
The Disappearance of COVID-19 Data Dashboards: The Case of Ephemeral Data


Abstract
1. Introduction
1.1. Pandemic Maps to Web Maps on Data Dashboards
1.2. COVID-19 Data Dashboards and Web Maps
2. Methods: Ephemeral Data—Status of COVID-19 Data Dashboards
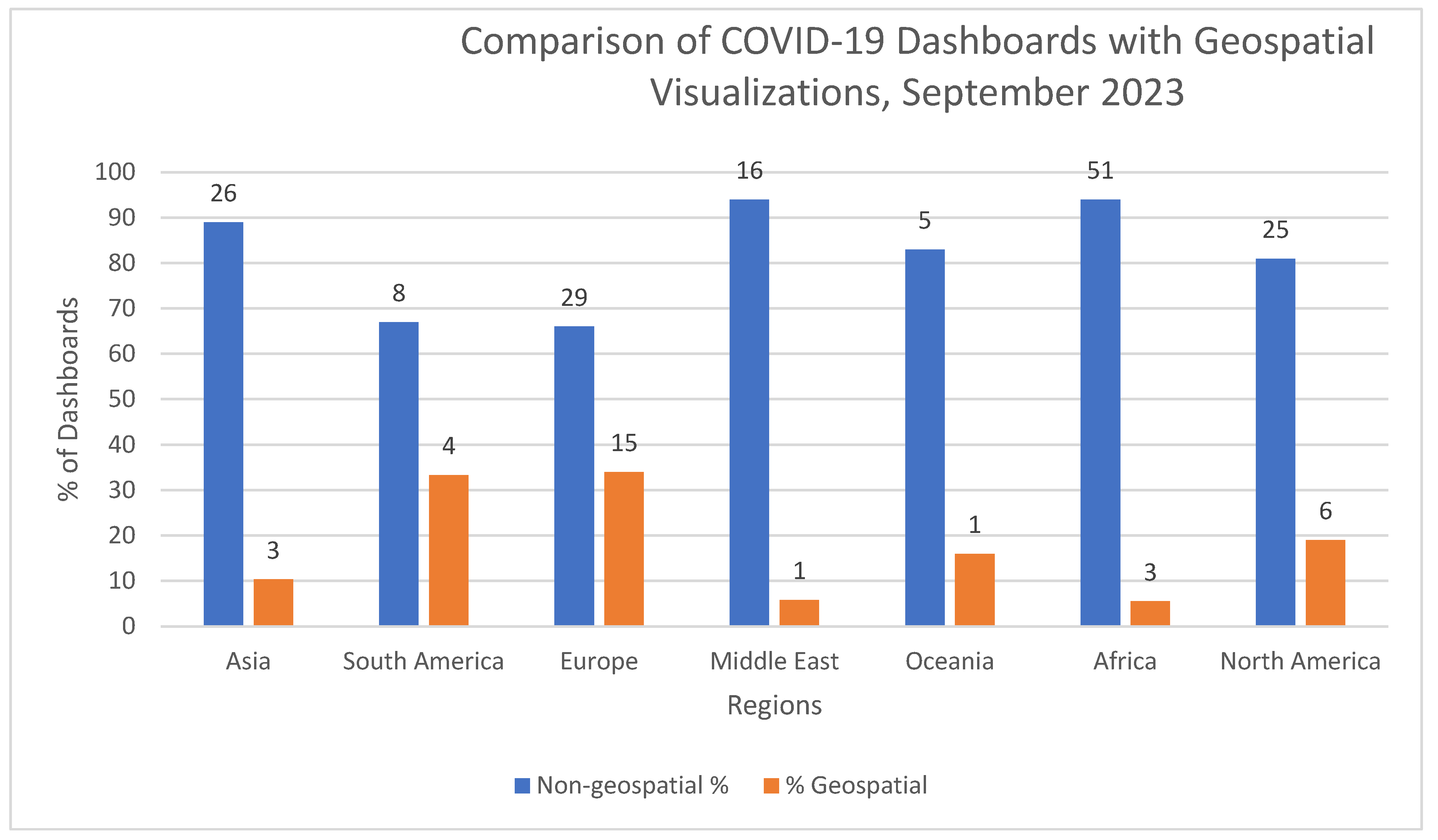
3. Results—Geospatial COVID-19 Data Dashboards
4. Discussion: Lessons Learned
4.1. Scale and Resolution
4.2. Boundaries
4.3. Metrics
4.4. Data Quality
4.5. Data Maintenance
5. Conclusions
- Know the audience: dashboards need functionality to meet the user needs and requirements of multilanguage settings of users.
