

Carfilzomib-Induced Thrombotic Microangiopathy Treated with Eculizumab: A Case Report and Rapid Literature Review

 , and
, and
Abstract
1. Introduction
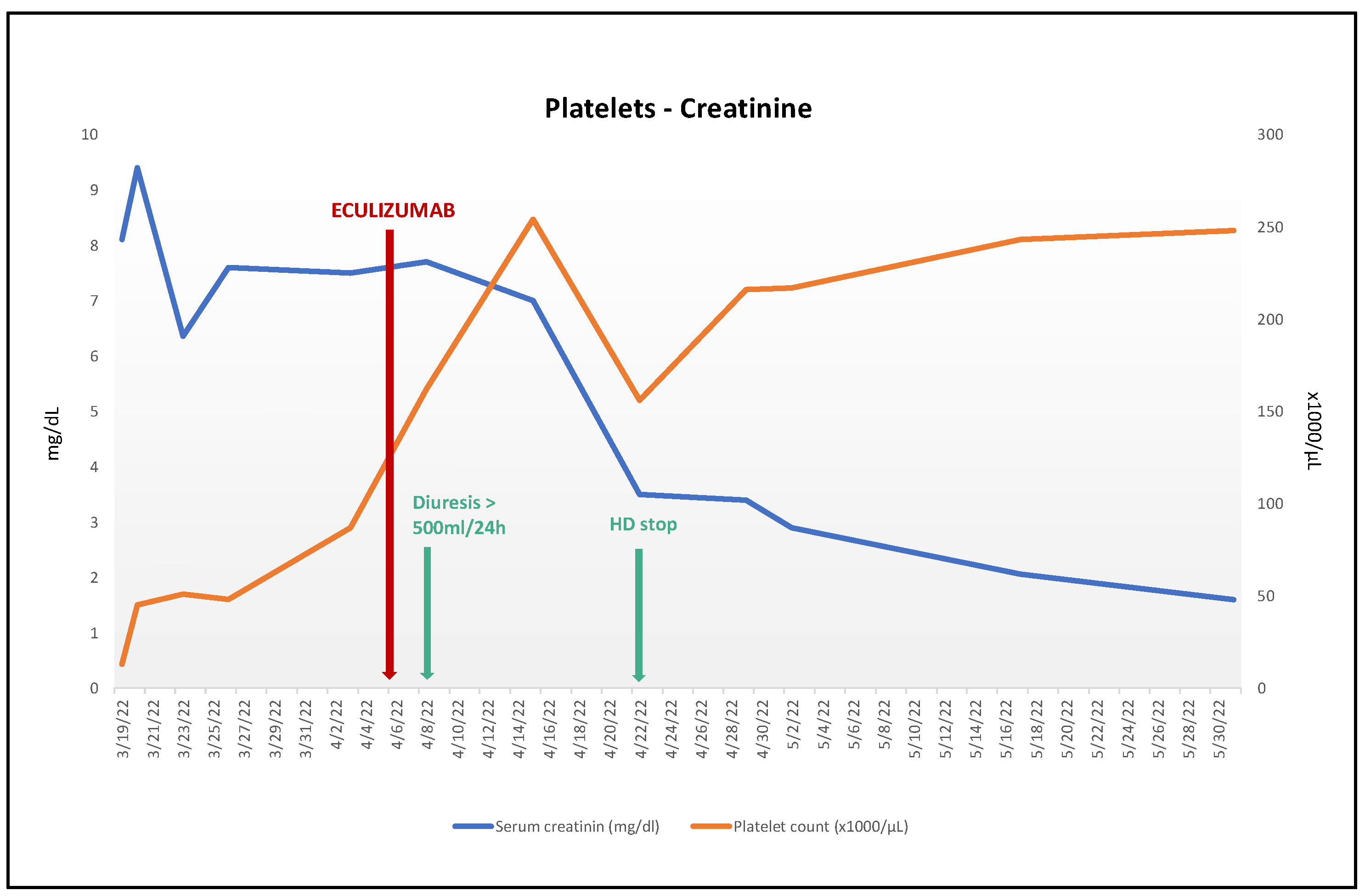
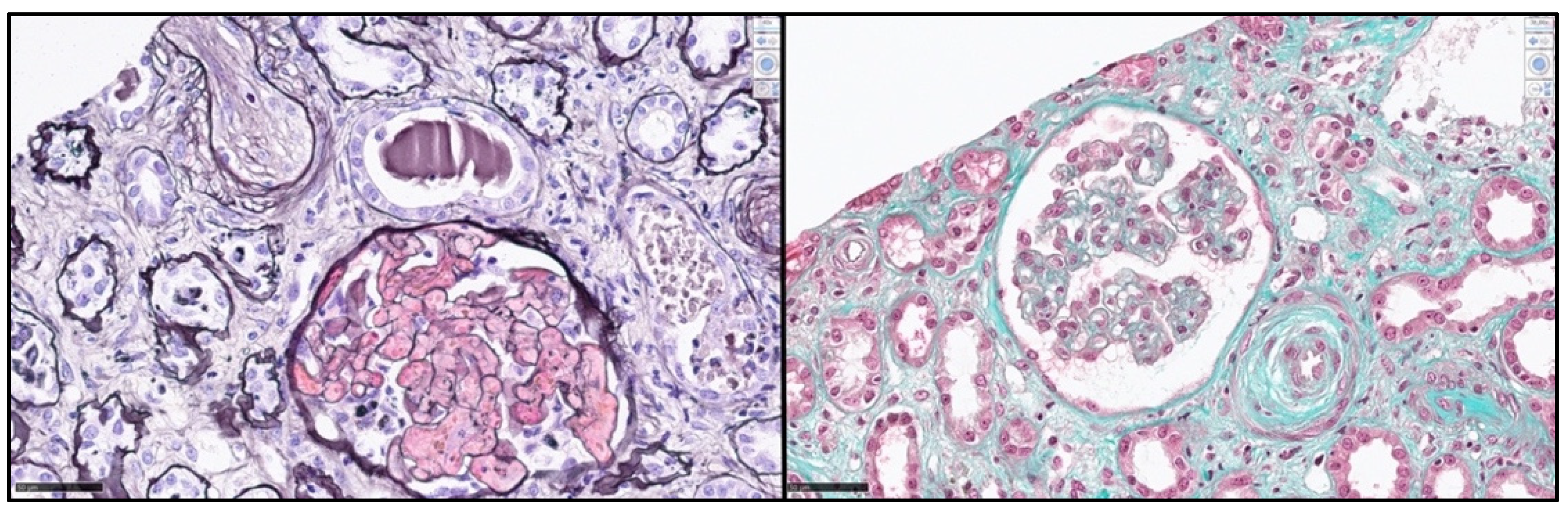
2. Case Report
3. Systematic Review
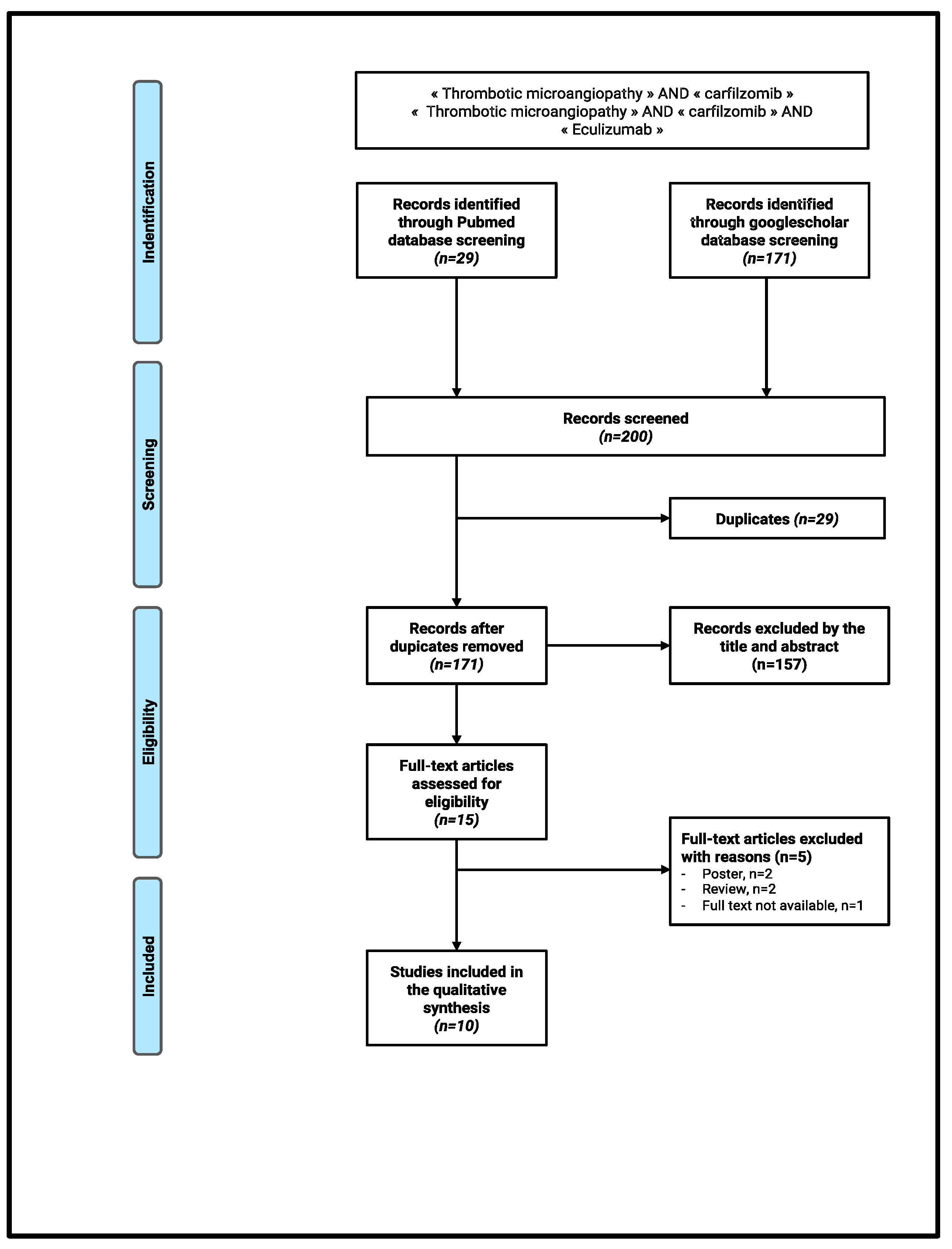
3.1. Materials and Methods
3.2. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
List of Abbreviations
| ADAMTS13 | a disintegrin and metalloproteinase with thrombospondin type 1 motif, member 13 |
| ANCA | anti-neutrophilic cytoplasmatic antibody |
| AKI | acute kidney injury |
| ASCT | autologous stem cell transplantation |
| CFZ | carfilzomib |
| D | dexamethasone |
| GFR | glomerular filtration rate |
| GVHD | graft-versus-host disease |
| HD | hemodialysis |
| Hg | hemoglobin |
| IQR | interquartile |
| KDIGO | kidney disease improving global outcomes |
| LDH | lactate dehydrogenase |
| PIs | proteasome inhibitors |
| PLT | platelet |
| SCr | serum creatinine |
| TMA | thrombotic microangiopathy |
| T | thalidomide |
| TTP | thrombotic thrombocytopenic purpura |
| VEGF | vascular epithelial growth factor |
| V | Velcade®, bortezomib |
References
- Coppo, P. Microangiopathies thrombotiques secondaires. Rev. Méd. Intern. 2017, 38, 731–736. [Google Scholar] [CrossRef] [PubMed]
- Masias, C.; Vasu, S.; Cataland, S.R. None of the above: Thrombotic microangiopathy beyond TTP and HUS. Blood 2017, 129, 2857–2863. [Google Scholar] [CrossRef] [PubMed]
- George, J.N.; Nester, C.M. Syndromes of thrombotic microangiopathy. N. Engl. J. Med. 2014, 371, 1847–1848. [Google Scholar] [CrossRef] [PubMed]
- Palma, L.M.P.; Sridharan, M.; Sethi, S. Complement in Secondary Thrombotic Microangiopathy. Kidney Int. Rep. 2021, 6, 11–23. [Google Scholar] [CrossRef] [PubMed]
- Al-Nouri, Z.L.; Reese, J.A.; Terrell, D.R.; Vesely, S.K.; George, J.N. Drug-induced thrombotic microangiopathy: A systematic review of published reports. Blood 2015, 125, 616–618. [Google Scholar] [CrossRef] [PubMed]
- Medina, P.J.; Sipols, J.M.; George, J.N. Drug-associated thrombotic thrombocytopenic purpura-hemolytic uremic syndrome. Curr. Opin. Hematol. 2001, 8, 286–293. [Google Scholar] [CrossRef]
