
Informed but Unvaccinated: A Cross-Sectional Study Among University Students in Ghana

 ,
,  ,
,  , , ,
, , , 
 and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Questionnaire
2.2. Study Design and Data Collection
2.3. Statistical Analysis
3. Results
3.1. Descriptive Statistics
3.1.1. Sociodemographic Information
3.1.2. Factors Influencing Vaccination
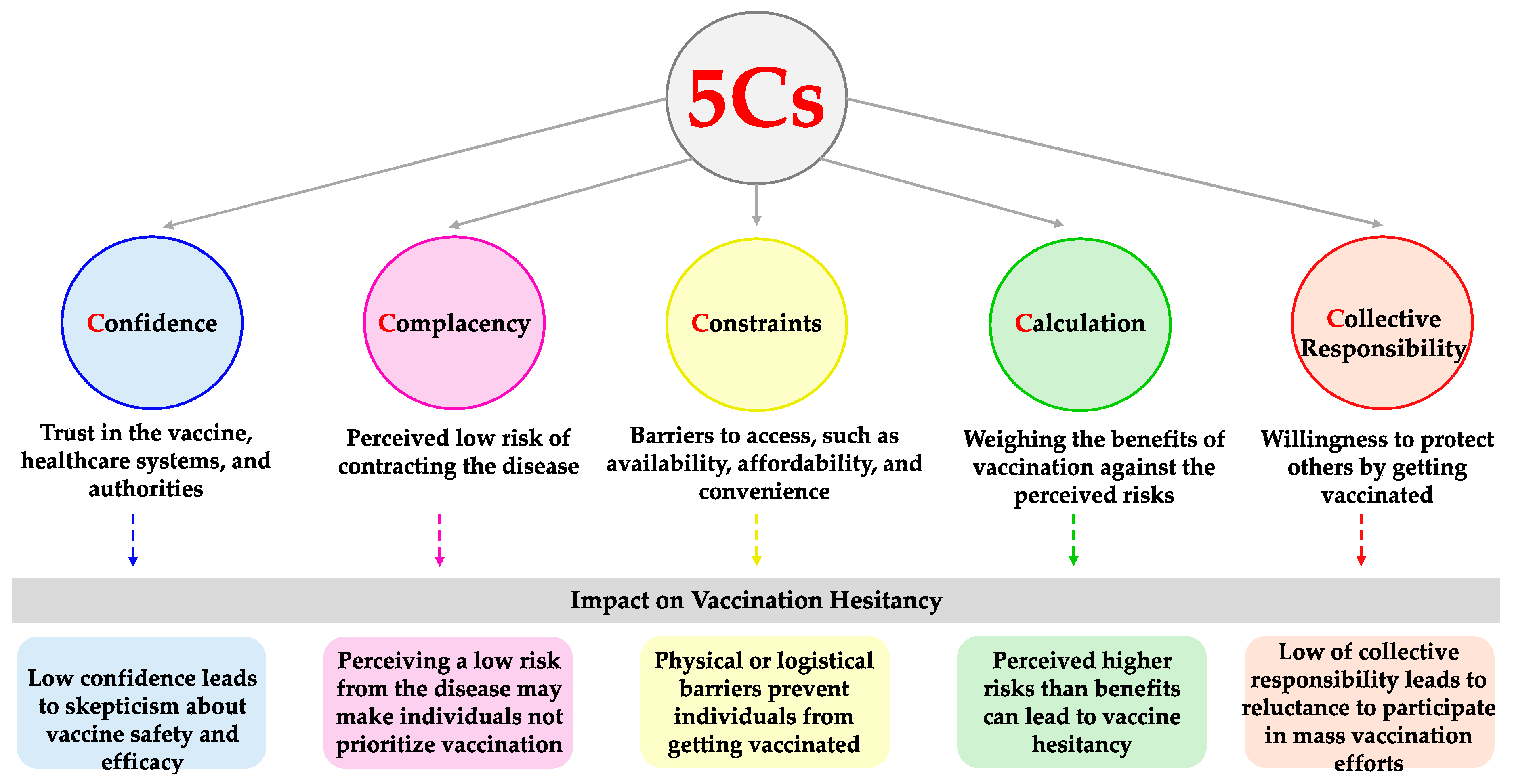
3.1.3. Distribution and Mean Scores of the 5Cs
