1. Introduction
Patients with an immunocompromised state are at risk of developing a long-term infection from the coronavirus 2 that causes severe acute respiratory syndrome (SARS-CoV-2). It has been shown that SARS-CoV-2 variants may emerge over the course of such chronic episodes of coronavirus disease 2019 (COVID-19) in multiple case reports [1,2]. Because a vast number of people across the world suffer from inherent or induced immunosuppression, the link between immunosuppression and the emergence of highly communicable or deadly SARS-CoV-2 variants has to be explored further and countermeasures developed [3].
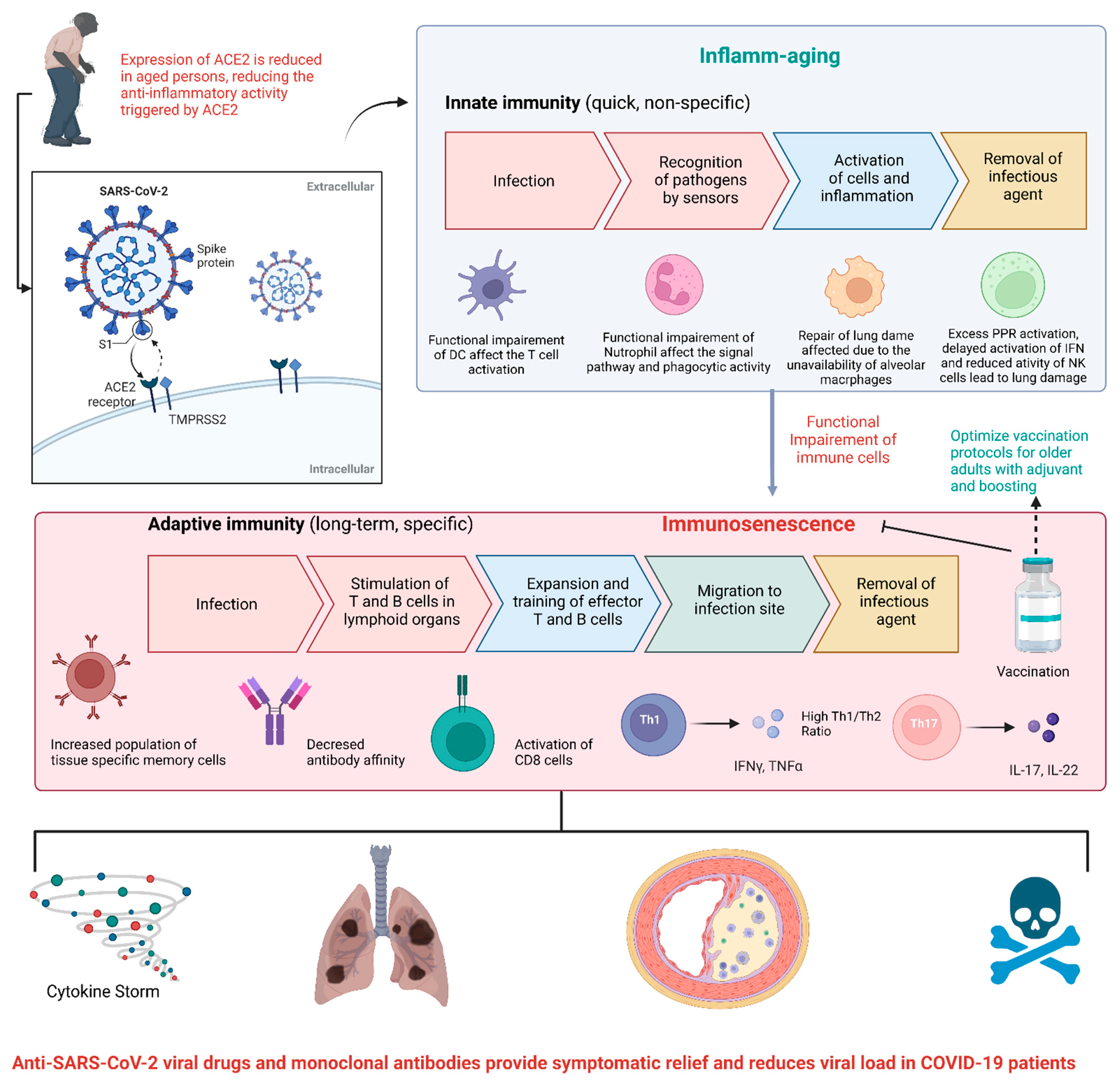
Variations in the host immune response with age affect not just the capacity to fight infections, but also the capacity to construct successful vaccination defences. “Immunosenescence and inflammaging are two essential characteristics of the ageing immune system, in which the aggregation of senescent immune cells contributes to its decrease while increasing inflammatory phenotypes promote immunological malfunction” [4,5]. Within lymphoid and nonlymphoid peripheral organs, age-related alterations in the immune system influence cells and soluble components of both innate and adaptive immune responses (Figure 1). These alterations influence not just infection vulnerability, but also illness development and clinical consequences.