- Data: Explanation of what and how data are collected from authoritative sources. If data are collected, collection methods are clearly described. The purpose and limitations of the data are described.
- Concise # of indicators: Targeted number of indicators are selected to enable viewing information at a glance. The rationale and purpose of specific indicators are defined.
- Data accessibility for downloading, analysis, archiving, and storage are described.
- Analysis: methods and instructions to analyze data and track trends with demonstrations are provided.
- Visualizations: Description of metadata that includes geographic scale/resolution. Use of intuitive color scheme, icons, and symbology.
- Time: description of updating schedule of data.
- Story telling: provide narratives that highlight key findings.
- Construction: dashboard construction that is easy to use with limited coding and low cost.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Interlandi, J. The Pandemic Weather Service: Inside the C.D.C.’s Ambitious New Plan to Predict Future Outbreaks. The New York Times Magazine, 18 November 2021; 38–39, 62–63. [Google Scholar]
- Crisan, A. The importance of data visualization in combating a pandemic. Am. J. Public Health 2022, 112, 893–895. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Statement on the 15th Meeting of International Health Regulations. 5 May 2023. Available online: https://www.who.int/news/item/05-05-2023-statement-on-the-fifteenth-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-coronavirus-disease-(covid-19)-pandemic#:~:text=The%20WHO%20Director%2DGeneral%20concurs,of%20international%20concern%20(PHEIC) (accessed on 18 September 2024).
- PBS. WHO Downgrades COVID-19 Pandemic. 5 May 2023. Available online: https://www.pbs.org/newshour/health/who-downgrades-covid-19-pandemic-says-its-no-longer-global-emergency (accessed on 13 January 2025).
- Cohen, J. COVID-19 is surging again—With far fewer serious cases. Science 2024, 385, 814–815. [Google Scholar] [CrossRef] [PubMed]
- Lyseen, A.; Nohr, C.; Sorensen, E.; Gudes, O.; Geraghty, E.; Shaw, N.; Bivona-Tellez, C. A review and framework for categorizing current research and development in health related geographical information systems (GIS) studies. IMIA Yearb. Med. Inform. 2014, 23, 110–124. [Google Scholar] [CrossRef]
- Zhao, B.; Kim, M.; Nam, E. Information disclosure contents of the COVID-19 data dashboards websites for South Korea, China, and Japan: A comparative study. Healthcare 2021, 9, 1487. [Google Scholar] [CrossRef]
- Nijkamp, P.; Kourtit, K. Place-specific Corona dashboards for health policy: Design and application of a ‘Dutchboard’. Sustainability 2022, 14, 836. [Google Scholar] [CrossRef]
- Clarkson, M. Web-based COVID-19 dashboards and trackers in the United States: Survey study. JMIR Hum. Factors 2023, 10, e43819. [Google Scholar] [CrossRef]
- Few, S. Dashboard Confusion. Perceptual Edge. 2004. Available online: https://www.perceptualedge.com/articles/ie/dashboard_confusion.pdf (accessed on 13 January 2025).
- Neumann, A. Web mapping and web cartography. In Encyclopedia of GIS; Shekhar, S., Xiong, H., Eds.; Springer: Boston, MA, USA, 2008. [Google Scholar] [CrossRef]
- Snowden, F. Epidemics and Society: From the Black Death to the Present; Yale University Press: New Haven, CT, USA, 2020. [Google Scholar]
- Centers for Disease Control (CDC). Definitions. 15 May 2024. Available online: https://www.cdc.gov/reproductive-health/glossary/?CDC_AAref_Val=https://www.cdc.gov/reproductivehealth/data_stats/glossary.html#cdc_generic_section_4-e (accessed on 6 September 2024).
