
Trauma-Sensitive Mindfulness for War Refugees: Communication of Preliminary Findings



Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Mindfulness Definitions and Applications
3.1.1. Meditation and Mindfulness
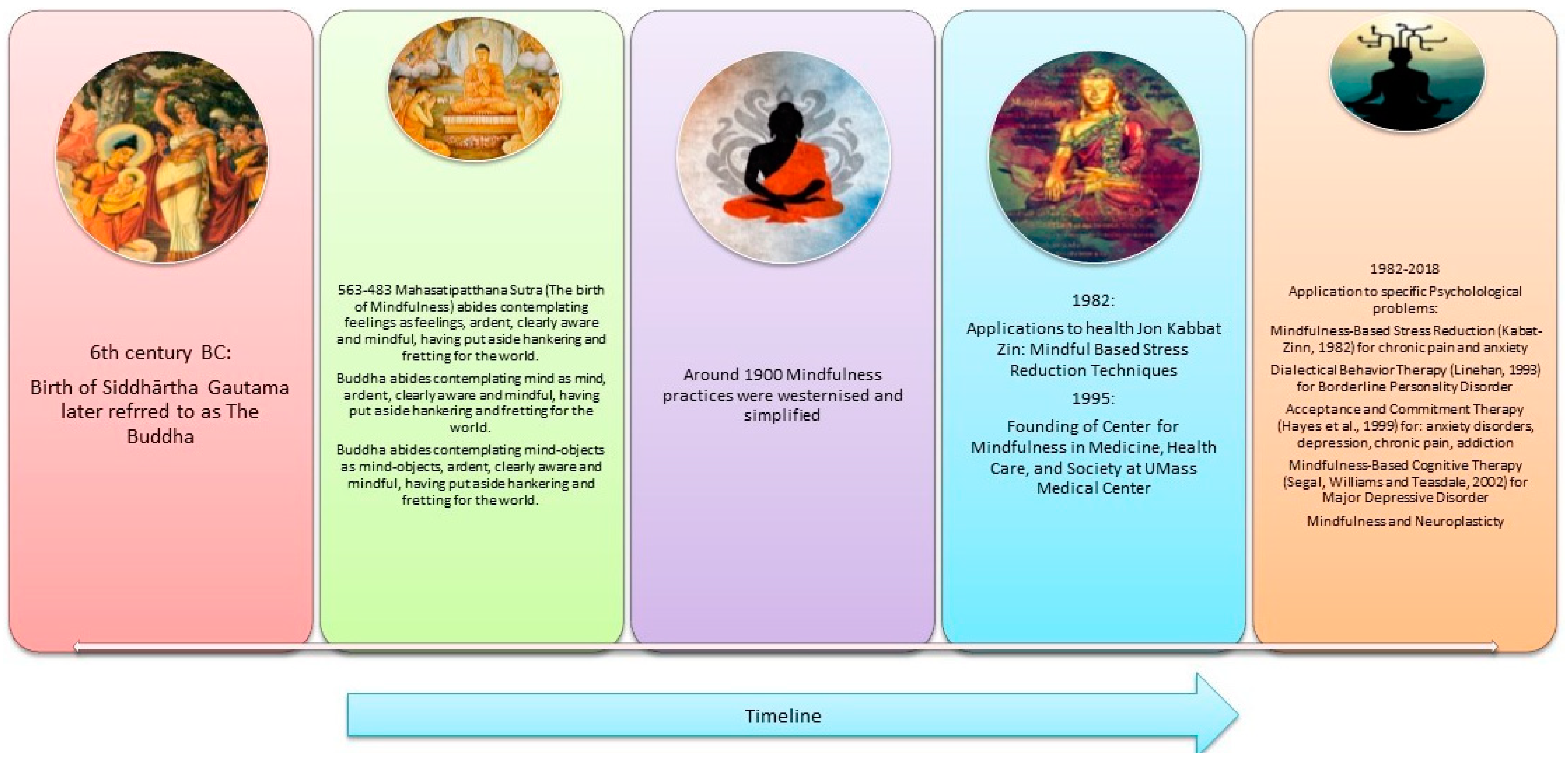
3.1.2. Mindfulness Theory
“The concept of mindfulness is most firmly rooted in Buddhist psychology, but it shares conceptual kinship with ideas advanced by a variety of philosophical and psychological traditions, including ancient Greek philosophy; phenomenology, existentialism, and naturalism in later Western European thought; and transcendentalism and humanism in America”.
