
Predictors of Complete Pathological Response with Chemoimmunotherapy in Triple-Negative Breast Cancer: A Meta-Analysis

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
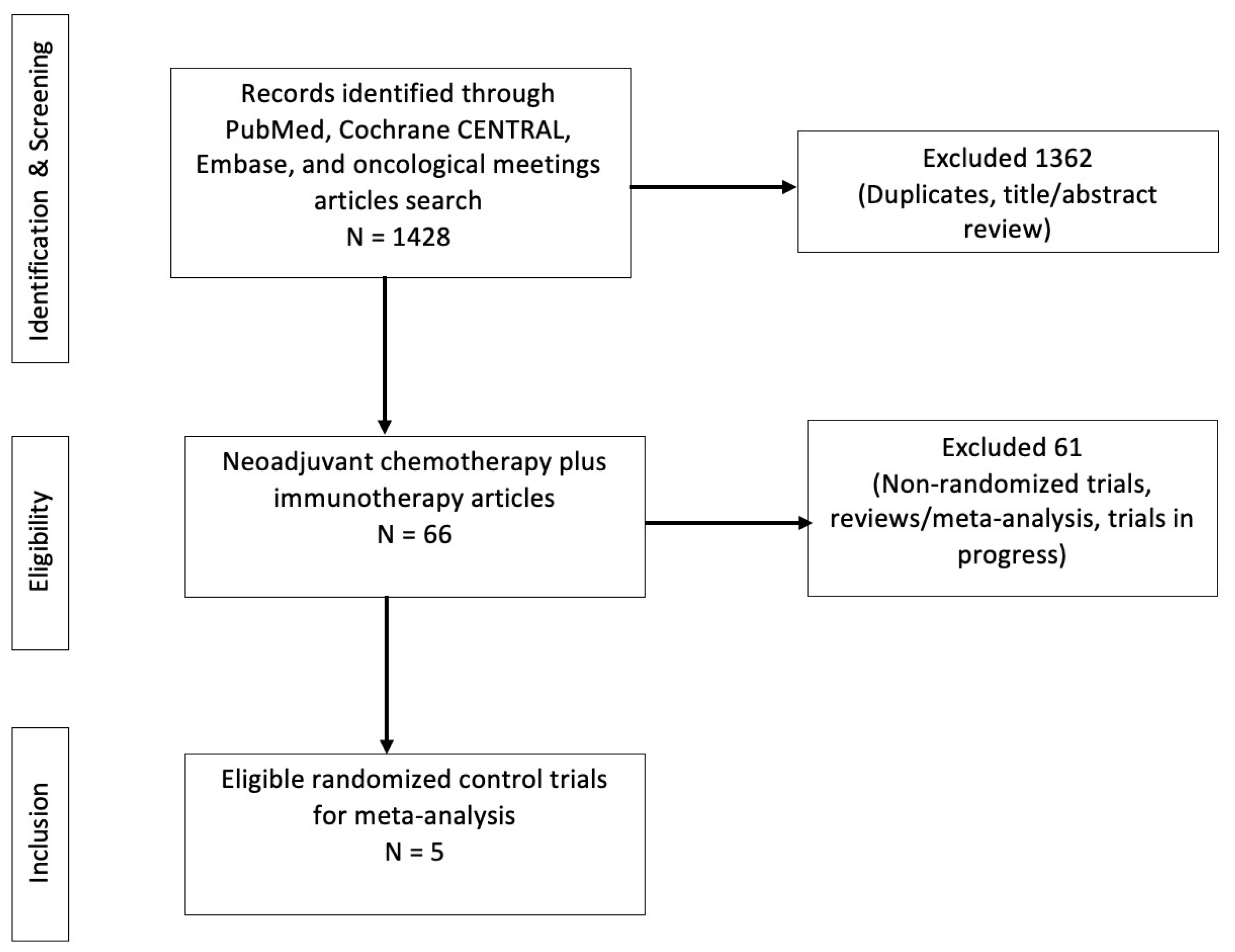
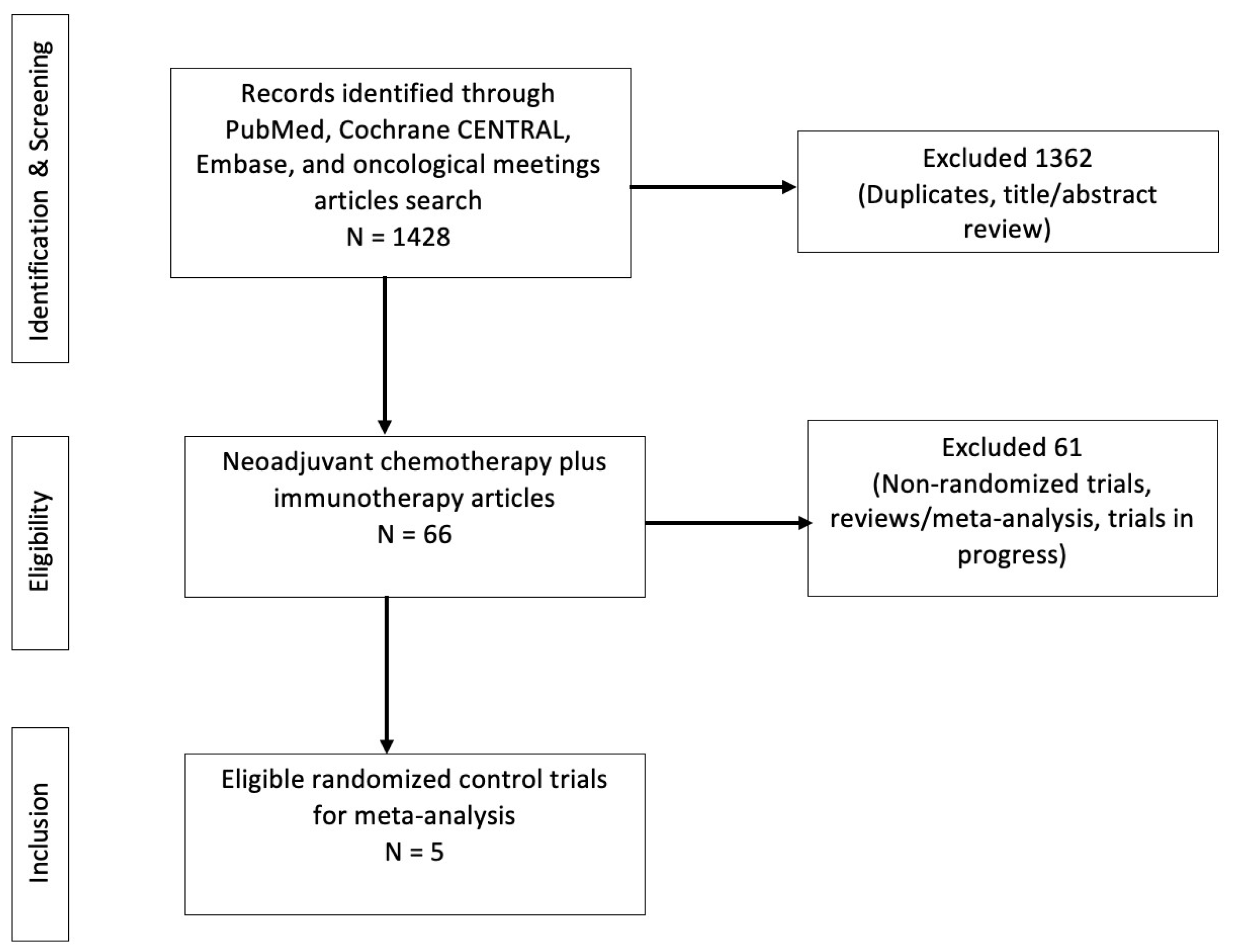
2.1. Selection Process and Eligibility
2.2. Data Collection Process
2.3. Statistical Analysis
3. Results
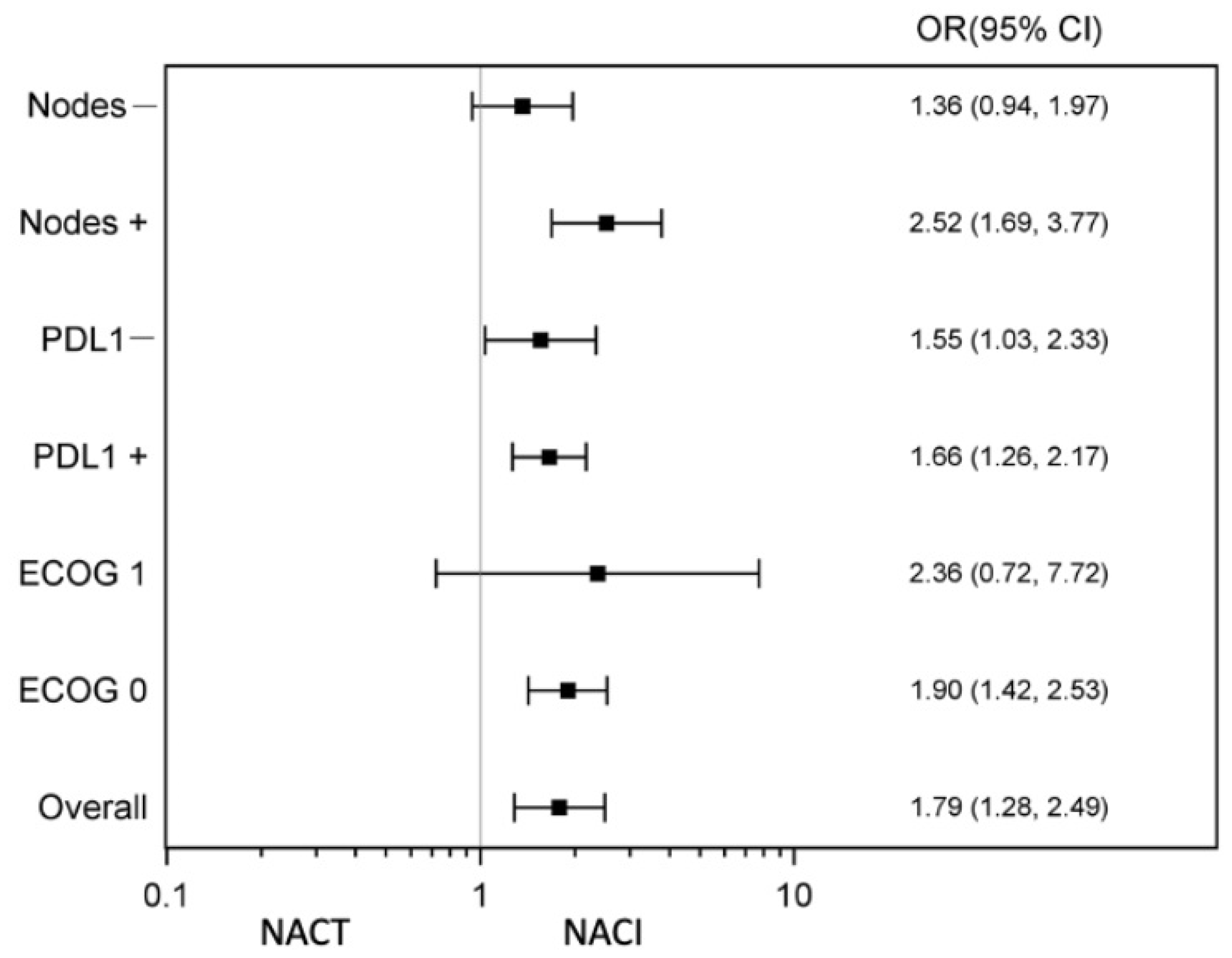
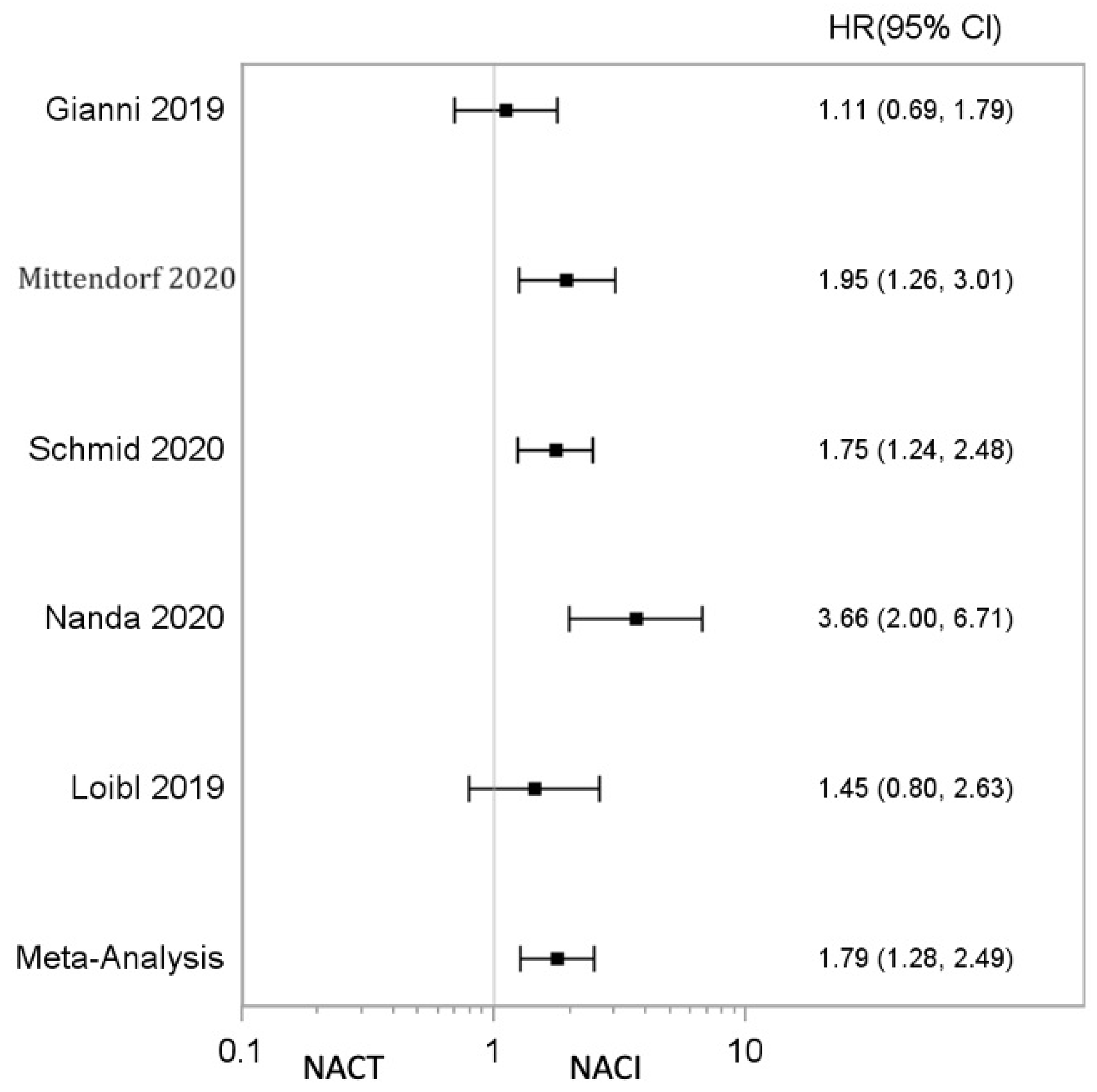
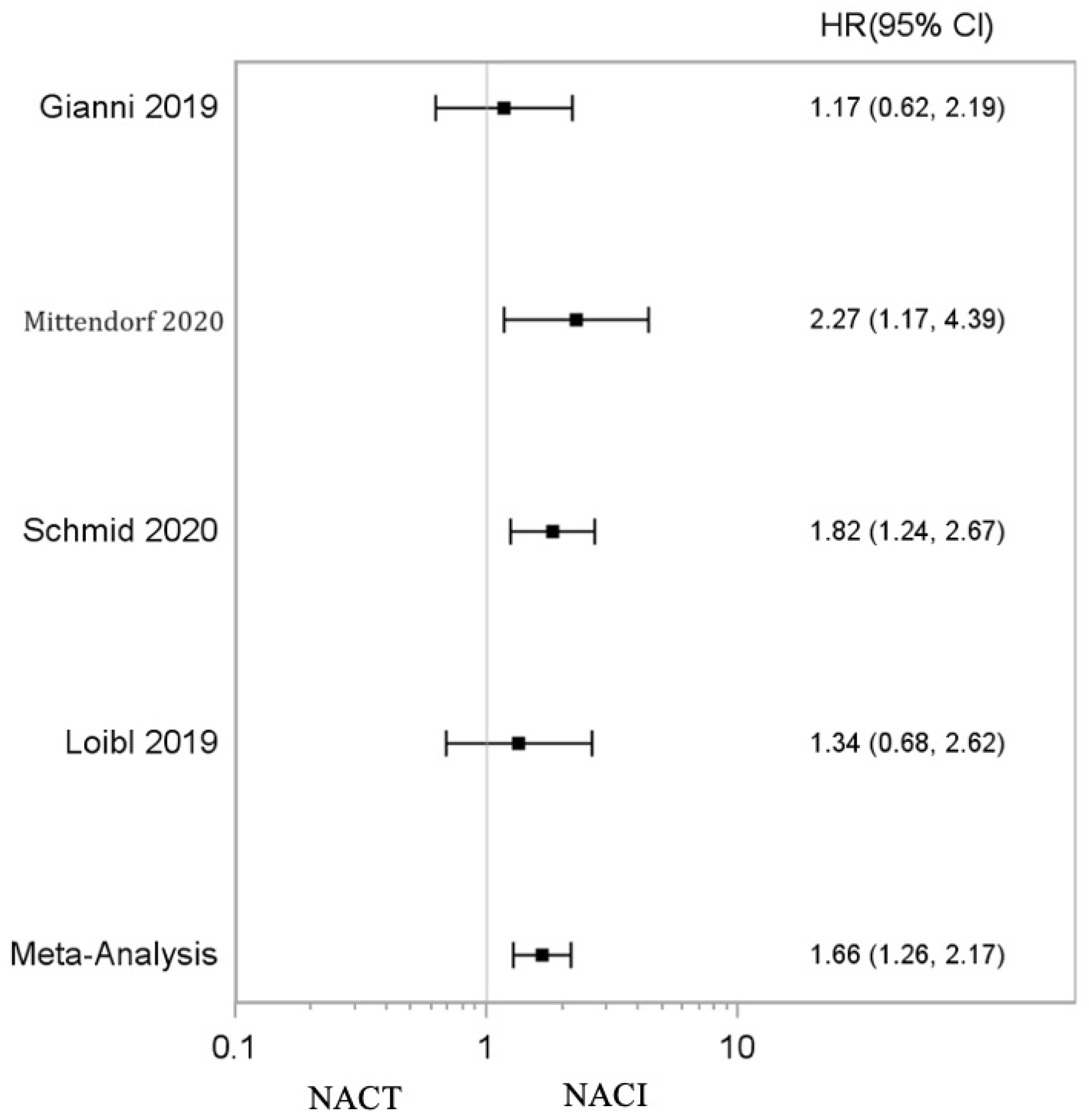
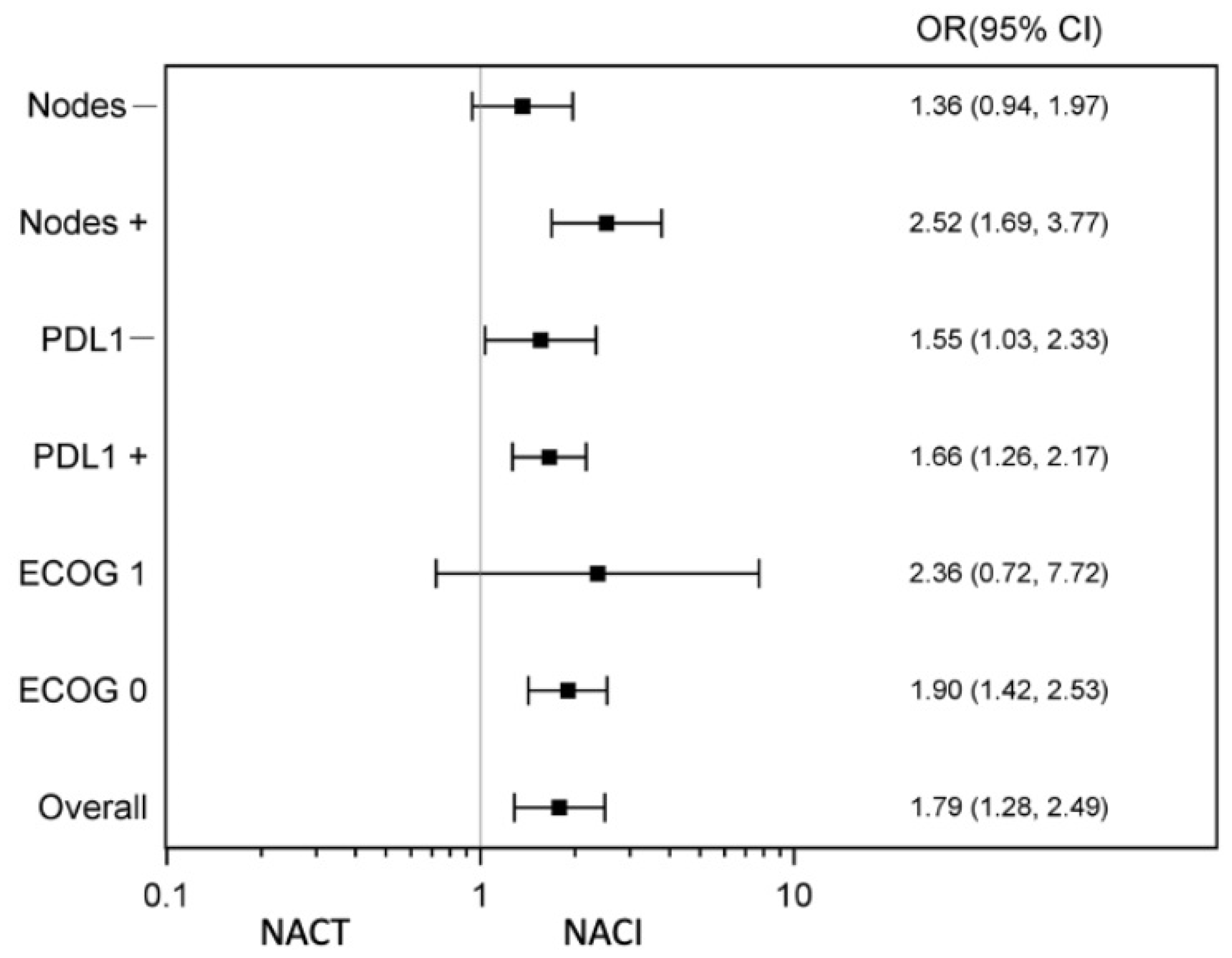
3.1. Factors Affecting Pathological Complete Response
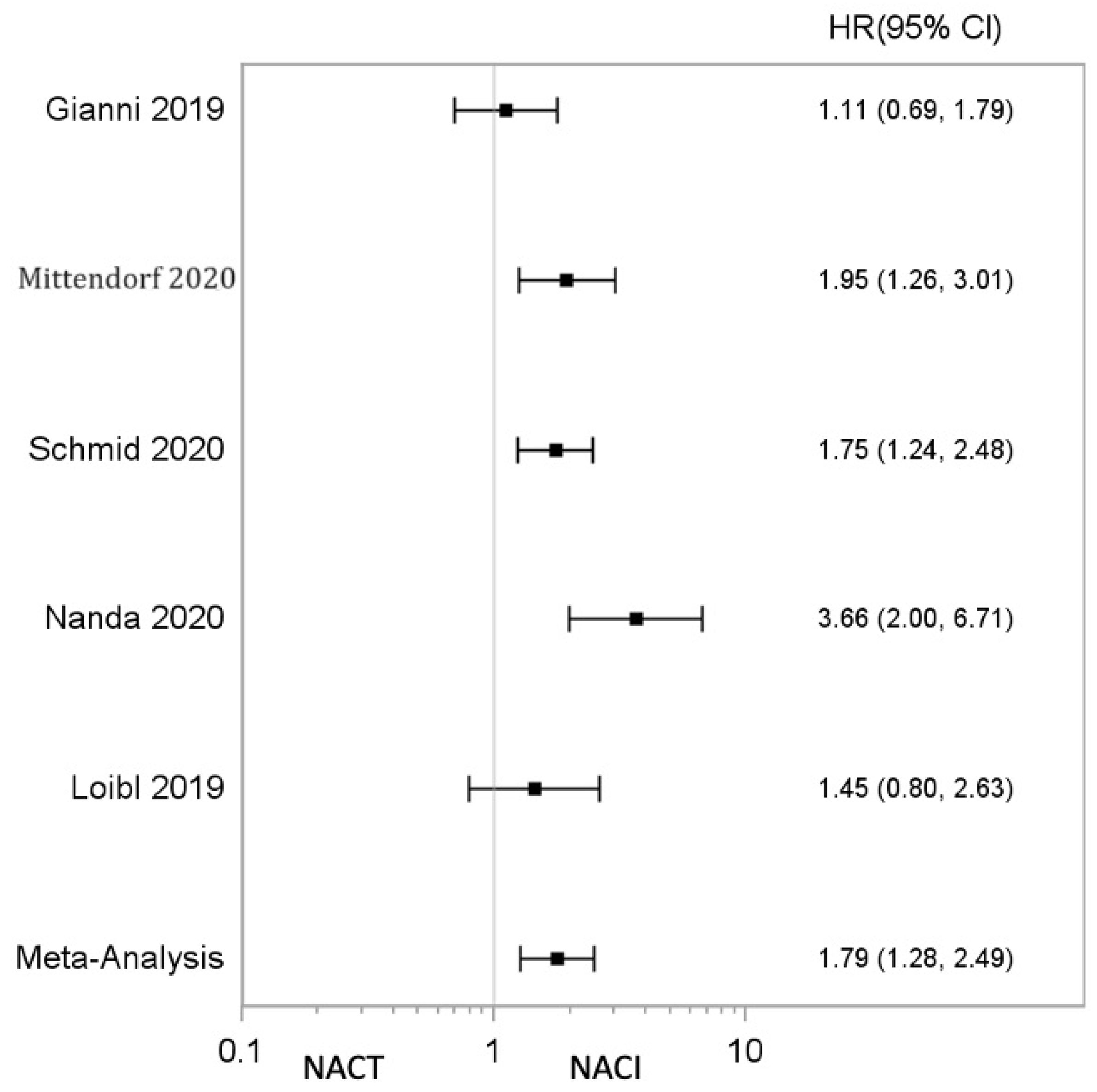
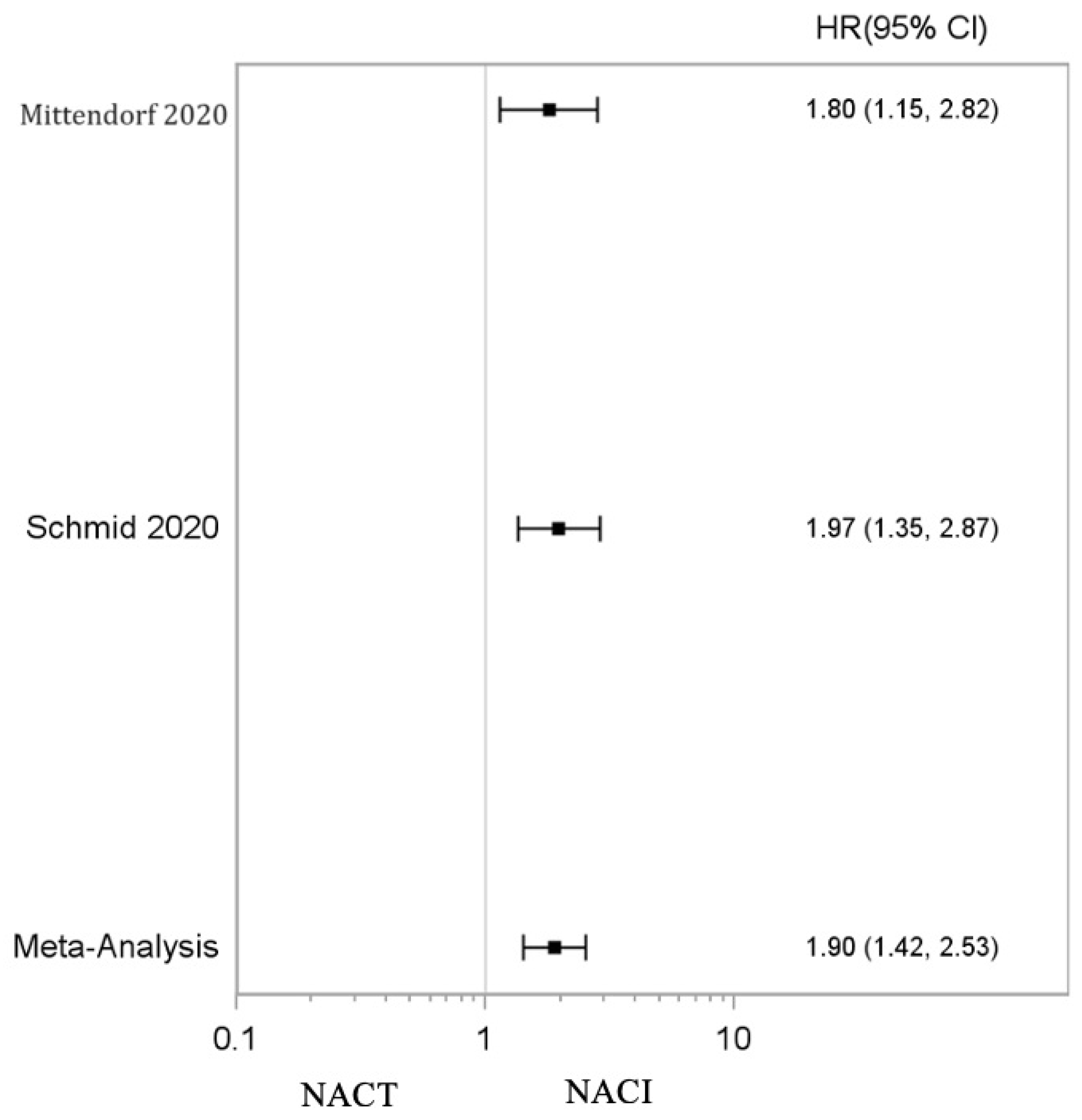
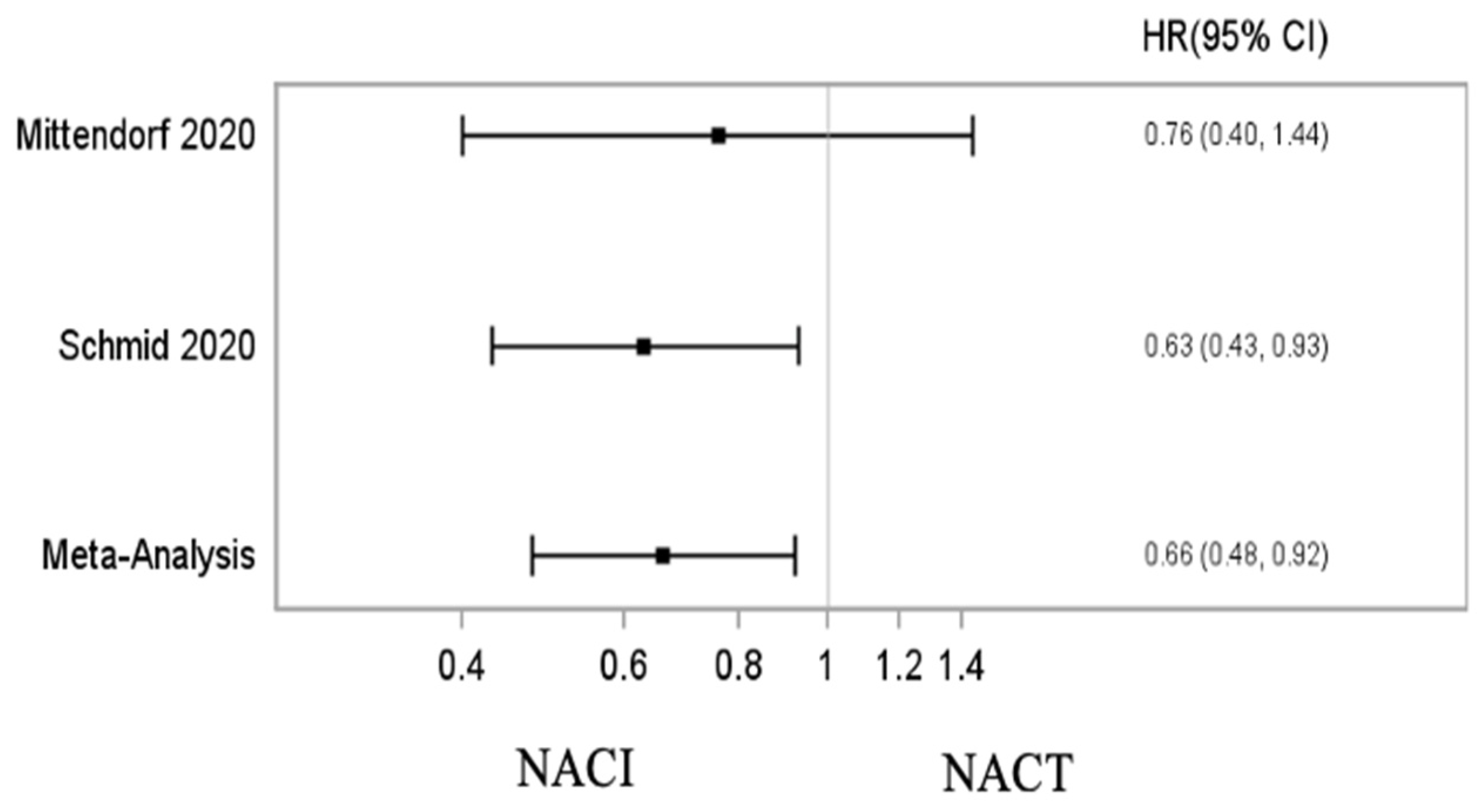
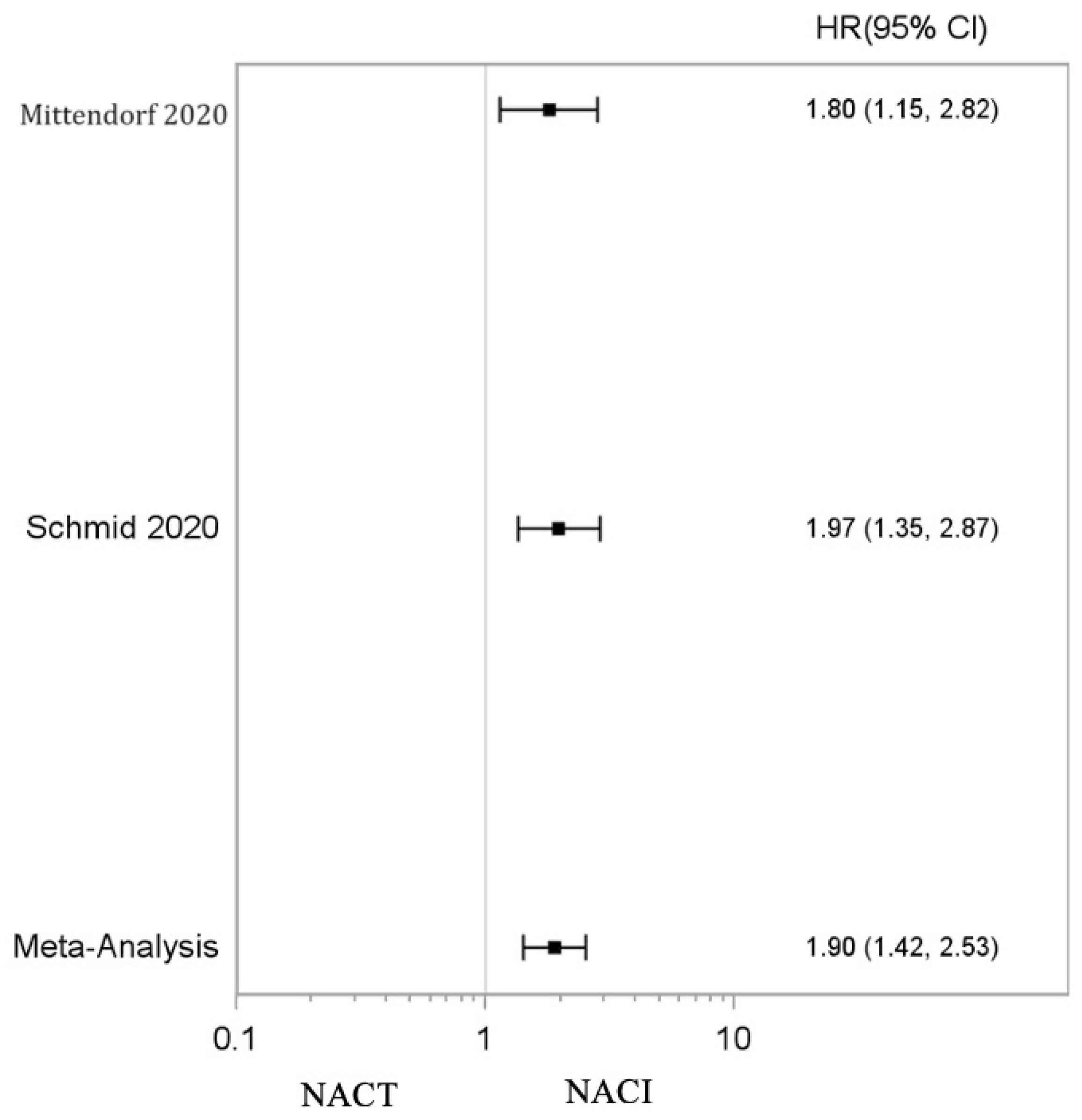
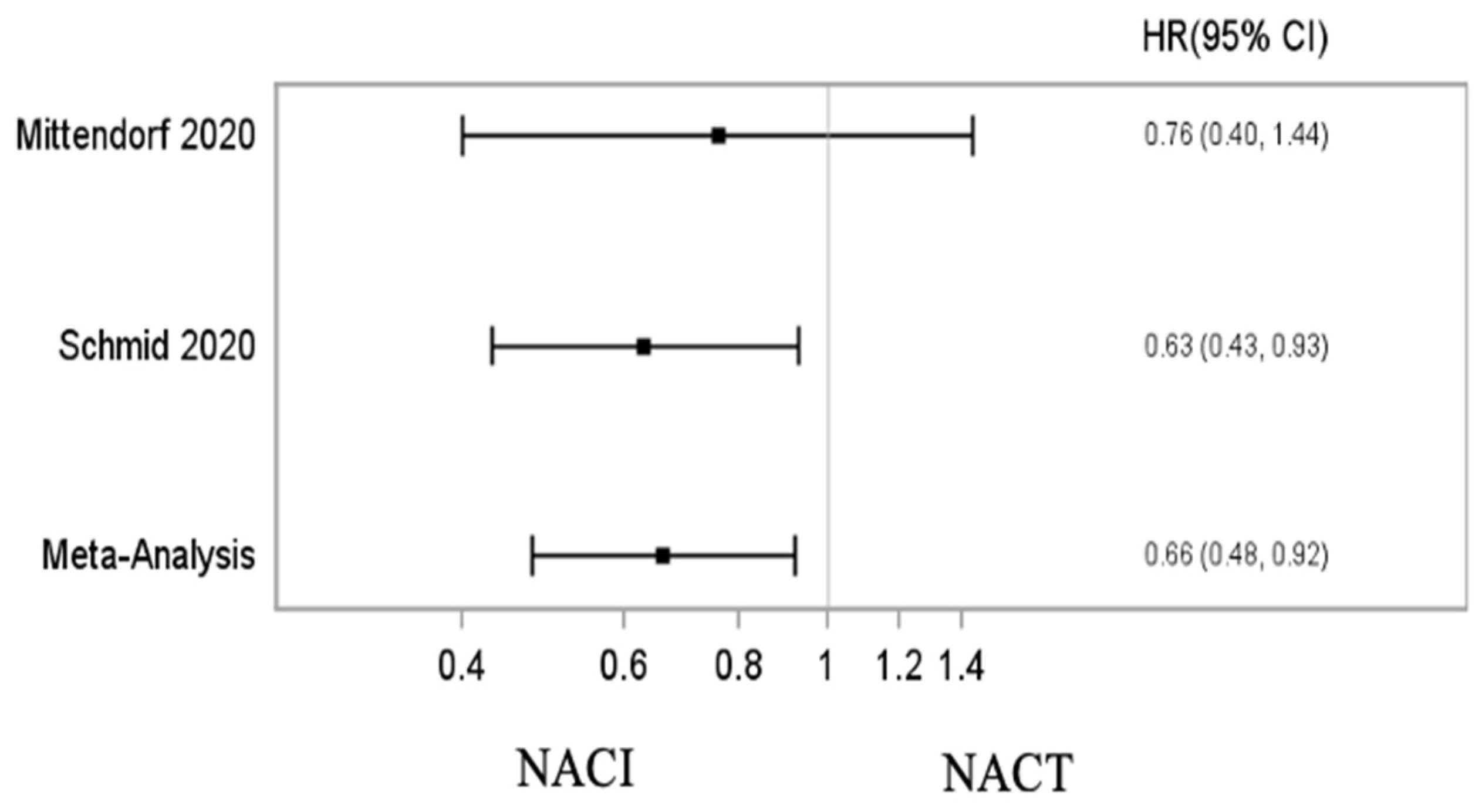
3.2. Impact of Addition of Neoadjuvant Immunotherapy on Survival Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aysola, K.; Desai, A.; Welch, C.; Xu, J.; Qin, Y.; Reddy, V.; Matthews, R.; Owens, C.; Okoli, J.; Beech, D.J.; et al. Triple Negative Breast Cancer—An Overview. Hered. Genet. 2013, 2013, 1. [Google Scholar] [CrossRef]
- Li, Y.; Zhang, H.; Merkher, Y.; Chen, L.; Liu, Z.N.; Leonov, S.; Chen, Y. Recent advances in therapeutic strategies for triple-negative breast cancer. J. Hematol. Oncol. 2022, 15, 121. [Google Scholar] [CrossRef] [PubMed]
- van den Ende, N.S.; Nguyen, A.H.; Jager, A.; Kok, M.; Debets, R.; van Deurzen, C.H.M. Triple-Negative Breast Cancer and Predictive Markers of Response to Neoadjuvant Chemotherapy: A Systematic Review. Int. J. Mol. Sci. 2023, 24, 2969. [Google Scholar] [CrossRef] [PubMed]
- Gupta, R.K.; Roy, A.M.; Gupta, A.; Takabe, K.; Dhakal, A.; Opyrchal, M.; Kalinski, P.; Gandhi, S. Systemic Therapy De-Escalation in Early-Stage Triple-Negative Breast Cancer: Dawn of a New Era? Cancers 2022, 14, 1856. [Google Scholar] [CrossRef] [PubMed]
- Mittendorf, E.A.; Zhang, H.; Barrios, C.H.; Saji, S.; Jung, K.H.; Hegg, R.; Koehler, A.; Sohn, J.; Iwata, H.; Telli, M.L.; et al. Neoadjuvant atezolizumab in combination with sequential nab-paclitaxel and anthracycline-based chemotherapy versus placebo and chemotherapy in patients with early-stage triple-negative breast cancer (IMpassion031): A randomised, double-blind, phase 3 trial. Lancet 2020, 396, 1090–1100. [Google Scholar] [CrossRef] [PubMed]