- World Health Organization (WHO). Definitions. 19 February 2021. Available online: https://www.publichealth.columbia.edu/news/epidemic-endemic-pandemic-what-are-differences#:~:text=It's%20important%20to%20note%20that,international%20and%20out%20of%20control (accessed on 6 September 2024).
- Gould, P. The Slow Plague: A Geography of the AIDS Pandemic; Blackwell Press: Oxford, UK, 1993. [Google Scholar]
- Engelmann, L. Mapping AIDS: Visual Histories of an Enduring Epidemic (Global Health Histories), 1st ed.; Cambridge University Press: Cambridge, UK, 2018. [Google Scholar]
- Centers for Disease Control (CDC). Ebola—Outbreak History. 6 May 2024. Available online: https://www.cdc.gov/ebola/outbreaks/index.html (accessed on 28 September 2024).
- Saurabh, S.; Prateek, S. Role of contact tracing in containing the 2014 Ebola outbreak: A review. Afr. Health Sci. 2017, 17, 225–236. [Google Scholar] [CrossRef]
- Pigott, D.; Golding, N.; Mylne, A.; Huang, Z.; Henry, A.; Weiss, D.; Brady, O.; Kraemer, M.; Smith, D.; Moyes, C.; et al. Mapping the zoonotic niche of Ebola virus disease in Africa. eLife 2014, 3, e04395. [Google Scholar] [CrossRef]
- Sills, J. Ebola: Mobility data. Science 2014, 346, 433. [Google Scholar]
- Victory, K.; Coronado, F.; Ifono, S.; Soropogui, T.; Dahl, B. Ebola Transmission Linked to a Single Traditional Funeral Ceremony—Kissdougou, Guinea, December 2014–January 2015. In Morbidity and Mortality Weekly Report (MMWR); Centers for Disease Control and Prevention: Atlanta, GA, USA, 2015. [Google Scholar]
- Cohen, J.; Tsanni, A. Pulling back the curtain. Science 2024, 385, 818–823. [Google Scholar] [CrossRef]
- Vahedi, A.; Moghaddasi, H.; Asadi, F.; Hosseini, A.; Nazemi, E. Applications, features, and key indicators for the development of COVID-19 dashboards: A systematic review study. Inform. Med. Unlocked 2022, 30, 100910. [Google Scholar] [CrossRef] [PubMed]
- Schulze, A.; Brand, F.; Geppert, J.; Bol, G. Digital dashboards visualizing public health data: A systematic review. Front. Public Health 2023, 11, 999958. [Google Scholar] [CrossRef] [PubMed]
- Everts, J. The dashboard pandemic. Dialogues Hum. Geogr. 2020, 10, 260–264. [Google Scholar] [CrossRef]
- Praharaj, S.; Solis, P.; Wentz, E. Deploying geospatial visualization dashboards to combat the socioeconomic impacts of COVID-19. Urban Anal. City Sci. 2022, 50, 1262–1279. [Google Scholar] [CrossRef]
- Samany, N.; Liu, H.; Aghataher, R.; Bayat, M. Ten GIS-based solutions for managing and controlling COVID-19 pandemic outbreak. SN Comput. Sci. 2022, 3, 269. [Google Scholar] [CrossRef]
- Dangermond, J.; De Vito, C.; Pesaresi, C. Using GIS in the time of COVID-19 crisis, casting a glance at the future. A joint discussion. J. Res. Didat. Geogr. 2020, 1, 195–205. [Google Scholar]
- Rosenkrantz, L.; Schuurman, N.; Bell, N.; Amram, O. The need for GIScience in mapping COVID-19. Health Place 2021, 67, 102389. [Google Scholar] [CrossRef]
