
Metalinguistic Awareness as Self-Management in People with Apraxia of Speech and Aphasia: Lived Experience from a Longitudinal Case Series


Abstract
:
1. Introduction
1.1. Outlining Aphasia and AOS in Spoken Communication
1.2. The Literature about Metalinguistic Skills in Aphasia and AOS
1.3. Self-Management for Long-Term Conditions
1.4. Aims
- (a)
- How did participants characterize their metalinguistic insights about their AOS and aphasia?
- (b)
- Did they attribute therapeutic relevance to their insights?
- (c)
- What are the implications for clinical practice?
1.5. Researcher Experience and Reflexivity
2. Materials and Methods
2.1. Ethical Considerations
2.2. Recruitment
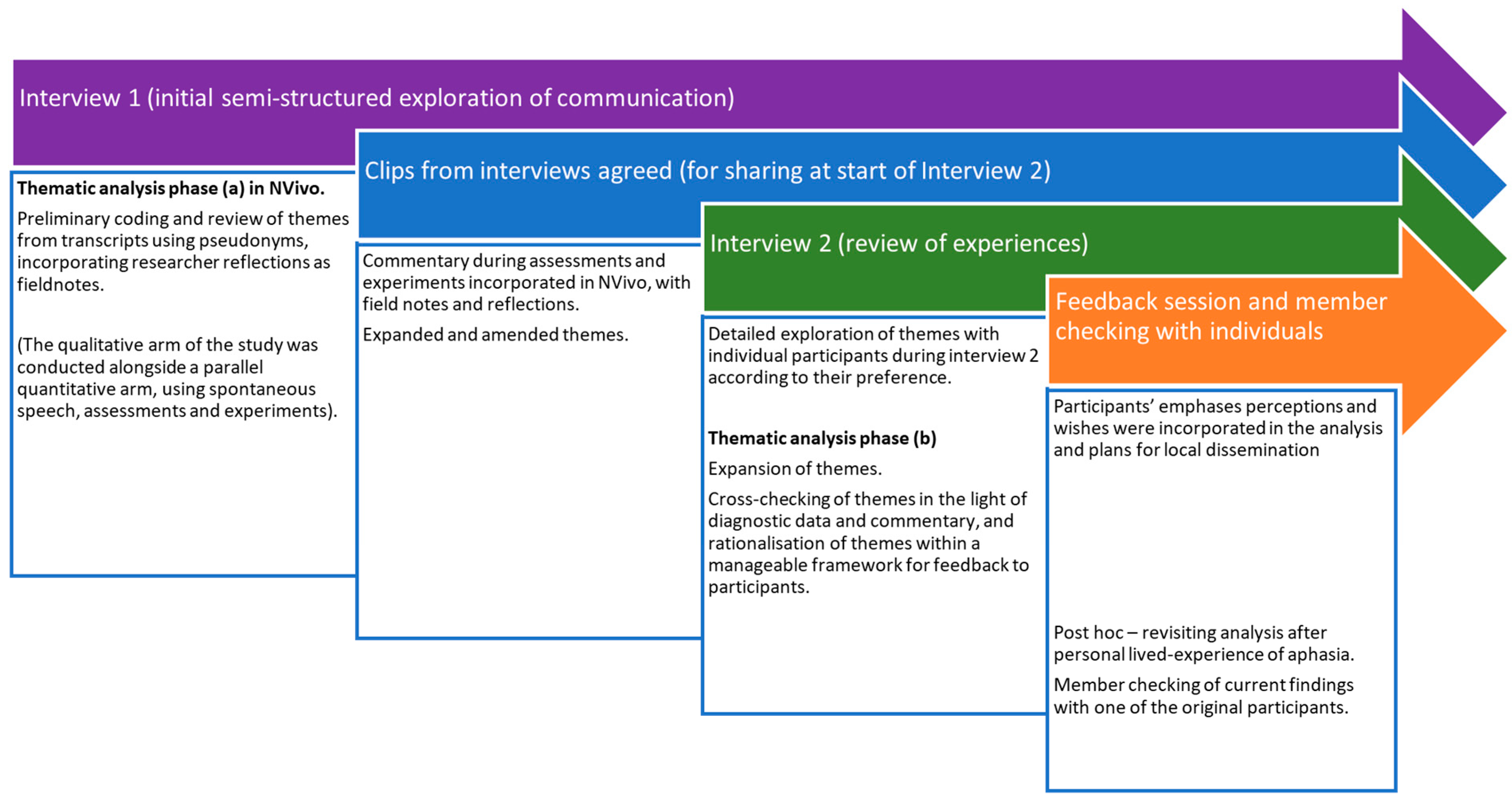
2.3. Data Collection and Analysis
- (1)
- An initial in-depth semi-structured video interview (Interview 1, see Section 2.4).