- Schmid, P.; Cortes, J.; Pusztai, L.; McArthur, H.; Kummel, S.; Bergh, J.; Denkert, C.; Park, Y.H.; Hui, R.; Harbeck, N.; et al. Pembrolizumab for Early Triple-Negative Breast Cancer. N. Engl. J. Med. 2020, 382, 810–821. [Google Scholar] [CrossRef] [PubMed]
- Nanda, R.; Liu, M.C.; Yau, C.; Shatsky, R.; Pusztai, L.; Wallace, A.; Chien, A.J.; Forero-Torres, A.; Ellis, E.; Han, H.; et al. Effect of Pembrolizumab Plus Neoadjuvant Chemotherapy on Pathologic Complete Response in Women with Early-Stage Breast Cancer: An Analysis of the Ongoing Phase 2 Adaptively Randomized I-SPY2 Trial. JAMA Oncol. 2020, 6, 676–684. [Google Scholar] [CrossRef] [PubMed]
- Loibl, S.; Untch, M.; Burchardi, N.; Huober, J.; Sinn, B.V.; Blohmer, J.U.; Grischke, E.M.; Furlanetto, J.; Tesch, H.; Hanusch, C.; et al. A randomised phase II study investigating durvalumab in addition to an anthracycline taxane-based neoadjuvant therapy in early triple-negative breast cancer: Clinical results and biomarker analysis of GeparNuevo study. Ann. Oncol. 2019, 30, 1279–1288. [Google Scholar] [CrossRef]
- Gianni, L.; Huang, C.S.; Egle, D.; Bermejo, B.; Zamagni, C.; Thill, M.; Anton, A.; Zambelli, S.; Bianchini, G.; Russo, S.; et al. Pathologic complete response (pCR) to neoadjuvant treatment with or without atezolizumab in triple-negative, early high-risk and locally advanced breast cancer: NeoTRIP Michelangelo randomized study. Ann. Oncol. 2022, 33, 534–543. [Google Scholar] [CrossRef]
- Gao, G.; Wang, Z.; Qu, X.; Zhang, Z. Prognostic value of tumor-infiltrating lymphocytes in patients with triple-negative breast cancer: A systematic review and meta-analysis. BMC Cancer 2020, 20, 179. [Google Scholar] [CrossRef]
- Chan, J.J.Y.; Tan, T.J.; Dent, R.A. Novel therapeutic avenues in triple-negative breast cancer: PI3K/AKT inhibition, androgen receptor blockade, and beyond. Ther. Adv. Med. Oncol. 2019, 11, 1758835919880429. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Nie, J.; Ma, X.; Wei, Y.; Peng, Y.; Wei, X. Targeting PI3K in cancer: Mechanisms and advances in clinical trials. Mol. Cancer 2019, 18, 26. [Google Scholar] [CrossRef] [PubMed]