3.2. Inferential Statistics
3.2.1. Evaluation of Factors Influencing Vaccination Behavior
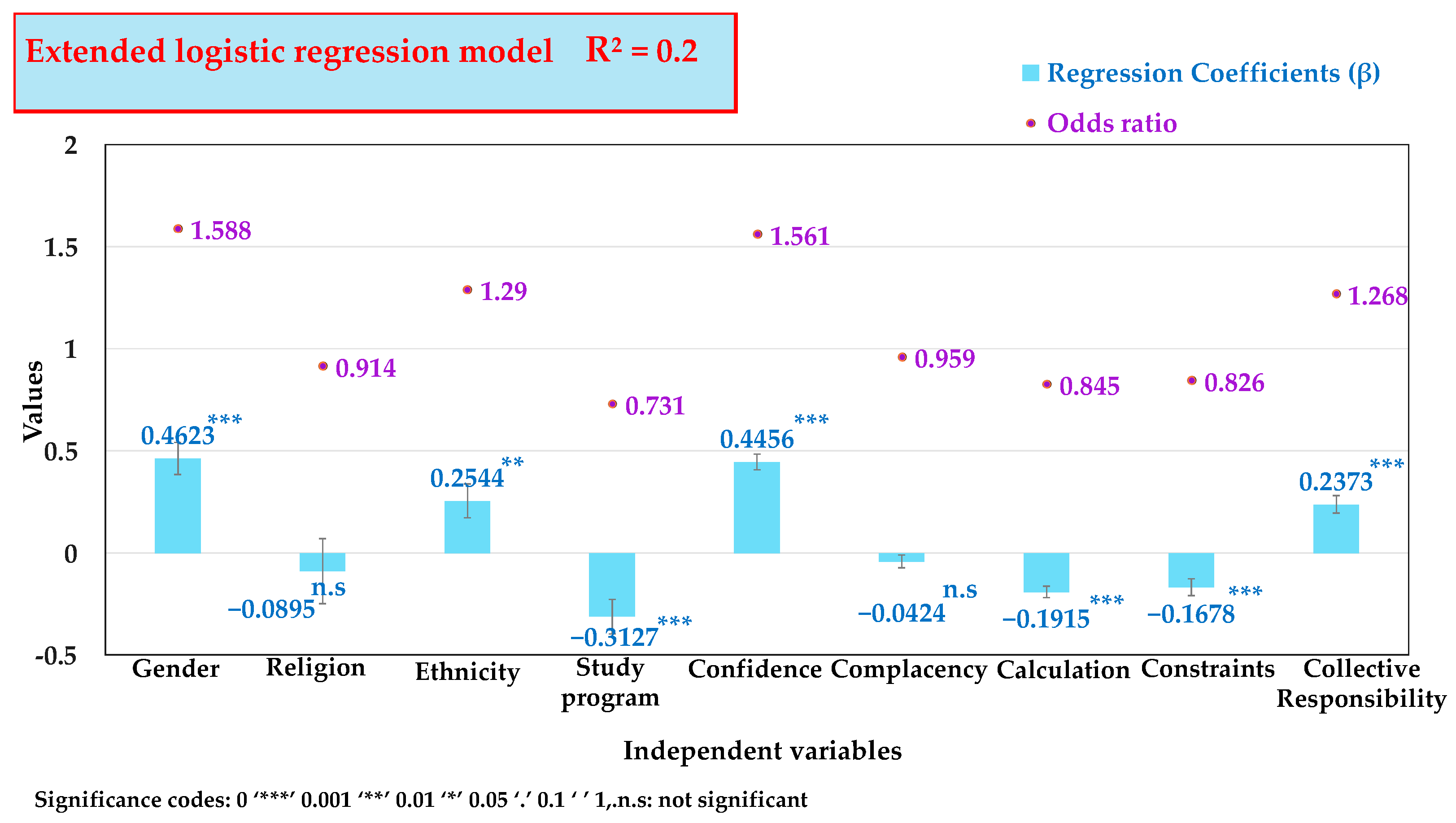
3.2.2. Multivariate Regression Explicating the 5Cs Model for Vaccination Hesitancy
4. Discussion
5. Limitations of This Study
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- COVID-19 Cases|WHO COVID-19 Dashboard. Available online: https://data.who.int/dashboards/covid19/cases (accessed on 2 September 2024).
