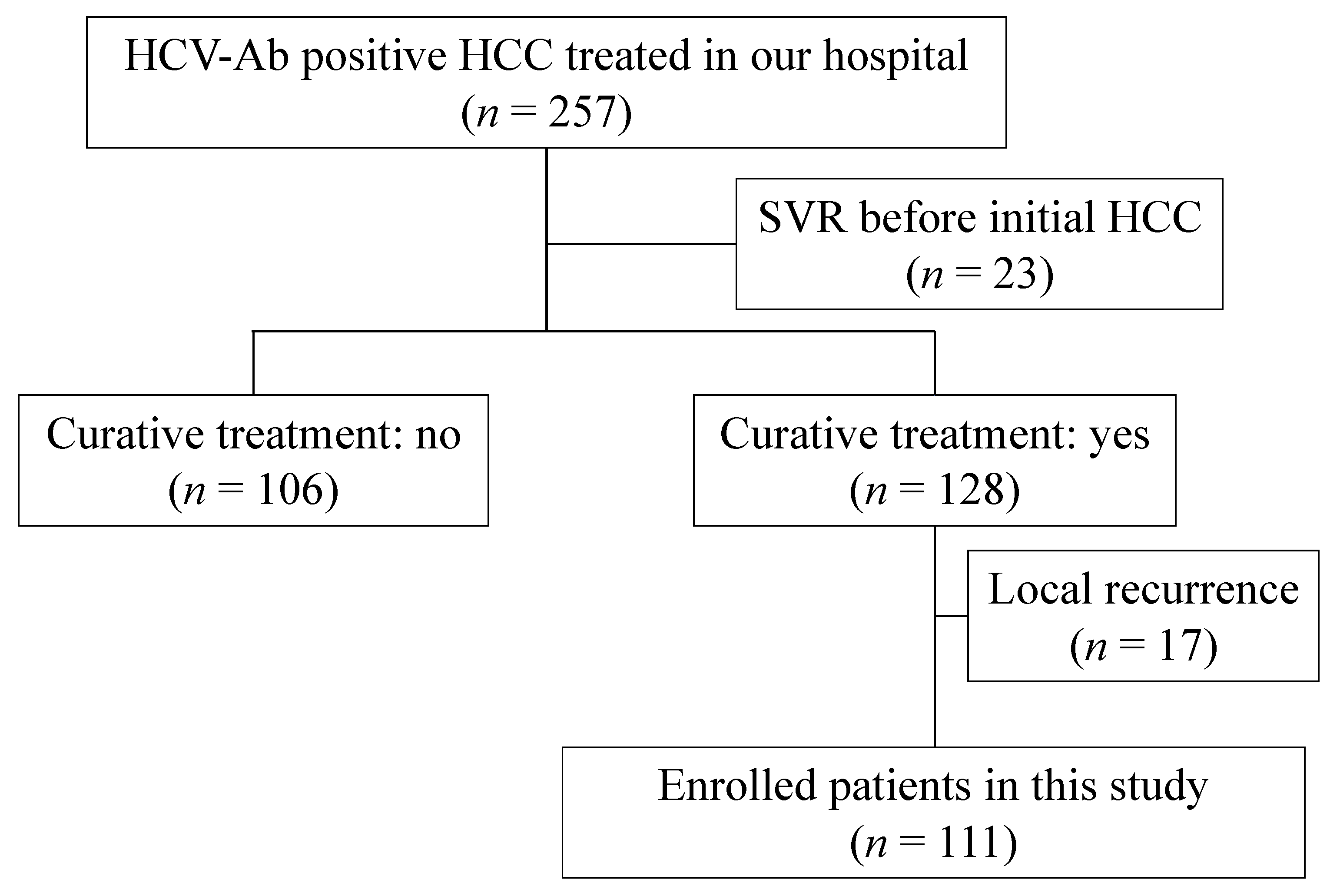
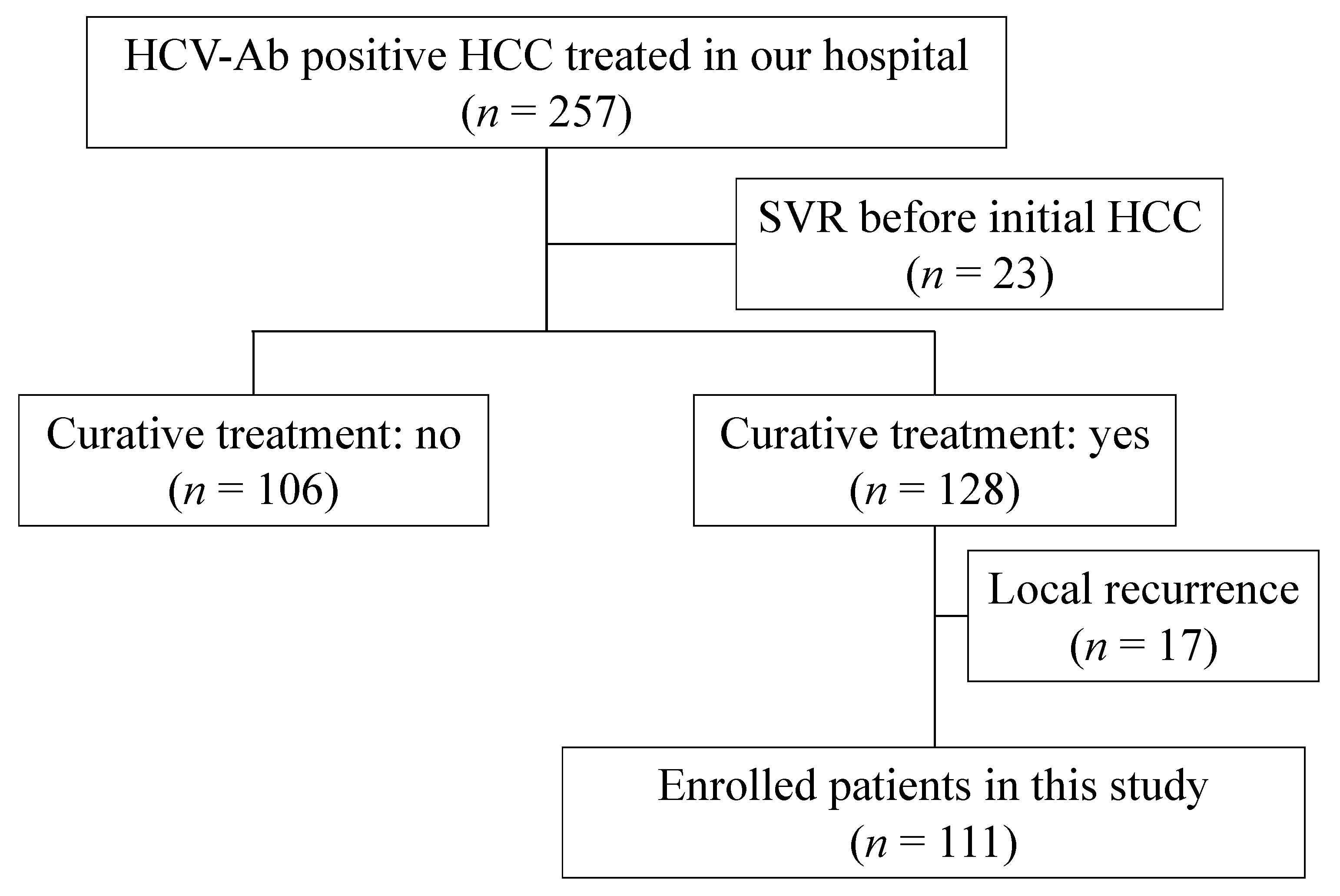
2.1. Patients, Treatment, and Determination of HCC Recurrence
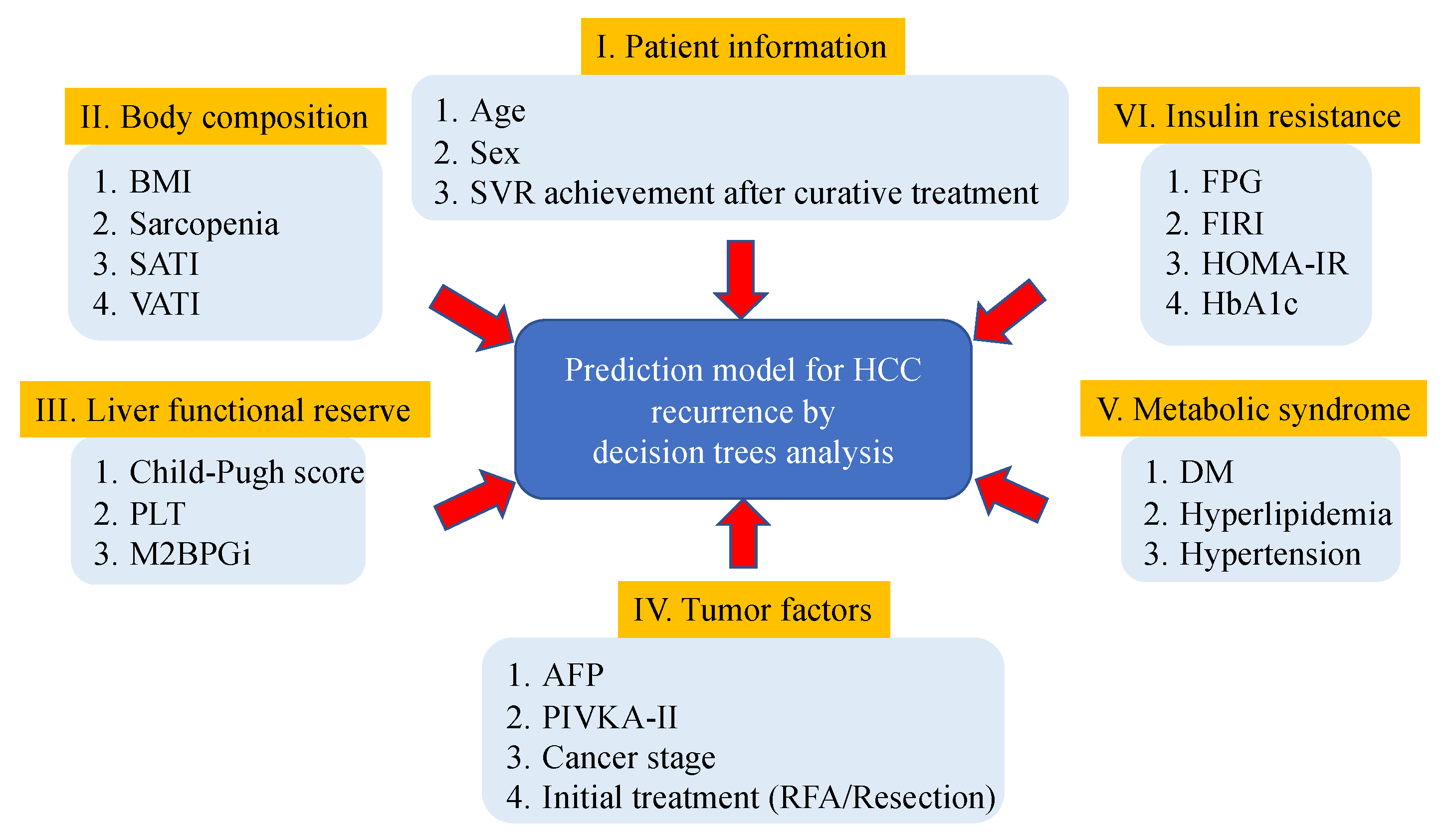
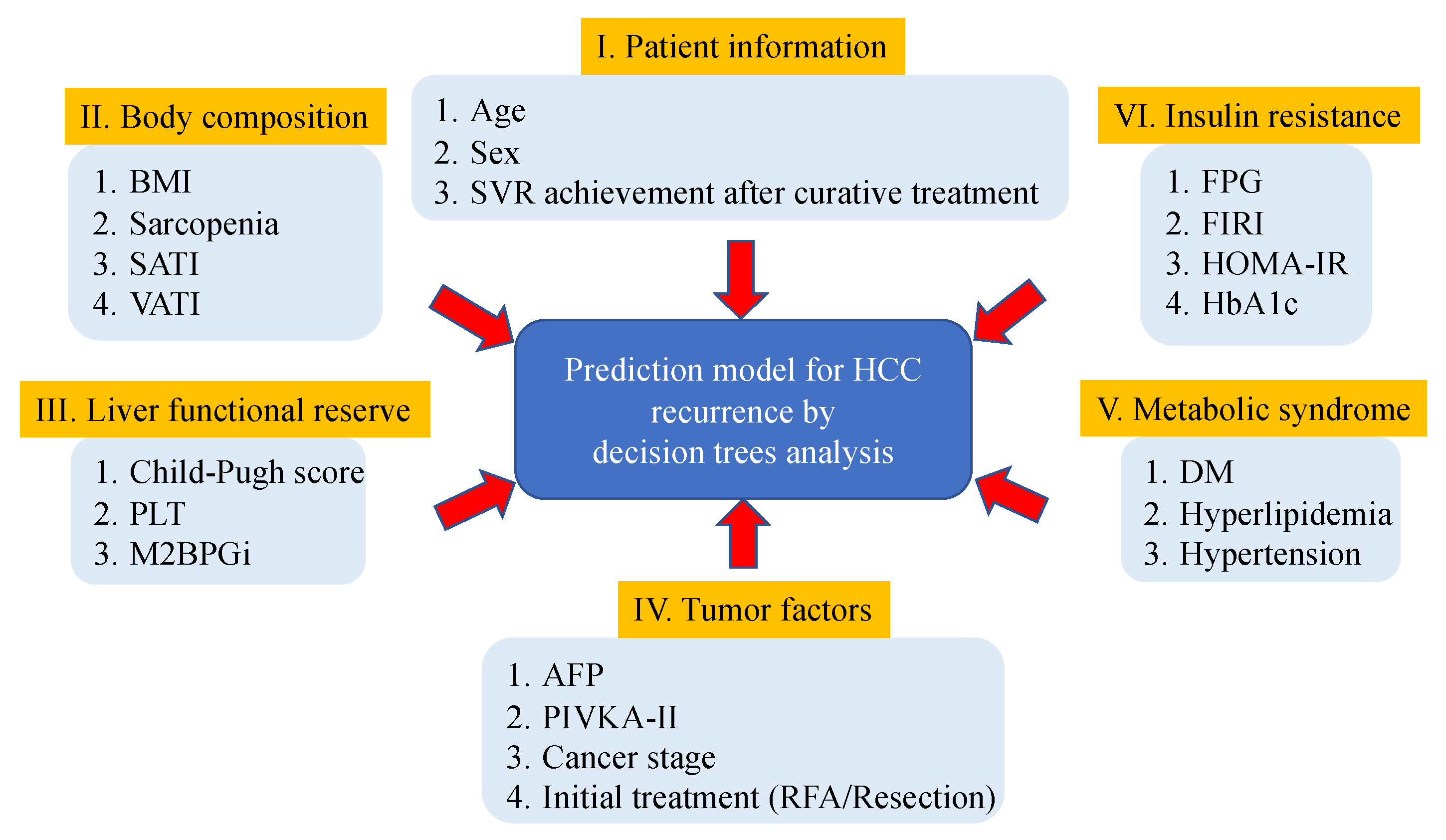
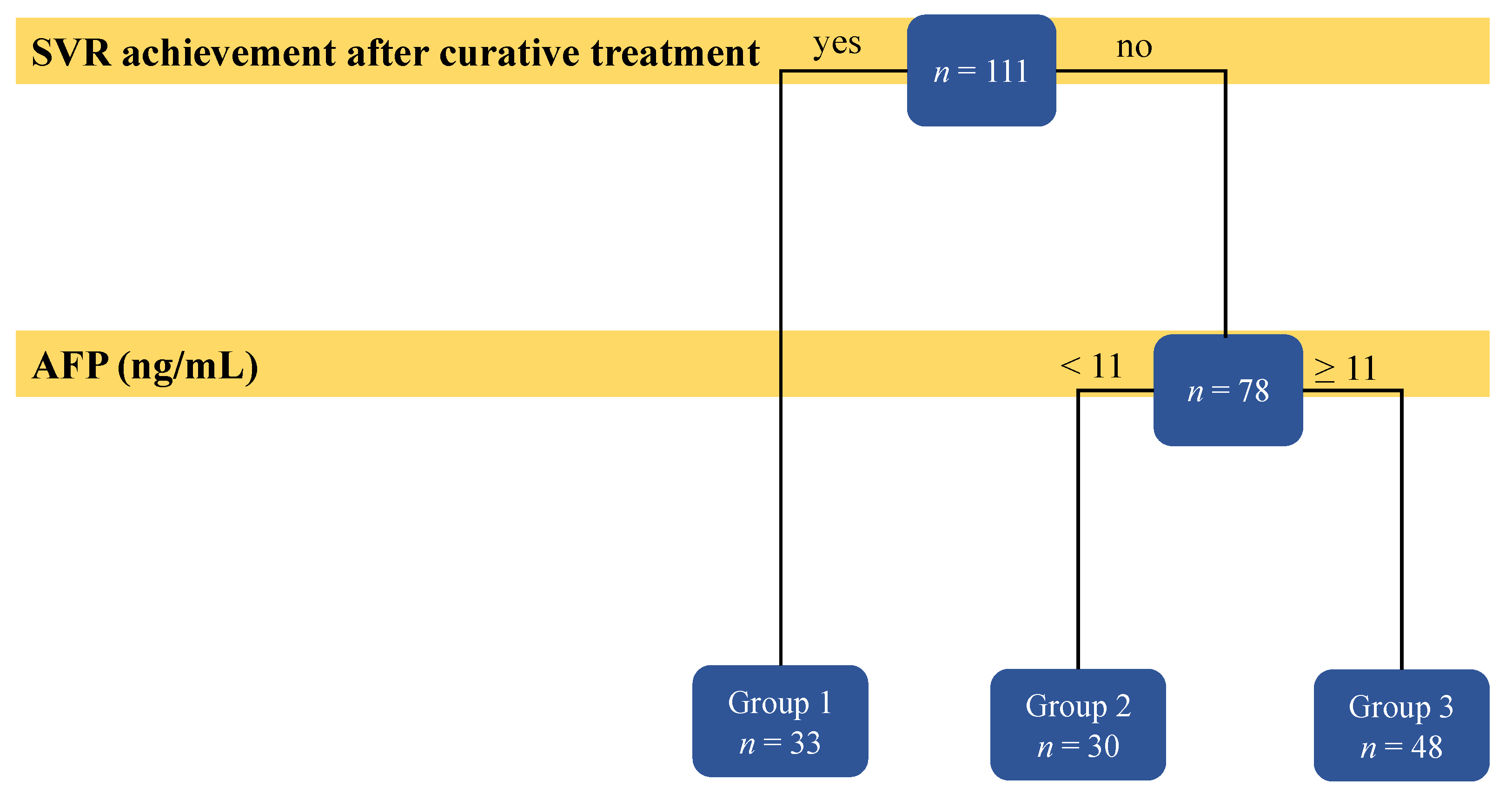
2.2. Decision Tree Analysis of Risk Factors Affecting Recurrence of HCV-Related HCC
2.3. Statistical Analyses
3. Results
3.1. Baseline Characteristics and Laboratory Data of the Participants
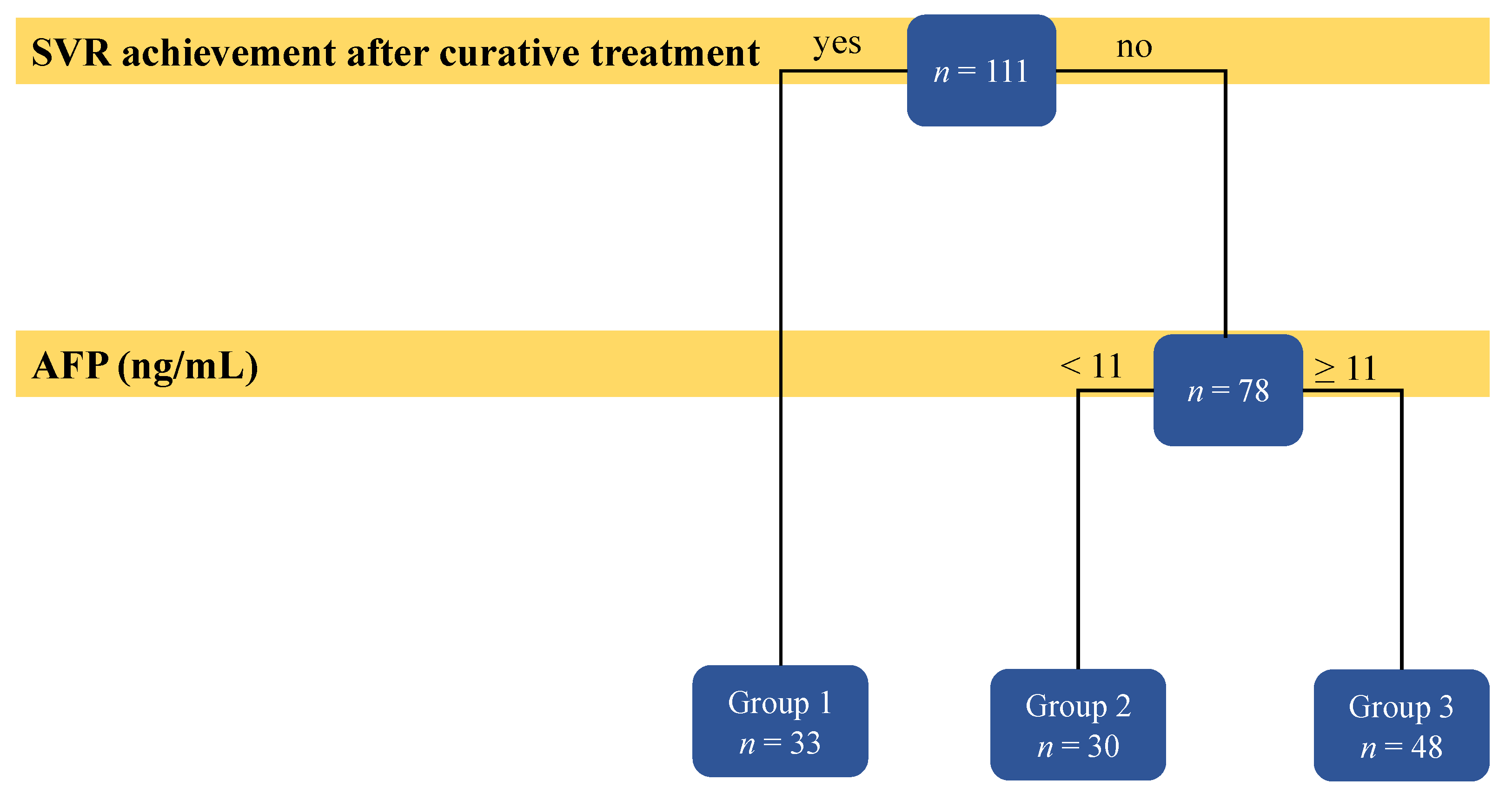
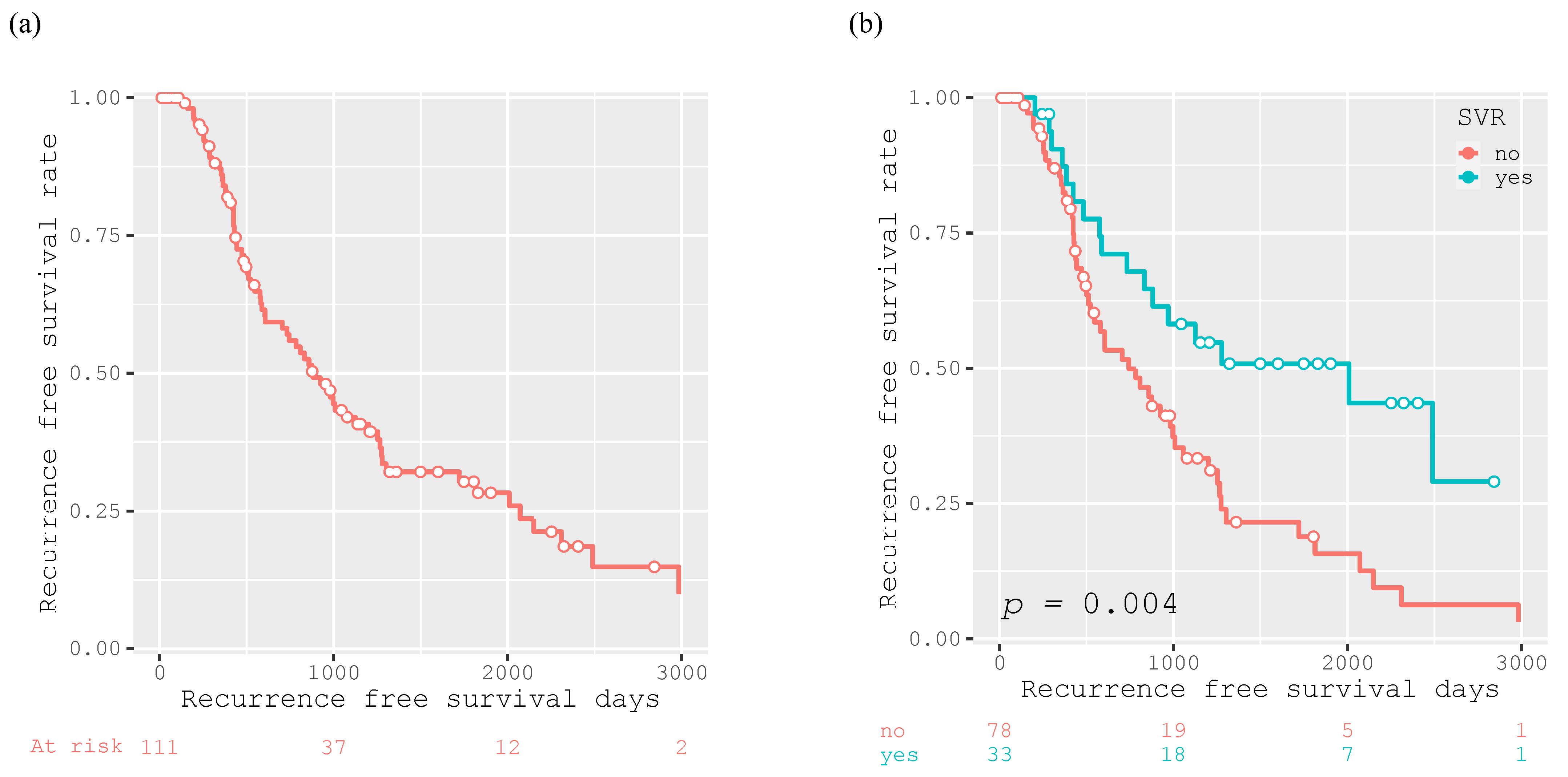
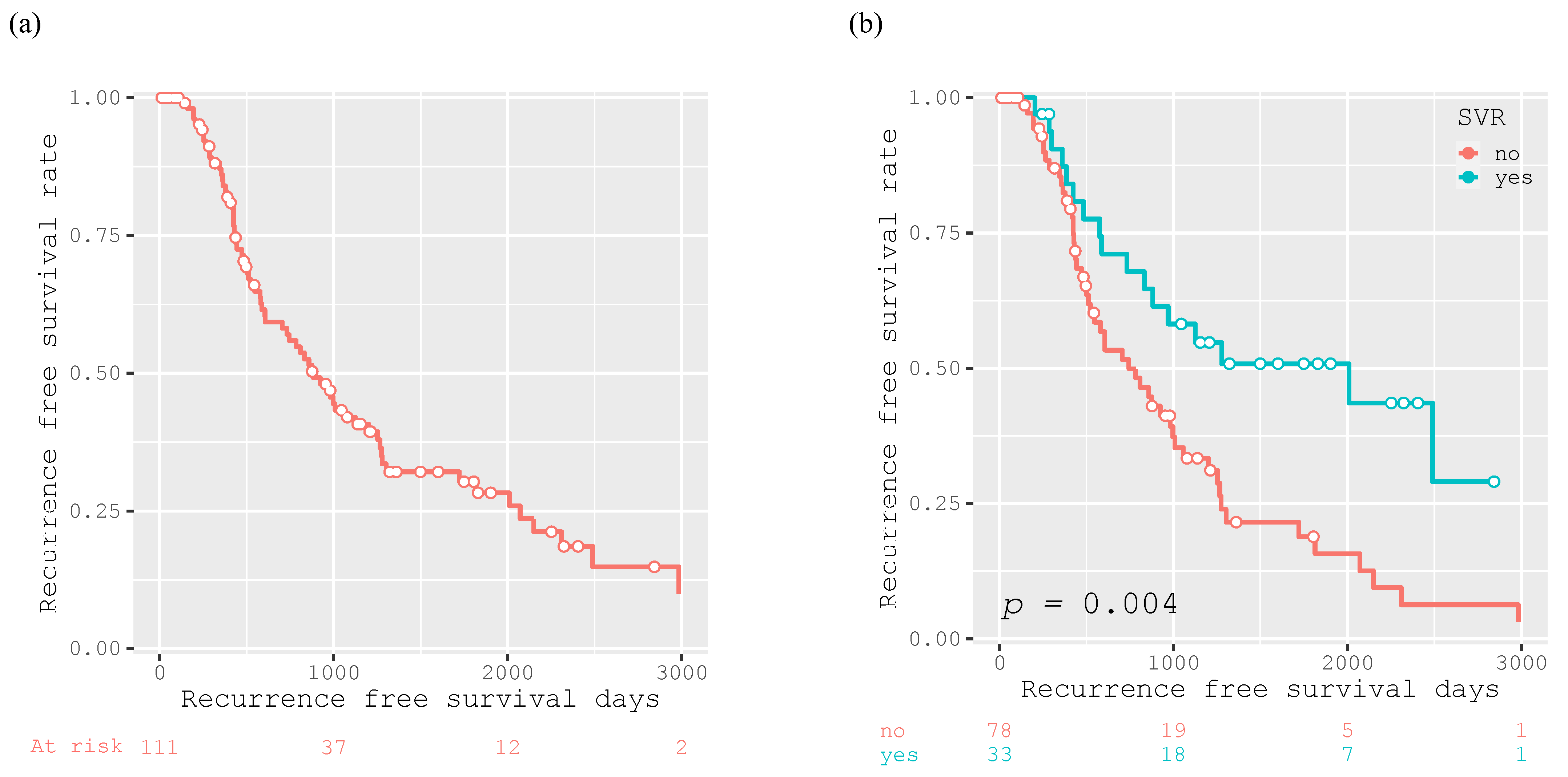
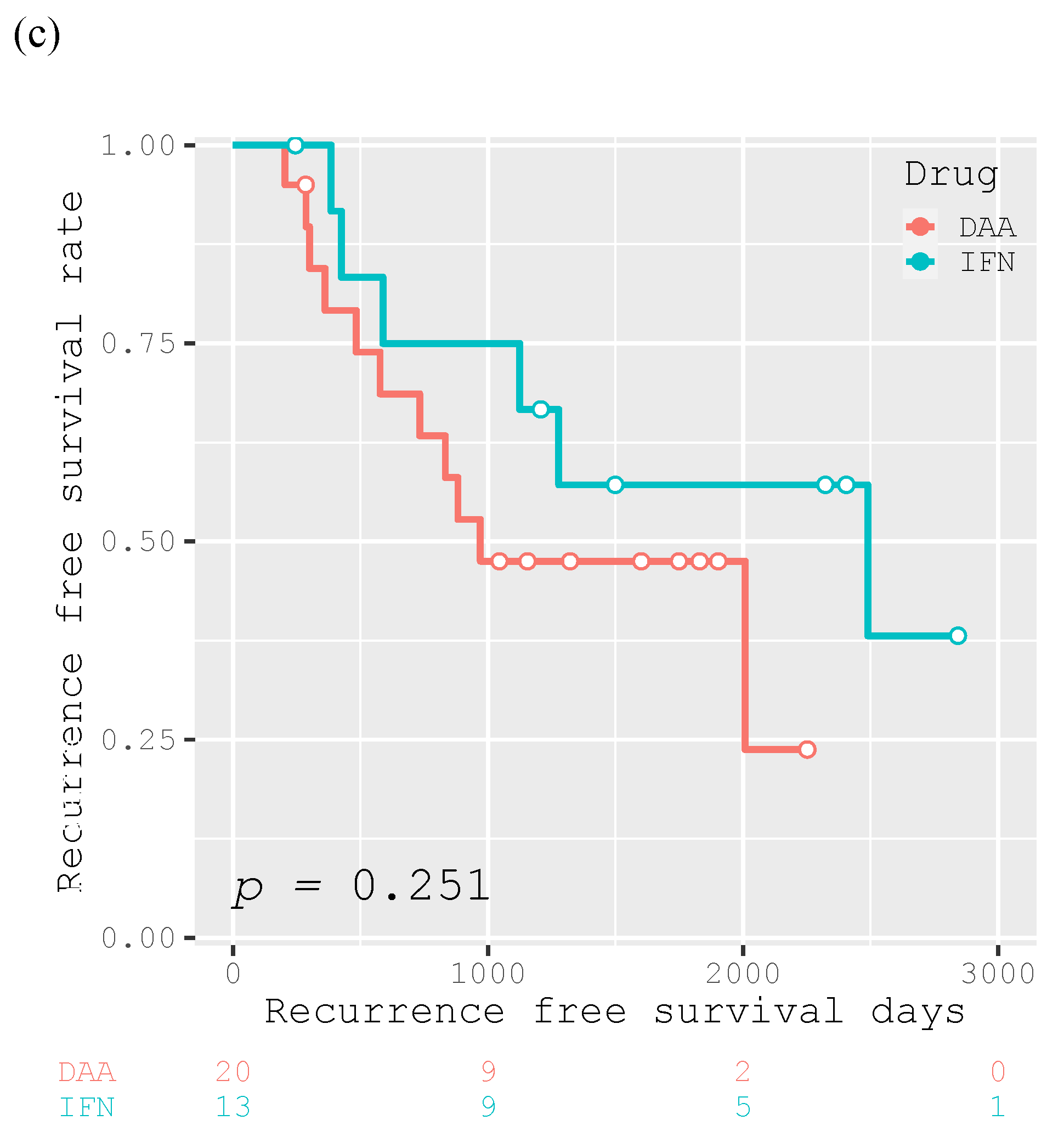
3.2. Risk Factors Affecting HCC Recurrence in HCV-Positive Patients after Curative Treatment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- El-Serag, H.B. Hepatocellular Carcinoma: An Epidemiologic View. J. Clin. Gastroenterol. 2002, 35, S72–S78. [Google Scholar] [CrossRef] [PubMed]
- Bosetti, C.; Turati, F.; la Vecchia, C. Hepatocellular Carcinoma Epidemiology. Best Pract. Res. Clin. Gastroenterol. 2014, 28, 753–770. [Google Scholar] [CrossRef] [PubMed]
- Shiina, S.; Tateishi, R.; Arano, T.; Uchino, K.; Enooku, K.; Nakagawa, H.; Asaoka, Y.; Sato, T.; Masuzaki, R.; Kondo, Y.; et al. Radiofrequency Ablation for Hepatocellular Carcinoma: 10-Year Outcome and Prognostic Factors. Am. J. Gastroenterol. 2012, 107, 569–577, quiz 578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poon, R.T. Prevention of Recurrence after Resection of Hepatocellular Carcinoma: A Daunting Challenge. Hepatology 2011, 54, 757–759. [Google Scholar] [CrossRef] [PubMed]