- Nedeljković, M.; Damjanović, A. Mechanisms of Chemotherapy Resistance in Triple-Negative Breast Cancer—How We Can Rise to the Challenge. Cells 2019, 8, 957. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; Chou, R.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Fournier, M.V.; Goodwin, E.C.; Chen, J.; Obenauer, J.C.; Tannenbaum, S.H.; Brufsky, A.M. A Predictor of Pathological Complete Response to Neoadjuvant Chemotherapy Stratifies Triple Negative Breast Cancer Patients with High Risk of Recurrence. Sci. Rep. 2019, 9, 14863. [Google Scholar] [CrossRef] [PubMed]
- Spring, L.M.; Fell, G.; Arfe, A.; Sharma, C.; Greenup, R.; Reynolds, K.L.; Smith, B.L.; Alexander, B.; Moy, B.; Isakoff, S.J.; et al. Pathological complete response after neoadjuvant chemotherapy and impact on breast cancer recurrence and survival: A comprehensive meta-analysis. Clin. Cancer Res. 2020, 26, 2838. [Google Scholar] [CrossRef] [PubMed]
- Schmid, P.; Salgado, R.; Park, Y.H.; Muñoz-Couselo, E.; Kim, S.B.; Sohn, J.; Im, S.A.; Foukakis, T.; Kuemmel, S.; Dent, R.; et al. Pembrolizumab plus chemotherapy as neoadjuvant treatment of high-risk, early-stage triple-negative breast cancer: Results from the phase 1b open-label, multicohort KEYNOTE-173 study. Ann. Oncol. 2020, 31, 569–581. [Google Scholar] [CrossRef]
- Ademuyiwa, F.O.; Gao, F.; Street, C.R.; Chen, I.; Northfelt, D.W.; Wesolowski, R.; Arora, M.; Brufsky, A.; Dees, E.C.; Santa-Maria, C.A.; et al. A randomized phase 2 study of neoadjuvant carboplatin and paclitaxel with or without atezolizumab in triple negative breast cancer (TNBC)—NCI 10013. npj Breast Cancer 2022, 8, 134. [Google Scholar] [CrossRef]
- Xin, Y.; Shen, G.; Zheng, Y.; Guan, Y.; Huo, X.; Li, J.; Ren, D.; Zhao, F.; Liu, Z.; Li, Z.; et al. Immune checkpoint inhibitors plus neoadjuvant chemotherapy in early triple-negative breast cancer: A systematic review and meta-analysis. BMC Cancer 2021, 21, 1261. [Google Scholar] [CrossRef]
- von Minckwitz, G.; Untch, M.; Blohmer, J.U.; Costa, S.D.; Eidtmann, H.; Fasching, P.A.; Gerber, B.; Eiermann, W.; Hilfrich, J.; Huober, J.; et al. Definition and impact of pathologic complete response on prognosis after neoadjuvant chemotherapy in various intrinsic breast cancer subtypes. J. Clin. Oncol. 2012, 30, 1796–1804. [Google Scholar] [CrossRef]