- Monteith, B.E.; Venner, C.P.; Reece, D.E.; Kew, A.K.; Lalancette, M.; Garland, J.S.; Shepherd, L.E.; Pater, J.L.; Hay, A.E. Drug-induced Thrombotic Microangiopathy with Concurrent Proteasome Inhibitor Use in the Treatment of Multiple Myeloma: A Case Series and Review of the Literature. Clin. Lymphoma Myeloma Leuk. 2020, 20, e791–e800. [Google Scholar] [CrossRef]
- Lodhi, A.; Kumar, A.; Saqlain, M.U.; Suneja, M. Thrombotic microangiopathy associated with proteasome inhibitors. Clin. Kidney J. 2015, 8, 632–636. [Google Scholar] [CrossRef]
- Yui, J.C.; Van Keer, J.; Weiss, B.N.; Waxman, A.J.; Palmer, M.B.; D’Agati, V.D.; Kastritis, E.; Dimopoulos, M.A.; Vij, R.; Bansal, D.; et al. Proteasome inhibitor associated thrombotic microangiopathy. Am. J. Hematol. 2016, 91, E348–E352. [Google Scholar] [CrossRef]
- Terao, T.; Tsushima, T.; Miura, D.; Ikeda, D.; Fukumoto, A.; Kuzume, A.; Tabata, R.; Narita, K.; Takeuchi, M.; Matsue, K. Carfilzomib-induced thrombotic microangiopathy is underestimated in clinical practice: A report of five patients and literature review. Leuk Lymphoma 2022, 63, 1102–1110. [Google Scholar] [CrossRef]
- Moliz, C.; Gutiérrez, E.; Cavero, T.; Redondo, B.; Praga, M. Eculizumab as a treatment for atypical hemolytic uremic syndrome secondary to carfilzomib. Nefrología (Engl. Ed.) 2019, 39, 86–88. [Google Scholar] [CrossRef] [PubMed]
- Darwin, A.; Malpica, L.; Dhanoa, J.; Hashmi, H. Carfilzomib-induced atypical haemolytic uraemic syndrome: A diagnostic challenge and therapeutic success. BMJ Case Rep. 2021, 14, e239091. [Google Scholar] [CrossRef]
- Gosain, R.; Gill, A.; Fuqua, J.; Volz, L.H.; Kessans Knable, M.R.; Bycroft, R.; Seger, S.; Gosain, R.; Rios, J.A.; Chao, J.-H. Gemcitabine and carfilzomib induced thrombotic microangiopathy: Eculizumab as a life-saving treatment. Clin. Case Rep. 2017, 5, 1926–1930. [Google Scholar] [CrossRef] [PubMed]
- Portuguese, A.J.; Lipe, B. Carfilzomib-induced aHUS responds to early eculizumab and may be associated with heterozygous CFHR3-CFHR1 deletion. Blood Adv. 2018, 2, 3443–3446. [Google Scholar] [CrossRef] [PubMed]
- Blasco, M.; Martínez-Roca, A.; Rodríguez-Lobato, L.G.; Garcia-Herrera, A.; Rosiñol, L.; Castro, P.; Fernández, S.; Quintana, L.F.; Cibeira, M.T.; Bladé, J.; et al. Complement as the enabler of carfilzomib-induced thrombotic microangiopathy. Br. J. Haematol. 2021, 193, 181–187. [Google Scholar] [CrossRef]