- Nagashima, I.; Hamada, C.; Naruse, K.; Osada, T.; Nagao, T.; Kawano, N.; Muto, T. Surgical Resection for Small Hepatocellular Carcinoma. Surgery 1996, 119, 40–45. [Google Scholar] [CrossRef]
- Koike, Y.; Shiratori, Y.; Sato, S.; Obi, S.; Teratani, T.; Imamura, M.; Hamamura, K.; Imai, Y.; Yoshida, H.; Shiina, S.; et al. Risk Factors for Recurring Hepatocellular Carcinoma Differ According to Infected Hepatitis Virus-an Analysis of 236 Consecutive Patients with a Single Lesion. Hepatology 2000, 32, 1216–1223. [Google Scholar] [CrossRef]
- Ikeda, K.; Saitoh, S.; Tsubota, A.; Arase, Y.; Chayama, K.; Kumada, H.; Watanabe, G.; Tsurumaru, M. Risk Factors for Tumor Recurrence and Prognosis after Curative Resection of Hepatocellular Carcinoma. Cancer 1993, 71, 19–25. [Google Scholar] [CrossRef]
- Adachi, E.; Maeda, T.; Matsumata, T.; Shirabe, K.; Kinukawa, N.; Sugimachi, K.; Tsuneyoshi, M. Risk Factors for Intrahepatic Recurrence in Human Small Hepatocellular Carcinoma. Gastroenterology 1995, 108, 768–775. [Google Scholar] [CrossRef]
- Imai, K.; Takai, K.; Hanai, T.; Suetsugu, A.; Shiraki, M.; Shimizu, M. Homeostatic Model Assessment of Insulin Resistance for Predicting the Recurrence of Hepatocellular Carcinoma after Curative Treatment. Int. J. Mol. Sci. 2019, 20, 605. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, N.; Takai, K.; Imai, K.; Shimizu, M.; Naiki, T.; Nagaki, M.; Moriwaki, H. Increased Levels of Serum Leptin Are a Risk Factor for the Recurrence of Stage I/II Hepatocellular Carcinoma after Curative Treatment. J. Clin. Biochem. Nutr. 2011, 49, 153–158. [Google Scholar] [CrossRef] [Green Version]