- Liedtke, C.; Mazouni, C.; Hess, K.R.; André, F.; Tordai, A.; Mejia, J.A.; Symmans, W.F.; Gonzalez-Angulo, A.M.; Hennessy, B.; Green, M.; et al. Response to neoadjuvant therapy and long-term survival in patients with triple-negative breast cancer. J. Clin. Oncol. 2008, 26, 1275–1281. [Google Scholar] [CrossRef]
- Squifflet, P.; Saad, E.D.; Loibl, S.; van Mackelenbergh, M.T.; Untch, M.; Rastogi, P.; Gianni, L.; Schneeweiss, A.; Conte, P.; Piccart, M.; et al. Re-Evaluation of Pathologic Complete Response as a Surrogate for Event-Free and Overall Survival in Human Epidermal Growth Factor Receptor 2-Positive, Early Breast Cancer Treated with Neoadjuvant Therapy Including Anti-Human Epidermal Growth Factor Receptor 2 Therapy. J. Clin. Oncol. 2023, 41, 2988–2997. [Google Scholar] [CrossRef] [PubMed]
- Roy, A.M.; Patel, A.; Catalfamo, K.; Attwood, K.; Khoury, T.; Yao, S.; Gandhi, S. Racial and Ethnic Disparity in Preoperative Chemosensitivity and Survival in Patients with Early-Stage Breast Cancer. JAMA Netw. Open 2023, 6, e2344517. [Google Scholar] [CrossRef] [PubMed]
- Bai, R.; Lv, Z.; Xu, D.; Cui, J. Predictive biomarkers for cancer immunotherapy with immune checkpoint inhibitors. Biomark. Res. 2020, 8, 34. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.; Du, K.; Ai, M.; Wang, B.; Lin, J.; Ren, A.; Chen, C.; Huang, Z.; Qiu, W.; Yuan, Y.; et al. PD-L1 expression as biomarker of efficacy of PD-1/PD-L1 checkpoint inhibitors in metastatic triple negative breast cancer: A systematic review and meta-analysis. Front. Immunol. 2023, 14, 1060308. [Google Scholar] [CrossRef] [PubMed]
- Deng, H.; Wang, L.; Wang, N.; Zhang, K.; Zhao, Y.; Qiu, P.; Qi, X.; Zhang, D.; Xu, F.; Liu, J. Neoadjuvant checkpoint blockade in combination with Chemotherapy in patients with tripe-negative breast cancer: Exploratory analysis of real-world, multicenter data. BMC Cancer 2023, 23, 29. [Google Scholar] [CrossRef] [PubMed]
- Barron, A.U.; Hoskin, T.L.; Day, C.N.; Hwang, E.S.; Kuerer, H.M.; Boughey, J.C. Association of Low Nodal Positivity Rate Among Patients with ERBB2-Positive or Triple-Negative Breast Cancer and Breast Pathologic Complete Response to Neoadjuvant Chemotherapy. JAMA Surg. 2018, 153, 1120–1126. [Google Scholar] [CrossRef] [PubMed]