- (a)
- The truth of suffering
- (b)
- The truth of the cause of suffering
- (c)
- The truth at the end of suffering
- (d)
- The truth of the path that leads to the end of suffering
“The concept of mindfulness is most firmly rooted in Buddhist psychology, but it shares conceptual kinship with ideas advanced by a variety of philosophical and psychological traditions, including ancient Greek philosophy; phenomenology, existentialism, and naturalism in later Western European thought; and transcendentalism and humanism in America”.
3.1.3. Mindfulness Practice and Its Value
3.1.4. TSM Definitions and Practices in the Treatment of PTSD
"Before we can respond to trauma, we first need to recognise it. As mindfulness providers, it′s up to us to notice nonverbal cues that someone is struggling with traumatic stress. Because of the way mindfulness meditation is generally practiced, this presents a unique challenge. Mental health professionals can assess trauma through direct conversation—reading facial expressions and noticing nonverbal cues—but silent meditation practice minimises such contact. Those of us teaching mindfulness to groups rely heavily on observation”.
3.1.5. Trauma and Polyvagal Theory
“Recruiting and exercising the social engagement system is the ‘go-to’ default activity that humans use to modulate stress. This capacity resides within the social engagement system because positive face-to-face interactions activate neural pathways through the vagus nerve that downregulate the sympathetic activation associated with both exercise and stress”.
3.1.6. Mindfulness from the Perspective of Polyvagal Theory
3.1.7. Mindfulness Meditation and Neuroplasticity: The East-Meets-West Dichotomy
“Neuroplasticity is the capacity of neurons to adapt to a changed environment (FitzGerald & Folan-Curran, 2002). According to Hebbian learning, pre-synaptic terminals change in numbers according to usage and each learning experience strengthens existing neuronal connections (Hebb, 1949).”
3.1.8. Available Psychological Interventions for War-Traumatised Refugees
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Vision. From the Field: Syrian Refugee Crisis: Facts, FAQs, and How to Help. 2018. Available online: https://www.worldvision.org/refugees-news-stories/syrian-refugee-crisis-facts (accessed on 10 July 2022).
- Lindert, J.; Carta, M.G.; Schäfer, I.; Mollica, R.F. Refugees mental health. A public mental health challenge. Eur. J. Public Health 2016, 26, 374–375. [Google Scholar] [CrossRef]
- Follette, V.; Palm, K.M.; Pearson, A.N. Mindfulness and trauma: Implications for treatment. J. Ration. -Emot. Cogn. -Behav. Ther. 2006, 24, 45–61. [Google Scholar] [CrossRef]
- Lin, Y.; Swanson, D.P.; Rogge, R.D. The Three Teachings of East Asia (TTEA) Inventory: Developing and Validating a Measure of the Interrelated Ideologies of Confucianism, Buddhism, and Taoism. Frontiers in Psychology: Cultural Psychology 2021. 2021. Available online: https://www.frontiersin.org/articles/10.3389/fpsyg.2021.626122/full (accessed on 12 July 2022).
- Cuncic, A. The Anxiety Workbook: A 7-Week Plan to Overcome Anxiety, Stop Worrying, and End Panic; Althea Press: Emeryville, CA, USA, 2017. [Google Scholar]
- Kabat-Zinn, J. Coming to Our Senses: Healing Ourselves and the World Through Mindfulness; Hyperion: New York, NY, USA, 2005. [Google Scholar]
- Sigel, D.; Bryson, T. The Whole-Brain Child: 12 Revolutionary Strategies to Nurture Your Child′s Developing Mind; Bantam Books Trade Paperbacks: New York, NY, USA, 2012. [Google Scholar]
- Shapero, B.G.; Greenberg, J.; Pedrelli, P.; de Jong, M.; Desbordes, G. Mindfulness-Based Interventions in Psychiatry. Focus 2018, 16, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Brown, K.W.; Ryan, R.M. The benefits of being present: Mindfulness and its role in psychological wellbeing. J. Personal. Soc. Psychol. 2003, 8, 822–848. [Google Scholar] [CrossRef]
- Greenberg, M. The Stress-Proof Brain: Master Your Emotional Response to Stress Using Mindfulness and Neuroplasticity; Raincoast Books/New Harbinger: Vancouver, BC, Canada, 2017. [Google Scholar]
- Mosby. Mosby’s Medical Dictionary, 9th ed.; Mosby Elsevier: St. Louis, MO, USA, 2013. [Google Scholar]
- Fossas, A. The Basics of Mindfulness: Where did IT Come from? Available online: https://welldoing.org/article/basics-of-mindfulness-come-from (accessed on 19 July 2022).
