Abstract
Background: Fear of COVID-19 has been associated with adverse mental and physical health outcomes, yet evidence from The Netherlands is limited. This study investigated associations between fear of COVID-19, mood, quality of life, immune fitness, and related health variables during the first Dutch national lockdown and identified key predictors of fear. Methods: In June–July 2020, n = 1020 Dutch adults completed an online survey assessing demographics, personality, mental resilience, pain sensitivity, pain catastrophizing, alcohol use, immune fitness, and mood. Retrospective ratings were provided for the pre-pandemic period (January–March 2020) and the first lockdown (March–May 2020). Fear of COVID-19 was measured using a modified Fear of COVID-19 Scale. Results: Overall, 13.2% of participants reported significant fear of COVID-19, which was associated with poorer mood, reduced quality of life, lower immune fitness, more severe COVID-19 symptoms, greater pain sensitivity, and higher levels of pain catastrophizing. Regression analysis explained 19.6% of the variance, with pre-pandemic anxiety (8.7%) and poorer immune fitness (3.4%) as the strongest predictors of fear of COVID-19, followed by lower psychoticism, lower mental resilience, older age, greater helplessness, and greater extraversion. Discussion: These findings suggest that a minority experienced high levels of fear of COVID-19 with substantial consequences, including negative effects on mood, immune fitness, and quality of life. The strong association with pre-existing anxiety and immune fitness highlights the need for early identification and targeted interventions for vulnerable groups to reduce psychological and physical health impacts in future public health crises.
1. Introduction
The 2019 coronavirus disease (COVID-19) pandemic profoundly affected global health and had a substantial psychosocial impact worldwide [1,2,3]. Fear of COVID-19, assessed with the Fear of COVID-19 Scale [4], has been linked to adverse mental and physical health outcomes, including elevated anxiety, stress, and depression [5,6,7,8,9,10,11,12]. However, reported prevalence rates vary across studies, with anxiety ranging from 6.3% to 50.9% and depression ranging from 14.6% to 63.8% [5,9], reflecting substantial variability across populations and study designs.
During the early phase of the pandemic, mental health problems were reported across diverse population groups, including post-traumatic symptoms in infected individuals and heightened anxiety among healthcare workers [13,14]. Lockdown measures, including the shift to online education, had marked effects on children, adolescents, and students, with widespread symptoms of anxiety and depression [15,16]. More than half of the general population experienced psychiatric symptoms [17], with the burden especially high among individuals with pre-existing mental health conditions, lower socioeconomic status, or healthcare-related occupations [15,18]. Nevertheless, meta-analytic findings indicate that the psychological impact of lockdowns varied considerably, with substantial resilience observed in unaffected subpopulations [19]. Fear of COVID-19 was particularly elevated among women and healthcare workers [13] and showed strong correlations with anxiety, but only moderate correlations with depression and stress [7,20]. Demographic factors such as female sex, younger age, urban residence, and pre-existing mental health conditions have been associated with higher fear levels [21], while cultural and geographical contexts may further shape these associations [22].
Despite the rapidly expanding body of international research, no quantitative studies have examined predictors of fear of COVID-19 and its associated health consequences in The Netherlands. This gap is important, as national responses, public communication, and societal structures can influence both the prevalence and the impact of pandemic-related fear, making findings from other countries not directly generalizable. The current, study therefore, evaluated fear of COVID-19 and its consequences during the first Dutch national lockdown (15 March 2020–11 May 2020).
This lockdown was characterized by strict social restrictions, widespread uncertainty, and the absence of vaccines or effective treatments. To combat the spread of the virus, measures included social distancing (i.e., keeping a 1.5 m distance from other individuals and the avoidance of crowded venues) [23], refraining from handshakes, regular handwashing, use of tissues, coughing and sneezing into the elbow, and staying home when experiencing symptoms [23]. Although facemasks were not mandatory, working from home was recommended for all but vital occupations (e.g., police and healthcare workers). Schools and universities were closed, with education continuing online. Social venues and most businesses were shut, except for supermarkets and pharmacies. Gatherings were limited to a maximum of three people, while the public received daily government and media updates on infection rates, hospitalizations, and deaths. Together, these conditions may have amplified fear of COVID-19, i.e., being afraid of contracting the disease and its consequences, particularly among vulnerable groups. Understanding the impact and correlations of such fear is essential to evaluate the broader impact of lockdowns on health and to identify individuals who may require targeted interventions.
