
Membrane Lipid Replacement with Glycerolphospholipids Slowly Reduces Self-Reported Symptom Severities in Chemically Exposed Gulf War Veterans


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Study Design
2.3. Statistics
3. Results
3.1. Subjects in the Study
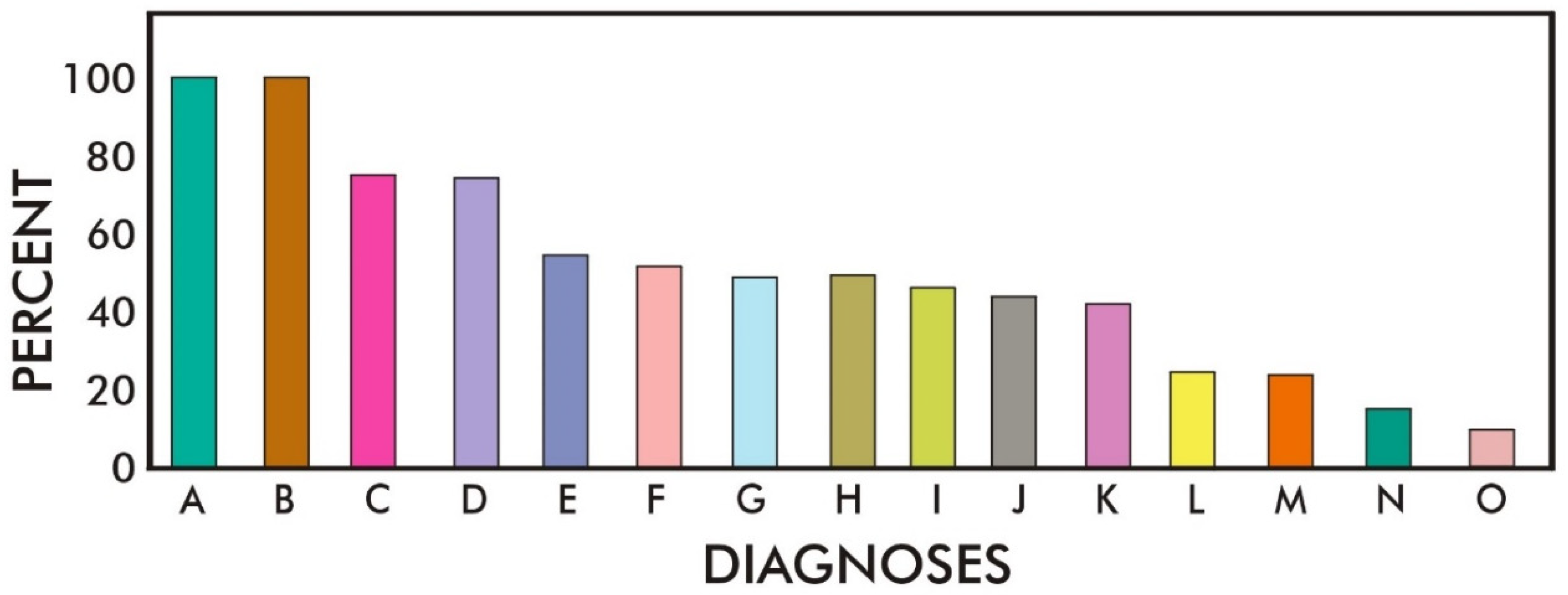