- Dixon, B.; Dearth, S.; Duszynski, T.; Grannis, S. Dashboards are trendy, visible components of data management in public health: Sustaining their use after the pandemic requires a broader view. Am. J. Public Health 2022, 112, 900903. [Google Scholar] [CrossRef]
- Berry, I.; Soucy, J.; Tuite, A.; Fisman, D. Open access epidemiological data and an interactive dashboard to monitor the COVID-19 outbreak in Canada. CMAJ 2020, 192, 15. [Google Scholar] [CrossRef]
- Gleeson, J.; Kitchin, R.; McCarthy, E. Dashboards and public health: The development, impacts, and lessons from the Irish Government COVID-19 dashboards. Am. J. Public Health 2022, 112, 809–944. [Google Scholar] [CrossRef]
- Khodaveisi, T.; Dhedarirad, H.; Bouraghi, H.; Mohammadpout, A.; Sajadi, F.; Hosseiniravandi, M. Characteristics and specifications of dashboards developed for the COVID-19 pandemic: A scoping review. J. Public Health 2024, 35, 553–574. [Google Scholar] [CrossRef] [PubMed]
- Boulos, M.; Geraghty, E. Geographical tracking and mapping of coronavirus disease COVID-19/severe respiratory syndrome coronavirus 2 (SARS-CoV-2) epidemic and associated events around the world: How 21st century GIS technologies are supporting the global fight against outbreaks and epidemics. Int. J. Health Geogr. 2020, 19, 8. [Google Scholar] [CrossRef]
- Ivankovic, D.; Barbazza, E.; Box, V.; Fernandes, O.; Gilmore, K.; Jansen, T.; Kara, P.; Larrain, N.; Lu, S.; Meza-Torres, B.; et al. Features Constituting Actionable COVID-19 Dashboards: Descriptive Assessment and Expert Appraisal of 158 Public Web-Based COVID-19 Dashboards. J. Med. Internal. Res. 2021, 23, e25682. [Google Scholar] [CrossRef] [PubMed]
- Bernasconi, A.; Grandi, S. A conceptual model for geo-online exploratory data visualization: The case of the COVID-19 pandemic. Information 2021, 12, 69. [Google Scholar] [CrossRef]
- Dong, E.; Ratcliff, J.; Goyea, T.; Katz, A.; Lau, R.; Ng, T.; Garcia, B.; Bolt, E.; Prata, S.; Zhang, D.; et al. The Johns Hopkins University center for systems science and engineering COVID-19 dashboard: Data collection process, challenges faced, and lessons learned. Personal View. Lancet 2022, 22, e360–e376. [Google Scholar] [CrossRef]
- UN-SALB (United Nations Second Administrative Level Boundaries). Available online: https://salb.un.org/en (accessed on 13 January 2025).
- Sha, D.; Liu, Y.; Liu, Q.; Li, Y.; Tian, Y.; Beaini, F.; Zhong, C.; Hu, T.; Wang, Z.; Lan, H.; et al. A spatial temporal data collection of viral cases for COVID-19 rapid response. Big Earth Data 2021, 5, 90–111. [Google Scholar] [CrossRef]
- Bakari, O.; Zando, M.; Blaser, M. Opinion: COVID-19 Lesson—Local Data Skills Matter. DevEx News. 14 January 2021. Available online: https://www.devex.com/news/sponsored/opinion-covid-19-lesson-local-data-skills-matter-98910 (accessed on 13 January 2025).