- (2)
- Multiple assessment visits in which they were encouraged to reflect, using neutral questions such as ‘How did that feel?’ ‘What happened there?’ K.M. also checked at the time that she had understood what the participant meant, using yes/no questions, gestures, and written cross-checking. The occurrence of a breakdown in spoken communication (errors of any kind) prompted extra commentary from them. The assessments used the sort of tests available in routine SLT practice.
- (3)
- Participation in experimental studies of repetition and reading, during which they were encouraged to volunteer comments.
- (4)
- Agreeing a video clip from Interview 1 to share with other participants (see Section 2.5).
- (5)
- A second interview in response to viewing the compiled video clips (see Section 2.6).
- (6)
- A feedback session where the overall findings were shared (see Section 2.7).
2.4. Interview 1
2.5. Rationale for Selecting the Video Clips
2.6. Interview 2 and Overall Analysis
2.7. Methodological Rigour
3. Results (Thematic Analysis)
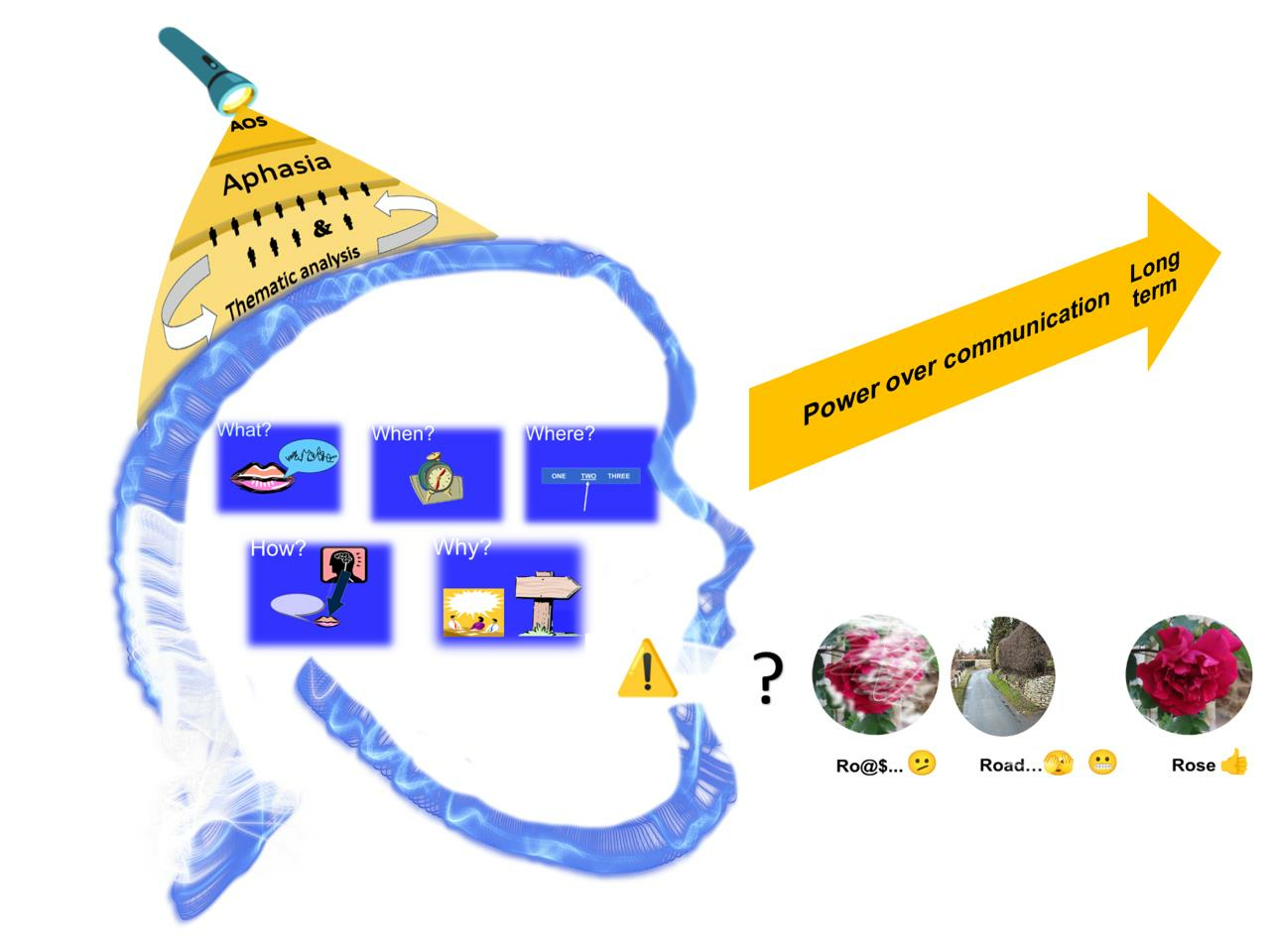
3.1. Metalinguistic Awareness of Spoken Communication Breakdown
3.1.1. Theme: What (Nature)
- L.D.:
- I’m accept it now … erm (-) but impatient (slaps table)
- C.E.:
- he’s a bit thick (circular gesture on side of head) … and that was bad … and that … and I-I-I didn’ like that … but you see I couldn’t … I couldn’t say … and that was that … and that was hard
3.1.2. Theme: When (Occurrence)
- L.D.:
- but er (-) (sighs) a wife and a husband (-) a crying (-) and laughing as well (gestures hands clasped) … erm (-) indignity ‘o things
3.1.3. Theme: Where (Context)
- B.G.:
- I can only er (-) (sighs) say certain words and er (-) er … slow-slowly (indicating communication card explaining his difficulties) and this one a (.) godsend to me