At present, knowledge on factors that may aggravate or moderate fear of COVID-19 is limited. However, demographic factors such as female sex, younger age, and pre-existing mental health conditions (e.g., anxiety and depression) have been associated with higher fear of COVID-19 levels [21]. Therefore, the present study aimed to examine the relationship between fear of COVID-19 and a broad range of demographic, psychological, lifestyle, and health correlates. As well as its relationship with mental health, quality of life, and immune fitness, this study sought to identify the strongest predictors of fear of COVID-19, including demographic, psychological, personality, lifestyle, and pre-pandemic mental or physical health conditions. Based on the previous literature, we hypothesized that pre-existing (mental) health conditions would be the strongest predictors of elevated fear of COVID-19.
2. Methods
Data were drawn from the “Corona lockdown: How fit are you?” (CLOFIT) Study [24] was an online survey conducted between 24 June and 26 July 2020 via the SurveyMonkey platform. Adults of both sexes, aged 18 years and older, were recruited through Facebook advertisements. The anonymous survey was approved by the Ethics Committee of the Faculty of Social and Behavioral Sciences of Utrecht University (approval code: FETC17–061, approval date: 8 June 2017), and all participants provided electronic informed consent. The survey collected data on demographics, mental resilience, personality, pain sensitivity, and pain catastrophizing, as well as retrospective ratings of fear of COVID-19, mood, health correlates, and alcohol consumption for the pre-pandemic period (January–March 15, 2020) and the first Dutch lockdown (15 March–11 May 2020). A detailed description of the CLOFIT methodology has been published elsewhere [24].
Demographic data included age, sex, weight, height, presence of underlying disease (yes, no), education level (low, middle, high), and ethnicity (Dutch, Western, non-Western). Body Mass Index (BMI) was calculated as kg/m2 [25]. Mental resilience was assessed using the Dutch version of the Brief Resilience Scale (BRS) [26], a 6-item questionnaire that measures the ability to recover from stress on a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree). Higher scores indicate greater resilience. Personality was assessed with the Dutch version of the 48-item Eysenck Personality Questionnaire [27,28], which yields subscales for psychoticism, extraversion, and neuroticism (score range 0–12), with higher scores reflecting stronger expression of the respective trait.
Pain sensitivity was measured using the shortened 10-item Pain Sensitivity Questionnaire (PSQ) [29]. For each item, pain intensity was rated from 0 (“no pain”) to 10 (“most intense pain imaginable”), and the mean score across items was calculated, with higher scores reflecting greater sensitivity. Pain catastrophizing was assessed with the shortened Pain Catastrophizing Scale (PCQ) [30], consisting of three items assessing rumination, magnification, and helplessness. Each item was rated from 1 (“not at all”) to 5 (“always”), and a sum score represented overall pain catastrophizing.
Fear of COVID-19 during the first lockdown was measured using a modified seven-item version of the Fear of COVID-19 Scale [4]. In the original version, the scoring on a 5-point Likert scale ranged from 1 (strongly disagree) to 5 (strongly agree) [4]. In the current study, the 1–5 range was adjusted to a range from -2 (strongly disagree) to +2 (strongly agree), with 0 as a neutral midpoint, and the mean score was used as an overall measure of fear [24]. This was performed to make the neutral midpoint clearer to the participants.
Assessments were conducted for both the pre-pandemic period (1 January–14 March 2020) and the first lockdown (15 March–11 May 2020). Mood and quality of life were assessed using single-item ratings. Mood items included stress, anxiety, depression, activity, fatigue, hostility, loneliness, and happiness, each rated on a scale from 0 (absent) to 10 (extreme) [31]. Quality of life was assessed on a 0 (very poor) to 10 (excellent) scale [32]. Immune fitness was measured using a single-item scale from 0 (poor) to 10 (excellent) [33], and immune fitness in the past year (2019) was assessed with the Immune Status Questionnaire (ISQ) [34].
COVID−19 symptoms were assessed with a nine-item scale covering sneezing, runny nose, sore throat, cough, malaise, high temperature (up to 38 °C), fever (≥38 °C), shortness of breath, and chest pain [24]. Each symptom was rated as none (0), mild (1), moderate (2), or severe (3). Two summary measures were derived: overall symptom severity (mean score across items) and symptom presence (number of symptoms with a score > 0).
Alcohol consumption was recorded as the number of alcoholic drinks and drinking days per week. In addition, participants reported the number of hangovers they experienced per month.