- Carballada, A.; Balsa-Barreiro, J. Geospatial analysis and mapping strategies for fine-grained and detailed COVID-19 data with GIS. Int. J. Geo-Inf. 2021, 10, 602. [Google Scholar] [CrossRef]
- Laituri, M.; Richardson, R.; Kim, J. (Eds.) The Geographies of COVID-19: Geospatial Stories of a Global Pandemic; Springer Nature: Cham, Switzerland, 2022. [Google Scholar]
- Marvel, S.; House, J.; Wheeler, M.; Song, K.; Zhou, Y.; Wright, F.; Chiu, W.; Rusyn, I.; Motsinger-Reif, A.; Reif, D. The COVID-19 pandemic vulnerability index (PVI) dashboard: Monitoring county-level vulnerability using visualization, statistical modeling, and machine learning. Environ. Health Perspect. 2021, 129, 17701. [Google Scholar] [CrossRef]
- Mbonglou, G.; John, R. Data and Dashboards for Measuring the social impact of COVID-19 in African Cities. In The Geographies of COVID-19: Geospatial Stories of a Global Pandemic; Laituri, M., Richardson, R., Kim, J., Eds.; Springer Nature: Cham, Switzerland, 2022. [Google Scholar]
- Yang, C.P.; Bao, S.; Guan, W.; Howell, K.; Hu, T.; Lan, H.; Li, Y.; Liu, Q.; Smith, J.; Srirenganathan, A.; et al. Challenges and Opportunities of the spatiotemporal responses to the global pandemic of COVID-19. Ann. GIS 2022, 28, 425–434. [Google Scholar] [CrossRef]
- Hu, T.; Guan, W.; Zhu, X.; Shao, Y.; Liu, L.; Du, J.; Liu, H.; Zhou, H.; Wang, J.; Sha, B.; et al. Building an open resources repository for COVID-19 research. Data Inf. Manag. 2020, 4, 130–147. [Google Scholar] [CrossRef]
- Yang, C.; Sha, D.; Liu, Q.; Li, Y.; Lan, H.; Guan, W.; Hu, T.; Li, Z.; Zhang, Z.; Thompson, J.; et al. Taking the pulse of COVID-19: A spatiotemporal perspective. Int. J. Digit. Earth 2020, 13, 1186–1211. [Google Scholar] [CrossRef]
- Agafonkin, V. Reimaging Projections for the Interactive Maps Era. MapBox Blog. 9 December 2021. Available online: https://www.mapbox.com/blog/adaptive-projections (accessed on 28 September 2024).
- Yusni, A. Coronovirus: Why Testing and Contact Tracing Isn’t a Simple Solution. The Conversation. 2020. Available online: https://theconversation.com/coronavirus-why-testing-and-contact-tracing-isnt-a-simple-solution-137214 (accessed on 13 January 2025).
- Farr, C. The COVID-19 Response Must Balance Civil Liberties and Public Health—Experts Explain How. CNBC–Tech. 2020. Available online: https://www.cnbc.com/2020/04/18/covid-19-response-vs-civil-liberties-striking-the-right-balance.html (accessed on 13 January 2025).
- Tsai, J.; Khazanchi, R.; Laflamme, E. Death by Missing Data: Uncollected Racial and Ethnic Pandemic Data Will Drive Inequities for Decades to Come. STAT News. 30 January 2023. Available online: https://www.statnews.com/2023/01/30/covid-19-missing-data-race-ethnicity-drive-inequities-decades-to-come/#:~:text=In%20a%20national%20dataset%20of,That's%2034%25%20of%20cases (accessed on 13 January 2025).
- Muhareb, R.; Giacaman, R. Tracking COVID-19 Responsibly. In Lancet; 26 May 2020. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7194718/ (accessed on 13 January 2025).
- Kennedy, H. Impact of Social Sciences Blog: Simple Data Visualisations Have Become Key to Communicating About the COVID-19 Pandemic, but We Know Little About Their Impact. Impact of Social Sciences Blog. 4 May 2020. Available online: https://blogs.lse.ac.uk/impactofsocialsciences/ (accessed on 13 January 2025).
- Rettner, R. Why Are Deaths from Coronavirus So High in Italy? LiveScience. 27 March 2020. Available online: https://www.livescience.com/why-italy-coronavirus-deaths-so-high.html (accessed on 13 January 2025).