- Stecklein, S.R.; Kimler, B.F.; Yoder, R.; Schwensen, K.; Staley, J.M.; Khan, Q.J.; O’dea, A.P.; Nye, L.E.; Elia, M.; Heldstab, J.; et al. CtDNA and residual cancer burden are prognostic in triple-negative breast cancer patients with residual disease. npj Breast Cancer 2023, 9, 10. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Ge, J.; Ma, D.; Yu, K. Immune-Activated Regional Lymph Nodes Predict Favorable Survival in Early-Stage Triple-Negative Breast Cancer. Front. Oncol. 2020, 10, 570981. [Google Scholar] [CrossRef]
- Liu, F.; Hardiman, T.; Wu, K.; Quist, J.; Gazinska, P.; Ng, T.; Purushotham, A.; Salgado, R.; Guo, X.; Pinder, S.E.; et al. Systemic immune reaction in axillary lymph nodes adds to tumor-infiltrating lymphocytes in triple-negative breast cancer prognostication. npj Breast Cancer 2021, 7, 86. [Google Scholar] [CrossRef]
- Hong, J.; Rui, W.; Fei, X.; Chen, X.; Shen, K. Association of tumor-infiltrating lymphocytes before and after neoadjuvant chemotherapy with pathological complete response and prognosis in patients with breast cancer. Cancer Med. J. 2021, 10, 7921–7933. [Google Scholar] [CrossRef]
- Oshi, M.; Roy, A.M.; Yan, L.; Sasamoto, M.; Tokumaru, Y.; Wu, R.; Yamada, A.; Yamamoto, S.; Chishima, T.; Narui, K.; et al. Accelerated glycolysis in tumor microenvironment is associated with worse survival in triple-negative but not consistently with ER+/HER2- breast cancer. Am. J. Clin. Cancer Res. 2023, 13, 3041–3054. [Google Scholar]
- Zhao, F.; Miyashita, M.; Hattori, M.; Yoshimatsu, T.; Howard, F.; Kaneva, K.; Jones, R.; Bell, J.S.K.; Fleming, G.F.; Jaskowiak, N.; et al. Racial Disparities in Pathological Complete Response Among Patients Receiving Neoadjuvant Chemotherapy for Early-Stage Breast Cancer. JAMA Netw. Open 2023, 6, e233329. [Google Scholar] [CrossRef] [PubMed]
- Roy, A.M.; Jiang, C.; Yao, S.; Perimbeti, S.; Gandhi, S. Does race influence long-term outcomes after neoadjuvant chemotherapy in breast cancer: A National Cancer Database analysis. J. Clin. Oncol. 2022, 40 (Suppl. S16), 606. [Google Scholar] [CrossRef]