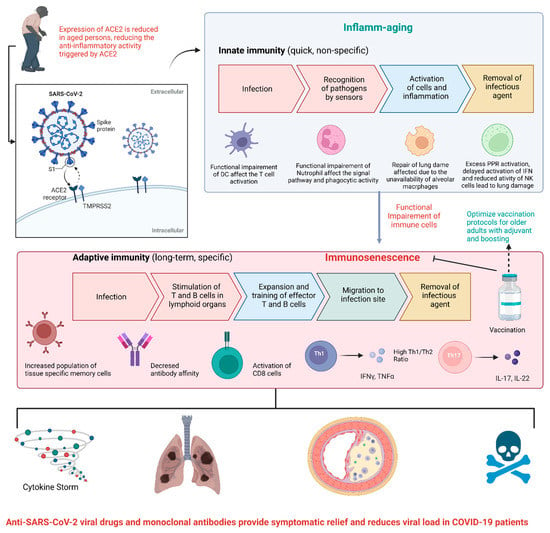
Figure 1.
Alteration of the immune system in the aged population and connection with COVID-19 management.
COVID-19 seems to show typical clinical symptoms in immunocompromised people. Cancer patients and solid-organ transplant recipients may have an increased chance of developing COVID-19 [6]. Based on present evidence, patients receiving biologics may not be at a greater risk of severe illness; nevertheless, it is unclear if they are at a reduced risk of severe COVID-19. According to Mueller AL [7], the viral replication process is favoured in aged and immunocompromised individuals due to inefficiency of the circulatory macrophages and cellular immunity. This situation allows hyperactivation of circulatory chemokines to enter systemic circulation with the activation of fibroblasts. The virus infects microvascular pericytes in other organs, and fluid fills the alveolus, limiting lung capacity. Microvasculature clotting is triggered by a cytokine storm, resulting in severe hypoxia, coagulopathy, and organ failure.
In summary, the age and immunocompromised state of the patient provides more time to SARS-CoV-2 in the host body with limited defence that ultimately leads to the viral mutations and emergence of new viral variants of SARS-CoV-2. As such, antiviral drugs and vaccinations are required to help immunocompromised patients fight against SARS-CoV-2 infection and severe COVID-19 disease.