3.2. Toxic Exposures
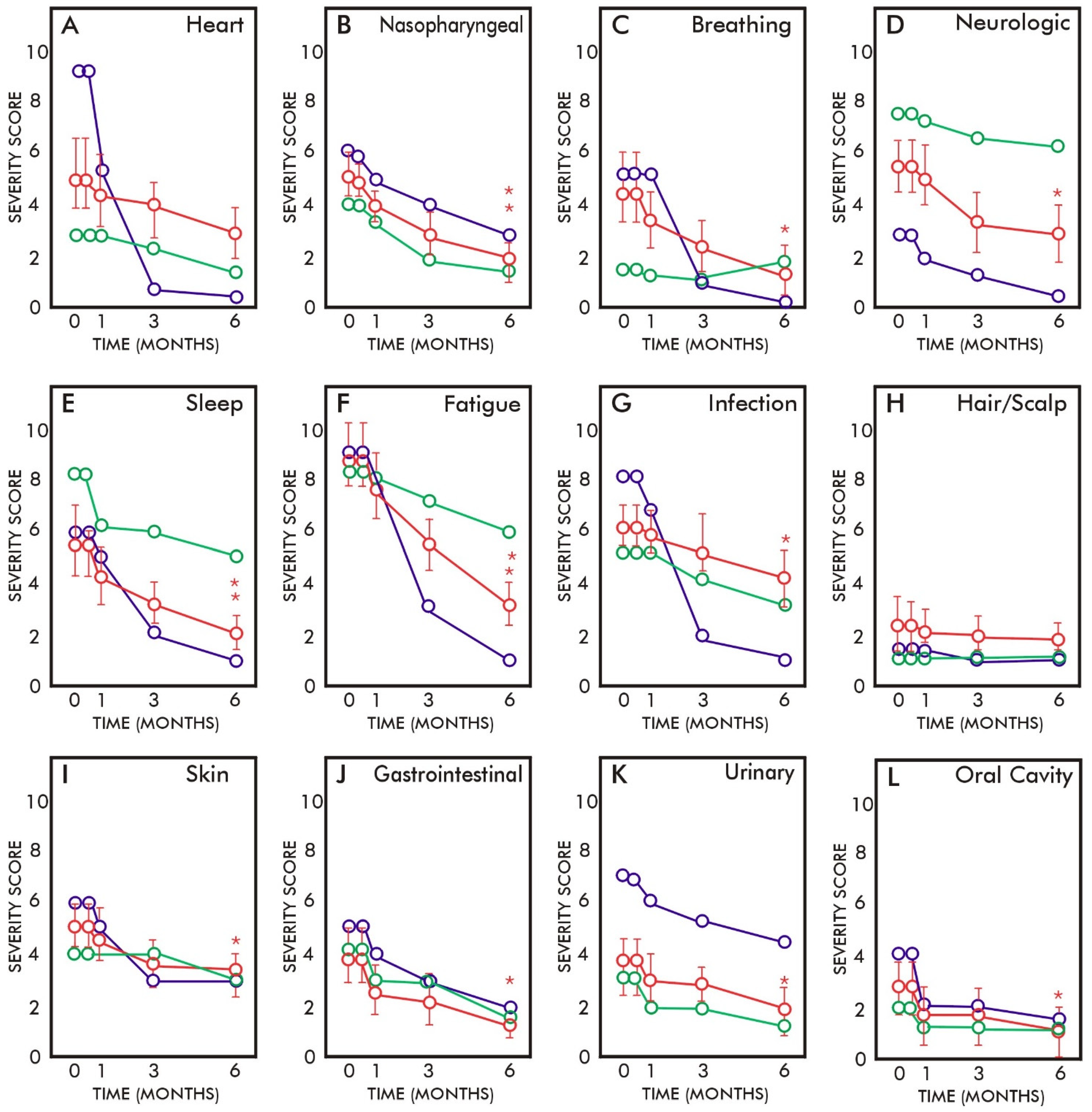
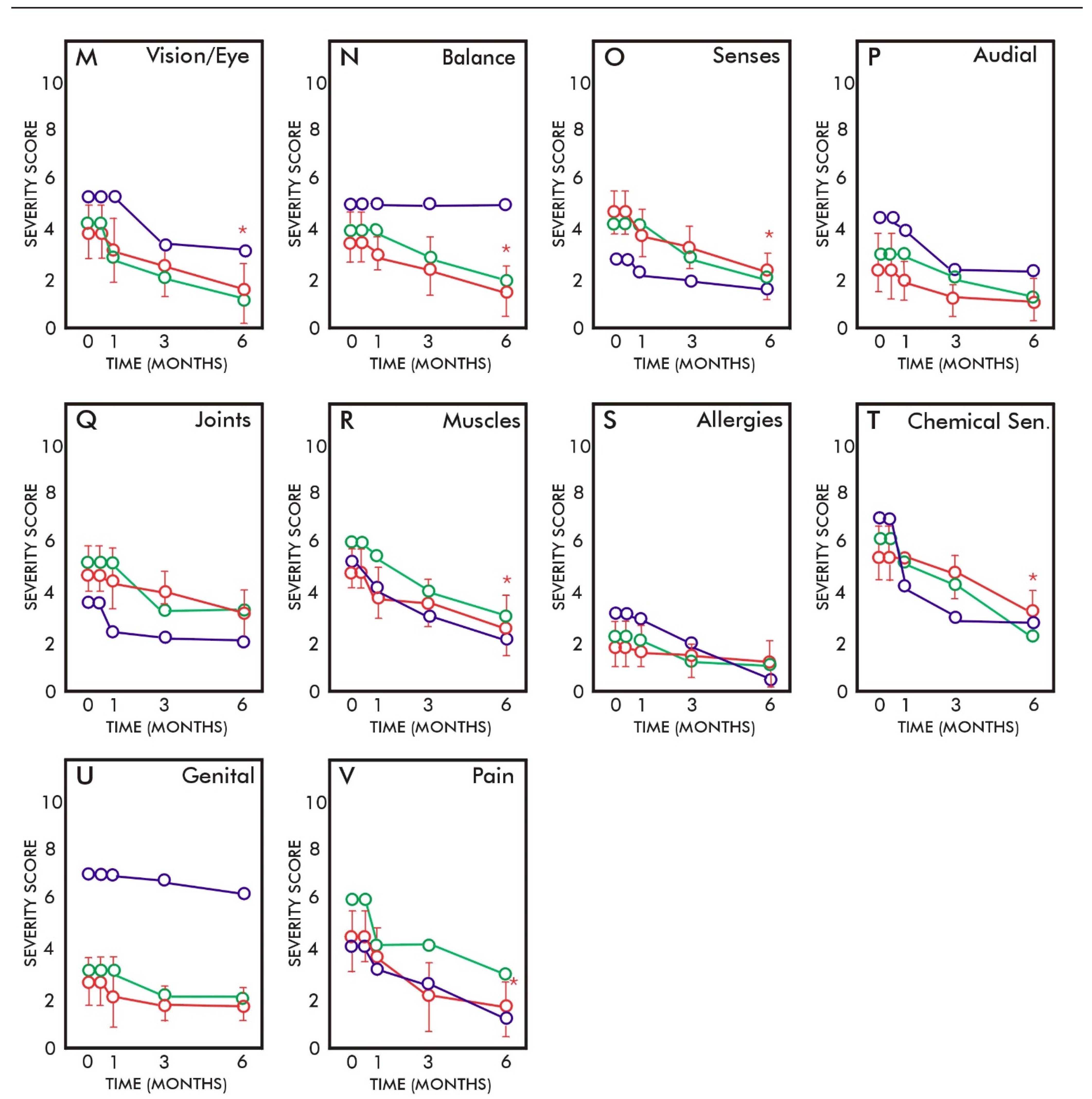
3.3. Symptom Severities during the Study
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Research Advisory Committee on Gulf War Veterans’ Illnesses. Gulf War Illness and the Health of Gulf War Veterans: Scientific Findings and Recommendations; U.S. Government Printing Office: Washington, DC, USA, 2008. Available online: https://www.va.gov/rac-gwvi/docs/Committee_Documents/GWIandHealthofGWVeterans_RAC-GWVIReport_2008.pdf (accessed on 22 April 2022).