- Jeebodh-Desai, L. The Implementation Of Trauma-Sensitive Mindfulness By An Educational Psychologist To Address Post-Traumatic Stress Disorder (Ptsd) Of War-Traumatised Refugees. Doctoral Dissertation, University of Johannesburg, Johannesburg, South Africa, 2022. [Google Scholar]
- Knight, F.L.M. Mindfulness: History, Technologies, Research, Applications. Techniques of Psychotherapy; Pepperdine University: Malibu, CA, USA, 2010. [Google Scholar]
- Thatcher, C. (Ed.) Insight Meditation: Practical Steps to Ultimate Truth; Vipassana Dhura Meditation Society: Aurora, CO, USA, 2011; Available online: https://www.vipassanadhura.com/PDF/practicalsteps.pdf (accessed on 10 May 2022).
- Goenka, S.N. Ten Discourses on Vipassana Meditation; Vipassana Mediation Association: India. 2013. Available online: https://www.dhamma.org/en-US/index (accessed on 18 July 2022).
- Brown, K.W.; Ryan, R.M.; Creswell, J.D. Mindfulness: Theoretical foundations and evidence for its salutary effects. Psychol. Inq. 2007, 18, 211–237. [Google Scholar] [CrossRef]
- Tang, Y.-Y.; Hölzel, B.K.; Posner, M.I. The neuroscience of mindfulness meditation. Nat. Rev. Neurosci. 2015, 16, 213–225. [Google Scholar] [CrossRef] [PubMed]
- Hölzel, B.K.; Carmody, J.; Vangel, M.; Congleton, C.; Yerramsetti, S.M.; Gard, T.; Lazar, S.W. Mindfulness practice leads to increases in regional brain gray matter density. Psychiatry Res. 2011, 191, 36–43. [Google Scholar] [CrossRef]
- Porges, S.W. The polyvagal perspective. Biol. Psychol. 2007, 74, 116–143. [Google Scholar] [CrossRef] [PubMed]
- Lazar, S.W.; Kerr, C.E.; Wasserman, R.H.; Gray, J.R.; Greve, D.N.; Treadway, M.T.; McGarvey, M.; Quinn, B.T.; Dusek, J.A.; Benson, H.; et al. Meditation experience is associated with increased cortical thickness. Neuroreport 2005, 16, 1893–1897. [Google Scholar] [CrossRef]
- Hunot, V.; Moore, T.H.M.; Caldwell, D.M.; Furukawa, T.A.; Davies, P.; Jones, H.; Honyashiki, M.; Chen, P.; Lewis, G.; Churchill, R. “Third wave” cognitive and behavioural therapies versus other psychological therapies for depression. Cochrane Database Syst. Rev. 2013. [Google Scholar] [CrossRef]
- Peteet, J.R. A fourth wave of psychotherapies: Moving beyond recovery toward well-being. Harv. Rev. Psychiatry 2018, 26, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Emamzadeh, A. The Fourth Wave of Psychotherapies: The Challenges Associated with the Latest Group of Psychotherapies. Psychology Today. [Blog Posted 18 April 2018]. Available online: https://www.psychologytoday.com/intl/blog/finding-new-home/201804/the-fourth-wave-psychotherapies (accessed on 10 June 2022).
- Cortright, B. Integral Psychology: Yoga, Growth, and Opening the Heart; State University of New York Press: Albany, NY, USA, 2007; Available online: https://www.amazon.com/Integral-Psychology-Opening-Transpersonal-Humanistic/dp/0791470725?asin=0791470725&revisionId=&format=4&depth=1 (accessed on 12 July 2022).