2. Bioinformatics and Drug Repurposing
Thus far, there have been over 6.35 million deaths due to COVID-19 and almost 550 million reported cases across the globe, conceivably being the largest threat to mankind in recent years [8]. The severity and outcome of COVID-19 greatly depend on the patient’s age and immunity [9]. Immunosenescence has become the emerging challenge for the aged population. Viral evolution in immunocompromised and aged patients is considered as an important factor in the emergence of viral variants [10]. Because of the change in genetic material of the virus, different variants of concern of SARS-CoV-2 have been identified during this pandemic, such as “alpha (B.1.1.7), beta (B.1.351), gamma (P.1), delta (B.1.617.2), and omicron (B.1.1.529)” which are associated with enhanced transmissibility and increase virulence [11,12,13,14,15,16,17]. In addition, omicron has diverged into sublineages “BA.1 (B.1.1.529.1), BA.2 (B.1.1.529.2) and BA.3 (B.1.1.529.3), and more recently, BA.4 and BA.5” have emerged, each having additional mutations to the spike protein and increased growth rate [18]. The development of variants is due to mutations in the virus spike protein in order to escape from the host immune system or to increase infectivity. The primary targets for most therapeutic methods against SARS-CoV-2 are against the spike protein and the receptor-binding domain (RBD), which alter the binding to the host cell receptor angiotensin-converting enzyme 2 (ACE2) [19,20,21,22,23,24,25,26,27]. Adding to this complexity, more recently, it has been shown that SARS-CoV-2 can enter host cells via additional receptors [28]. At present, there are no efficacious antiviral drugs available for COVID-19 treatment even though a number of antivirals are being used in moderate–severe disease individuals, those at high risk and the immunocompromised, such as remdesivir [29], with a number showing promise as antivirals [30]. However, Ritonavir-Boosted Nirmatrelvir (Paxlovid) that is in current use in the US and elsewhere, and has been shown to be effective in treating disease and preventing hospitalization if administered within 5 days of the onset of symptoms [31]. In spite of the fact that coronaviruses have undergone notable genetic evolution, they still have remarkable similarities, which should be the basis for the identification of promising targets for antiviral therapies to combat the pandemic.
Since the advent of the COVID-19 pandemic, the application of bioinformatics and drug repurposing has accelerated the research efforts for COVID-19 drug discovery. Different chembioinformatic approaches (fragment-based, structure-based, and ligand-based modelling strategies), and immunobioinformatics may be useful hall markers to prioritize the drug candidate and vaccine candidate, respectively, for further experiments [32,33,34]. Computational drug repurposing (repositioning) is an effective approach to identifying novel drug-target interactions using the drugs already known to be safe, which provides the advantages of significantly reducing the time for drug development and reduced failure rate [35]. This approach typically includes a virtual screening of drug libraries to find suitable drug–target pairs using molecular-shape similarity methods and molecular docking and binding free energy calculations to predict binding affinity. Numerous monoclonal antibody (mAb)-based treatments with repurposed mAbs and novel SARS-CoV-2-specific mAbs are available for COVID-19 management [36]. In addition, nano-based drug delivery systems can be applied for efficient targeted delivery [37,38,39,40,41].
3. Impact of Vaccines
Within 6 months of the global pandemic, millions of cases surged with many hospitalizations and deaths, in particular to the elderly and those with underlying secondary disease and weak immune systems. As a consequence, this added much strain to the health care system as well as the global economic status suffering huge losses, primarily in tourism, aviation, entertainment, sports, retail and hospitality due to COVID-19 restrictions. Many suffered social and psychological issues including the aged, children, students and health workers. As quickly as the pandemic came upon us, so did world-wide efforts to develop effective vaccines against SARS-CoV-2 virus. Several vaccines were approved as emergency-use rollouts around the world and numerous are in preclinical and in human clinical trials. A number of vaccine platforms have been used with the aim to deliver viral constituents or fragments of the virus to immune cells, to stimulate antibody and/or T cell responses. As of June 2022, the WHO documented 147 vaccines in clinical development and 195 vaccines in the preclinical development stage for COVID-19. Some of the platforms used include live attenuated or whole inactivated virus as have been in traditional vaccines, viral-vectors, small virus-like particles, mRNA, DNA, proteins, peptides and DC-based vaccines [42].
Vaccination aims to prevent disease or transmission in the community. With world-wide mass vaccinations, COVID-19 disease can be controlled, by preventing hospitalizations, severe disease and death. The Pfizer-BioNTech, Moderna and Johnson & Johnson vaccines have been authorized by the Food and Drug Administration (FDA, USA) and especially the immunocompromised and elderly have been advised to receive booster injections. In fact, in a study of 780,225 veterans in the Veterans Health Administration covering 2.7% of the US population, vaccination protected against death in those infected against the delta variant. In those aged <65years, vaccination decreased death by 73% (Johnson & Johnson), 81.5% (Moderna) and 84.3% (Pfizer-BioNTech), and for those above 65 years, protection was 52.2%, 75.5% and 70.1%, respectively [43]. In the UK, the Oxford-AstraZeneca vaccine offered 91% effectiveness (in 115,000 people) in preventing death in those who were double-vaccinated and had subsequently tested positive for the delta variant [44].