- A.S.:
- when it’s, it’s, it’s er a nay er (-) a verb … it’s (gestures palms moving apart), it’s um … it isn’t as simple (-) as a noun … with the with the noun … it’s very positive what it is … but with the vo-verb it’s the … the sense (-) can be conveyed not so easily
- B.S.:
- I don’t do this … because I ca-can’t do it any more … I could read when I was a kid … but now it can’t … I don’t seem to be very good today (-) ‘cause I can’t make that … I don’t kno-know at all
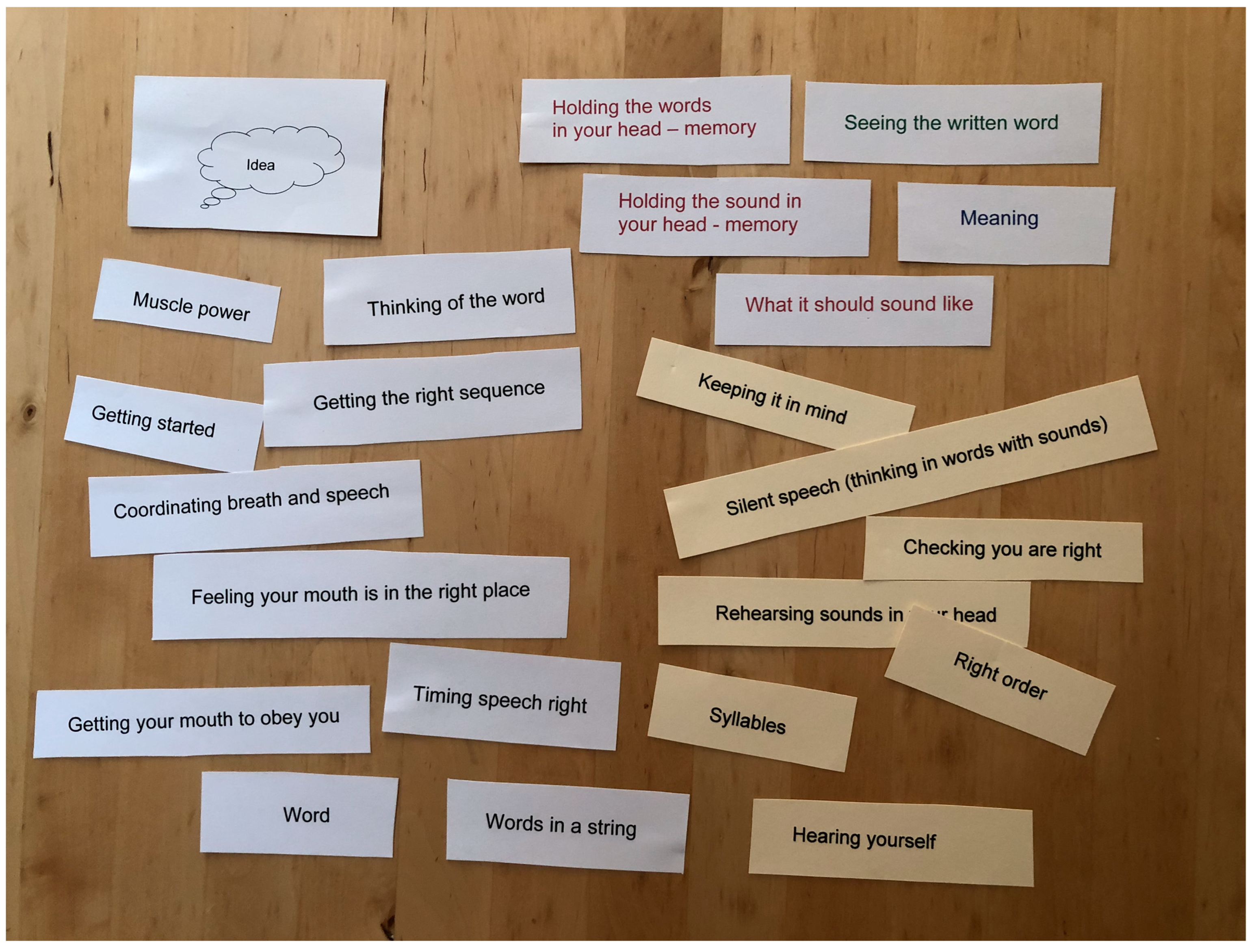
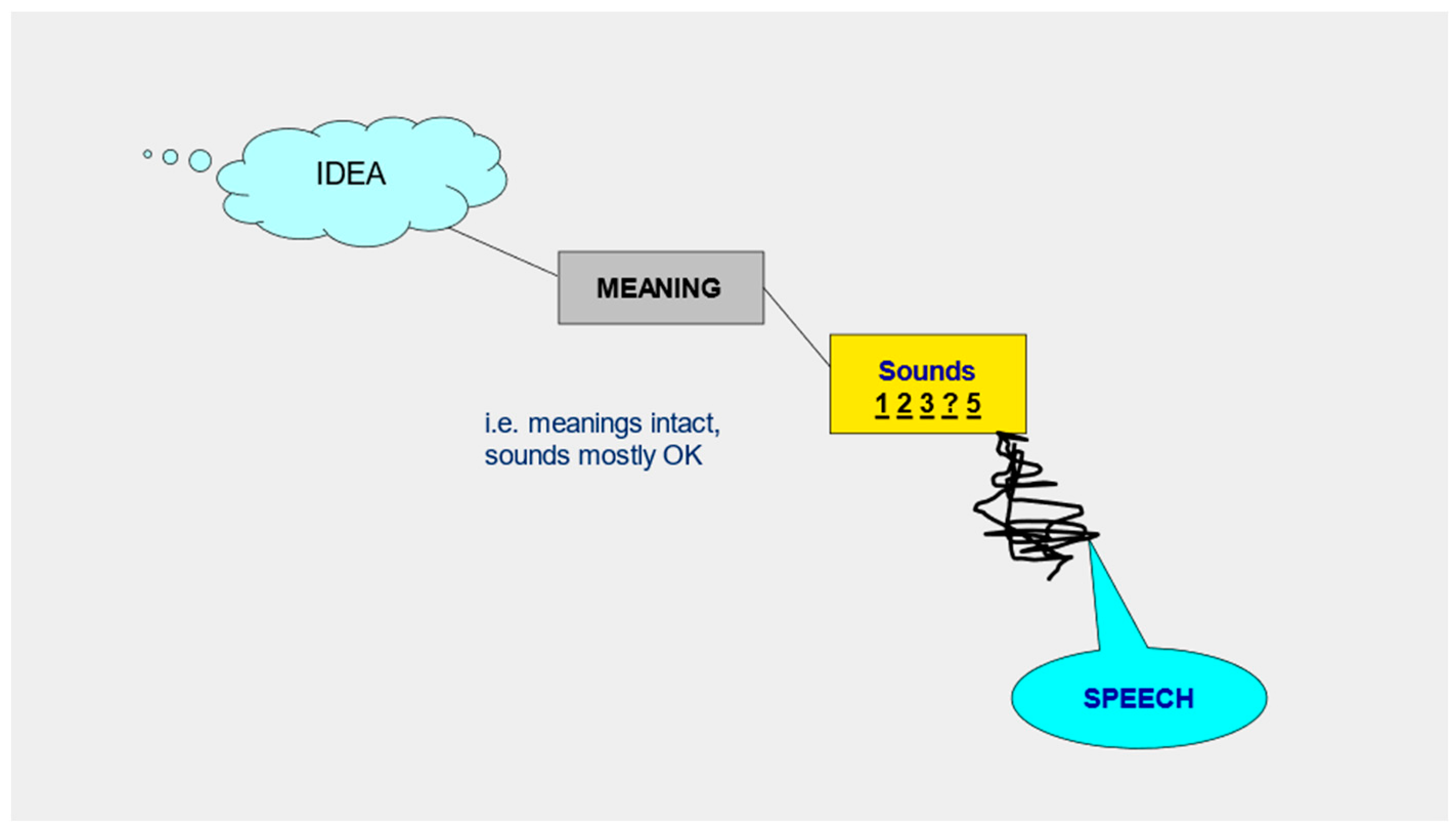
3.1.4. Theme: How (Mechanism)
- B.S.:
- the only thing I can say is that … that I in here (-) knows what it is (points to both sides of head) but (-) when I have to take this (point to back of head) … if er whatever it is … a-a-a-and (-) go here to here (points form head to mouth) … I cannot … there is nothing … there’s something either er … it, it doesn’t go any anywhere (opens hands) … or … it’s er i-it is something which erm I say to myself that ‘you know … what this is’ (points into mouth) (-) but you can’t tell it (points out of mouth)
- K.M.:
- so (-) can you describe to me what’s happening? when when it’s difficult?
- J.R.:
- ooh erm … it ‘ere (points to left side of head) … it not com(.)ing (--) out (points to mouth)
- K.M.:
- yes
- J.R.:
- yeah
- K.M.:
- you got it in your head
- J.R.:
- yeah … a but i’ it won’t (-) (significant effort) come
- J.R.:
- everything (-) in there (points to side of head)
- K.M.:
- even the sounds
- J.R.:
- yes
- K.M.:
- but when you come to say it
- J.R.:
- it won’t come out (gestures from mouth rhythmically 3 times)
- K.M.:
- when you said to me before that you’d got magpies in your head
- J.R.:
- yes
- K.M.:
- is that
- J.R.:
- yes
- K.M.:
- echoing round?
