
Why Does Vascular Access Dysfunction Occur despite Brachial Artery Blood Flow Being Higher than Preset Blood Flow?


{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
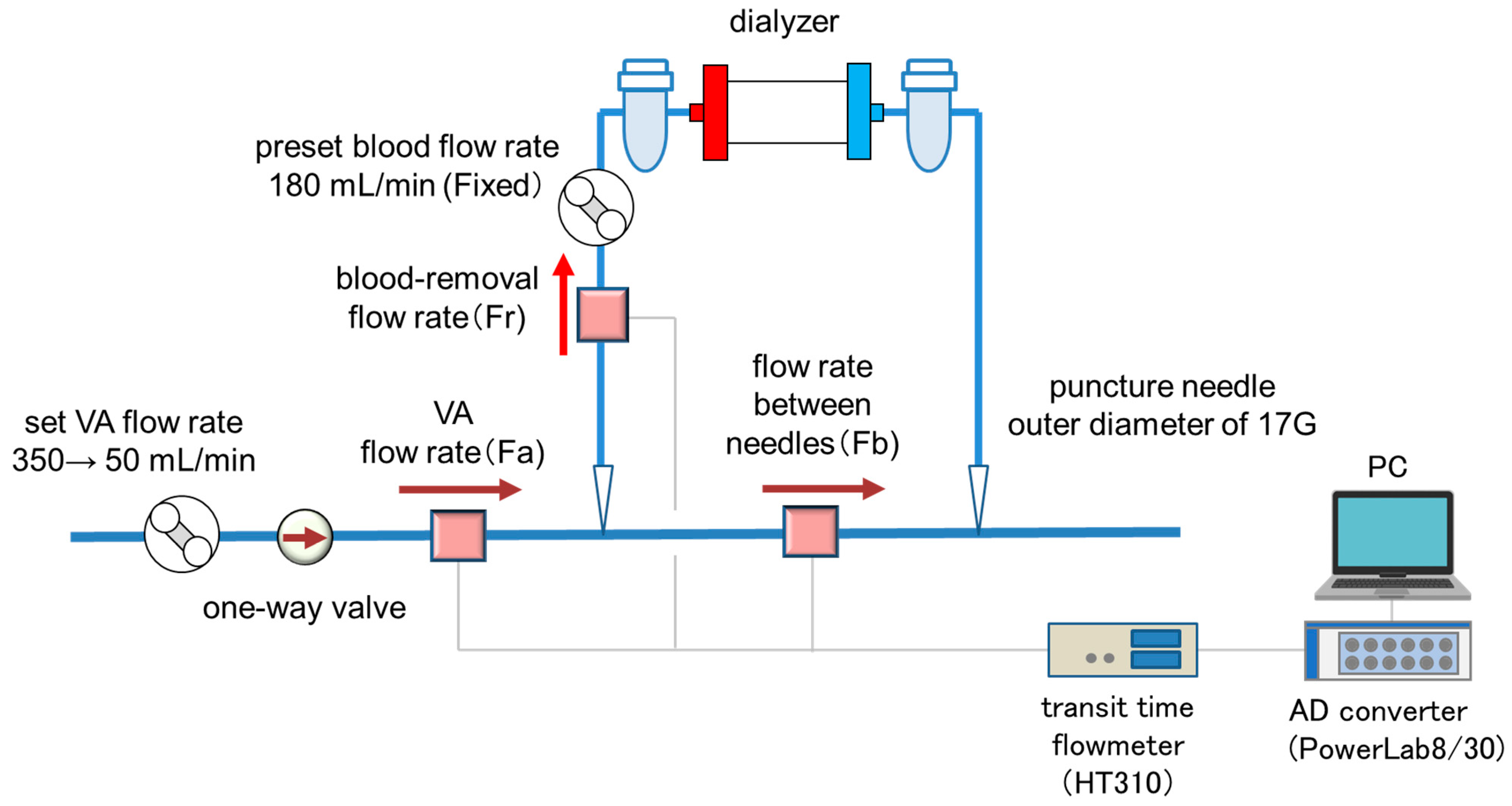
2.1. Experimental Circuit
2.2. Experimental Conditions and Methods for Calculating Actual Blood-Removal Flow and Recirculation Rate
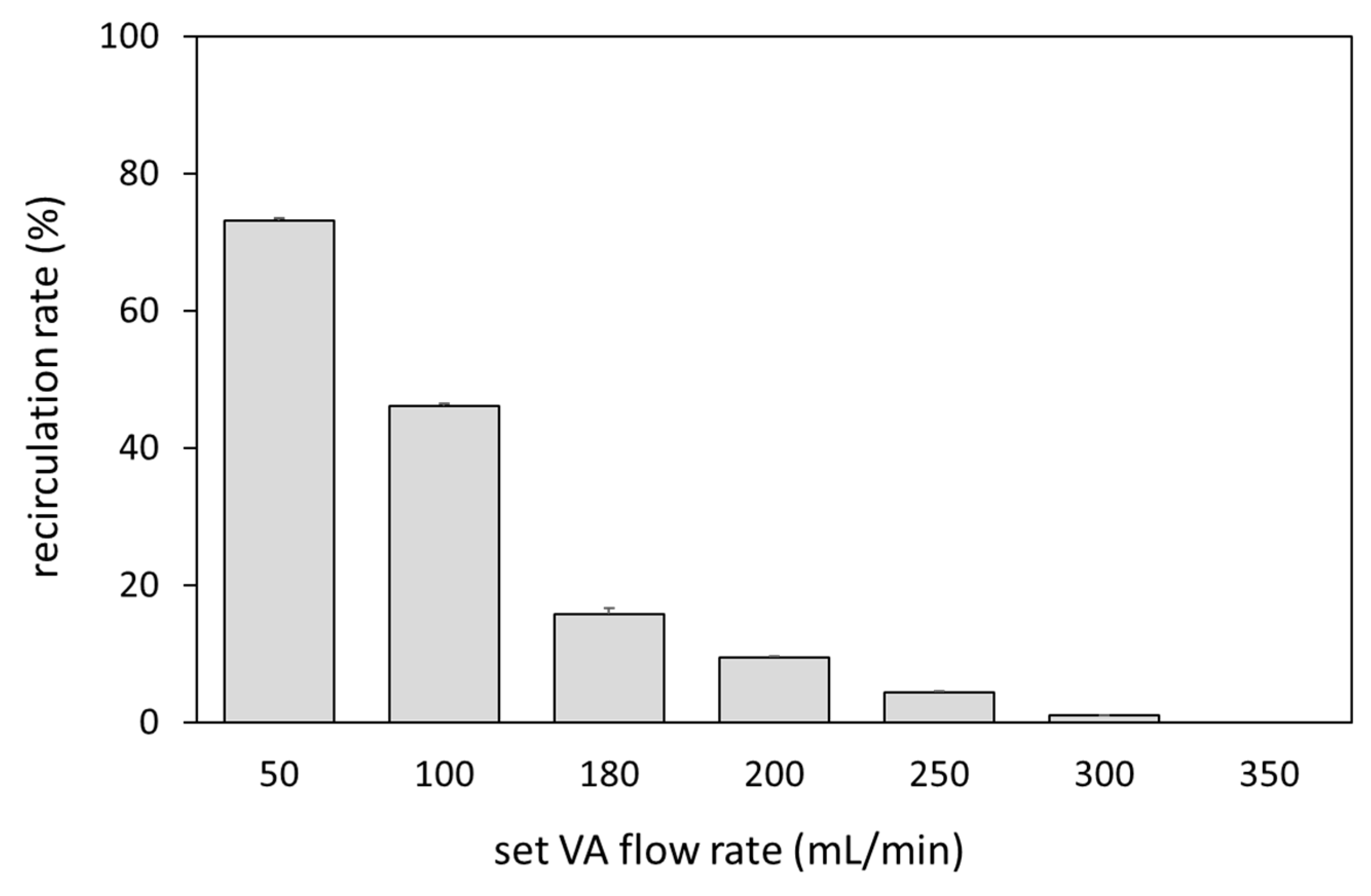
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kukita, K.; Ohira, S.; Amano, I.; Naito, H.; Azuma, N.; Ikeda, K.; Kanno, Y.; Satou, T.; Sakai, S.; Sugimoto, T.; et al. 2011 update Japanese Society for Dialysis Therapy Guidelines of Vascular Access Construction and Repair for Chronic Hemodialysis. Ther. Apher. Dial. 2015, 19 (Suppl. 1), 1–39. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, T.; Matsumura, O.; Matsuda, A.; Hasegawa, H.; Mitarai, T. Brachial artery blood flow measurement: A simple and non-invasive method to evaluate the need for arteriovenous fistula repair. Dial. Transpl. 2011, 40, 206–210. [Google Scholar] [CrossRef]
- Sato, T.; Tsuboi, M.; Onogi, T.; Miwa, N.; Sakurai, H.; Ookubo, K.; Matsubara, C.; Kasuga, H. Standard Procedures of Endovascular Treatment for Vascular Access Stenosis in our Facility—Clinical Usefulness of Ultrasonography. J. Vasc. Access 2015, 16 (Suppl. 10), S34–S37. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.; Lee, Y.-J.; Kim, S.