Like most vaccines, there are reports that vaccination against SARS-CoV-2 can cause, in some cases, pain at the injection site, fever, fatigue, and headache. Other reported effects include decreased haemoglobin levels, increased bilirubin levels, altered serum glutamic-oxaloacetic transaminase and serum glutamic pyruvic transaminase [45,46], edema [47], erythema [48], myocarditis [49], thrombosis, and thrombocytopenia [50]. Several clinical trials are being conducted in order to assess the safety profile of different COVID-19 vaccine platforms. Overall, despite the rare adverse reactions reported, vaccination protects against hospitalizations and deaths, even in breakthrough cases.
Author Contributions
All authors contributed to the conceptualization, design, writing, and editing of the article. All authors read, reviewed, and approved the final paper. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Acknowledgments
This Special Issue recognizes the 75th year anniversary of the LM College of Pharmacy, Ahmedabad Gujarat India. V.P.C. would like to thank the Department of Pharmaceutics and Pharmaceutical Technology and M.T.C the Department of Pharmaceutical Chemistry of LM College of Pharmacy Gujarat India. V.A. would like to thank the Immunology and Translational Research Group and the Greek Orthodox Archdiocese of Australia for funding the COVID-19 research. Figure 1 was created with biorender.com.
Conflicts of Interest
The authors declare no conflict of interest with respect to the authorship and publication of this article.
References
- Avanzato, V.A.; Matson, M.J.; Seifert, S.N.; Pryce, R.; Williamson, B.N.; Anzick, S.L.; Barbian, K.; Judson, S.D.; Fischer, E.R.; Martens, C.; et al. Case Study: Prolonged Infectious SARS-CoV-2 Shedding from an Asymptomatic Immunocompromised Individual with Cancer. Cell 2020, 183, 1901–1912.e9. [Google Scholar] [CrossRef]
- Choi, B.; Choudhary, M.C.; Regan, J.; Sparks, J.A.; Padera, R.F.; Qiu, X.; Solomon, I.H.; Kuo, H.-H.; Boucau, J.; Bowman, K.; et al. Persistence and Evolution of SARS-CoV-2 in an Immunocompromised Host. N. Engl. J. Med. 2020, 383, 2291–2293. [Google Scholar] [CrossRef]
- Corey, L.; Beyrer, C.; Cohen, M.S.; Michael, N.L.; Bedford, T.; Rolland, M. SARS-CoV-2 Variants in Patients with Immunosuppression. N. Engl. J. Med. 2021, 385, 562–566. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, V.; Gadi, N.; Spihlman, A.P.; Wu, S.C.; Choi, C.H.; Moulton, V.R. Aging, Immunity, and COVID-19: How Age Influences the Host Immune Response to Coronavirus Infections? Front. Physiol. 2021, 11, 571416. [Google Scholar] [CrossRef] [PubMed]
- Feehan, J.; Tripodi, N.; Apostolopoulos, V. The twilight of the immune system: The impact of immunosenescence in aging. Maturitas 2021, 147, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Fung, M.; Babik, J.M. COVID-19 in Immunocompromised Hosts: What We Know So Far. Clin. Infect. Dis. 2020, 72, 340–350. [Google Scholar] [CrossRef]
- Mueller, A.L.; McNamara, M.S.; Sinclair, D.A. Why does COVID-19 disproportionately affect older people? Aging 2020, 12, 9959–9981. [Google Scholar] [CrossRef]