Statistical Analysis
Data were analyzed using SPSS (IBM Corp., Released 2013. IBM SPSS Statistics for Windows, Version 30.0. Armonk, NY, USA: IBM Corp.). The fear of COVID data was not normally distributed. Therefore, nonparametric tests were applied. First, it was determined how demographic variables are related to fear of COVID. Group comparisons between two categories (e.g., sex, underlying disease) were conducted using the Independent Samples Mann–Whitney U Test, and comparisons across more than two categories (e.g., ethnicity, education level) were conducted using the Independent Samples Kruskal–Wallis Test. When applicable, Bonferroni’s correction was applied, and results were considered significant at p < 0.05. Percentual data were compared using Chi-squared tests. Second, participants were divided into two groups: those with significant fear of COVID-19 (score > 0) and those with limited or no fear (score ≤ 0). Demographics, mood, health correlations, alcohol consumption, personality, and pain sensitivity and catastrophizing were compared between the two groups. The comparisons were conducted with the Independent Samples Mann–Whitney U Test. When applicable, Bonferroni’s correction was applied, and results were considered significant at p < 0.05. Third, associations between fear of COVID-19 and other variables were assessed with Spearman’s correlations (significance threshold p < 0.05).
Finally, a stepwise linear regression analysis was performed to identify predictors of fear of COVID-19 during the first lockdown. Potential predictor variables included demographics (age, sex, BMI, ethnicity, education level, underlying disease), immune status (past year’s immune status, pre-COVID immune fitness), psychological measures (stress, anxiety, depression, activity, tiredness, hostility, loneliness, happiness, quality of life, mental resilience) personality traits (psychoticism, neuroticism, extraversion), pain-related measures (pain sensitivity, rumination, magnification, helplessness, total catastrophizing score), and alcohol-related measures (alcoholic drinks per week, drinking days per week hangovers per month).
3. Results
Data from n = 1020 participants in the CLOFIT study were included in the analysis. The mean (SD) fear of COVID-19 score during the first lockdown period was −1.0 (0.9). The distribution of scores, ranging from no fear to great fear, is shown in Figure 1.
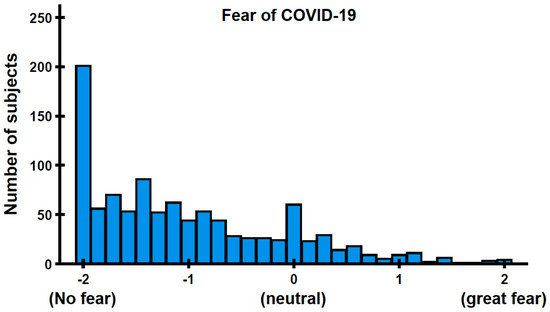
Figure 1.
Distribution of fear of COVID-19 during the first lockdown period in The Netherlands.
As illustrated in Figure 1, the majority of participants reported limited or no fear of COVID-19, with scores below the neutral midpoint (0). In contrast, 13.2% of participants scored above 0, indicating the presence of fear. Fear of COVID-19 scores by demographic characteristics are summarized in Table 1. Men reported significantly lower fear of COVID-19 scores than women (p < 0.001). Higher education was associated with lower fear of COVID-19, with a significant difference observed between the low and high education groups (p = 0.019). Participants without underlying disease reported significantly less fear than those with an underlying disease (p < 0.001). No significant differences were observed by ethnicity (p = 0.823).

Table 1.
Fear of COVID-19 according to demographics.
Participants were divided into two groups: those with a significant fear of COVID-19 (score > 0, mean (SD) = +0.7 (0.5)) and those with limited or no fear (score ≤ 0, mean (SD) = −1.3 (0.6)). Table 2 presents the outcomes for both groups during the first lockdown. Compared to participants with limited/no fear, those with a significant fear of COVID-19 reported poorer mood, lower immune fitness, more frequent and severe COVID-19 symptoms, reduced mental resilience and psychoticism, higher neuroticism, and greater pain sensitivity and catastrophizing.
Table 2.
Study outcomes assessed for the first COVID-19 lockdown.
In the group with significant fear of COVID-19, women, individuals with lower education, and those with underlying diseases were overrepresented. No significant group differences were observed for ethnicity.
The overall study outcomes and their correlations with fear of COVID-19 are summarized in Table 3. Significant associations were found for all mood items, quality of life, and immune fitness, with the strongest correlations observed for anxiety, immune fitness, stress, and mental resilience.
Table 3.
Correlations of fear of COVID-19 with the study outcomes (assessed for the first COVID-19 lockdown).
Predictors of Fear of COVID-19
A regression analysis was conducted to identify pre-pandemic person characteristics that could predict fear of COVID-19. Results of the stepwise regression analysis are shown in Table 4. A significant model was found (F(7, 350) = 13.421, p < 0.001). The model explained 19.6% of the variance in fear of COVID-19, with pre-COVID-19 anxiety emerging as the strongest predictor (8.7%), followed by pre-COVID-19 immune fitness (3.4%).