- Pitlik, S.D. COVID-19 Compared to Other Pandemic Diseases. Rambam Maimonides Med. J. 2020, 11, e0027. [Google Scholar] [CrossRef] [PubMed]
- Boakye, E.A.; Hongjiang, Z.; Ahia, B.N.K.; Damoah, M.A. COVID-19 Pandemic: Exploring the Fiscal and Monetary Policies for Mitigating the Socio-Economic Impact on Ghana’s Economy. In New Innovations in Economics, Business and Management Vol. 9; Erokhin, V., Ed.; Book Publisher International (A Part of SCIENCEDOMAIN International): London, UK, 2022; pp. 22–39. ISBN 978-93-5547-719-4. [Google Scholar]
- Barrett, R.; Zuckerman, M.; Dudgeon, M.R.; Armelagos, G.J. Emerging Infections: Three Epidemiological Transitions from Prehistory to the Present; Oxford University Press: Oxford, UK, 2024; ISBN 978-0-19-265484-7. [Google Scholar]
- Awedoba, A.K.; Kamski, B.; Mehler, A.; Sebudubudu, D. Africa Yearbook Volume 16: Politics, Economy and Society South of the Sahara in 2019. In Africa Yearbook Volume 16; Brill: Leiden, The Netherlands, 2020; ISBN 978-90-04-43001-3. [Google Scholar]
- Journell, W. Post-Pandemic Social Studies: How COVID-19 Has Changed the World and How We Teach; Teachers College Press: New York, NY, USA, 2021; ISBN 978-0-8077-8068-8. [Google Scholar]
- Fieselmann, J.; Annac, K.; Erdsiek, F.; Yilmaz-Aslan, Y.; Brzoska, P. What Are the Reasons for Refusing a COVID-19 Vaccine? A Qualitative Analysis of Social Media in Germany. BMC Public Health 2022, 22, 846. [Google Scholar] [CrossRef]
- Heinze, A.-S.; Weisskircher, M. How Political Parties Respond to Pariah Street Protest: The Case of Anti-Corona Mobilisation in Germany. Ger. Politics 2022, 32, 563–584. [Google Scholar]
- Klich-Kluczewska, B.; von Puttkamer, J.; Rebitschek, I. (Eds.) Biopolitics in Central and Eastern Europe in the 20th Century: Fearing for the Nation; Routledge: London, UK, 2022; ISBN 978-1-003-16108-0. [Google Scholar]
- MacDonald, N.E. Vaccine Hesitancy: Definition, Scope and Determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef] [PubMed]
- Bedford, H.; Attwell, K.; Danchin, M.; Marshall, H.; Corben, P.; Leask, J. Vaccine Hesitancy, Refusal and Access Barriers: The Need for Clarity in Terminology. Vaccine 2018, 36, 6556–6558. [Google Scholar] [CrossRef]
- COVID-19 Vaccines. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/covid-19-vaccines (accessed on 2 September 2024).
- Sinuraya, R.K.; Nuwarda, R.F.; Postma, M.J.; Suwantika, A.A. Vaccine Hesitancy and Equity: Lessons Learned from the Past and How They Affect the COVID-19 Countermeasure in Indonesia. Glob. Health 2024, 20, 11. [Google Scholar] [CrossRef]
- Nuwarda, R.F.; Ramzan, I.; Weekes, L.; Kayser, V. Vaccine Hesitancy: Contemporary Issues and Historical Background. Vaccines 2022, 10, 1595. [Google Scholar] [CrossRef]
- Hamson, E.; Forbes, C.; Wittkopf, P.; Pandey, A.; Mendes, D.; Kowalik, J.; Czudek, C.; Mugwagwa, T. Impact of Pandemics and Disruptions to Vaccination on Infectious Diseases Epidemiology Past and Present. Hum. Vaccines Immunother. 2023, 19, 2219577. [Google Scholar] [CrossRef]
- Snyder, M.R.; McGinty, M.D.; Shearer, M.P.; Meyer, D.; Hurtado, C.; Nuzzo, J.B. Outbreaks of Hepatitis A in US Communities, 2017–2018: Firsthand Experiences and Operational Lessons From Public Health Responses. Am. J. Public Health 2019, 109, S297–S302. [Google Scholar] [CrossRef]
- Abdin, A.Y.; De Pretis, F.; Landes, J. Fast Methods for Drug Approval: Research Perspectives for Pandemic Preparedness. Int. J. Environ. Res. Public Health 2023, 20, 2404. [Google Scholar] [CrossRef]
- Buonomo, B.; Della Marca, R. A Behavioural Vaccination Model with Application to Meningitis Spread in Nigeria. Appl. Math. Model. 2024, 125, 334–350. [Google Scholar] [CrossRef]
- Immunization Coverage. Available online: https://www.who.int/news-room/fact-sheets/detail/immunization-coverage (accessed on 2 September 2024).