- Koch, T. 1831: The map that launched the idea of global health. Int. J. Epidemiol. 2014, 43, 1014–1020. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, N.; Marriott, A.; Dabi, N.; Lowthers, M.; Lawson, M.; Mugehera, L. Inequity Kills; Oxfam International: Oxford, UK, 2022. [Google Scholar]
- Gawande, A. The aftermath of a pandemic requires as much focus as the start. NY Times, 16 March 2023. [Google Scholar]
- Phelan, A.; Carlson, C. A treaty to break the pandemic cycle. Science 2022, 377, 475–477. [Google Scholar] [CrossRef] [PubMed]
- Offit, P. For the Next Pandemic; National Geographic: Washington, DC, USA, 2024; pp. 17–20. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors | Topic |
|---|---|
| Crisan (2022) [2] | General discussion of visualization, use of real time data, no specifics on maps |
| Everts (2020) [25] | Scale limitations of pandemic data; lack of mapping and representation of risk groups such vulnerable populations (i.e., poor, ethnic groups) |
| Samany et al. (2022) [27] | GIS-based tools and services to track and monitor COVID-19 pandemic; discussion of web map but does address issues related to spatial scale (i.e., local data) |
| Dangermond et al. (2020) [28] | GIS dashboards for data dissemination; cloud-based services to deliver GIS products; issues of privacy and spatial data scale/granularity |
| Rosenkrantz et al. (2021) [29] | Need for more granular-scale data and complex databases to address multiple social, economic, and health care issues |
| Dixon et al. (2022) [30] | Long-term sustainability of data dashboards for public health; need for technically trained workforce to utilize GIS technology |
| Authors | Location | Topic |
|---|---|---|
| Zhao et al. (2021) [7] | Republic of Korea, China, Japan | Comparative study of data dashboards; only Japan dashboard included maps |
| Nikjamp and Kourtit (2022) [8] | The Netherlands | Discussion of regional and local-level data; local data are defined as the municipality |
| Clarkson (2023) [9] | USA | U.S. COVID-19 web-based dashboards and trackers |
| Berry et al. (2020) [31] | Canada | Monitoring of COVID-19 outbreak by province/territory |
| Gleeson et al. (2022) [32] | Ireland | Development and impacts of COVID-19 dashboards; Ireland map with counties |
| Khodaveisi et al. (2024) [33] | Multiple countries (26) | Granularity of COVID-19 data for dashboards; no specific discussion of maps on dashboards |
| Authors | # Reviewed | Timeframe | Topic |
|---|---|---|---|
| Boulos and Geraghty (2020) [34] | 6 dashboards | 2020 | Geographical tracking and mapping of COVID-19; GIS technologies |
| Ivankovic et al. (2021) [35] | 158 dashboards | July 2020 | Actionable COVID-19 dashboards |
| Bernasconi and Grandi (2021) [36] | 121 dashboards | 20 February–3 May 2020 | COVID-19 geo-dashboards |
| Praharaj et al. (2022) [26] | 68 dashboards | 2020–2021 | Public web-based dashboards of COVID-19 |
| Vahedi et al. (2022) [23] | 19 articles | 2020–2021 | Interactive dashboard articles on key performance indicators for COVID-19 |
| Schultze et al. (2023) [24] | 65 articles (35 articles on COVID-19) | 2010–2020 | Literature review on public health issues addressed by dashboards |
| Clarkson (2023) [9] Khodaveisi et al. (2024) [33] | 128 dashboards 26 articles (place-specific data dashboards) | August 2020–June 2022 August 2021 | COVID-19 web-based dashboards and trackers in the U.S. Granularity of data and data processing of COVID-19 indicators |
| Count and Percentage of Data Dashboards by Region—Historic, Accessible, Operating, and Geospatial (September 2023) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Region | Total Countries | Historic a (Count/%) | Accessible b (Count/%) | Operating c (Count/%) | Geospatial d (Count/%) | ||||