- Abdou, Y.; Attwood, K.; Cheng, T.D.; Yao, S.; Bandera, E.V.; Zirpoli, G.R.; Ondracek, R.P.; Stein, L.; Bshara, W.; Khoury, T.; et al. Racial differences in CD8+ T cell infiltration in breast tumors from Black and White women. Breast Cancer Res. 2020, 22, 62. [Google Scholar] [CrossRef] [PubMed]
- Bansil, S.; Silva, A.; Taniguchi, A.; Wiedmer, C.; Fernandez, M.; Pagano, I.; Vierkoetter, K.; Killeen, J.; Fukui, J. Racial/Ethnic Differences Among Tumor-Infiltrating Lymphocytes in Breast Cancer Tumors. Oncologist 2023, 28, 116–122. [Google Scholar] [CrossRef] [PubMed]
- Li, C.L.; Wu, C.C.; Kan, J.Y.; Chen, F.; Hou, M.; Chuang, C.; Huang, H.; Ou-Yang, F. The impact of age group in breast cancer survival outcome according to neoadjuvant treatment response: A matched case–control study. Kaohsiung J. Med. Sci. 2022, 38, 277–282. [Google Scholar] [CrossRef] [PubMed]
- Loibl, S.; Jackisch, C.; Lederer, B.; Untch, M.; Paepke, S.; Kümmel, S.; Schneeweiss, A.; Huober, J.; Hilfrich, J.; Hanusch, C.; et al. Outcome after neoadjuvant chemotherapy in young breast cancer patients: A pooled analysis of individual patient data from eight prospectively randomized controlled trials. Breast Cancer Res. Treat. 2015, 152, 377–387. [Google Scholar] [CrossRef] [PubMed]
- Chou, H.H.; Kuo, W.L.; Yu, C.C.; Tsai, H.P.; Shen, S.C.; Chu, C.H.; Yu, M.C.; Lo, Y.F.; Dabora, M.A.; Chang, H.K.; et al. Impact of age on pathological complete response and locoregional recurrence in locally advanced breast cancer after neoadjuvant chemotherapy. Biomed. J. 2019, 42, 66–74. [Google Scholar] [CrossRef]
- Wang, X.Q.; Danenberg, E.; Huang, C.; Egle, D.; Callari, M.; Bermejo, B.; Dugo, M.; Zamagni, C.; Thill, M.; Anton, A.; et al. Spatial predictors of immunotherapy response in triple-negative breast cancer. Nature 2023, 621, 868–876. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Trial | Phase | Sample Size | Intervention vs. Control Arm | Endpoints | Pathological Complete Response (Intervention vs. Control Arm) | Pathological Complete Response (Intervention vs. Control Arm) Based on PD-L1 Status |
|---|---|---|---|---|---|---|