- Treleaven, D.A. Trauma-Sensitive Mindfulness: Practices for Safe and Transformative Healing; W.W. Norton: New York, NY, USA, 2018. [Google Scholar]
- Boyd, J.E.; Lanius, R.A.; McKinnon, M.C. Mindfulness-based treatments for posttraumatic stress disorder: A review of the treatment literature and neurobiological evidence. J. Psychiatry Neurosci. 2018, 43, 7–25. [Google Scholar] [CrossRef] [PubMed]
- Lang, A.J.; Strauss, J.L.; Bomyea, J.; Bormann, J.E.; Hickman, S.D.; Good, R.C.; Essex, M. The theoretical and empirical basis for meditation as an intervention for PTSD. Behav. Modif. 2012, 36, 759–786. [Google Scholar] [CrossRef] [PubMed]
- Wagner, D. Polyvagal Theory in Practice. 2016. Counselling Today. Available online: https://ct.counseling.org/2016/06/polyvagal-theory-practice/ (accessed on 5 July 2022).
- Levine, P.A. Waking the Tiger: Healing Trauma: The Innate Capacity to Transform Overwhelming Experiences; North Atlantic Books: London, UK, 1997. [Google Scholar]
- Porges, S.W. The Polyvagal Theory: Neurophysiological Foundations of Emotions, Attachment, Communication, and Self-Regulation; W. W. Norton: New York, NY, USA, 2011. [Google Scholar]
- Levine, P.; Porges, S.W.; Phillips, M. Healing Trauma and Pain through Polyvagal Science. 2015. Available online: https://maggiephillipsphd.com/Polyvagal/EBookHealingTraumaPainThroughPolyvagalScience.pdf (accessed on 5 June 2022).
- Grossman, P.; Niemann, L.; Schmidt, S.; Walach, H. Mindfulness-based stress reduction and health benefits: A meta-analysis. J. Psychosom. Res. 2004, 57, 35–43. [Google Scholar] [CrossRef]
- Lucas, A.R.; Klepin, H.D.; Porges, S.W.; Rejeski, J. Mindfulness-based movement: A Polyvagal perspective. Integr. Cancer Ther. 2016, 17, 5–15. [Google Scholar] [CrossRef] [PubMed]
- Siegel, D.J. The Mindful Therapist: A Clinician′s Guide to Mindsight and Neural Integration (Norton Series on Interpersonal Neurobiology); W. W. Norton: New York, NY, USA, 2010. [Google Scholar]
- Cayoun, B. Mindfulness-integrated CBT: Principles and Practice; John Wiley & Sons: London, UK, 2011. [Google Scholar] [CrossRef]
- Davidson, R.J.; Kabat-Zinn, J.; Schumacher, J.; Rosenkrantz, M.; Muller, D.; Santorelli, S.F.; Sheridan, J.F. Alterations in brain and immune function produced by mindfulness meditation. Psychosom. Med. 2003, 65, 564–570. [Google Scholar] [CrossRef]
- Sanes, J.N.; Donoghue, J.P. Plasticity and primary motor cortex. Annu. Rev. Neurosci. 2000, 23, 393–415. [Google Scholar] [CrossRef]
- Nocon, A.; Eberle-Sejari, R.; Unterhitzenberger, J.; Rosner, R. The effectiveness of psychosocial interventions in war-traumatized refugee and internally displaced minors: Systematic review and meta-analysis. Eur. J. Psychotraumatol. 2017, 8, 1388709. [Google Scholar] [CrossRef]
- Šehović, M. Evaluation of results of cognitive-behavioural therapy with traumatised children of dis-placed persons. In The Psychosocial Consequences of War: Results of Empirical Research from the Territory of Former Yugoslavia; Powell, S., Durakovic-Belko, E., Powell, S., Durakovic-Belko, E., Eds.; Otisak d.o.o.: Sarajevo, Bosnia-Herzegovina, 2002; pp. 265–266. [Google Scholar]
- Oras, R.; de Ezpeleta, S.C.; Ahmad, A. Treatment of traumatized refugee children with Eye Movement Desensitization and Reprocessing in a psychodynamic context. Nordic J. Psychiatry 2004, 58, 199–203. [Google Scholar] [CrossRef]
- Onyut, L.P.; Neuner, F.; Schauer, E.; Ertl, V.; Odenwald, M.; Schauer, M.; Elbert, T. Narrative Exposure Therapy as a treatment for child war survivors with posttraumatic stress disorder: Two case reports and a pilot study in an African refugee settlement. BMC Psychiatry 2005, 5, 7. [Google Scholar] [CrossRef]