| Asia | 29 | 12 | 41.38 | 18 | 62.07 | 9 | 31.03 | 3 | 10.34 |
| South America | 14 | 8 | 57.14 | 8 | 57.14 | 4 | 28.57 | 5 | 35.71 |
| Europe | 44 | 24 | 54.55 | 28 | 63.64 | 16 | 36.36 | 15 | 34.09 |
| Middle East | 17 | 7 | 41.18 | 7 | 41.18 | 2 | 11.76 | 2 | 11.76 |
| Oceania | 6 | 6 | 100 | 6 | 100 | 2 | 33.33 | 1 | 16.67 |
| Africa | 54 | 18 | 33.33 | 21 | 38.80 | 9 | 16.67 | 7 | 12.96 |
| North/Central America | 31 | 13 | 41.94 | 16 | 51.61 | 6 | 19.35 | 6 | 19.35 |
| Total | 195 | 88 | 45.13 | 104 | 53.3 | 48 | 24.62 | 39 | 20 |
| Count and Percentage of Data Dashboards by Region—Accessible and Operating (June 2024) | |||||
|---|---|---|---|---|---|
| Region | Total Countries | Accessible * (Count/%) | Operating * (Count/%) | ||
| Asia | 29 | 9 | 31.03 | 3 | 10.34 |
| South America | 14 | 7 | 50 | 1 | 7.14 |
| Europe | 44 | 26 | 50.09 | 8 | 18.18 |
| Middle East | 17 | 6 | 35.29 | 1 | 5.88 |
| Oceania | 6 | 5 | 83.33 | 2 | 33.33 |
| Africa | 54 | 10 | 33.33 | 4 | 7.41 |
| North/Central America | 31 | 14 | 45.16 | 4 | 11.79 |
| Total | 195 | 77 | −13.85 | 23 | −12.82 |
| Count By Region—Type (June 2024) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Region | Total Countries | Functioning a (Count/%) | Functioning, NLU b (Count/%) | Broken Link c (Count/%) | Redirect d (Count/%) | Page Deleted e (Count/%) | Not Loading f (Count/%) | ||||||
| Asia | 29 | 3 | 10.34 | 6 | 20.69 | 11 | 37.93 | 7 | 24.14 | 2 | 6.9 | 0 | 0 |
| South America | 14 | 1 | 7.14 | 6 | 42.86 | 5 | 35.71 | 1 | 7.14 | 1 | 7.14 | 0 | 0 |
| Europe | 44 | 8 | 18.18 | 18 | 40.91 | 8 | 18.18 | 4 | 9.09 | 6 | 13.64 | 0 | 0 |
| Middle East | 17 | 1 | 5.88 | 5 | 29.41 | 5 | 29.41 | 5 | 29.41 | 1 | 5.88 | 0 | 0 |
| Oceania | 6 | 2 | 33.33 | 3 | 50 | 0 | 0 | 0 | 0 | 1 | 16.67 | 0 | 0 |
| Africa | 54 | 4 | 7.41 | 6 | 11.11 | 9 | 16.67 | 25 | 46.3 | 7 | 12.96 | 3 | 5.56 |
| North/Central America | 31 | 5 | 16.13 | 9 | 29.03 | 3 | 9.68 | 8 | 25.81 | 6 | 19.35 | 0 | 0 |
| Total | 195 | 24 | 12.31 | 53 | 27.18 | 41 | 21.3 | 50 | 25.64 | 24 | 12.31 | 3 | 1.54 |
| Repository | Description | Internet Address | Topic |
|---|---|---|---|
| GitHub | Sha et al. (2021) [39] | https://github.com/stccenter/COVID-19-Data (accessed 13 January 2025) | Spatiotemporal data collection of viral cases for COVID-19 rapid response. |
| Harvard Dataverse | Hu et al. (2020) [46] | https://dataverse.harvard.edu/dataverse/covid19 (accessed 13 January 2025) | Open resource repository for COVID-19 research. |
| HDX | COVID-19 pandemic datasets (81) from organizations and government health agencies; 7 archived datasets. Link to data dashboard if available; ArcGIS online interactive maps if dashboard is still accessible. | https://data.humdata.org/dataset (accessed 13 January 2025) | Repository of COVID-19 datasets that include subnational data of COVID-19 cases and deaths. Access to health services with an option to view interactive maps using ArcGIS online if available. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laituri, M.; Kalra, Y.; Yang, C. The Disappearance of COVID-19 Data Dashboards: The Case of Ephemeral Data. COVID 2025, 5, 12. https://doi.org/10.3390/covid5010012
Laituri M, Kalra Y, Yang C. The Disappearance of COVID-19 Data Dashboards: The Case of Ephemeral Data. COVID. 2025; 5(1):12. https://doi.org/10.3390/covid5010012
Chicago/Turabian StyleLaituri, Melinda, Yogya Kalra, and Chaowei Yang. 2025. "The Disappearance of COVID-19 Data Dashboards: The Case of Ephemeral Data" COVID 5, no. 1: 12. https://doi.org/10.3390/covid5010012
APA StyleLaituri, M., Kalra, Y., & Yang, C. (2025). The Disappearance of COVID-19 Data Dashboards: The Case of Ephemeral Data. COVID, 5(1), 12. https://doi.org/10.3390/covid5010012