Table 4.
Stepwise regression analysis of predictors of fear of COVID-19.
4. Discussion
This study examined how fear of COVID-19 related to mood, quality of life, immune fitness, and other health variables during the first national lockdown in The Netherlands and identified its strongest predictors. Pre-pandemic anxiety and poorer immune fitness emerged as the most important predictors, together explaining 19.6% of the variance in fear of COVID-19 levels. These findings are consistent with international studies showing that individuals with pre-existing emotional vulnerabilities are more prone to heightened fear during health crises [7,10,35,36,37]. Similarly, studies from other countries have reported higher fear of COVID-19 among women, individuals with underlying medical conditions, and those with lower socioeconomic status, as well as among those with higher levels of anxiety, depression, and stress before the pandemic [15,18,21,38,39]. The observed link between poor immune fitness and greater fear is also consistent with earlier research showing that individuals who perceive their immune system as weaker tend to experience more anxiety [40].
Several other factors contributed to fear of COVID-19, including lower psychoticism, higher pre-pandemic depression, older age, greater helplessness, lower mental resilience, and higher pre-pandemic stress. The negative association with psychoticism may reflect personality traits such as reduced concern for social norms or lower emotional responsiveness, which could dampen the perceived threat of a pandemic [41]. The association with older age may be explained by repeated media emphasis on older adults as particularly vulnerable to severe COVID-19 outcomes, including hospitalization and death [42]. Finally, greater helplessness and lower resilience are likely to reduce the capacity to adapt to stressful circumstances such as a pandemic, whereas higher resilience has been shown to protect against psychological distress in other studies [43].
Although no significant group differences were observed for most alcohol-related measures, fear of COVID-19 was modest but significantly correlated with consuming fewer drinks and shorter drinking duration during the heaviest drinking occasion. This pattern may reflect more cautious behavior among individuals with greater fear of COVID-19, consistent with risk avoidance tendencies observed in other health domains [44,45].
Participants with higher fear also showed greater pain sensitivity and higher scores on all pain catastrophizing subscales (rumination, magnification, helplessness), as well as on the overall catastrophizing score. These pain-related associations have rarely been reported in the COVID-19 literature and may suggest an interaction between pain perception, cognitive–emotional appraisal, and heightened threat sensitivity during pandemics. Increased pain perception could reflect a broader psychological vulnerability profile linked to pandemic-related fear. In particular, catastrophizing, particularly helplessness, may have intensified perceived health threats and sustained fear of COVID-19. The specific context of the first Dutch lockdown, with strict restrictions, continuous media coverage, and the absence of vaccines or treatments, may have further amplified these perceptions, particularly among psychologically or physically vulnerable groups.
Prolonged fear and stress can have negative physiological consequences. Chronic activation of stress response suppresses immune function, increases vulnerability to infection, and may delay recovery [46]. Although acute stress may temporarily enhance immunity, chronic stress consistently impairs immune responses and elevates disease risk [46]. Several mechanisms may underlie these associations: individuals with high pre-existing anxiety may process health-related information in a more threatening way, amplifying perceived danger and fear responses [47]. Similarly, those who perceive their immune fitness as poorer may experience heightened psychological vulnerability, characterized by poorer mood, greater loneliness, and increased anxiety, which in turn can intensify responses to symptoms and perceived health risks.
This study has several strengths. The relatively large and diverse sample allowed for the examination of a wide range of demographic, psychological, and health-related variables. The use of validated questionnaires and the focus on the early stage of the pandemic provide a unique baseline for understanding the interplay between fear, health, and mood during a period of high uncertainty. Importantly, the inclusion of pre-pandemic measures of mood and immune fitness strengthened the ability to identify predictors rather than relying solely on concurrent associations.
However, several limitations must also be acknowledged. The cross-sectional design precludes causal inference. Next, the retrospective assessments may have introduced potential recall bias, as participants may have misremembered or idealized their pre-pandemic state. Recruitment through social media may have led to selection bias, resulting in an overrepresentation of individuals with internet access and a particular interest in health-related topics, thereby limiting generalizability. All data were self-reported, which may be affected by social desirability or subjective interpretation of health and mood. Furthermore, the study focused only on the first lockdown, and findings may not extend to later stages of the pandemic when the epidemiological situation, government measures, and risk perceptions had changed substantially. Finally, only a relatively small proportion of participants reported high levels of fear (13.2%), leading to skewed data distributions and potentially reduced statistical power for group comparisons. In the current study, motives for fear of COVID-19 were not evaluated. It can be hypothesized that fear of COVID-19 was low for the majority of participants as they regarded themselves as not belonging to groups at increased risk (e.g., elderly, those with underlying diseases). Future research should evaluate the motives for fear of COVID-19. Finally, as the study was conducted in The Netherlands, results may differ in countries with other lockdown strategies or cultural contexts.