- Bhutani, D.; Assal, A.; Mapara, M.Y.; Prinzing, S.; Lentzsch, S. Case Report: Carfilzomib-induced Thrombotic Microangiopathy With Complement Activation Treated Successfully with Eculizumab. Clin. Lymphoma Myeloma Leuk. 2020, 20, e155–e157. [Google Scholar] [CrossRef]
- Casiez, C.; Pica, G.M.; Bally, S. Syndrome hémolytique et urémique lié au carfilzomib: Évolution favorable sous éculizumab. Néphrol. Thér. 2020, 16, 221–224. [Google Scholar] [CrossRef]
- Freyer, C.W.; Bange, E.M.; Skuli, S.; Hsu, M.; Lin, J.; Cuker, A.; Cohen, A.D.; Garfall, A. Carfilzomib-Induced Atypical Hemolytic Uremic Syndrome in a Patient With Heterozygous CFHR3/CFHR1 Deletion Treated with Eculizumab. Clin. Lymphoma Myeloma Leuk. 2021, 21, e845–e849. [Google Scholar] [CrossRef]
- Rassner, M.; Baur, R.; Wäsch, R.; Schiffer, M.; Schneider, J.; Mackensen, A.; Engelhardt, M. Two cases of carfilzomib-induced thrombotic microangiopathy successfully treated with Eculizumab in multiple myeloma. BMC Nephrol. 2021, 22, 32. [Google Scholar] [CrossRef]
- Scheggi, V.; Merilli, I.; Cesaroni, E.; Alterini, B. Carfilzomib-induced thrombotic microangiopathy: A case report. J. Oncol. Pharm. Pract. 2022, 28, 754–758. [Google Scholar] [CrossRef]
- Chen, Y.; Ooi, M.; Lim, S.F.; Lin, A.; Lee, J.; Nagarajan, C.; Phipps, C.; Lee, Y.S.; Grigoropoulos, N.F.; Lao, Z.; et al. Thrombotic microangiopathy during carfilzomib use: Case series in Singapore. Blood Cancer J. 2016, 6, e450. [Google Scholar] [CrossRef] [PubMed]
- Hamad, C.D.; Hoelscher, Z.C.; Tchakarov, A.; Kala, J. Influenza-induced thrombotic microangiopathy in a patient with cancer on proteasome inhibitor: A diagnostic dilemma. CEN Case Rep. 2022, 11, 321–327. [Google Scholar] [CrossRef]
- Miyata, T.; Fan, X. A second hit for TMA. Blood. 2012, 120, 1152–1154. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, T.A.; Kremer Hovinga, J.A.; Schatzberg, D.; Wagner, D.D.; Lämmle, B. Circulating DNA and myeloperoxidase indicate disease activity in patients with thrombotic microangiopathies. Blood 2012, 120, 1157–1164. [Google Scholar] [CrossRef] [PubMed]
- Lopes da Silva, R. Viral-associated thrombotic microangiopathies. Hematol./Oncol. Stem Cell Ther. 2011, 4, 51–59. [Google Scholar] [CrossRef]