- J.R.:
- yes, yes
- K.M.:
- and it’s
- J.R.:
- and I’m trying to (points with both fingers to sides of head) … you know get you to ‘tame’ (circular repeated gesture forwards with left hand) … trying to get (.) the (.) same difference
- K.M.:
- mm (nods) yes
- J.R.:
- because otherwise it won’t come
- K.M.:
- when you’re saying in unison with me …we’re both talking at the same time
- J.R.:
- yes
- K.M.:
- you’re fine aren’t you
- J.R.:
- yes
- K.M.:
- it’s where you have to keep it in your head
- J.R.:
- (points to her head) yes
- K.M.:
- and then say it
- J.R.:
- yes, yes
- J.R.:
- ye-ye-ye-yes (points to side of head, then both sides) … because no-not (-) it (-) really listening in here … ‘come on’
3.1.5. Theme: Why (Purpose)
- J.R.:
- but why is it the coming out? (points out of mouth)
- L.D.:
- I can’t speak anyway (hand across chest)(-) but um (gestures left hand … across) a baby … but um (-) every day mmmm (looks deliberately from left to right and back) … what’s going on (-) inside of a mind (left hand towards left side of head)
- D.R.:
- er because (-) er (-) because I will go to one two three different words that I might be taking … and in the end (-) I can’t (-) worked out how to do this … and so (-) I’ll go (-) you know one those three (-) … go to the one I need … that I can get
- C.E.:
- I know the words … mm … I went … I’m talking about writing wrong … that … the word is wrong
- K.M.:
- so your spellings
- C.E.:
- that’s right … and sometimes … that was all right … that was all right … but it’s, it’s the middle
- K.M.:
- so when you spell a word … the beginning and the end are OK
- C.E.:
- yeah
- K.M.:
- but the middle is where it’s likely to go wrong
- C.E.:
- yeah
- R.G.:
- it’s as same(-) having someone (-) who knows wh-what they go, you going through
- B.S.:
- I looked (-) out a different person
- K.M.:
- when you see yourself
- B.S.:
- was me … yeah … it was me … but this other person there (-) he’s n-that isn’t me … but the … I-I felt (laughs) I felt (sighs) … I-s er-tr (-) well I-s er-ss … was (-) not (-) not ill
3.2. Self Management
3.2.1. Metalinguistic Awareness at Multiple Levels
3.2.2. Processing Load
3.2.3. Empowerment
3.3. Therapeutic Assessment
4. Discussion
4.1. Clinical Applications
- (A)
- Linguistic load—choosing to use short words, slow rate, selecting frequent and concrete word forms, and simple grammar.
- (B)
- Cognitive load—reducing the competing demands on memory and attention; making use of additional modalities such as reading to enhance production; and enabling practice towards automaticity.
- (C)
- Environmental stress—through ‘calming’ and relaxation; reducing tiredness and fatigue; and educating ‘other people’ to respond well.