- White, R.F.; Steele, L.; O’Callaghan, P.P.; Sullivan, K.; Binns, J.H.; Golomb, B.A.; Bloom, F.E.; Bunker, J.A.; Crawford, F.; Graves, J.C.; et al. Recent research on Gulf War Illness and other health problems in veterans of the 1991 Gulf War: Effects of toxicant exposures during deployment. Cortex 2016, 74, 449–475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fukuda, K.; Nisenbaum, R.; Stewart, M.A.; Thompson, W.W.; Robin, L.; Washko, R.M.; Noah, D.L.; Barrett, D.H.; Randall, B.; Herwaldt, B.L.; et al. Chronic multisymptom illness affecting Air Force veterans of the Gulf War. JAMA 1998, 280, 981–988. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.K.; Mahan, C.M.; Lee, K.Y.; Magee, C.A.; Murphy, F.M. Illnesses among United States veterans of the Gulf War: A population-based survey of 30,000 veterans. J. Occup. Environ. Med. 2000, 42, 491–501. [Google Scholar] [CrossRef] [PubMed]
- Doebbeling, B.N.; Clarke, W.R.; Watson, D.; Torner, J.C.; Woolson, R.F.; Voelker, M.D.; Barrett, D.H.; Schwartz, D.A. Is there a Persian Gulf War syndrome? Evidence from a large population-based survey of veterans and nondeployed controls. Am. J. Med. 2000, 108, 695–704. [Google Scholar] [CrossRef]
- Proctor, S.P.; Heeren, T.; White, R.F.; Wolfe, J.; Borgos, M.S.; Davis, J.D.; Pepper, L.; Clapp, R.; Sutker, P.B.; Vasteerling, J.J.; et al. Health status of Persian Gulf War veterans: Self-reported symptoms, environmental exposures and the effect of stress. Int. J. Epidemiol. 1998, 27, 1000–1010. [Google Scholar] [CrossRef]
- Nicolson, G.L.; Berns, P.; Nasralla, M.; Haier, J.; Nicolson, N.L.; Nass, M. Gulf War Illnesses: Chemical, radiological and biological exposures resulting in chronic fatiguing illnesses can be identified and treated. J. Chronic Fatigue Syndr. 2003, 11, 135–154. [Google Scholar] [CrossRef]
- Yee, M.K.; Janulewicz, P.A.; Seichepine, D.R.; Sullivan, K.A.; Proctor, S.P.; Krengel, M.H. Multiple mild traumatic brain injuries are associated with increased rates of health symptoms and Gulf War illness in a cohort of 1990–1991 Gulf War veterans. Brain Sci. 2017, 7, 79. [Google Scholar] [CrossRef]
- Golomb, B.A. Acetylcholinesterase inhibitors and Gulf War Illnesses. Proc. Natl. Acad. Sci. USA 2008, 105, 4295–4300. [Google Scholar] [CrossRef] [Green Version]
- Nicolson, G.L.; Nasralla, M.; Nicolson, N.L.; Haier, J. High prevalence of mycoplasmal infections in symptomatic (Chronic Fatigue Syndrome) family members of mycoplasma-positive Gulf War Illness patients. J. Chronic Fatigue Syndr. 2003, 11, 21–36. [Google Scholar] [CrossRef]
- Nicolson, G.L.; Nasralla, M.; Haier, J.; Pomfret, J. High frequency of systemic mycoplasmal infections in Gulf War veterans and civilians with Amytrophic Lateral Sclerosis (ALS). J. Clin. Neurosci. 2002, 9, 525–529. [Google Scholar] [CrossRef] [Green Version]
- Korényi-Both, A.L.; Korényi-Both, A.L.; Juncer, J.A. Al-Eskan disease: Pursian Gulf Syndrome. Mil. Med. 1997, 162, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hodgson, M.J.; Kipen, H.M. Gulf War Illnesses: Causation and treatment. J. Occup. Environ. Med. 1999, 41, 443–452. [Google Scholar] [CrossRef] [PubMed]
- Nicolson, G.L.; Ash, M.E. Membrane Lipid Replacement for chronic illnesses, aging and cancer using oral glycerolphospholipid formulations with fructooligosaccharides to restore phospholipid function in cellular membranes, organelles, cells and tissues. Biochim. Biophys. Acta Biomembr. 2017, 1859, 1704–1724. [Google Scholar] [CrossRef] [PubMed]
- Nicolson, G.L.; Ferreira de Mattos, G.; Ash, M.; Settineri, R.; Escribá, P.V. Fundamentals of Membrane Lipid Replacement, a natural medicine approach to reducing fatigue, pain, and other symptoms while restoring function in chronic illnesses and aging. Membranes 2021, 11, 944. [Google Scholar] [CrossRef]
- Nicolson, G.L.; Ferreira de Mattos, G. A brief introduction to some aspects of the Fluid—Mosaic Model of membrane structure and its importance to Membrane Lipid Replacement. Membranes 2021, 11, 947. [Google Scholar] [CrossRef]