- Feehan, J.; Apostolopoulos, V. Is COVID-19 the worst pandemic? Maturitas 2021, 149, 56–58. [Google Scholar] [CrossRef]
- Schultze, J.L.; Aschenbrenner, A.C. COVID-19 and the human innate immune system. Cell 2021, 184, 1671–1692. [Google Scholar] [CrossRef]
- Bhattacharyya, R.P.; Hanage, W.P. Challenges in Inferring Intrinsic Severity of the SARS-CoV-2 Omicron Variant. N. Engl. J. Med. 2022, 386, e14. [Google Scholar] [CrossRef]
- Chavda, V.P.; Apostolopoulos, V. Omicron Variant (B.1.1.529) of SARS-CoV-2: Threat for the elderly? Maturitas 2022, 158, P78–P81. [Google Scholar] [CrossRef]
- Chavda, V.P.; Vora, L.K.; Pandya, A.K.; Patravale, V.B. Intranasal vaccines for SARS-CoV-2: From challenges to potential in COVID-19 management. Drug Discov. Today 2021, 26, 2619–2636. [Google Scholar] [CrossRef]
- Chavda, V.P.; Patel, A.B.; Vaghasiya, D.D. SARS-CoV-2 variants and vulnerability at the global level. J. Med. Virol. 2022, 94, 2986–3005. [Google Scholar] [CrossRef]
- Chavda, V.P.; Apostolopoulos, V. Global impact of delta plus variant and vaccination. Expert Rev. Vaccines 2022, 21, 597–600. [Google Scholar] [CrossRef]
- Chavda, V.P.; Ghali, E.N.H.K.; Yallapu, M.M.; Apostolopoulos, V. Therapeutics to tackle Omicron outbreak. Immunotherapy 2022, 14, 833–838. [Google Scholar] [CrossRef]
- Huang, Z.; Chavda, V.P.; Vora, L.K.; Gajjar, N.; Apostolopoulos, V.; Shah, N.; Chen, Z.-S. 2-Deoxy-D-Glucose and its Derivatives for the COVID-19 Treatment: An Update. Front. Pharmacol. 2022, 13, 899633. [Google Scholar] [CrossRef]
- Chavda, V.P.; Apostolopoulos, V. Is Booster Dose Strategy Sufficient for Omicron Variant of SARS-CoV-2? Vaccines 2022, 10, 367. [Google Scholar] [CrossRef]
- Mahase, E. COVID-19: What do we know about omicron sublineages? BMJ 2022, 376, o358. [Google Scholar] [CrossRef]
- Chavda, V.P.; Gajjar, N.; Shah, N.; Dave, D.J. Darunavir ethanolate: Repurposing an anti-HIV drug in COVID-19 treatment. Eur. J. Med. Chem. Rep. 2021, 3, 100013. [Google Scholar] [CrossRef]
- Chavda, V.P.; Kapadia, C.; Soni, S.; Prajapati, R.; Chauhan, S.C.; Yallapu, M.M.; Apostolopoulos, V. A global picture: Therapeutic perspectives for COVID-19. Immunotherapy 2022, 14, 351–371. [Google Scholar] [CrossRef]
- Chavda, V.P.; Hossain, K.; Beladiya, J.; Apostolopoulos, V. Nucleic Acid Vaccines for COVID-19: A Paradigm Shift in the Vaccine Development Arena. Biologics 2021, 1, 337–356. [Google Scholar] [CrossRef]
- Chavda, V.P.; Patel, A.B.; Vihol, D.; Vaghasiya, D.D.; Ahmed, K.M.S.B.; Trivedi, K.U.; Dave, D.J. Herbal Remedies, Nutraceuticals, and Dietary Supplements for COVID-19 Management: An Update. Clin. Complement. Med. Pharmacol. 2022, 2, 100021. [Google Scholar] [CrossRef]
- Chavda, V.P.; Bezbaruah, R.; Athalye, M.; Parikh, P.K.; Chhipa, A.S.; Patel, S.; Apostolopoulos, V. Replicating Viral Vector-Based Vaccines for COVID-19: Potential Avenue in Vaccination Arena. Viruses 2022, 14, 759. [Google Scholar] [CrossRef]
- Krishnan, A.; Gangadaran, P.; Chavda, V.P.; Jogalekar, M.P.; Muthusamy, R.; Valu, D.; Vadivalagan, C.; Ramani, P.; Laishevtcev, A.; Katari, N.K.; et al. Convalescent serum-derived exosomes: Attractive niche as COVID-19 diagnostic tool and vehicle for mRNA delivery. Exp. Biol. Med. 2022, 13, 15353702221092984. [Google Scholar] [CrossRef]
