
The Effect of Movement Control Order for Various Population Mobility Phases during COVID-19 in Malaysia

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Data Sources
2.2. Population Mobility
2.3. Descriptive Analysis
2.4. Comparative Analysis
2.4.1. Comparison with Pre-MCO Levels
2.4.2. Comparison within Each MCO Levels
3. Results
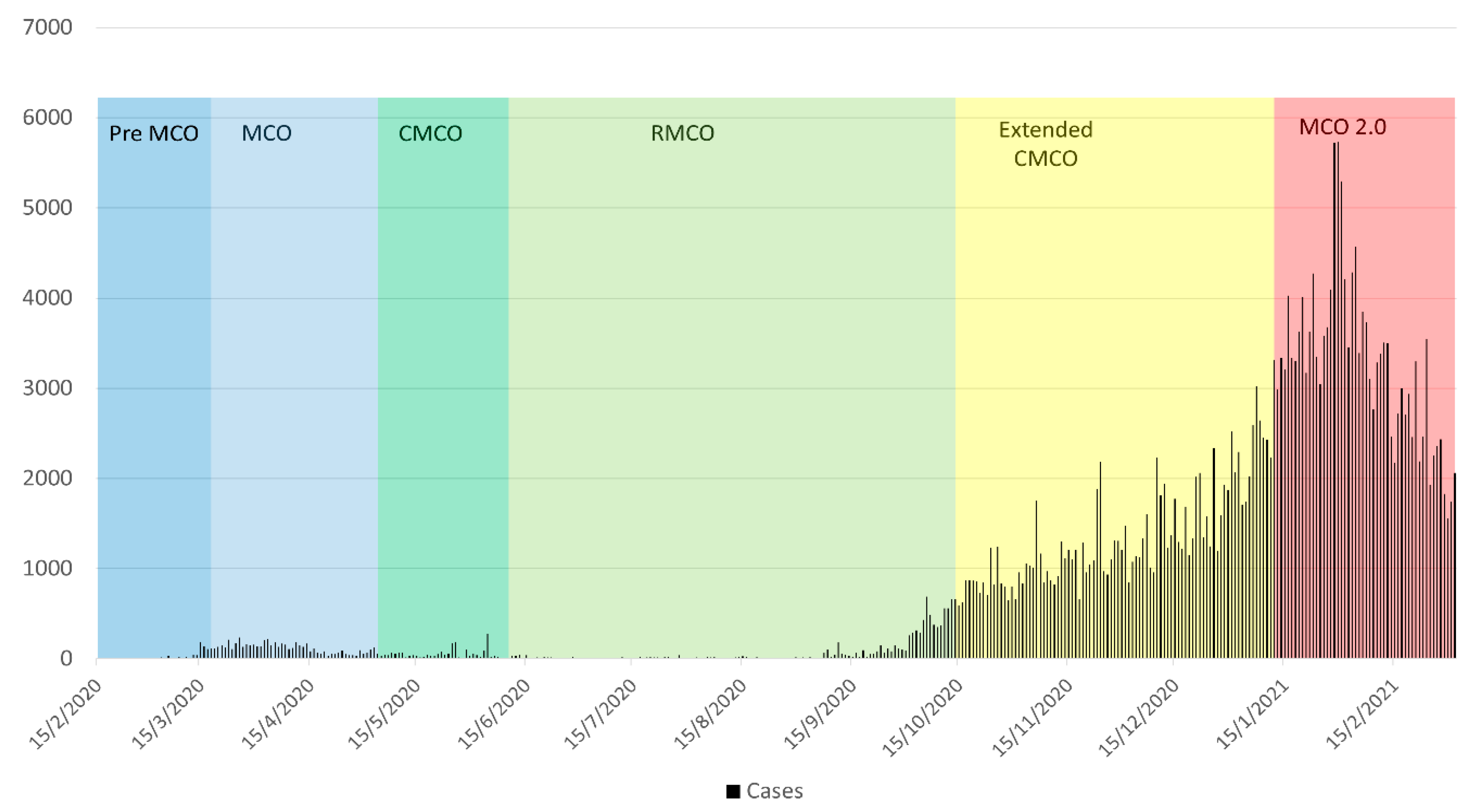
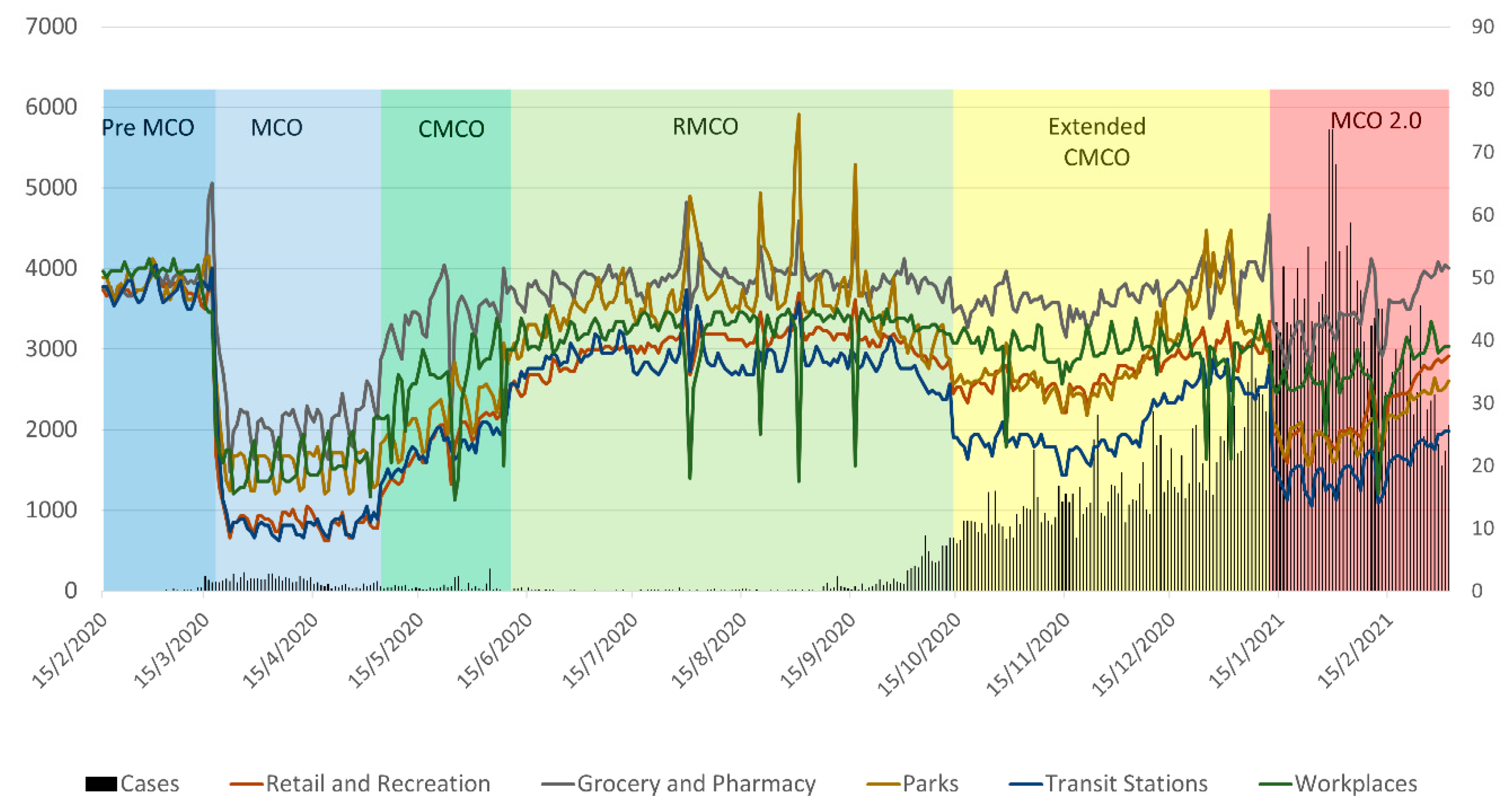
3.1. Characteristics of the COVID-19 Case Trends
3.2. MCO Effects on Average Mobility Trends—Descriptive Analysis
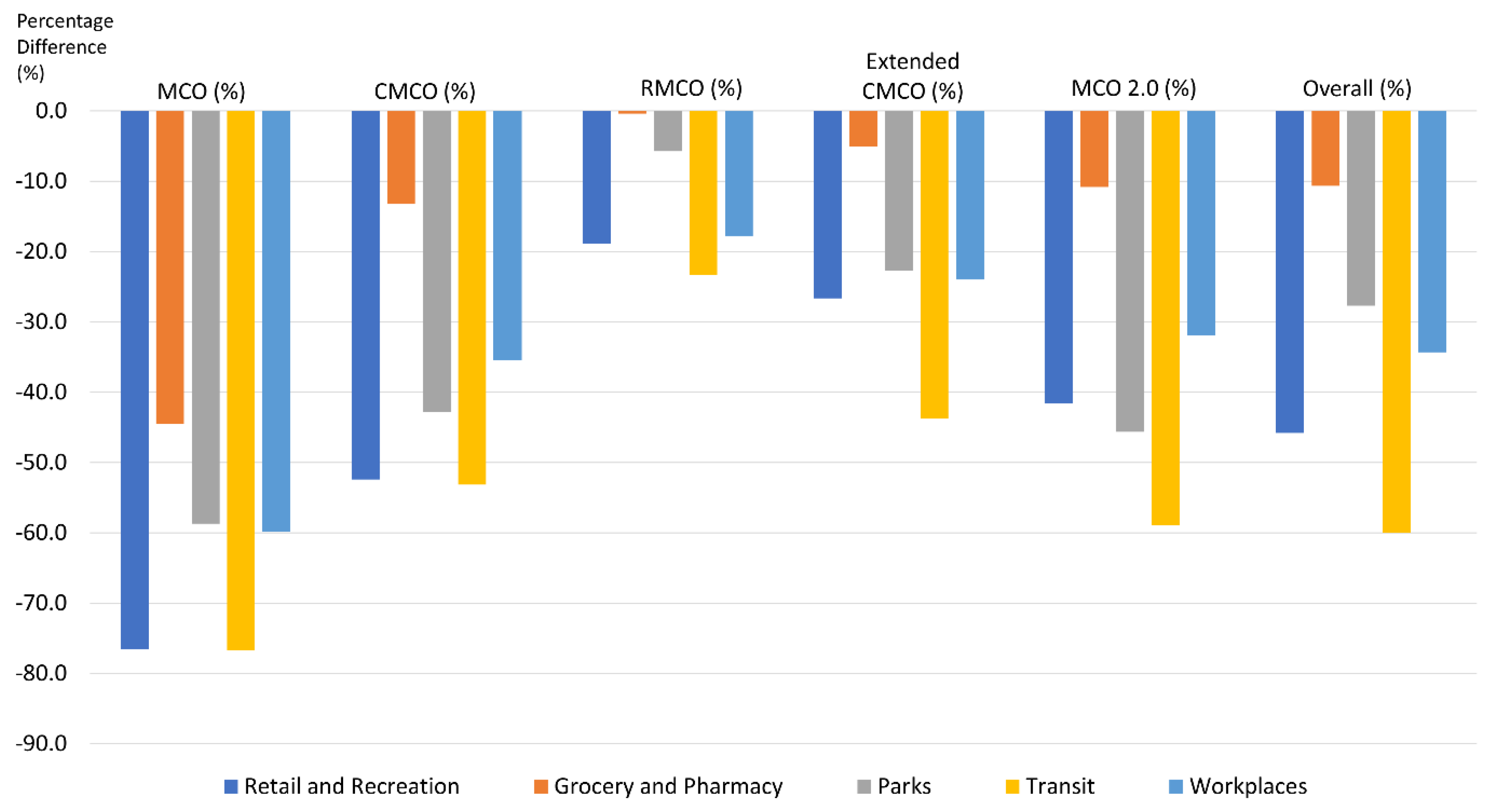
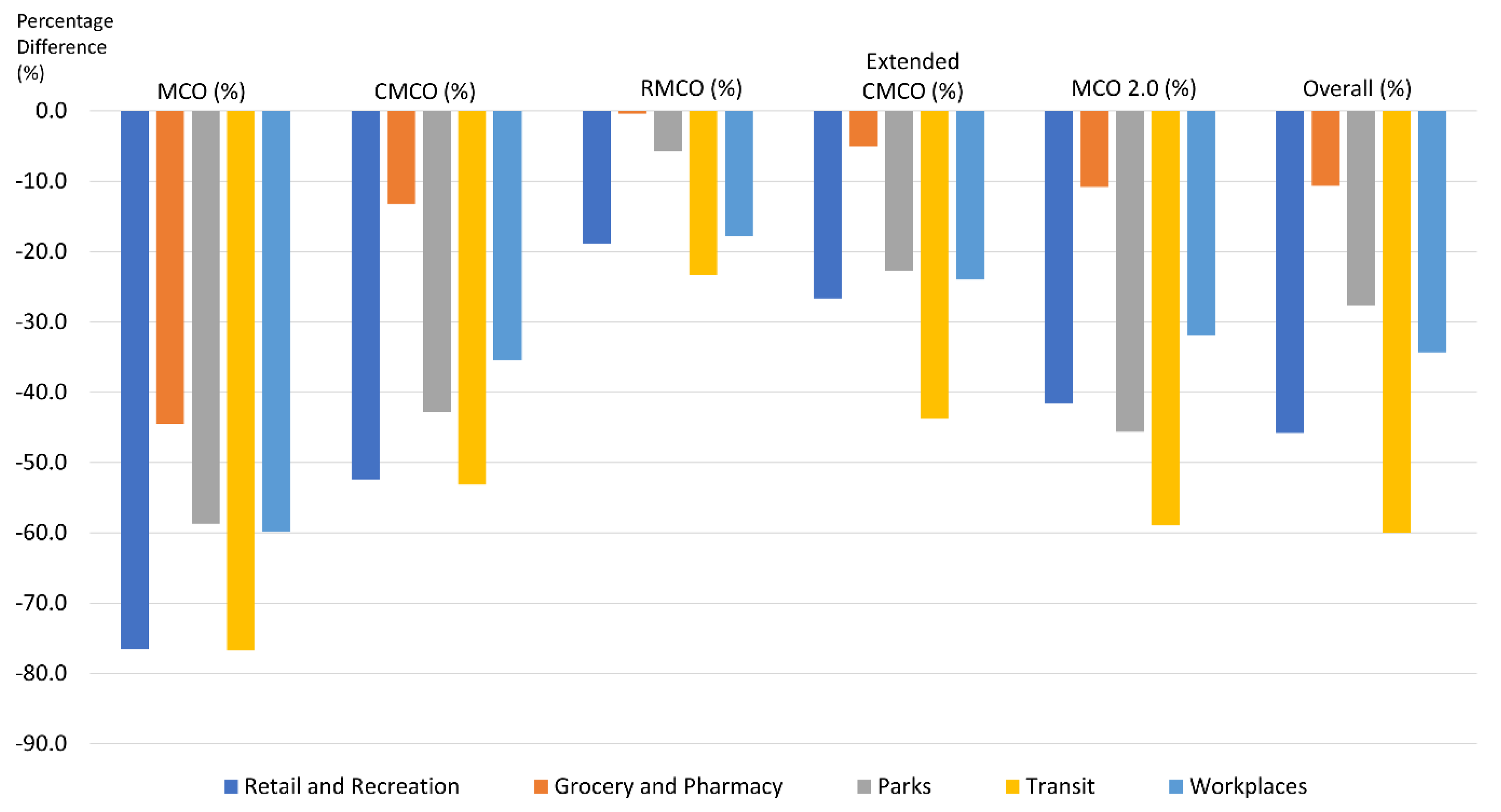