- Douglas, K.W.; Pollock, K.G.J.; Young, D.; Catlow, J.; Green, R. Infection Frequently Triggers Thrombotic Microangiopathy in Patients with Preexisting Risk Factors: A Single-Institution Experience. J. Clin. Apher. 2010, 25, 47–53. [Google Scholar] [CrossRef]
- Thoreau, B.; von Tokarski, F.; Bauvois, A.; Bayer, G.; Barbet, C.; Cloarec, S.; Mérieau, E.; Lachot, S.; Garot, D.; Bernard, L.; et al. Infection in Patients with Suspected Thrombotic Microangiopathy Based on Clinical Presentation. Clin. J. Am. Soc. Nephrol. 2021, 16, 1355–1364. [Google Scholar] [CrossRef] [PubMed]
- Tsujii, N.; Nogami, K.; Yoshizawa, H.; Hayakawa, M.; Isonishi, A.; Matsumoto, M.; Shima, M. Influenza-associated thrombotic microangiopathy with unbalanced von Willebrand factor and a disintegrin and metalloproteinase with a thrombospondin type 1 motif, member 13 levels in a heterozygous protein S-deficient boy. Pediatr. Int. 2016, 58, 926–929. [Google Scholar] [CrossRef]
- Bitzan, M.; Zieg, J. Influenza-associated thrombotic microangiopathies. Pediatr Nephrol. 2018, 33, 2009–2025. [Google Scholar] [CrossRef] [PubMed]
- Fink, E.E.; Mannava, S.; Bagati, A.; Bianchi-Smiraglia, A.; Nair, J.R.; Moparthy, K.; Lipchick, B.C.; Drokov, M.; Utley, A.; Ross, J.; et al. Mitochondrial thioredoxin reductase regulates major cytotoxicity pathways of proteasome inhibitors in multiple myeloma cells. Leukemia 2016, 30, 104–111. [Google Scholar] [CrossRef]
- Golubovic, E.; Miljkovic, P.; Zivic, S.; Jovancic, D.; Kostic, G. Hemolytic uremic syndrome associated with novel influenza A H1N1 infection. Pediatr. Nephrol. 2011, 26, 149–150. [Google Scholar] [CrossRef] [PubMed]
- Fribley, A.; Zeng, Q.; Wang, C.Y. Proteasome Inhibitor PS-341 Induces Apoptosis through Induction of Endoplasmic Reticulum Stress-Reactive Oxygen Species in Head and Neck Squamous Cell Carcinoma Cells. Mol. Cell. Biol. 2004, 24, 9695–9704. [Google Scholar] [CrossRef] [PubMed]
- Rajagopal, R.; Bennett, R.; Liang, J.; Royle, G. High dose carfilzomib proteasome inhibition induces anemia by oxidative hemolysis: A case series of 8 patients from a single centre. Am. J. Hematol. 2019, 94, E215–E216. [Google Scholar] [CrossRef] [PubMed]