- Imai, K.; Takai, K.; Maeda, T.; Watanabe, S.; Hanai, T.; Suetsugu, A.; Shiraki, M.; Shimizu, M. Increased Visceral Fat Volume Raises the Risk for Recurrence of Hepatocellular Carcinoma after Curative Treatment. Oncotarget 2018, 9, 14058–14067. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suzuki, Y.; Imai, K.; Takai, K.; Hanai, T.; Hayashi, H.; Naiki, T.; Nishigaki, Y.; Tomita, E.; Shimizu, M.; Moriwaki, H. Hepatocellular Carcinoma Patients with Increased Oxidative Stress Levels Are Prone to Recurrence after Curative Treatment: A Prospective Case Series Study Using the d-ROM Test. J. Cancer Res. Clin. Oncol. 2013, 139, 845–852. [Google Scholar] [CrossRef] [PubMed]
- Waziry, R.; Hajarizadeh, B.; Grebely, J.; Amin, J.; Law, M.; Danta, M.; George, J.; Dore, G.J. Hepatocellular Carcinoma Risk Following Direct-Acting Antiviral HCV Therapy: A Systematic Review, Meta-Analyses, and Meta-Regression. J. Hepatol. 2017, 67, 1204–1212. [Google Scholar] [CrossRef]
- Kanwal, F.; Kramer, J.; Asch, S.M.; Chayanupatkul, M.; Cao, Y.; El-Serag, H.B. Risk of Hepatocellular Cancer in HCV Patients Treated With Direct-Acting Antiviral Agents. Gastroenterology 2017, 153, 996–1005.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reig, M.; Mariño, Z.; Perelló, C.; Iñarrairaegui, M.; Ribeiro, A.; Lens, S.; Díaz, A.; Vilana, R.; Darnell, A.; Varela, M.; et al. Unexpected High Rate of Early Tumor Recurrence in Patients with HCV-Related HCC Undergoing Interferon-Free Therapy. J. Hepatol. 