- Ehntholt, K.A.; Smith, P.A.; Yule, W. School based cognitive-behavioural therapy group intervention for refugee children who have experienced war-related trauma. Clin. Child Psychol. Psychiatry 2005, 10, 235–250. [Google Scholar] [CrossRef]
- Möhlen, H.; Parzer, P.; Resch, F.; Brunner, R. Psychosocial support for war-traumatized child and adolescent refugees: Evaluation of a short-term treatment program. Aust. N. Z. J. Psychiatry 2005, 39, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Catani, C.; Kohiladevy, M.; Ruf, M.; Schauer, E.; Elbert, T.; Neuner, F. Treating children traumatized by war and Tsunami: A comparison between exposure therapy and meditation-relaxation in North-East Sri Lanka. BMC Psychiatry 2009, 9, 22. [Google Scholar] [CrossRef]
- Schauer, E. Trauma Treatment for Children in War: Build-up of an Evidence-Based Large-Scale Mental Health Intervention in North-Eastern Sri Lanka. Doctoral Dissertation, University of Konstanz, Konstanz, Germany, 2008. [Google Scholar]
- Schottelkorb, A.A.; Doumas, D.M.; Garcia, R. Treatment for childhood refugee trauma: A randomized, controlled trial. Int. J. Play. Ther. 2012, 21, 57–73. [Google Scholar] [CrossRef]
- Ooi, C.S. The Efficacy and Social Validity of A Group Cognitive Behavioural Therapy for Young Migrants from War-Affected Countries. Doctoral Dissertation, Curtin University, Perth, Australia, 2012. [Google Scholar]
- Tol, W.A.; Komproe, I.H.; Jordans, M.J.D.; Vallipuram, A.; Sipsma, H.; Sivayokan, S.; Macy, R.D.; de Jong, J.T. Outcomes and moderators of a preventive school-based mental health intervention for children affected by war in Sri Lanka: A cluster randomized trial. World Psychiatry Off. J. World Psychiatr. Assoc. 2012, 11, 114–122. [Google Scholar]
- Betancourt, T.S.; Newnham, E.A.; Layne, C.M.; Kim, S.; Steinberg, A.M.; Ellis, H.; Birman, D. Trauma history and psychopathology in war-affected refugee children referred for trauma-related mental health services in the USA. J. Traumatic Stress 2012, 25, 682–690. [Google Scholar] [CrossRef]
- Ooi, C.S.; Rooney, R.M.; Roberts, C.; Kane, R.T.; Wright, B.; Chatzisarantis, N. The efficacy of a group cognitive behavioral therapy for war-affected young migrants living in Australia: A cluster randomized controlled trial. Front. Psychol. 2016, 7, 1641. [Google Scholar] [CrossRef]
- Pfeiffer, E.; Goldbeck, L. Evaluation of a Trauma-Focused Group Intervention for Unaccompanied Young Refugees: A Pilot Study. J. Traumatic Stress 2017, 30, 531–536. [Google Scholar] [CrossRef]
- O’Shea, B.; Hodes, M.; Down, G.; Bramley, J. A school-based mental health service for refugee children. Clin. Child Psychol. Psychiatry 2000, 5, 189–201. [Google Scholar] [CrossRef]
- Dybdahl, R. Children and mothers in war: An outcome study of a psychosocial intervention program. Child Dev. 2001, 72, 1214–1230. [Google Scholar] [CrossRef]
- Šestan, D. Participation in a program of psychosocial support and reduction of posttraumatic symptoms in preschool children and their mothers. In The Psychosocial Consequences of War: Results of Empirical Research from the Territory of Former Yugoslavia; Powell, S., Durakovic-Belko, E., Eds.; Otisak d.o.o.: Sarajevo, Bosnia-Herzegovina, 2002; pp. 255–257. [Google Scholar]
- Thabet, A.A.; Vostanis, P.; Karim, K. Group crisis intervention for children during ongoing war conflict. Eur. Child Adolesc. Psychiatry 2005, 14, 262–269. [Google Scholar] [CrossRef]
- Fazel, M.; Doll, H.; Stein, A. A school-based mental health intervention for refugee children: An exploratory study. Clin. Child Psychol. Psychiatry 2009, 14, 297–309. [Google Scholar] [CrossRef] [PubMed]