- Chavda, V.P.; Vora, L.K.; Vihol, D.R. COVAX-19Ⓡ Vaccine: Completely blocks virus transmission to non-immune individuals. Clin. Complement. Med. Pharmacol. 2021, 1, 100004. [Google Scholar] [CrossRef]
- Basu, D.; Chavda, V.P.; Mehta, A.A. Therapeutics for COVID-19 and post COVID-19 complications: An update. Curr. Res. Pharmacol. Drug Discov. 2022, 3, 100086. [Google Scholar] [CrossRef]
- Chavda, V.; Feehan, J.; Apostolopoulos, V. A Veterinary Vaccine for SARS-CoV-2: The First COVID-19 Vaccine for Animals. Vaccines 2021, 9, 631. [Google Scholar] [CrossRef]
- Gadanec, L.; McSweeney, K.; Qaradakhi, T.; Ali, B.; Zulli, A.; Apostolopoulos, V. Can SARS-CoV-2 Virus Use Multiple Receptors to Enter Host Cells? Int. J. Mol. Sci. 2021, 22, 992. [Google Scholar] [CrossRef]
- Russo, P.; Tacconelli, E.; Olimpieri, P.P.; Celant, S.; Colatrella, A.; Tomassini, L.; Palù, G. Mortality in SARS-CoV-2 Hospitalized Patients Treated with Remdesivir: A Nationwide, Registry-Based Study in Italy. Viruses 2022, 14, 1197. [Google Scholar] [CrossRef]
- Ridgway, H.; Chasapis, C.T.; Kelaidonis, K.; Ligielli, I.; Moore, G.J.; Gadanec, L.K.; Zulli, A.; Apostolopoulos, V.; Mavromoustakos, T.; Matsoukas, J.M. Understanding the Driving Forces That Trigger Mutations in SARS-CoV-2: Mutational Energetics and the Role of Arginine Blockers in COVID-19 Therapy. Viruses 2022, 14, 1029. [Google Scholar] [CrossRef]
- Burki, T. The future of Paxlovid for COVID-19. Lancet Respir. Med. 2022, 10, e68. [Google Scholar] [CrossRef]
- Hassanzadeganroudsari, M.; Ahmadi, A.; Rashidi, N.; Hossain, K.; Habib, A.; Apostolopoulos, V. Computational Chemistry to Repurposing Drugs for the Control of COVID-19. Biologics 2021, 1, 111–128. [Google Scholar] [CrossRef]
- Chavda, V.P.; Ertas, Y.N.; Walhekar, V.; Modh, D.; Doshi, A.; Shah, N.; Anand, K.; Chhabria, M. Advanced Computational Methodologies Used in the Discovery of New Natural Anticancer Compounds. Front. Pharmacol. 2021, 12, 702611. [Google Scholar] [CrossRef] [PubMed]
- Chavda, V.; Sheta, S.; Changani, D.; Chavda, D. New Bioinformatics Platform-Based Approach for Drug Design. In Computation in Bioinformatics: Multidisciplinary Applications; Scrivener Publishing LLC: Beverly, MA, USA, 2021; pp. 101–120. [Google Scholar] [CrossRef]
- Sahoo, B.M.; Ravi Kumar, B.V.V.; Sruti, J.; Mahapatra, M.K.; Banik, B.K.; Borah, P. Drug Repurposing Strategy (DRS): Emerging Approach to Identify Potential Therapeutics for Treatment of Novel Coronavirus Infection. Front. Mol. Biosci. 2021, 8, 628144. [Google Scholar] [CrossRef]
- Chavda, V.P.; Prajapati, R.; Lathigara, D.; Nagar, B.; Kukadiya, J.; Redwan, E.M.; Uversky, V.N.; Kher, M.N.; Patel, R. Therapeutic monoclonal antibodies for COVID-19 management: An update. Expert Opin. Biol. Ther. 2022, 22, 763–780. [Google Scholar] [CrossRef]
- Chavda, V.P. Nanobased Nano Drug Delivery: A Comprehensive Review. In Applications of Targeted Nano Drugs and Delivery Systems; Mohapatra, S.S., Ranjan, S., Dasgupta, N., Mishra, R.K., Eds.; Elsevier: Amsterdam, The Netherlands, 2019; Chapter 4; pp. 69–92. [Google Scholar] [CrossRef]