2016, 65, 719–726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kokudo, N.; Takemura, N.; Hasegawa, K.; Takayama, T.; Kubo, S.; Shimada, M.; Nagano, H.; Hatano, E.; Izumi, N.; Kaneko, S.; et al. Clinical Practice Guidelines for Hepatocellular Carcinoma: The Japan Society of Hepatology 2017 (4th JSH-HCC Guidelines) 2019 Update. Hepatol. Res. 2019, 49, 1109–1113. [Google Scholar] [CrossRef]
- Quinlan, J.R. Induction of Decision Trees. Mach. Learn. 1986, 1, 81–106. [Google Scholar] [CrossRef] [Green Version]
- Nishikawa, H.; Shiraki, M.; Hiramatsu, A.; Moriya, K.; Hino, K.; Nishiguchi, S. Japan Society of Hepatology Guidelines for Sarcopenia in Liver Disease (1st Edition): Recommendation from the Working Group for Creation of Sarcopenia Assessment Criteria. Hepatol. Res. 2016, 46, 951–963. [Google Scholar] [CrossRef]
- El-Serag, H.B.; Hampel, H.; Javadi, F. The Association between Diabetes and Hepatocellular Carcinoma: A Systematic Review of Epidemiologic Evidence. Clin. Gastroenterol. Hepatol. 2006, 4, 369–380. [Google Scholar] [CrossRef]
- Falade-Nwulia, O.; Suarez-Cuervo, C.; Nelson, D.R.; Fried, M.W.; Segal, J.B.; Sulkowski, M.S. Oral Direct-Acting Agent Therapy for Hepatitis c Virus Infection: A Systematic Review. Ann. Intern. Med. 2017, 166, 637–648. [Google Scholar] [CrossRef] [Green Version]
- Foster, G.R.; Irving, W.L.; Cheung, M.C.M.; Walker, A.J.; Hudson, B.E.; Verma, S.; McLauchlan, J.; Mutimer, D.J.; Brown, A.; Gelson, W.T.H.; et al. Impact of Direct Acting Antiviral Therapy in Patients with Chronic Hepatitis C and Decompensated Cirrhosis. J. Hepatol. 2016, 64, 1224–1231. [Google Scholar] [CrossRef] [PubMed]