| Gianni 2019 [9]/ NeoTRIP Trial | Phase 2 | 280 | Intervention Arm: Neoadjuvant carboplatin AUC 2 (area under the curve) and nab-paclitaxel 125 mg/m2 i.v. on days 1 and 8, along with atezolizumab 1200 mg i.v. on day 1. Both regimens were given every 3 weeks for eight cycles. Control Arm: Neoadjuvant carboplatin AUC 2 and nab-paclitaxel 125 mg/m2 i.v. on days 1 and 8 without atezolizumab. | Primary endpoint: EFS Secondary endpoint: pCR | 48.6% vs. 44.4%; OR: 1.18; 95% CI = 0.74–1.89; p = 0.48 | PD-L1 +: 59.5% vs. 51.9% PD-L1 −: 33.9% vs. 35.4%. |
| Mittendorf 2020 [5]/IMpassion031 | Phase 3 | 333 | Intervention arm: Chemotherapy plus intravenous atezolizumab (at a dose of 840 mg) every two weeks. Control arm: Chemotherapy plus placebo every 2 weeks Chemotherapy consisted of nab-paclitaxell at 125 mg/m2 weekly for 12 weeks, followed by doxorubicin at 60 mg/m2 and cyclophosphamide at 600 mg/m2 every two weeks for eight weeks. | Co-primary endpoints: pCR in intention-to-treat and PD-L-1-positive patients | 58% vs. 41%; 95% CI = 6–27; p = 0.004 | PD-L1 +: 69% vs. 49% PD-L1 −: 48% vs. 34% |
| Schmid 2020 [6]/Keynote-522 | Phase 3 | 1174 | Intervention Arm: Neoadjuvant therapy with four cycles of pembrolizumab (200 mg) every three weeks. Neoadjuvant therapy included paclitaxel (80 mg/m2 of the body-surface area once weekly) and carboplatin (at a dose based on an area under the concentration–time curve of 5 mg/mL/min once every 3 weeks, or 1.5 mg/mL/min once weekly in the first 12 weeks). An additional four cycles of pembrolizumab were administered. Subsequent treatment with doxorubicin (60 mg/m2) or epirubicin (90 mg/m2) with cyclophosphamide (600 mg/m2 once every 3 weeks in the subsequent 12 weeks). Adjuvant pembrolizumababab was administered every three weeks for up to nine cycles. Control Arm: Neoadjuvant therapy (similar to intervention arm) with four cycles of placebo every three weeks. Adjuvant placebo was administered every three weeks for up to nine cycles. | Co-primary endpoints: pCR at the time of definitive surgery and EFS in the intention-to-treat population | 64.8% vs. 51.2%; 95% CI: 5.4 to 21.8; p < 0.001 | PD-L1 +: 68.9% vs. 54.9% PD-L1 −: 45.3% vs. 30.3% |