- Frimat, M.; Tabarin, F.; Dimitrov, J.D.; Poitou, C.; Halbwachs-Mecarelli, L.; Fremeaux-Bacchi, V.; Roumenina, L.T. Complement activation by heme as a secondary hit for atypical hemolytic uremic syndrome. Blood 2013, 122, 282–292. [Google Scholar] [CrossRef]
- Roumenina, L.T.; Rayes, J.; Lacroix-Desmazes, S.; Dimitrov, J.D. Heme: Modulator of Plasma Systems in Hemolytic Diseases. Trends Mol. Med. 2016, 22, 200–213. [Google Scholar] [CrossRef]
- Jindal, N.; Jandial, A.; Jain, A.; Lad, D.; Prakash, G.; Khadwal, A.; Nada, R.; Sethi, J.; Ahluwalia, J.; Malhotra, P. Carfilzomib-induced thrombotic microangiopathy: A case based review. Hematol. Oncol. Stem Cell Ther. 2020; ahead of print. [Google Scholar]
- El-Bietar, J.; Warren, M.; Dandoy, C.; Myers, K.C.; Lane, A.; Wallace, G.; Davies, S.M.; Jodele, S. Histologic Features of Intestinal Thrombotic Microangiopathy in Pediatric and Young Adult Patients after Hematopoietic Stem Cell Transplantation. Biol. Blood Marrow Transplant. 2015, 21, 1994–2001. [Google Scholar] [CrossRef]
- Narimatsu, H.; Kami, M.; Hara, S.; Matsumura, T.; Miyakoshi, S.; Kusumi, E.; Kakugawa, Y.; Kishi, Y.; Murashige, N.; Yuji, K.; et al. Intestinal thrombotic microangiopathy following reduced-intensity umbilical cord blood transplantation. Bone Marrow Transpl. 2005, 36, 517–523. [Google Scholar] [CrossRef][Green Version]
- Komeno, Y.; Ogawa, S.; Ishida, T.; Takeuchi, K.; Tsujino, S.; Kurokawa, M.; Aoki, K.; Kanda, Y.; Chiba, S.; Motokura, T.; et al. Ischemic colitis as a manifestation of thrombotic microangiopathy following bone marrow transplantation. Intern Med. 2003, 42, 1228–1232. [Google Scholar] [CrossRef][Green Version]
- Nishio, M. Small intestinal thrombotic microangiopathy following kidney transplantation diagnosed by balloon-assisted enteroscopy. Ann. Gastroenterol. 2021, 34, 119–121. [Google Scholar] [CrossRef]
- Nunius, C.; Büttner-Herold, M.; Bertz, S.; Schiffer, M.; Buchholz, B. Isolated thrombotic microangiopathy of the small intestine in a patient with atypical hemolytic uremic syndrome—A case report. BMC Nephrol. 2020, 21, 104. [Google Scholar] [CrossRef]
- Stansborough, R.L.; Gibson, R.J. Proteasome inhibitor-induced gastrointestinal toxicity. Curr. Opin. Support. Palliat. Care 2017, 11, 133–137. [Google Scholar] [CrossRef] [PubMed]