The findings have important implications for public health policy and pandemic preparedness. They underscore the need to identify individuals with high pre-existing anxiety, low immune fitness, and elevated pain sensitivity early, as these groups are particularly vulnerable to elevated fear during pandemics. Tailored mental health support, resilience training, and evidence-based communication strategies may help reduce fear and mitigate its negative effects on mental and physical health. Public health communication should strike a balance between providing accurate risk information and avoiding unnecessary alarm, since excessive fear can worsen mental health outcomes and reduce quality of life.
Future research should examine how fear of COVID-19 and its predictors evolved across different phases of the pandemic, including subsequent lockdown periods. Comparative studies across different cultural and policy contexts may further clarify how environmental and societal factors shape fear responses. Together, these efforts can inform more targeted, timely, and effective strategies to protect population well-being in future public health crises.
5. Conclusions
During the first Dutch lockdown, fear of COVID-19 was most strongly associated with higher pre-pandemic anxiety and poorer immune fitness, with additional contributions from depression, lower resilience, stress, older age, helplessness, and psychoticism. A greater fear of COVID-19 was associated with poorer mental health, reduced quality of life, and lower immune fitness. These findings emphasize the importance of early identification of psychologically and physically vulnerable groups in future health crises, along with targeted interventions to strengthen resilience and support both mental and physical well-being.
Author Contributions
Conceptualization, P.K., P.A.H., D.M.D., A.M., M.N.Z., J.G., G.B., A.S. and J.C.V.; methodology, P.K. and J.C.V.; formal analysis, J.C.V.; writing—original draft preparation, P.K., D.M.D., P.A.H. and J.C.V.; writing—review and editing, P.K., P.A.H., D.M.D., A.M., M.N.Z., J.G., G.B., A.S. and J.C.V. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the Faculty of Social and Behavioral Sciences of Utrecht University (approval code: FETC17–061, approval date: 8 June 2017).
Informed Consent Statement
Electronic informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data are available upon reasonable request from the corresponding author.
Conflicts of Interest
Over the past 3 years, J.C.V. has received research grants from Danone and acted as a consultant/advisor for Eisai, KNMP, Med Solutions, Mozand, Red Bull, Sen-Jam Pharmaceutical, and Toast! D.M.D., A.M., M.N.Z., and J.C.V. received travel support from Sen-Jam Pharmaceutical. J.G. is a part-time employee of Nutricia Danone and received research grants from Nutricia Research Foundation, Top Institute Pharma, Top Institute Food and Nutrition, GSK, STW, NWO, Friesland Campina, CCC, Raak-Pro, and EU. A.S. has acted as a consultant/expert advisor to Bayer, Coca Cola, Danone, Delica Therapeutics, GlaxoSmithKline, Naturex, Nestlé, McCormick, Metavate Consultancy, PepsiCo, Pfizer, Pharmavite, REVIV, Sanofi, and Verdure Sciences and has held research grants from Abbott Nutrition, Arla Foods, the Australian Research Council, Bayer, DuPont, Fonterra, GlaxoSmithKline, the High Value Nutrition Fund, and the National Health and Medical Research Council, Nutricia-Danone, Sanofi. A.S. is on the Scientific Advisory Board of Sen-Jam Pharmaceutical. P.A.H., P.K., and G.B. have no potential conflicts of interest to disclose.