3.3. MCO Effects on Average Mobility Trends—Comparative Analysis with Pre-MCO Levels
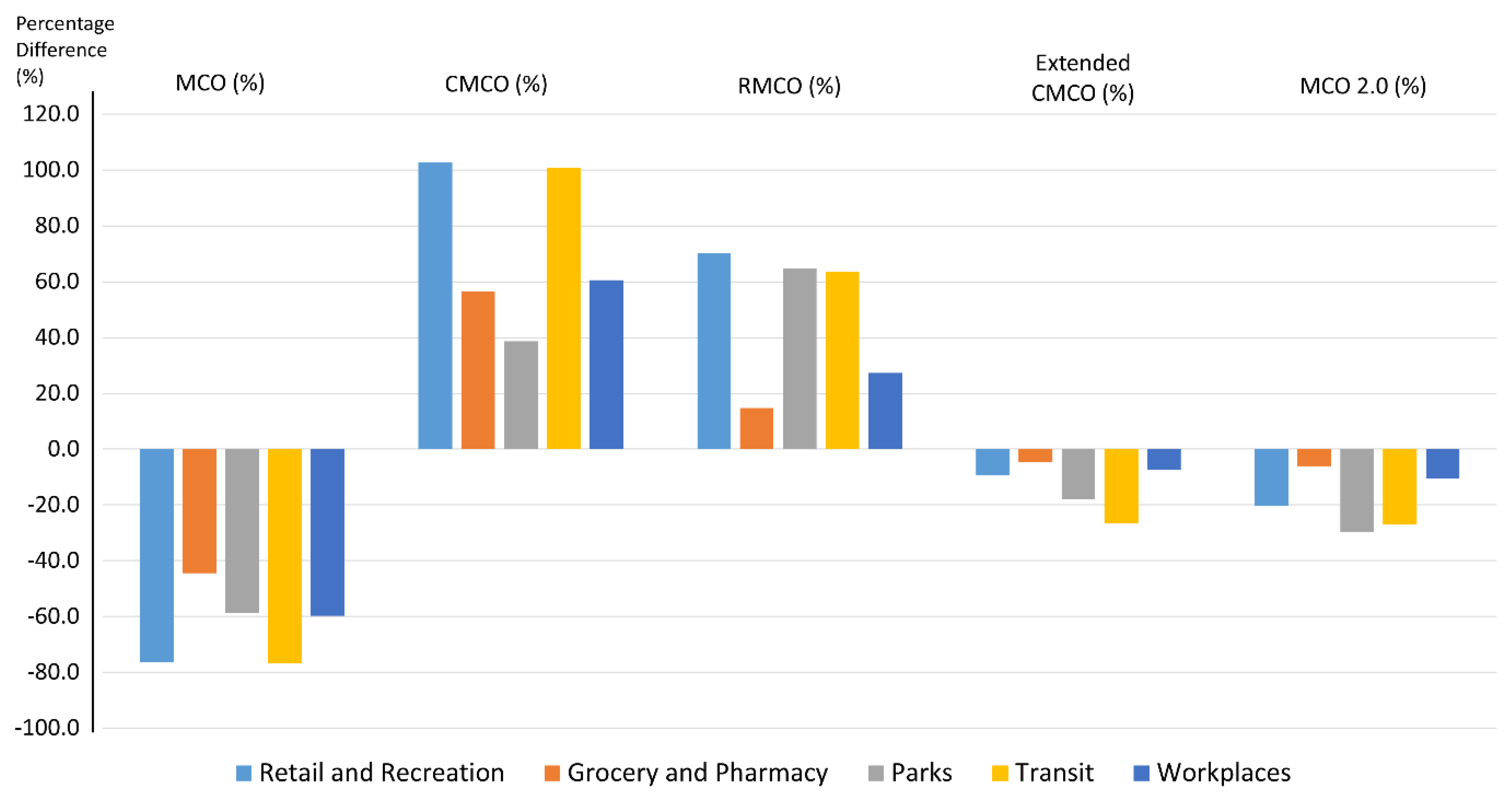
3.4. MCO Effects on Average Mobility Trends—Comparative Analysis within Each MCO Phases
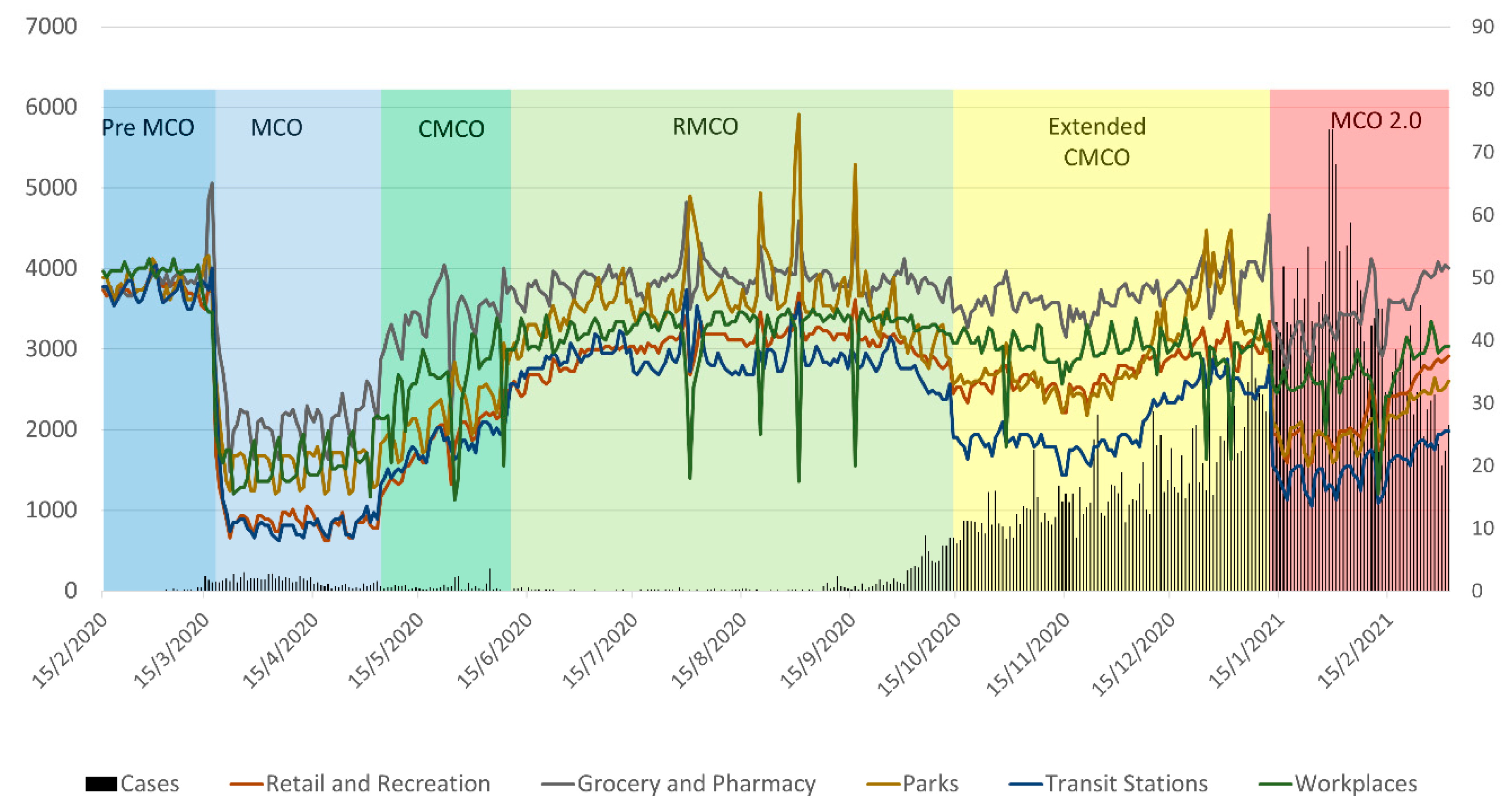
3.5. Case Trends and the Average Mobility Percentage Change during the MCO Phases
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cucinotta, D.; Vanelli, M. WHO Declares COVID-19 a Pandemic. Acta Biomed. 2020, 91, 157–160. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health Malaysia. MOH. 2021. Available online: https://www.moh.gov.my/ (accessed on 27 January 2021).
- Bergman, N.K.; Fishman, R.; Mobility Levels and COVID-19 Transmission Rates. MedRxiv. 2020. Available online: https://www.medrxiv.org/content/10.1101/2020.05.06.20093039v2.full.pdf (accessed on 10 March 2021).
- Cartenì, A.; Di Francesco, L.; Martino, M. How mobility habits influenced the spread of the COVID-19 pandemic: Results from the Italian case study. Sci. Total Environ. 2020, 741, 140489. [Google Scholar] [CrossRef] [PubMed]
- CDC. How 2019-nCoV Spreads. 2020. Available online: https://www.cdc.gov/%0Acoronavirus/2019-ncov/about/transmission.html (accessed on 10 March 2021).