- Nogales Rincón, O.; Huerta Madrigal, A.; Merino Rodriguez, B.; González Asanza, C.; Cos Arregui, E.; Menchén Fernández-Pacheco, P. Rectal bleeding and diarrhea caused by bortezomib-induced colitis. Gastroenterol. Hepatol. 2010, 33, 753–754. [Google Scholar] [CrossRef] [PubMed]
- Siniscalchi, A.; Tendas, A.; Ales, M.; Fratoni, S.; Cupelli, L.; Dentamaro, T.; Scaramucci, L.; Giovannini, M.; Caravita, T.; Santeusanio, G.; et al. Bortezomib-related colon mucositis in a multiple myeloma patient. Support Care Cancer 2009, 17, 325–327. [Google Scholar] [CrossRef] [PubMed]
- Moon, S.J.; Min, C.K.; Lee, D.G.; Lee, S.; Lee, J.W.; Min, W.S.; Kim, C.-C.; Kim, M.; Park, G.; Kim, Y. Pseudomembranous Colitis following Bortezomib Therapy in a Myeloma Patient. Acta Haematol. 2007, 117, 211–214. [Google Scholar] [CrossRef] [PubMed]
- Sun, K.; Wilkins, D.E.C.; Anver, M.R.; Sayers, T.J.; Panoskaltsis-Mortari, A.; Blazar, B.R.; Welniak, L.A.; Murphy, W.J. Differential effects of proteasome inhibition by bortezomib on murine acute graft-versus-host disease (GVHD): Delayed administration of bortezomib results in increased GVHD-dependent gastrointestinal toxicity. Blood 2005, 106, 3293–3299. [Google Scholar] [CrossRef] [PubMed]
- Pritts, T.A.; Hungness, E.S.; Hershko, D.D.; Robb, B.W.; Sun, X.; Luo, G.J.; Fischer, J.E.; Wong, H.R.; Hasselgren, P.-O. Proteasome inhibitors induce heat shock response and increase IL-6 expression in human intestinal epithelial cells. Am. J. Physiol.-Regul. Integr. Comp. Physiol. 2002, 282, R1016–R1026. [Google Scholar] [CrossRef]
- Ghouzali, I.; Azhar, S.; Bôle-Feysot, C.; Ducrotté, P.; Déchelotte, P.; Coëffier, M. Proteasome inhibitors exacerbate interleukin-8 production induced by protease-activated receptor 2 in intestinal epithelial cells. Cytokine 2016, 86, 41–46. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Reference | N° of Case | Age Sex | Hemopathy | N° Line | Treatment | CFZ Total Dose | Time from CFZ Start to TMA | Hemopathy Status | SCr Peak (mg/dL) | HD | PE | Time from TMA to Eculizumab | Complement Pathway Testing | Eculizumab Protocol | HD Evolution after Eculizumab | CFZ Stop | Latest SCr (mg/dL) | Follow-Up |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Reported case | 1 | 48 F | MM | 6 | 1. VTD 2. VRD 3. ASCT + RD 4. Allogenic SCT + RD 5. PD 6. KD | 7721 mg | Cycle 20, day 5 | CR | 9.4 | Yes | No | 19 days | Normal CH50, C3, C4 | 900 mg/w for 4 weeks +1200 mg/2 weeks (>4800 mg) | Weaning off within 15 days | Yes | 1.5 | CR |