- Atinga, R.A.; Koduah, A.; Abiiro, G.A. Understanding the Policy Dynamics of COVID-19 Vaccination in Ghana through the Lens of a Policy Analytical Framework. Health Res. Policy Syst. 2022, 20, 94. [Google Scholar] [CrossRef] [PubMed]
- Nonvignon, J.; Owusu, R.; Asare, B.; Adjagba, A.; Aun, Y.W.; Yeung, K.H.T.; Azeez, J.N.K.; Gyansa-Lutterodt, M.; Gulbi, G.; Amponsa-Achiano, K.; et al. Estimating the Cost of COVID-19 Vaccine Deployment and Introduction in Ghana Using the CVIC Tool. Vaccine 2022, 40, 1879–1887. [Google Scholar] [CrossRef]
- COVID-19 Data|WHO COVID-19 Dashboard. Available online: https://data.who.int/dashboards/covid19/data (accessed on 11 November 2024).
- Geoghegan, S.; O’Callaghan, K.P.; Offit, P.A. Vaccine Safety: Myths and Misinformation. Front. Microbiol. 2020, 11, 372. [Google Scholar] [CrossRef]
- Peters, M.D.J. Addressing Vaccine Hesitancy and Resistance for COVID-19 Vaccines. Int. J. Nurs. Stud. 2022, 131, 104241. [Google Scholar] [CrossRef] [PubMed]
- Yeboah, P.; Daliri, D.B.; Abdin, A.Y.; Appiah-Brempong, E.; Pitsch, W.; Panyin, A.B.; Adusei, E.B.A.; Razouk, A.; Nasim, M.J.; Jacob, C. Knowledge into the Practice against COVID-19: A Cross-Sectional Study from Ghana. Int. J. Environ. Res. Public Health 2021, 18, 12902. [Google Scholar] [CrossRef]
- Poland, C.M.; Jacobson, R.M.; Opel, D.J.; Marcuse, E.K.; Poland, G.A. Political, Ethical, Social, and Psychological Aspects of Vaccinology. In Vaccinology; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2015; pp. 335–357. ISBN 978-1-118-63803-3. [Google Scholar]
- Betsch, C.; Schmid, P.; Heinemeier, D.; Korn, L.; Holtmann, C.; Böhm, R. Beyond Confidence: Development of a Measure Assessing the 5C Psychological Antecedents of Vaccination. PLoS ONE 2018, 13, e0208601. [Google Scholar] [CrossRef]
- Sallam, M. COVID-19 Vaccine Hesitancy Worldwide: A Concise Systematic Review of Vaccine Acceptance Rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef]
- Daley, M.F.; Narwaney, K.J.; Shoup, J.A.; Wagner, N.M.; Glanz, J.M. Addressing Parents’ Vaccine Concerns: A Randomized Trial of a Social Media Intervention. Am. J. Prev. Med. 2018, 55, 44–54. [Google Scholar] [CrossRef]
- Askelson, N.M.; Campo, S.; Lowe, J.B.; Smith, S.; Dennis, L.K.; Andsager, J. Using the Theory of Planned Behavior to Predict Mothers’ Intentions to Vaccinate Their Daughters Against HPV. J. Sch. Nurs. 2010, 26, 194–202. [Google Scholar] [CrossRef]
- Omer, S.B.; Orenstein, W.A.; Koplan, J.P. Go Big and Go Fast—Vaccine Refusal and Disease Eradication. N. Engl. J. Med. 2013, 368, 1374–1376. [Google Scholar] [CrossRef] [PubMed]
- Petrocelli, J.V. Factor Validation of the Consideration of Future Consequences Scale: Evidence for a Short Version. J. Soc. Psychol. 2003, 143, 405–413. [Google Scholar] [CrossRef] [PubMed]
- Fox, J.; Weisberg, S. An R Companion to Applied Regression; SAGE Publications: Los Angeles, CA, USA, 2018; ISBN 978-1-5443-3648-0. [Google Scholar]
- Buuren, S.V.; Groothuis-Oudshoorn, K. Mice: Multivariate Imputation by Chained Equations in R. J. Stat. Softw. 2011, 45, 1–67. [Google Scholar] [CrossRef]