Abbreviations
The following abbreviations are used in this manuscript:
| COVID-19 | 2019 coronavirus disease |
| SARS-CoV-2 | Severe acute respiratory syndrome coronavirus 2 |
| CLOFIT | Corona lockdown: How fit are you? |
| BMI | Body mass index |
| BRS | Brief Resilience Scale |
| PSQ | Pain Sensitivity Questionnaire |
| PCQ | Pain Catastrophizing Scale |
| ISQ | Immune Status Questionnaire |
| BAC | Blood alcohol concentration |
References
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Docherty, A.B.; Harrison, E.M.; Green, C.A.; Hardwick, H.E.; Pius, R.; Norman, L.; Holden, K.A.; Read, J.M.; Dondelinger, F.; Carson, G.; et al. Features of 20 133 UK patients in hospital with Covid-19 using the ISARIC WHO Clinical Characterisation Protocol: Prospective observational cohort study. BMJ 2020, 369, m1985. [Google Scholar] [CrossRef]
- Ahorsu, D.K.; Lin, C.-Y.; Imani, V.; Saffari, M.; Griffiths, M.D.; Pakpour, A.H. The fear of COVID-19 scale: Development and initial validation. Int. J. Ment. Health Addict. 2022, 20, 1537–1545. [Google Scholar] [CrossRef] [PubMed]
- Dubey, S.; Biswas, P.; Ghosh, R.; Chatterjee, S.; Dubey, M.J.; Chatterjee, S.; Lahiri, D.; Lavie, C.J. Psychosocial impact of COVID-19. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 779–788. [Google Scholar] [CrossRef] [PubMed]
- Aknin, L.B.; De Neve, J.-E.; Dunn, E.W.; Fancourt, D.E.; Goldberg, E.; Helliwell, J.F.; Jones, S.P.; Karam, E.; Layard, R.; Lyubomirsky, S.; et al. Mental health during the first year of the COVID-19 pandemic: A review and recommendations for moving forward. Perspect. Psychol. Sci. 2022, 17, 915–936. [Google Scholar] [CrossRef]
- Şimşir, Z.; Koç, H.; Seki, T.; Griffiths, M.D. The relationship between fear of COVID-19 and mental health problems: A meta-analysis. Death Stud. 2022, 46, 515–523. [Google Scholar] [CrossRef]
- Alimoradi, Z.; Ohayon, M.M.; Griffiths, M.D.; Lin, C.-Y.; Pakpour, A.H. Fear of COVID-19 and its association with mental health-related factors: Systematic review and meta-analysis. BJPsych Open 2022, 8, e73. [Google Scholar] [CrossRef]
- Callaway, E.; Ledford, H. How bad is Omicron? What scientists know so far. Nature 2021, 600, 197–199. [Google Scholar] [CrossRef]
- Çıkrıkçı, Ö.; Çıkrıkçı, N.; Griffiths, M. Fear of COVID-19, stress and depression: A meta-analytic test of the mediating role of anxiety. Psychol. Psychother. 2022, 95, 853–874. [Google Scholar] [CrossRef]
- Chenchula, S.; Karunakaran, P.; Sharma, S.; Chavan, M. Current evidence on efficacy of COVID-19 booster dose vaccination against the Omicron variant: A systematic review. J. Med. Virol. 2022, 94, 2969–2976. [Google Scholar] [CrossRef]
- Autenrieth, L.K.; Asselmann, E.; Melzig, C.A.; Benke, C. Fear of COVID-19 predicts increases in anxiety, depressive symptoms, health anxiety, psychosocial distress, and loneliness: Findings from a prospective two-year follow-up study. J. Psychiatr. Res. 2024, 177, 162–168. [Google Scholar] [CrossRef]
- Luo, F.; Ghanei Gheshlagh, R.; Dalvand, S.; Saedmoucheshi, S.; Li, Q. Systematic review and meta-analysis of fear of COVID-19. Front. Psychol. 2021, 12, 661078. [Google Scholar] [CrossRef] [PubMed]
- Dragioti, E.; Li, H.; Tsitsas, G.; Lee, K.H.; Choi, J.; Kim, J.; Choi, Y.J.; Tsamakis, K.; Estradé, A.; Agorastos, A.; et al. A large-scale meta-analytic atlas of mental health problems prevalence during the COVID-19 early pandemic. J. Med. Virol. 2022, 94, 1935–1949. [Google Scholar] [CrossRef] [PubMed]
- Panchal, U.; Salazar De Pablo, G.; Franco, M.; Moreno, C.; Parellada, M.; Arango, C.; Fusar-Poli, P. The impact of COVID-19 lockdown on child and adolescent mental health: Systematic review. Eur. Child. Adolesc. Psychiatry 2023, 32, 1151–1177. [Google Scholar] [CrossRef] [PubMed]