-R. Value of Doppler evaluation of physically abnormal fistula: Hemodynamic guidelines and access outcomes. Korean J. Intern. Med. 2019, 34, 137–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ishii, T.; Suzuki, Y.; Nakayama, T.; Ohmori, M.; Masai, S.; Sasagawa, N.; Ohyama, K. Duplex ultrasound for the prediction of vascular events associated with arteriovenous fistulas in hemodialysis patients. J. Vasc. Access 2016, 17, 499–505. [Google Scholar] [CrossRef] [PubMed]
- Nitta, K.; Abe, M.; Masakane, I.; Hanafusa, N.; Taniguchi, M.; Hasegawa, T.; Nakai, S.; Wada, A.; Hamano, T.; Hoshino, J.; et al. Annual dialysis data report 2018, JSDT Renal Data Registry: Dialysis fluid quality, hemodialysis and hemodiafiltration, peritoneal dialysis, and diabetes. Ren. Replace. Ther. 2020, 6, 51. [Google Scholar] [CrossRef]
- Colombo, A.; Provenzano, M.; Rivoli, L.; Donato, C.; Capria, M.; Leonardi, G.; Chiarella, S.; Andreucci, M.; Fuiano, G.; Bolignano, D.; et al. Utility of Blood Flow/Resistance Index Ratio (Q x) as a Marker of Stenosis and Future Thrombotic Events in Native Arteriovenous Fistulas. Front. Surg. 2021, 7, 604347. [Google Scholar] [CrossRef] [PubMed]
- Maduell, F.; Vera, M.; Arias, M.; Serra, N.; Blasco, M.; Bergadá, E.; Fontsere, N.; Cases, A.; Campistol, J.M. Influence of the ionic dialysance monitor on Kt measurement in hemodialysis. Am. J. Kidney Dis. 2008, 52, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y.; Park, E.J.; Chang, J.H.; Han, B.G.; Kim, G.H. Use of blood temperature monitor with Twister device for the surveillance of vascular access in maintenance hemodialysis: Comparison with Doppler ultrasonography. J. Vasc. Access 2021, 22, 218–224. [Google Scholar] [CrossRef] [PubMed]