- Tahata, Y.; Hikita, H.; Mochida, S.; Kawada, N.; Enomoto, N.; Ido, A.; Yoshiji, H.; Miki, D.; Hiasa, Y.; Takikawa, Y.; et al. Sofosbuvir plus Velpatasvir Treatment for Hepatitis C Virus in Patients with Decompensated Cirrhosis: A Japanese Real-World Multicenter Study. J. Gastroenterol. 2021, 56, 67–77. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.M.; Stepanova, M.; Afdhal, N.; Kowdley, K.V.; Zeuzem, S.; Henry, L.; Hunt, S.L.; Marcellin, P. Improvement of Health-Related Quality of Life and Work Productivity in Chronic Hepatitis C Patients with Early and Advanced Fibrosis Treated with Ledipasvir and Sofosbuvir. J. Hepatol. 2015, 63, 337–345. [Google Scholar] [CrossRef] [PubMed]
- Deterding, K.; Höner zu Siederdissen, C.; Port, K.; Solbach, P.; Sollik, L.; Kirschner, J.; Mix, C.; Cornberg, J.; Worzala, D.; Mix, H.; et al. Improvement of Liver Function Parameters in Advanced HCV-Associated Liver Cirrhosis by IFN-Free Antiviral Therapies. Aliment. Pharmacol. Ther. 2015, 42, 889–901. [Google Scholar] [CrossRef]
- Colombo, M. Screening for Cancer in Viral Hepatitis. Clin. Liver Dis. 2001, 5, 109–122. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | (n = 111) |
|---|---|
| Sex (male/female) | 73/38 |
| Age (years) | 71.7 ± 8.1 |
| BMI (kg/m2) | 22.3 ± 3.0 |
| Sarcopenia (yes/no) | 44/67 |
| SATI (cm2/m2) | 36.5 ± 22.3 |
| VATI (cm2/m2) | 33.1 ± 23.2 |
| Diabetes mellitus (yes/no) | 32/79 |
| Hypertension (yes/no) | 42/69 |
| Hyperlipidemia (yes/no) | 1/110 |