- Hendriksen, P.A.; Garssen, J.; Bijlsma, E.Y.; Engels, F.; Bruce, G.; Verster, J.C. COVID-19 lockdown-related changes in mood, health and academic functioning. Eur. J. Investig. Health Psychol. Educ. 2021, 11, 1440–1461. [Google Scholar] [CrossRef]
- Lazary, J. Acute effects of the first period of COVID-19 pandemic on mental state. Neuropsychopharmacol. Hung. 2020, 22, 172–177. [Google Scholar]
- Filindassi, V.; Pedrini, C.; Sabadini, C.; Duradoni, M.; Guazzini, A. Impact of COVID-19 first wave on psychological and psychosocial dimensions: A systematic review. COVID 2022, 2, 273–340. [Google Scholar] [CrossRef]
- Prati, G.; Mancini, A.D. The psychological impact of COVID-19 pandemic lockdowns: A review and meta-analysis of longitudinal studies and natural experiments. Psychol. Med. 2021, 51, 201–211. [Google Scholar] [CrossRef]
- Erbiçer, E.S.; Metin, A.; Çetinkaya, A.; Şen, S. The relationship between fear of COVID-19 and depression, anxiety, and stress. Eur. Psychol. 2022, 26, 323–333. [Google Scholar] [CrossRef]
- Quadros, S.; Garg, S.; Ranjan, R.; Vijayasarathi, G.; Mamun, M.A. Fear of COVID 19 infection across different cohorts: A scoping review. Front. Psychiatry 2021, 12, 708430. [Google Scholar] [CrossRef] [PubMed]
- Erbiçer, E.S.; Metin, A.; Şen, S. COVID-19 Related fear and anxiety: A systematic review and meta-analysis. Humanist. Perspect. 2025, 7, 165–182. [Google Scholar] [CrossRef]
- Rijksoverheid. Coronavirus COVID-19. Available online: https://www.rijksoverheid.nl/onderwerpen/coronavirus-covid-19 (accessed on 25 January 2021).
- Kiani, P.; Merlo, A.; Saeed, H.M.; Benson, S.; Bruce, G.; Hoorn, R.; Kraneveld, A.D.; Van De Loo, A.J.A.E.; Severeijns, N.R.; Sips, A.S.M.; et al. Immune fitness, and the psychosocial and health consequences of the COVID-19 pandemic lockdown in The Netherlands: Methodology and design of the CLOFIT study. Eur. J. Investig. Health Psychol. Educ. 2021, 11, 199–218. [Google Scholar] [CrossRef] [PubMed]
- Quetelet, M.A. A Treatise on Man and the Development of His Faculties; William and Robert Chambers: Edinburgh, UK, 1842. [Google Scholar]
- Smith, B.W.; Wiggins, K.; Dalen, J.; Bernard, J. Brief Resilience Scale: Assessing the ability to bounce back. Int. J. Behav. Med. 2008, 15, 194–200. [Google Scholar] [CrossRef]
- Sanderman, R.; Eysenck, S.B.G.; Arrindell, W.A. Crosscultural comparison of personality traits: The Netherlands and England. Psychol. Rep. 1991, 69, 1091–1096. [Google Scholar] [CrossRef]
- Sanderman, R.; Arrindell, W.A.; Ranchor, A.V.; Eysenck, H.J.; Eysenck, S.B.G. Het Meten van Persoonlijkheidskenmerken Met de Eysenck Personality Questionnaire (EPQ), Een Handleiding. Tweede Herziene Druk; UMCG/Rijksuniversiteit Groningen, Research Institute SHARE: Groningen, The Netherlands, 2012. [Google Scholar]
- Ruscheweyh, R.; Marziniak, M.; Stumpenhorst, F.; Reinholz, J.; Knecht, S. Pain sensitivity can be assessed by self-rating: Development and validation of the pain sensitivity questionnaire. Pain 2009, 146, 65–74. [Google Scholar] [CrossRef]
- Darnall, B.D.; Sturgeon, J.A.; Cook, K.F.; Taub, C.J.; Roy, A.; Burns, J.W.; Sullivan, M.; Mackey, S.C. Development and validation of a daily pain catastrophizing scale. J. Pain 2017, 18, 1139–1149. [Google Scholar] [CrossRef]
- Verster, J.C.; Sandalova, E.; Garssen, J.; Bruce, G. The use of single-item ratings versus traditional multiple-item questionnaires to assess mood and health. Eur. J. Investig. Health Psychol. Educ. 2021, 11, 183–198. [Google Scholar] [CrossRef]
- Verster, J.C.; Išerić, E.; Ulijn, G.A.; Oskam, S.M.P.; Garssen, J. Single-item assessment of quality of life: Associations with well-being, mood, health correlates, and lifestyle. J. Clin. Med. 2024, 13, 5217. [Google Scholar] [CrossRef]