| Gosain et al., 2017, USA [13] | 1 | 61 M | MM | 5 | 1. VRD 2. CyVD 3. M-ASCT 4. VD 5. KD | NA | Cycle 9, day 5 | PR | 5.54 | Yes | Yes | 2 days | NA | 900 mg/w for 4 weeks +1200 mg/2w (>4800 mg) | Weaning off within 6 weeks | NA | <1 | NA |
| Portuguese et al., 2018, USA [14] | 2 | 59 M 66 M | MM Plasma cell leukemia | 3 1 | 1. KRD 2. M-ASCT 3. KR 1. CyK | 1826 mg TCD 329 mg TCD | Cycle 4, day 17 Cycle 2, day 2 | NA NA | 3.46 3.2 | Yes Yes | Yes Yes | 2 days 6 days | Negative functional activity No antibody heterozygous CFH3–CFH1 deletion Negative functional activity No anti-FH antibodies heterozygous CFH3–CFH1 deletion | 900 mg/w for 3 weeks (=2700 mg) 600 mg/d for 11 days (=6600 mg) | Weaning off within 1 month HD pursuit | NA NA | 0.8 From anuria to oliguria | NA Month 5: HD pursuit |
| Bhutani al., 2020, USA [16] | 1 | 44 F | Plasmacytoma | 6 | 1. VRD 2. RD 3. DaraPD 4. VD/ CAVE 5. M-ASCT 6. KP | 20 mg/m2 + 56 mg/m2 | Cycle 1, day 10 | NA | 6.3 | Yes | No | 13 days | Normal C3–C4 Elevated Bb fragment | 900 mg/w for 4 weeks +1200 mg/15 days for 3 months (=10,800 mg) | Weaning off within 16 days | NA | <1 | CR |
| Blasco et al., 2020, Spain [15] | 1 | 41 M | Plasmacytoma | 3 | N°. NA N° + 1. M-ASCT N° + 2. KRD | 27 mg/m2 | Cycle 6, day 2 | NA | 13.7 | No | No | 3 days | Elevated C5b9s endothelial cells deposition | NA | No HD | NA | <2 | NA |
| Casiez et al., 2020, France [17] | 1 | 66 M | MM | 3 | 1. VRD 2. M-ASCT 3. KRD | 6228 mg TCD | Cycle 22, day 8 | CR | 14,4 | Yes | Yes | 17 days | Normal CH50, C3–C4 Normal Factor H and I Normal MCP membrane expression No anti-FH antibodies | 900 mg/w for 4 weeks +1200 mg (=4800 mg) | Weaning off HD within 1 month | Yes | 2.8 | Month 3: PR |
| Freyer et al., 2021, USA [18] | 1 | 51 F | MM | 2 | 1. VRD 2. KD | 20 mg/m2 | Cycle 1, day 2 | NA | 5.89 | Yes | No | 12 days | Normal CH50, C3–C4 heterozygous CFH3–CFH1 deletion | 900 mg/w for 4 weeks +1200 mg (>4800 mg) | HD pursuit | NA | NA | Day 154: death |