| FPG (mg/dL) | 107.6 ± 29.6 |
| FIRI (µIU/mL) | 10.9 ± 9.7 |
| HOMA-IR | 2.9 ± 3.1 |
| HbA1c (%) | 5.9 ± 1.1 |
| Child-Pugh score (5/6/7/8/9/10) | 60/30/14/5/1/1 |
| M2BPGi (C.O.I) | 5.0 ± 3.6 |
| PLT (×104/µL) | 11.7 ± 5.5 |
| Stage (I/II/III/IV) | 50/47/13/1 |
| AFP (ng/mL) | 417 ± 2039 |
| PIVKA-II (mAU/mL) | 759 ± 3268 |
| Initial treatment (resection/RFA) | 41/70 |
| SVR achievement after curative treatment (yes/no) | 33/78 |
| Variables | Group 1 | Group 2 | Group 3 | p-Value |
|---|---|---|---|---|
| Sex (male/female) | 24/9 | 22/8 | 27/21 | 0.210 |
| Age (years) | 70.4 ± 7.4 | 74.4 ± 8.4 | 70.8 ± 8.1 | 0.092 |
| BMI (kg/m2) | 21.5 ± 3.0 | 22.5 ± 3.3 | 22.7 ± 2.8 | 0.240 |
| Sarcopenia (yes/no) | 12/21 | 13/17 | 19/29 | 0.827 |
| SATI (cm2/m2) | 32.9 ± 23.7 | 35.3 ± 23.7 | 39.7 ± 20.2 | 0.374 |
| VATI (cm2/m2) | 28.8 ± 20.5 | 36.0 ± 26.5 | 34.1 ± 22.8 | 0.432 |
| Diabetes mellitus (yes/no) | 9/24 | 9/21 | 14/34 | 1.000 |
| Hypertension (yes/no) | 18/15 | 10/20 | 14/34 | 0.069 |
| Hyperlipidemia (yes/no) | 0/33 | 0/30 | 1/47 | 1.000 |
| FPG (mg/dL) | 108.7 ± 23.5 | 110.2 ± 45.9 | 105.2 ± 19.8 | 0.753 |
| FIRI (µIU/mL) | 12.5 ± 11.1 | 9.8 ± 11.7 | 10.5 ± 7.1 | 0.558 |
| HOMA-IR | 3.4 ± 3.1 | 2.7 ± 4.5 | 2.8 ± 2.0 | 0.665 |
| HbA1c (%) | 6.0 ± 1.1 | 6.0 ± 1.5 | 5.8 ± 0.8 | 0.563 |
| Child-Pugh score (5/6/7/8/9/10) | 18/9/5/1/00 | 19/5/4/1/0/1 | 23/16/5/3/1/0 | 0.741 |
| M2BPGi (C.O.I) | 5.1 ± 5.1 | 4.4 ± 2.8 | 5.3 ± 2.9 | 0.880 |
| PLT (×104/µL) | 12.4 ± 5.4 | 13.5 ± 5.9 | 10.1 ± 4.9 | 0.211 |
| Stage (I/II/III/IV) | 15/16/2/0 | 15/11/3/1 | 20/20/8/0 | 0.560 |