- Salman, M.; Mallhi, T.H.; Tanveer, N.; Shehzadi, N.; Khan, H.M.; Mustafa, Z.U.; Khan, T.M.; Hussain, K.; Mohamed, M.S.; Maqbool, F.; et al. Evaluation of Conspiracy Beliefs, Vaccine Hesitancy, and Willingness to Pay towards COVID-19 Vaccines in Six Countries from Asian and African Regions: A Large Multinational Analysis. Vaccines 2022, 10, 1866. [Google Scholar] [CrossRef] [PubMed]
- Arko, A.B. COVID-19 Vaccine Hesitancy and Acceptance among University Students in Ghana. ADRRI J. Arts Soc. Sci. 2023, 20, 52–74. [Google Scholar]
- Rancher, C.; Moreland, A.D.; Smith, D.W.; Cornelison, V.; Schmidt, M.G.; Boyle, J.; Dayton, J.; Kilpatrick, D.G. Using the 5C Model to Understand COVID-19 Vaccine Hesitancy across a National and South Carolina Sample. J. Psychiatr. Res. 2023, 160, 180–186. [Google Scholar] [CrossRef]
- Willis, D.E.; Andersen, J.A.; Bryant-Moore, K.; Selig, J.P.; Long, C.R.; Felix, H.C.; Curran, G.M.; McElfish, P.A. COVID-19 Vaccine Hesitancy: Race/Ethnicity, Trust, and Fear. Clin. Transl. Sci. 2021, 14, 2200–2207. [Google Scholar] [CrossRef]
- Howard, M.C. Gender and Vaccination: Understanding the Multifaceted Role of a Multidimensional Conceptualization of Vaccine Hesitancy. Psychol. Health Med. 2024, 29, 1055–1062. [Google Scholar] [CrossRef]
- Saaka, S.A.; Mohammed, K.; Pienaah, C.K.A.; Luginaah, I. Child Malaria Vaccine Uptake in Ghana: Factors Influencing Parents’ Willingness to Allow Vaccination of Their Children under Five (5) Years. PLoS ONE 2024, 19, e0296934. [Google Scholar] [CrossRef]
- Kibongani Volet, A.; Scavone, C.; Catalán-Matamoros, D.; Capuano, A. Vaccine Hesitancy Among Religious Groups: Reasons Underlying This Phenomenon and Communication Strategies to Rebuild Trust. Front. Public Health 2022, 10, 824560. [Google Scholar] [CrossRef]
- Asuman, D.; Ackah, C.G.; Enemark, U. Inequalities in Child Immunization Coverage in Ghana: Evidence from a Decomposition Analysis. Health Econ. Rev. 2018, 8, 9. [Google Scholar] [CrossRef] [PubMed]
- Kuuyi, A.; Kogi, R. Factors Contributing to Immunization Coverage among Children Less than 5 Years in Nadowli-Kaleo District of Upper West Region, Ghana. PLoS Glob. Public Health 2024, 4, e0002881. [Google Scholar] [CrossRef]
- Asante, R.; Gyimah-Boadi, E. Ethnic Structure, Inequality and Governance of the Public Sector in Ghana; United Nations Research Institute for Social Development: Geneva, Switzerland, 2004. [Google Scholar]
- Nicola, M.; Sohrabi, C.; Mathew, G.; Kerwan, A.; Al-Jabir, A.; Griffin, M.; Agha, M.; Agha, R. Health Policy and Leadership Models during the COVID-19 Pandemic: A Review. Int. J. Surg. 2020, 81, 122–129. [Google Scholar] [CrossRef]
- Nwachukwu, G.; Rihan, A.; Nwachukwu, E.; Uduma, N.; Elliott, K.S.; Tiruneh, Y.M. Understanding COVID-19 Vaccine Hesitancy in the United States: A Systematic Review. Vaccines 2024, 12, 747. [Google Scholar] [CrossRef]
- Mudhune, V.; Ondeng’e, K.; Otieno, F.; Otieno, D.B.; Bulinda, C.M.; Okpe, I.; Nabia, S.; Bar-Zeev, N.; Otieno, O.; Wonodi, C. Determinants of COVID-19 Vaccine Acceptability among Healthcare Workers in Kenya—A Mixed Methods Analysis. Vaccines 2023, 11, 1290. [Google Scholar] [CrossRef] [PubMed]