| Nanda 2020 [7]/I-SPY2 Trial | Phase 2 | 250 | Intervention arm: Pembrolizumab (200 mg i.v. pembrolizumab every 3 weeks for 4 cycles) to standard neoadjuvant chemotherapy. Control arm: Standard neoadjuvant chemotherapy alone. Neoadjuvant chemotherapy in both arms: 80 mg/m2 i.v. paclitaxel weekly for 12 weeks, followed by 4 cycles of 60 mg/m2 doxorubicin plus 600 mg/m2 i.v. cyclophosphamide every 2 to 3 weeks. | Primary endpoint: pCR Secondary endpoints: RCB, 3-year EFS; distant recurrence-free survival | 60% vs. 22% (TNBC); 95% CI: 44 to 75 | Not available |
| Loibl 2019 [8]/ GeparNuevo Trial | Phase 2 | 174 | Intervention arm: ** Durvalumab every 4 weeks with neoadjuvant chemotherapy. Control arm: Placebo with neoadjuvant chemotherapy. Neoadjuvant chemotherapy in both arms: nab-paclitaxenab-paclitaxel weekly for 12 weeks), followed by dose-dense epirubicin 90 mg/m2, and cyclophosphamide 600 mg/m2. | Primary endpoint: pCR | 53.4% (95% CI = 42.5–61.4%) vs. 44.2% (95% CI = 33.5–55.3%; unadjusted continuity corrected χ2p = 0.287 Window phase: 61.0% vs. 41.4%; OR = 2.22; 95% CI = 1.06–4.64; p = 0.035 | PD-L1 +: 58% vs. 50.7% PD-L1 −: 44.4% vs. 18.2% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roy, A.M.; Chintamaneni, S.; Alaklabi, S.; Awada, H.; Attwood, K.; Gandhi, S. Predictors of Complete Pathological Response with Chemoimmunotherapy in Triple-Negative Breast Cancer: A Meta-Analysis. Onco 2024, 4, 1-14. https://doi.org/10.3390/onco4010001
Roy AM, Chintamaneni S, Alaklabi S, Awada H, Attwood K, Gandhi S. Predictors of Complete Pathological Response with Chemoimmunotherapy in Triple-Negative Breast Cancer: A Meta-Analysis. Onco. 2024; 4(1):1-14. https://doi.org/10.3390/onco4010001
Chicago/Turabian StyleRoy, Arya Mariam, Supritha Chintamaneni, Sabah Alaklabi, Hassan Awada, Kristopher Attwood, and Shipra Gandhi. 2024. "Predictors of Complete Pathological Response with Chemoimmunotherapy in Triple-Negative Breast Cancer: A Meta-Analysis" Onco 4, no. 1: 1-14. https://doi.org/10.3390/onco4010001
APA StyleRoy, A. M., Chintamaneni, S., Alaklabi, S., Awada, H., Attwood, K., & Gandhi, S. (2024). Predictors of Complete Pathological Response with Chemoimmunotherapy in Triple-Negative Breast Cancer: A Meta-Analysis. Onco, 4(1), 1-14. https://doi.org/10.3390/onco4010001