| AFP (ng/mL) | 288.6 ± 727.8 | 4.9 ± 2.7 | 763.9 ± 3022.6 | 0.256 |
| PIVKA-II (mAU/mL) | 1137.9 ± 5026.9 | 385.2 ± 1297.2 | 734.1 ± 2305.2 | 0.662 |
| Initial treatment (resection/RFA) | 15/18 | 11/19 | 15/33 | 0.672 |
| Median RFS (days) | 2009 | 1267 | 501 | <0.001 |
| Variables | HR (95% CI) | p-Value |
|---|---|---|
| Sex (male vs. female) | 0.978 (0.594–1.611) | 0.932 |
| Age (years) | 0.999 (0.965–1.035) | 0.971 |
| BMI (kg/m2) | 1.028 (0.950–1.112) | 0.487 |
| Sarcopenia (yes vs. no) | 0.739 (0.448–1.220) | 0.238 |
| SATI (cm2/m2) | 1.004 (0.993–1.015) | 0.428 |
| VATI (cm2/m2) | 1.005 (0.994–1.015) | 0.352 |
| Diabetes mellitus (yes vs. no) | 0.853 (0.493–1.477) | 0.572 |
| Hypertension (yes vs. no) | 0.930 (0.571–1.516) | 0.773 |
| Hyperlipidemia (yes vs. no) | 2.368 (0.323–17.33) | 0.396 |
| FPG (mg/dL) | 0.994 (0.983–1.004) | 0.246 |
| FIRI (µIU/mL) | 1.009 (0.989–1.029) | 0.365 |
| HOMA-IR | 1.022 (0.961–1.087) | 0.491 |
| HbA1c (%) | 0.810 (0.620–1.059) | 0.124 |
| Child-Pugh score | 1.042 (0.794–1.367) | 0.766 |
| M2BPGi (C.O.I) | 0.932(0.778–1.117) | 0.447 |
| PLT (×104/µL) | 0.962 (0.918–1.008) | 0.105 |
| Stage | 1.365 (0.948–1.965) | 0.093 |
| AFP (≥11 vs. <11 ng/mL) | 1.619 (0.981–2.673) | 0.059 |
| Initial treatment (RFA vs. resection) | 1.166 (0.708–1.917) | 0.546 |
| SVR achievement (yes vs. no) | 0.449 (0.257–0.783) | 0.005 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Imai, K.; Takai, K.; Unome, S.; Miwa, T.; Maeda, T.; Hanai, T.; Shirakami, Y.; Suetsugu, A.; Shimizu, M. Sustained Virological