- Dureab, F.; Al-Awlaqi, S.; Jahn, A. COVID-19 in Yemen: Preparedness Measures in a Fragile State. Lancet Public Health 2020, 5, e311. [Google Scholar] [CrossRef] [PubMed]
- Mercola, J.; Cummins, R. The Truth About COVID-19: Exposing The Great Reset, Lockdowns, Vaccine Passports, and the New Normal; Chelsea Green Publishing: Chelsea, VT, USA, 2021; ISBN 978-1-64502-088-2. [Google Scholar]
- Fuchs, C. Communicating COVID-19: Everyday Life, Digital Capitalism, and Conspiracy Theories in Pandemic Times; Emerald Group Publishing: Leeds, UK, 2021; ISBN 978-1-80117-720-7. [Google Scholar]
- Sundstrom, B.; Cartmell, K.B.; White, A.A.; Well, H.; Pierce, J.Y.; Brandt, H.M. Correcting HPV Vaccination Misinformation Online: Evaluating the HPV Vaccination NOW Social Media Campaign. Vaccines 2021, 9, 352. [Google Scholar] [CrossRef]
- Cao, A.; Ueta, M.; Uchibori, M.; Murakami, M.; Kunishima, H.; Santosh Kumar, R.; Prommas, P.; Tomoi, H.; Gilmour, S.; Sakamoto, H.; et al. Trust in Governments, Public Health Institutions, and Other Information Sources as Determinants of COVID-19 Vaccine Uptake Behavior in Japan. Vaccine 2024, 42, 3684–3692. [Google Scholar] [CrossRef]
- Edwards, A.L. The Social Desirability Variable in Personality Assessment and Research; Dryden Press: Ft Worth, TX, USA, 1957; pp. viii, 108. [Google Scholar]
- Stöber, J. The Social Desirability Scale-17 (SDS-17). Eur. J. Psychol. Assess. 2001, 17, 222–232. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Vaccination-Related Factors | Valid | Mean | SD |
|---|---|---|---|
| Vaccine Experience | 1878 | 0.64 | 0.30 |
| Conspiracy Mentality | 1797 | 0.7 | 0.24 |
| Vaccine Attributes | 3486 | 0.2 | 0.23 |
| 5Cs | Mean | SD |
|---|---|---|
| Confidence | 2.30 | 1.31 |
| Complacency | 4.40 | 1.79 |
| Constraints | 3.88 | 1.95 |
| Calculation | 1.98 | 1.09 |
| Collective Responsibility | 2.88 | 1.19 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yeboah, P.; Abdin, A.Y.; Gyasi, T.O.; Anyimiah, P.; Osafo, N.; Skotzke, P.; Pitsch, W.; Brobbey, M.O.; Panyin, A.B.; Razouk, A.; et al. Informed but Unvaccinated: A Cross-Sectional Study Among University Students in Ghana. COVID 2025, 5, 47. https://doi.org/10.3390/covid5040047
Yeboah P, Abdin AY, Gyasi TO, Anyimiah P, Osafo N, Skotzke P, Pitsch W, Brobbey MO, Panyin AB, Razouk A, et al. Informed but Unvaccinated: A Cross-Sectional Study Among University Students in Ghana. COVID. 2025; 5(4):47. https://doi.org/10.3390/covid5040047
Chicago/Turabian StyleYeboah, Prince, Ahmad Yaman Abdin, Trudy Osei Gyasi, Priscilla Anyimiah, Newman Osafo, Philip Skotzke, Werner Pitsch, Mahmood Oppong Brobbey, Anto Berko Panyin, Afraa Razouk, and et al. 2025. "Informed but Unvaccinated: A Cross-Sectional Study Among University Students in Ghana" COVID 5, no. 4: 47. https://doi.org/10.3390/covid5040047
APA StyleYeboah, P., Abdin, A. Y., Gyasi, T. O., Anyimiah, P., Osafo, N., Skotzke, P., Pitsch, W., Brobbey, M. O., Panyin, A. B., Razouk, A., Nasim, M. J., & Jacob, C. (2025). Informed but Unvaccinated: A Cross-Sectional Study Among University Students in Ghana. COVID, 5(4), 47. https://doi.org/10.3390/covid5040047