- Betancourt, T.S.; Newnham, E.A.; Brennan, R.T.; Verdeli, H.; Borisova, I.; Neugebauer, R.; Bass, J.; Bolton, P. Moderators of treatment effectiveness for war-affected youth with depression in northern Uganda. J. Adolesc. Health Off. Publ. Soc. Adolesc. Med. 2012, 51, 544–550. [Google Scholar] [CrossRef] [PubMed]
- Kalantari, M.; Yule, W.; Dyregrov, A.; Neshatdoost, H.; Ahmadi, S.J. Efficacy of writing for recovery on traumatic grief symptoms of Afghani refugee bereaved adolescents: A randomized control trial. Omega 2012, 65, 139–150. [Google Scholar] [CrossRef]
- Lange-Nielsen, I.I.; Kolltveit, S.; Thabet, A.A.M.; Dyregrov, A.; Pallesen, S.; Johnsen, T.B.; Laberg, J.C. Short-term effects of a writing intervention among adolescents in Gaza. J. Loss Trauma 2012, 17, 403–422. [Google Scholar] [CrossRef]
- Ellis, B.H.; Miller, A.B.; Abdi, S.; Barrett, C.; Blood, E.; Betancourt, T.S. Multi-tier mental health program for refugee youth. J. Consult. Clin. Psychol. 2013, 81, 129–140. [Google Scholar] [CrossRef]
- Van der Kolk, B. The Body Keeps the Score: Brain, Mind and Body in the Healing of Trauma; Penguin Books: New York, NY, USA, 2015. [Google Scholar]


{kind=link}
| Evidence-Based Treatment | Sources | |
|---|---|---|
| Eclectic cognitive behavioural therapy (CBT) with other elements | Šehović | [40] |
| Eye movement desensitisation and reprocessing within a psychodynamic therapy | Oras, De Ezpeleta & Ahmad | [41] |
| Strict CBT | Onyut et al. | [42] |
| Eclectic CBT with other elements | Ehntholt, Smith & Yule | [43] |
| Eclectic CBT with other elements | Möhlen et al. | [44] |
| Strict CBT | Catani et al. | [45] |
| Strict CBT | Schauer | [46] |
| Strict CBT | Schottelkorb, Doumas & Garcia | [47] |
| Eclectic CBT with other elements | Ooi | [48] |
| Eclectic CBT with other elements | Tol et al. | [49] |
| Interpersonal therapy (IPT) | Betancourt et al. | [50] |
| Eclectic CBT with other elements | Ooi et al. | [51] |
| Strict CBT | Pfeiffer & Goldbeck | [52] |
| Non-Evidence-Based Treatment | Researched by | |
|---|---|---|
| Mixed interventions/eclectic therapy | O’Shea | [53] |
| Psychosocial support combined with medical care | Dybdahl | [54] |
| Psychosocial support | Šestan | [55] |
| Crisis intervention | Thabet, Vostanis & Karim | [56] |
| Psychoeducation | Thabet, Vostanis & Karim | [56] |
| Meditation and relaxation techniques | Schauer | [46] |
| Mixed interventions/eclectic therapy | Fazel, Doll & Stein | [57] |
| Creative play | Betancourt | [58] |
| Writing intervention (writing for recovery) | Kalantari et al. | [59] |
| Writing intervention (writing for recovery) | Lange-Nielsen et al. | [60] |
| A systemic approach with preventive skill-building | Ellis et al. | [61] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeebodh-Desai, L.; Dwarika, V.M. Trauma-Sensitive Mindfulness for War Refugees: Communication of Preliminary Findings. Trauma Care 2022, 2, 556-568. https://doi.org/10.3390/traumacare2040046
Jeebodh-Desai L, Dwarika VM. Trauma-Sensitive Mindfulness for War Refugees: Communication of Preliminary Findings. Trauma Care. 2022; 2(4):556-568. https://doi.org/10.3390/traumacare2040046
Chicago/Turabian StyleJeebodh-Desai, Laila, and Veronica M. Dwarika. 2022. "Trauma-Sensitive Mindfulness for War Refugees: Communication of Preliminary Findings" Trauma Care 2, no. 4: 556-568. https://doi.org/10.3390/traumacare2040046
APA StyleJeebodh-Desai, L., & Dwarika, V. M. (2022). Trauma-Sensitive Mindfulness for War Refugees: Communication of Preliminary Findings. Trauma Care, 2(4), 556-568. https://doi.org/10.3390/traumacare2040046