- Marques, M.G.; Ibeas, J.; Botelho, C.; Maia, P.; Ponce, P. Doppler Ultrasound: A Powerful Tool for Vascular Access Surveillance. Semin. Dial. 2014, 28, 206–210. [Google Scholar] [CrossRef] [PubMed]
- Coyne, D.W.; Delmez, J.; Spence, G.; Windus, D.W. Impaired delivery of hemodialysis prescriptions: An analysis of causes and an approach to evaluation. J. Am. Soc. Nephrol. 1997, 8, 1315–1318. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ono, J.-i.; Oiwa, T.; Ogasawara, Y.; Mochizuki, S. Why Does Vascular Access Dysfunction Occur despite Brachial Artery Blood Flow Being Higher than Preset Blood Flow? Kidney Dial. 2022, 2, 38-43. https://doi.org/10.3390/kidneydial2010005
Ono J-i, Oiwa T, Ogasawara Y, Mochizuki S. Why Does Vascular Access Dysfunction Occur despite Brachial Artery Blood Flow Being Higher than Preset Blood Flow? Kidney and Dialysis. 2022; 2(1):38-43. https://doi.org/10.3390/kidneydial2010005
Chicago/Turabian StyleOno, Jun-ichi, Takushi Oiwa, Yasuo Ogasawara, and Seiichi Mochizuki. 2022. "Why Does Vascular Access Dysfunction Occur despite Brachial Artery Blood Flow Being Higher than Preset Blood Flow?" Kidney and Dialysis 2, no. 1: 38-43. https://doi.org/10.3390/kidneydial2010005
APA StyleOno, J.-i., Oiwa, T., Ogasawara, Y., & Mochizuki, S. (2022). Why Does Vascular Access Dysfunction Occur despite Brachial Artery Blood Flow Being Higher than Preset Blood Flow? Kidney and Dialysis, 2(1), 38-43. https://doi.org/10.3390/kidneydial2010005