- Verster, J.C.; Kraneveld, A.D.; Garssen, J. The assessment of immune fitness. J. Clin. Med. 2022, 12, 22. [Google Scholar] [CrossRef]
- Wilod Versprille, L.J.F.; Van De Loo, A.J.A.E.; Mackus, M.; Arnoldy, L.; Sulzer, T.A.L.; Vermeulen, S.; Abdulahad, S.; Huls, H.; Baars, T.; Scholey, A.; et al. Development and validation of the Immune Status Questionnaire (ISQ). Int. J. Environ. Res. Public Health 2019, 16, 4743. [Google Scholar] [CrossRef]
- Coelho, C.M.; Suttiwan, P.; Arato, N.; Zsido, A.N. On the nature of fear and anxiety triggered by COVID-19. Front. Psychol. 2020, 11, 581314. [Google Scholar] [CrossRef]
- Murphy, L.; Markey, K.; O’Donnell, C.; Moloney, M.; Doody, O. The impact of the COVID-19 pandemic and its related restrictions on people with pre-existent mental health conditions: A scoping review. Arch. Psychiat. Nurs. 2021, 35, 375–394. [Google Scholar] [CrossRef] [PubMed]
- Leung, C.M.C.; Ho, M.K.; Bharwani, A.A.; Cogo-Moreira, H.; Wang, Y.; Chow, M.S.C.; Fan, X.; Galea, S.; Leung, G.M.; Ni, M.Y. Mental disorders following COVID-19 and other epidemics: A systematic review and meta-analysis. Transl. Psychiatry 2022, 12, 205. [Google Scholar] [CrossRef] [PubMed]
- Asmundson, G.J.G.; Paluszek, M.M.; Landry, C.A.; Rachor, G.S.; McKay, D.; Taylor, S. Do pre-existing anxiety-related and mood disorders differentially impact COVID-19 stress responses and coping? J. Anxiety Disord. 2020, 74, 102271. [Google Scholar] [CrossRef]
- Jarego, M.; Ferreira-Valente, A.; Sánchez-Rodríguez, E.; Miró, J.; Costa, P.; Pais-Ribeiro, J. Socioeconomic status, social support, coping, and fear predict mental health status during the first year of the COVID-19 pandemic: A 1-year longitudinal study. Curr. Psychol. 2024, 43, 35672–35685. [Google Scholar] [CrossRef]
- Kiani, P.; Hendriksen, P.A.; Balikji, J.; Severeijns, N.R.; Sips, A.S.M.; Bruce, G.; Garssen, J.; Verster, J.C. COVID-19 lockdown effects on mood: Impact of sex, age, and underlying disease. Psychiatry Int. 2023, 4, 307–323. [Google Scholar] [CrossRef]
- Kampe, L.; Hörz-Sagstetter, S.; Bohn, J.; Remmers, C. How personality functioning relates to psychological distress and behavioral attitudes during the Covid-19 pandemic. Eur. Arch. Psychiatry Clin. Neurosci. 2025, 275, 167–180. [Google Scholar] [CrossRef]
- Zhu, C.; Zhang, T.; Li, Q.; Chen, X.; Wang, K. Depression and anxiety during the COVID-19 pandemic: Epidemiology, mechanism, and treatment. Neurosci. Bull. 2023, 39, 675–684. [Google Scholar] [CrossRef]
- Sugawara, D.; Gu, Y.; Masuyama, A.; Ng, S.L.; Phoo, E.Y.M.; Raja Reza Shah, R.I.A.B.; Kubo, T.; Chishima, Y.; Tee, E.Y.J. RE-COVER project: A survey on resilience, mental health, and fear of Covid-19 in four countries. BMC Res. Notes 2021, 14, 409. [Google Scholar] [CrossRef]
- Haucke, M.; Heinz, A.; Heinzel, S.; Liu, S. Investigating the impact of COVID-19 related worries and loneliness on alcohol consumption: An ecological momentary assessment. Eur. Arch. Psychiat. Clin. Neurosci. 2024. ahead of print. [Google Scholar] [CrossRef]
- Rodriguez, L.M.; Litt, D.M.; Stewart, S.H. Drinking to cope with the pandemic: The unique associations of COVID-19-related perceived threat and psychological distress to drinking behaviors in American men and women. Addict. Behav. 2020, 110, 106532. [Google Scholar] [CrossRef]
- Balakin, E.; Yurku, K.; Ivanov, M.; Izotov, A.; Nakhod, V.; Pustovoyt, V. Regulation of stress-induced immunosuppression in the context of neuroendocrine. Cytokine, and Cellular Processes. Biology 2025, 14, 76. [Google Scholar] [CrossRef]
- Jessup, S.C.; Knowles, K.A.; Olatunji, B.O. Linking the estimation of threat and COVID-19 fear and safety behavior use: Does intolerance of uncertainty matter? Int. J. Cogn. Ther. 2022, 15, 479–491. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).