| Rassner et al., 2021, Germany [19] | 2 | 43 F 59 M | MM MM | 4 2 | 1. VAD/VCyD 2. KRD 3. M-ASCT 4. KRD 1. Elotuzumab/KRD 2. M-ASCT | NA NA | Cycle 3, day 2 Cycle 4, last day | PR PR | NA NA | Yes Yes | Yes Yes | NA 5 days | Consumed C3 and C4 NA | 900 mg/w for 7 weeks (=6300 mg) 900 mg/w for 4 weeks +1200 mg/2w × 2 (=6000 mg) | Weaning off within 1 month Wearing off | Yes Yes | <2 mg/dL NA eGFR from 10 to 32 mL/min | Year 1: CR of TMA and MM Month 4: CR of TMA and MM |
| Darwin et al., 2021, USA [12] | 1 | 53 F | MM—GVHD | 3 | 1. VRD 2. Allogenic SCT: FluMV/Tacrolimus-MTX 3. DaraKD | 56 mg/m2 | Cycle 18, day 7 | CR | 5.2 | No | Yes | 10 days | Normal CH50, C3–C4 | 900 mg/w for 4 weeks +1200 mg/2w (>4800 mg) | No HD | Yes | 1 mg/dL | CR |
| Scheggi et al., 2021, Italy [20] | 1 | 75 M | MM | 1 | 1. KRD | NA | Cycle 2, day 4 | NA | 7.77 | Yes | No | 2 days | NA | 900 mg/w for 4 weeks +1200 mg/2w (>4800 mg) | Weaning off within 1 month | NA | 2.48 mg/dL | NA |
| Moliz et al., 2018, Spain [11] | 1 | 71 F | MM | NA | 1. DaraKD | NA | Cycle 2, day 2 | NA | 2.6 | No | Yes | NA | NA | 900 mg/w for 3 weeks (=2700 mg) | No HD | NA | 1.1 mg/L | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pallotti, F.; Queffeulou, C.; Bellal, M.; Jean-Jacques, B.; Gac, A.-C.; Chatelet, V.; Boyer, A.; Gueutin, V. Carfilzomib-Induced Thrombotic Microangiopathy Treated with Eculizumab: A Case Report and Rapid Literature Review. Kidney Dial. 2022, 2, 625-637. https://doi.org/10.3390/kidneydial2040056
Pallotti F, Queffeulou C, Bellal M, Jean-Jacques B, Gac A-C, Chatelet V, Boyer A, Gueutin V. Carfilzomib-Induced Thrombotic Microangiopathy Treated with Eculizumab: A Case Report and Rapid Literature Review. Kidney and Dialysis. 2022; 2(4):625-637. https://doi.org/10.3390/kidneydial2040056
Chicago/Turabian StylePallotti, Federica, Claire Queffeulou, Mathieu Bellal, Bastien Jean-Jacques, Anne-Claire Gac, Valérie Chatelet, Annabel Boyer, and Victor Gueutin. 2022. "Carfilzomib-Induced Thrombotic Microangiopathy Treated with Eculizumab: A Case Report and Rapid Literature Review" Kidney and Dialysis 2, no. 4: 625-637. https://doi.org/10.3390/kidneydial2040056
APA StylePallotti, F., Queffeulou, C., Bellal, M., Jean-Jacques, B., Gac, A.-C., Chatelet, V., Boyer, A., & Gueutin, V. (2022). Carfilzomib-Induced Thrombotic Microangiopathy Treated with Eculizumab: A Case Report and Rapid Literature Review. Kidney and Dialysis, 2(4), 625-637. https://doi.org/10.3390/kidneydial2040056