- Mayor, S.; Presley, J.F.; Maxfield, F.R. Sorting of membrane components from endosomes and subsequent recycling to the cell surface occurs by a bulk flow process. J. Cell Biol. 1993, 121, 1257–1269. [Google Scholar] [CrossRef] [Green Version]
- Nicolson, G.L.; Breeding, P.C. Membrane Lipid Replacement for reduction of pain, fatigue, gastrointestinal and other symptoms in patients with peripheral pain: Case reports. Case Rep. Rev. 2020, 1, 1–3. [Google Scholar] [CrossRef]
- Nicolson, G.L. Membrane Lipid Replacement: Clinical studies using a natural medicine approach to restoring membrane function and improving health. Int. J. Clin. Med. 2016, 7, 133–143. [Google Scholar] [CrossRef] [Green Version]
- Nicolson, G.L.; Breeding, P.C.; Settineri, R.; Ferreira de Mattos, G. Aging and chronic illnesses: Membrane Lipid Replacement for restoring mitochondrial function and reducing fatigue, pain, and other symptoms in aged individuals. Bioact. Comp. Health Dis. 2020, 3, 194–203. [Google Scholar] [CrossRef]
- Steele, L. Prevalence and patterns of gulf war illness in Kansas veterans: Association of symptoms with characteristics of person, place, and time of military service. Am. J. Epidemol. 2000, 152, 992–1002. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Statistical notes: Cronbach’s alpha. Br. Med. J. 1997, 314, 572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abou-Donia, M.B.; Conboy, L.A.; Kokkotou, E.; Jacobson, E.; Elmasry, E.M.; Elkafrawy, P.; Neely, M.; Bass, C.R.; Sullivan, K. Screening for novel central nervous system biomarkers in veterans with gulf war illness. Neurotoxicol. Teratol. 2017, 61, 36–46. [Google Scholar] [CrossRef] [PubMed]
- Nicolson, G.L.; Nicolson, N.L. Diagnosis and treatment of mycoplasmal infections in Persian Gulf War Illness-CFIDS patients. Int. J. Occup. Med. Immunol. Toxicol. 1996, 5, 69–78. [Google Scholar]
- Vojdani, A.; Franco, A.R. Multiplex PCR for the detection of Mycoplasma fermentans, M. hominis and M. penetrans in patients with Chronic Fatigue Syndrome, Fibromyalgia, Rheumatoid Arthritis and Gulf War Illness. J. Chronic Fatigue Syndr. 1999, 5, 187–197. [Google Scholar] [CrossRef]
- Sartin, J.S. Gulf War Illnesses: Causes and controversies. Mayo Clinic Proc. 2000, 75, 811–819. [Google Scholar] [CrossRef] [Green Version]
- Abou-Donia, M.B.; Wilmarth, K.R. Neurotoxicity resulting from coexposure to pyridostigmine bromide, DEET and permethrin: Implications of Gulf War exposures. J. Toxicol. Environ. Health 1996, 48, 35–56. [Google Scholar] [CrossRef]
- Haley, R.W.; Kurt, T.L. Self-reported exposure to neurotoxic chemical combinations in the Gulf War. A cross-sectional epidemiologic study. JAMA 1997, 277, 231–237. [Google Scholar] [CrossRef]
- Koslik, H.J.; Hamilton, G.; Golomb, B.A. Mitochondrial dysfunction in Gulf War Illness revealed by 31Phosphorus magnetic resonance spectroscopy: A case-control study. PLoS ONE 2014, 9, e92887. [Google Scholar] [CrossRef] [Green Version]
- Hernández-Camacho, J.D.; Bernier, M.; López-Lluch, G.; Navas, P. Coenzyme Q10 supplementation in aging and disease. Front. Physiol. 2018, 9, 44. [Google Scholar] [CrossRef] [Green Version]
- Golomb, B.A.; Allison, M.; Koperski, S.; Koslik, H.J.; Devaraj, S.; Ritchie, J.B. Coenzyme Q10 benefits symptoms in Gulf War veterans: Results of a randomized double-blind study. Neural Comput. 2014, 26, 2594–2651. [Google Scholar] [CrossRef]
- Nicolson, G.L. Mitochondrial dysfunction and chronic disease: Treatment with natural supplements. Integr. Med. 2014, 13, 35–43. [Google Scholar]
- Nicolson, G.L. Mitochondrial dysfunction and chronic disease: Treatment with natural supplements. Altern. Ther. Health Med. 2014, 20 (Suppl. S1), 18–25. [Google Scholar] [PubMed]