- Hao, C.; Zou, X.; Lv, G.; McLaughlin, M.; Li, X.; Ling, L. The influence of migration on the burden of and response to infectious disease threats in China: A theoretically informed review. J. Public Adm. 2014, 4, 4–28. [Google Scholar]
- Phan, L.; Nguyen, T.; Luong, Q.; Nguyen, T.; Nguyen, H.; Le, H.; Nguyen, T.; Cao, T.; Pham, Q.D. Importation and Human-to-Human Transmission of a Novel Coronavirus in Vietnam. N. Engl. J. Med. 2020, 382, 872–874. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, P.; Hunter, T.; Bayen, A.M.; Schechtner, K.; González, M.C. Understanding road usage patterns in urban areas. Sci. Rep. 2013, 2, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, D.; Huang, J.; Li, Y.; Zhang, F.; Xu, C.; He, T. Exploring human mobility with multi-source data at extremely large metropolitanscales. ACM 2014, 201–212. [Google Scholar]
- Yuan, J.; Zheng, Y.; Xie, X. Discovering regions of different functions in a city using human mobility and pois. In Proceedings of the 12th ACM SIGKDD International Conference on Knowledge Discoveryand Data Mining, Beijing, China, 12–16 August 2012. [Google Scholar]
- Google LLC. Google COVID-19 Community Mobility Reports. 2020. Available online: https://www.google.com/%0Acovid19/mobility/ (accessed on 5 February 2021).
- Kraemer, M.; Yang, C.-H.; Gutierrez, B.; Wu, C.-H.; Klein, B.; Pigott, D. The effect of human mobility and control measures on the COVID-19 epidemic. China Sci. 2020, 368, 493–497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, A.; Liu, L.; Wang, C.; Guo, H.; Hao, X.; Wang, Q. Association of public health interventions with the epidemiology of the COVID-19 outbreak in Wuhan, China. JAMA: J. Am. Med. Assoc. 2020, 323, 1915–1923. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Institute for Health Systems Research, Ministry of Health Malaysia. Malaysia Health Sector Response to COVID-19 Pandemic, 1st ed.; Institute for Health Systems Research, Ministry of Health Malaysia: Putrajaya, Malaysia, 2020. Available online: http://library.nih.gov.my/e-doc/Flip-Book/Malaysian-Health-Sector-Response-to-COVID-19-Pandemic/index.html (accessed on 10 March 2021).
- Bernama. MCO: Travel Now Restricted to 10-km Radius. 2020. Available online: https://www.bernama.com/en/general/news.php?id=1827627 (accessed on 1 October 2021).
- Zolkepli, F.; Sivanandam, H. MCO Compliance at 97% but 482 Arrests over 26–27 March 2020. Available online: https://www.thestar.com.my/news/nation/2020/03/28/mco-compliance-at-97-but-482-arrests-over-march-26-27 (accessed on 10 March 2021).
- Disease Control Division Malaysia. Responding to COVID-19 Pandemic [Powerpoint Slides]; Disease Control Division Malaysia: Kuala Lumpur, Malaysia, 2020. [Google Scholar]
- World Health Organization. Current Situation and Key Insights. 27 December 2020. Available online: https://www.who.int/docs/default-source/coronaviruse/covid-strategy-update-14april2020.pdf (accessed on 10 March 2021).
- Kurian, S.J.; Bhatti, A.; Alvi, M.A.; Ting, H.H.; Storlie, C.; Wilson, P.M.; Shah, N.D.; Liu, H.; Bydon, M. Correlations Between COVID-19 Cases and Google Trends Data in the United States: A State-by-State Analysis. Mayo Clin. Proc. 2020, 95, 2370–2381. [Google Scholar] [CrossRef] [PubMed]
- Rovetta, A. Reliability of Google Trends: Analysis of the Limits and Potential of Web Infoveillance during COVID-19 Pandemic and for Future Research. Front. Res. Metr. Anal. 2021, 6, 670226. [Google Scholar] [CrossRef] [PubMed]
- Vyas, L.; Nantapong, B. The impact of working from home during COVID-19 on work and life domains: An exploratory study on Hong Kong. Policy Des. Pract. 2020, 4, 59–76. [Google Scholar] [CrossRef]
- Siqin, W.; Yan, L.; Tao, H. Examining the Change of Human Mobility Adherent to Social Restriction Policies and Its Effect on COVID-19 Cases in Australia. Int. J. Environ. Res. Public Health 2020, 17, 7930. [Google Scholar] [CrossRef]
- Tashny, S. Coronavirus Malaysia: PM Blames Sabah Election as among Causes of Huge Infection Surge; The Coronavirus Pandemic. 2020. Available online: https://www.scmp.com/week-asia/health-environment/article/3104421/coronavirus-malaysia-pm-blames-sabah-election-among (accessed on 18 March 2021).