Response Is the Most Effective in Preventing Hepatocellular Carcinoma Recurrence after Curative Treatment in Hepatitis C Virus-Positive Patients: A Study Using Decision Tree Analysis. Int. J. Transl. Med. 2022, 2, 345-354. https://doi.org/10.3390/ijtm2030027
Imai K, Takai K, Unome S, Miwa T, Maeda T, Hanai T, Shirakami Y, Suetsugu A, Shimizu M. Sustained Virological Response Is the Most Effective in Preventing Hepatocellular Carcinoma Recurrence after Curative Treatment in Hepatitis C Virus-Positive Patients: A Study Using Decision Tree Analysis. International Journal of Translational Medicine. 2022; 2(3):345-354. https://doi.org/10.3390/ijtm2030027
Chicago/Turabian StyleImai, Kenji, Koji Takai, Shinji Unome, Takao Miwa, Toshihide Maeda, Tatsunori Hanai, Yohei Shirakami, Atsushi Suetsugu, and Masahito Shimizu. 2022. "Sustained Virological Response Is the Most Effective in Preventing Hepatocellular Carcinoma Recurrence after Curative Treatment in Hepatitis C Virus-Positive Patients: A Study Using Decision Tree Analysis" International Journal of Translational Medicine 2, no. 3: 345-354. https://doi.org/10.3390/ijtm2030027
APA StyleImai, K., Takai, K., Unome, S., Miwa, T., Maeda, T., Hanai, T., Shirakami, Y., Suetsugu, A., & Shimizu, M. (2022). Sustained Virological Response Is the Most Effective in Preventing Hepatocellular Carcinoma Recurrence after Curative Treatment in Hepatitis C Virus-Positive Patients: A Study Using Decision Tree Analysis. International Journal of Translational Medicine, 2(3), 345-354. https://doi.org/10.3390/ijtm2030027