- Agadjanyan, M.; Vasilevko, V.; Ghochikyan, A.; Berns, P.; Kesslak, P.; Settineri, R.A.; Nicolson, G.L. Nutritional supplement (NTFactor) restores mitochondrial function and reduces moderately severe fatigue in aged subjects. J. Chronic Fatigue Syndr. 2003, 11, 23–36. [Google Scholar] [CrossRef]
- Nicolson, G.L.; Settineri, R.; Ellithorpe, E. Lipid Replacement Therapy with a glycophospholipid formulation with NADH and CoQ10 significantly reduces fatigue in intractable chronic fatiguing illnesses and chronic Lyme disease. Int. J. Clin. Med. 2012, 3, 164–170. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez, M.J.; Seyfried, T.; Nicolson, G.L.; Barclay, B.; Matta, J.; Vasquez, A.; Agostino, D.D.; Olalde, J.; Duconge, J.; Hunninghake, R.; et al. Mitochondrial correction: A new therapeutic paradigm for cancer and degenerative diseases. J. Orthomol. Med. 2018, 33, 1–20. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Signs or Symptoms from the Trial Symptom Survey Form |
|---|---|
| Heart | palpitations, chest pain, skipped beats, racing pulse, chest pressure |
| Nasopharyngeal | congestion, nasal discharge, sinus pain, sore throat, sneezing, coughing, throat clearing |
| Breathing | unable to breathe deeply, wheezing, shortness of breath |
| Neurological | depression, loss of interest, suicidal thoughts, mood swings, memory loss, irritability, headaches, concentration |
| Sleep | insomnia, nightmares, unrefreshed sleep |
| Fatigue | chronic fatigue, malaise, tiredness |
| Pain | widespread pain, skeletomuscular pain, neck pain, back pain, headache |
| Infections | fever, night sweats, swollen glands, frequent colds, mouth sores |
| Hair/Scalp | hair loss, discoloration, scalp itch |
| Skin | rashes, reddening, itching, peeling, color change, slow wound healing, growths on skin, fungus, sores |
| Gastrointestinal | stomach pain, cramps, flatus, diarrhea, bloating, blood in stool, nausea, vomiting, excessive thirst, loss of interest in food |
| Urinary | bladder control, frequent urination, blood in urine |
| Oral cavity | loose teeth, bleeding gums, abscesses, increased salivation, dry mouth, hoarseness, coated tongue, lip sores |
| Vision | blurred vision, double vision, loss of night vision, loss of acuity. light sensitivity, floaters, twitching, dry eyes, itchy eyes, watery eyes |
| Balance | poor balance, vertigo, steadiness |
| Senses | tinnitus, hearing loss, loss of smell, loss of taste, cold sensitivity |
| Audial | stuttering, difficulty finding words, numbness of lips, drooling |
| Joints | joint pain, loss of mobility, ache |
| Muscles | muscle pain, burning, spasms, ache, cramps, loss of strength, swelling |
| Allergy | increased allergic sensitivities, increased sensitivities to biologicals |
| Genital | genital pain, itching, swelling, impotence |
| Chemical Sensitivity | sensitivities to fumes, exhaust, smoke, fuel |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nicolson, G.L.; Breeding, P.C. Membrane Lipid Replacement with Glycerolphospholipids Slowly Reduces Self-Reported Symptom Severities in Chemically Exposed Gulf War Veterans. Int. J. Transl. Med. 2022, 2, 164-173. https://doi.org/10.3390/ijtm2020014
Nicolson GL, Breeding PC. Membrane Lipid Replacement with Glycerolphospholipids Slowly Reduces Self-Reported Symptom Severities in Chemically Exposed Gulf War Veterans. International Journal of Translational Medicine. 2022; 2(2):164-173. https://doi.org/10.3390/ijtm2020014
Chicago/Turabian StyleNicolson, Garth L., and Paul C. Breeding. 2022. "Membrane Lipid Replacement with Glycerolphospholipids Slowly Reduces Self-Reported Symptom Severities in Chemically Exposed Gulf War Veterans" International Journal of Translational Medicine 2, no. 2: 164-173. https://doi.org/10.3390/ijtm2020014
APA StyleNicolson, G. L., & Breeding, P. C. (2022). Membrane Lipid Replacement with Glycerolphospholipids Slowly Reduces Self-Reported Symptom Severities in Chemically Exposed Gulf War Veterans. International Journal of Translational Medicine, 2(2), 164-173. https://doi.org/10.3390/ijtm2020014