- Rampal, L.; Liew, B.S. Malaysia’s third COVID-19 wave—A paradigm shift required. Med. J. Malays. 2021, 76, 1–4. [Google Scholar]
- UITP. The Future of Mobility Post-COVID. Available online: https://cms.uitp.org/wp/wp-content/uploads/2020/10/2020-ADL-FoM-Lab-UITP_Future-of-Mobility-post-COVID-study.pdf (accessed on 20 September 2021).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Phases | Dates of Enforcement | Characteristics |
|---|---|---|
| Pre-MCO | Prior to 18 March 2020 |
|
| MCO | 18 March2020–3 May2020 |
|
| Conditional MCO (CMCO) | 4 May 2020–9 June2020 |
|
| Recovery MCO (RMCO) | 10 June 2020–13 October 2020 |
|
| Extended CMCO | 14 October 2020–12 January 2021 |
|
| MCO 2.0 | 13 January 2021–4 March2021 |
|
| Period | Category | Retail and Recreation | Grocery and Pharmacy | Parks | Transit Stations | Workplaces |
|---|---|---|---|---|---|---|
| Pre-MCO 15 February 2020–17 March 2020 | Average Mobility | 48.1 | 49.9 | 48.9 | 48.0 | 50.5 |
| Range | 45.0–51.5 | 47.0–65.0 | 46.0–53.5 | 45.0–52.0 | 44.5–53.0 | |
| MCO 18 March 2020–3 May 2020 | Average Mobility | 11.3 | 27.7 | 20.2 | 11.2 | 20.3 |
| Range | 8–22 | 19–43 | 15.5–34 | 8–32 | 15–27.5 | |
| CMCO 4 May 2020–9 June 2020 | Average Mobility | 22.9 | 43.3 | 28.0 | 22.5 | 32.6 |
| Range | 10–32 | 26.5–48 | 17–39.5 | 11.5–27 | 14.5–43.5 | |
| RMCO 10 June 2020–13 October 2020 | Average Mobility | 39.0 | 49.7 | 46.1 | 36.8 | 41.5 |
| Range | 31–47.5 | 44.5–62 | 35.5–76 | 30.5–48 | 17.5–45 | |
| Extended CMCO 14 October 2020–12 January 2021 | Average Mobility | 35.3 | 47.4 | 37.8 | 27.0 | 38.4 |
| Range | 28.5–43 | 40.5–60 | 28–57.5 | 18.5–37 | 21–44 | |
| MCO 2.0 13 January 2021– 4 March 2021 | Average Mobility | 28.1 | 44.5 | 26.6 | 19.7 | 34.4 |
| Range | 20.5–37.5 | 35.5–53 | 20–34 | 13.5–25.5 | 15.5–43 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rajendran, K.; Ahmad, N.; Singh, S.; Heng, L.-C.; Ismail, R.; Shaharudin, R.; Aris, T.; Sundram, B.M. The Effect of Movement Control Order for Various Population Mobility Phases during COVID-19 in Malaysia. COVID 2021, 1, 590-601. https://doi.org/10.3390/covid1030049
Rajendran K, Ahmad N, Singh S, Heng L-C, Ismail R, Shaharudin R, Aris T, Sundram BM. The Effect of Movement Control Order for Various Population Mobility Phases during COVID-19 in Malaysia. COVID. 2021; 1(3):590-601. https://doi.org/10.3390/covid1030049
Chicago/Turabian StyleRajendran, Kamesh, Nadhar Ahmad, Sarbhan Singh, Lai-Chee Heng, Rohaida Ismail, Rafiza Shaharudin, Tahir Aris, and Bala Murali Sundram. 2021. "The Effect of Movement Control Order for Various Population Mobility Phases during COVID-19 in Malaysia" COVID 1, no. 3: 590-601. https://doi.org/10.3390/covid1030049
APA StyleRajendran, K., Ahmad, N., Singh, S., Heng, L.-C., Ismail, R., Shaharudin, R., Aris, T., & Sundram, B. M. (2021). The Effect of Movement Control Order for Various Population Mobility Phases during COVID-19 in Malaysia. COVID, 1(3), 590-601. https://doi.org/10.3390/covid1030049