- Chavda, V.P. Nanotherapeutics and Nanobiotechnology. In Applications of Targeted Nano Drugs and Delivery Systems; Elsevier: Amsterdam, The Netherlands, 2019; pp. 1–13. [Google Scholar]
- Chen, R.-P.; Chavda, V.P.; Patel, A.B.; Chen, Z.-S. Phytochemical Delivery Through Transferosome (Phytosome): An Advanced Transdermal Drug Delivery for Complementary Medicines. Front. Pharmacol. 2022, 13, 850862. [Google Scholar] [CrossRef]
- Chavda, V.P.; Patel, A.B.; Mistry, K.J.; Suthar, S.F.; Wu, Z.-X.; Chen, Z.-S.; Hou, K. Nano-Drug Delivery Systems Entrapping Natural Bioactive Compounds for Cancer: Recent Progress and Future Challenges. Front. Oncol. 2022, 12, 867655. [Google Scholar] [CrossRef]
- Chavda, V.P.; Vihol, D.; Mehta, B.; Shah, D.; Patel, M.; Vora, L.K.; Pereira-Silva, M.; Paiva-Santos, A.C. Phytochemical-loaded liposomes for anticancer therapy: An updated review. Nanomedicine 2022, 17, 547–568. [Google Scholar] [CrossRef]
- Hossain, K.; Hassanzadeganroudsari, M.; Feehan, J.; Apostolopoulos, V. The race for a COVID-19 vaccine: Where are we up to? Expert Rev. Vaccines 2021, 21, 355–376. [Google Scholar] [CrossRef]
- Cohn, B.A.; Cirillo, P.M.; Murphy, C.C.; Krigbaum, N.Y.; Wallace, A.W. SARS-CoV-2 vaccine protection and deaths among US veterans during 2021. Science 2022, 375, 331–336. [Google Scholar] [CrossRef]
- Sheikh, A.; Robertson, C.; Taylor, B. BNT162b2 and ChAdOx1 nCoV-19 Vaccine Effectiveness against Death from the Delta Variant. N. Engl. J. Med. 2021, 385, 2195–2197. [Google Scholar] [CrossRef]
- Kaur, R.J.; Dutta, S.; Bhardwaj, P.; Charan, J.; Dhingra, S.; Mitra, P.; Singh, K.; Yadav, D.; Sharma, P.; Misra, S. Adverse Events Reported From COVID-19 Vaccine Trials: A Systematic Review. Indian J. Clin. Biochem. 2021, 36, 427–439. [Google Scholar] [CrossRef]
- Ali, N. Relationship Between COVID-19 Infection and Liver Injury: A Review of Recent Data. Front. Med. 2020, 7, 458. [Google Scholar] [CrossRef]
- Fasano, G.; Bennardo, L.; Ruffolo, S.; Passante, M.; Ambrosio, A.G.; Napolitano, M.; Provenzano, E.; Nisticò, S.P.; Patruno, C. Erythema Migrans-like COVID Vaccine Arm: A Literature Review. J. Clin. Med. 2022, 11, 797. [Google Scholar] [CrossRef]
- Petruzzi, M.; Galleggiante, S.; Messina, S.; della Vella, F. Oral erythema multiforme after Pfizer-BioNTech COVID-19 vaccination: A report of four cases. BMC Oral Health 2022, 22, 90. [Google Scholar] [CrossRef]
- Gargano, J.W.; Wallace, M.; Hadler, S.C.; Langley, G.; Su, J.R.; Oster, M.E.; Broder, K.R.; Gee, J.; Weintraub, E.; Shimabukuro, T.; et al. Use of mRNA COVID-19 Vaccine After Reports of Myocarditis Among Vaccine Recipients: Update from the Advisory Committee on Immunization Practices—United States, June 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 977–982. [Google Scholar] [CrossRef]
- Bhuyan, P.; Medin, J.; da Silva, H.G.; Yadavalli, M.; Shankar, N.K.; Mullerova, H.; Arnold, M.; Nord, M. Very rare thrombosis with thrombocytopenia after second AZD1222 dose: A global safety database analysis. Lancet 2021, 398, 577–578. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).