4.2. Rigour and Limitations
4.3. Future Directions
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participant | Gender (M/F) | Age | Months Post-Stroke at 1st Contact | Lesion Site from CT Scan (All Left Hemisphere; (h) Indicates Hematoma) | Previous Occupation |
|---|---|---|---|---|---|
| L.D. | F | 45 | 42 | frontoparietal and temporoparietal (h) | Nursing sister |
| B.G. | M | 68 | 30 | parietal | Factory worker |
| J.R. | F | 57 | 23 | frontoparietal | Care worker |
| M.L. | M | 56 | 97 | (no details) | Railway worker |
| D.R. | M | 64 | 9 | ‘middle cerebral artery territory’ | Company director |
| B.S. | M | 69 | 9 | temporoparietal (h) | Factory worker |
| C.E. | M | 54 | 24 | temporoparietal and external capsule | Sales representative |
| R.G. | M | 75 | 12 | frontal | Agricultural worker |
| P.Y. | F | 51 | 4 | no details—later found to be progressive | Secretary |
| A.S. | M | 79 | 12 | parietal | Army/civil servant |
| B.J. | M | 65 | 4 | temporal and parietal | Engineer |
| Assessment | Max | Norms | Broca’s | Conduction | Anomic | Group | Pilot | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean (SD) | B.G. | J.R. | M.L. | D.R. | B.S. | C.E. | R.G. | P.Y. | A.S. | B.J. | Mean (SD) | L.D. | ||
| Auditory discrimination (PALPA 4) | 40 | 39 (1.70) | 36 | 40 | 37 | 38 | 37 | 38 | 40 | 38 | 40 | 36 | 38 (1.56) | 39 |
| Non-word repetition (PALPA 8) | 30 | n/a | 14 | 11 | 20 | 23 | 14 | 1 | 23 | 27 | 17 | 26 | 17.6 (7.95) | 27 |
| Non-word reading (PALPA 8) | 30 | n/a | 4 | 1 | 6 | 23 | 15 | 2 | 15 | 13 | 12 | 6 | 9.7 (7.02) | 3 |
| Auditory rhyme judgement (PALPA 15) | 60 | n/a | 57 | 49 | 46 | 57 | 58 | 50 | 58 | 57 | 53 | 41 | 52.6 (5.91) | 51 |
| Written rhyme judgement (PALPA 15) | 60 | 53.12 (5.10) | 45 | 27 | 32 | 50 | 7 | 40 | 55 | 47 | 50 | 41 | 39.4 (14.21) | 40 |
| Auditory synonyms (PALPA 49) | 60 | n/a | 54 | 40 | 52 | 42 | 57 | 41 | 59 | 58 | 60 | 51 | 51.4 (7.75) | 54 |
| Visual synonyms (PALPA 50) | 60 | 56.75 (2.15) | n/t | 34 | 40 | 51 | 58 | 55 | n/t | 57 | n/t | 51 | 49.43 (9.07) | 60 |
| Max | Norms | A.S. | B.G. | B.J. | B.S. | C.E. | D.R. | J.R. | M.L. | P.Y. | R.G. | Mean (SD) | L.D. | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| GRAMMATICAL DOMAIN | |||||||||||||||
| Test for Reception of Grammar (TROG) [58] (taking data from age 12) | Raw score | 80 | 69 | 70 | 75 | 69 | 58 | 59 | 68 | 68 | 73 | 76 | 68.5 (5.99) | 56 | |
| Standard score | 100 (15) | 89 | 82 | n/a | 71 | 55 | 57 | 71 | 57 | 82 | 98 | 73.56 (15.35) | 67 | ||
| Blocks failed | 20 | abnormal if fail > 6 | 3 | 4 | 1 | 6 | 12 | 10 | 7 | 10 | 4 | 2 | 5.9 (3.75) | 7 | |
| Reversible Sentence Comprehension Test [59] | Actions | 10 | 8 to 10 | 10 | 8 | 10 | 9 | 7 | 9 | 9 | 3 | 9 | 10 | 8.4 (2.12) | 6 |
| Non-actions | 10 | 6 to 10 | 3 | 7 | 8 | 6 | 9 | 2 | 7 | 10 | 9 | 9 | 7 (2.67) | 6 | |
| Adjectives | 10 | 7 to 10 | 7 | 6 | 8 | 8 | 4 | 8 | 9 | 9 | 9 | 6 | 7.4 (1.65) | 6 | |
| Prepositions | 10 | 8 to 10 | 10 | 9 | 10 | 10 | 7 | 9 | 10 | 9 | 8 | 10 | 9.2 (1.03) | 8 | |
| Total | 40 | 29 to 40 | 30 | 30 | 36 | 33 | 27 | 28 | 35 | 31 | 35 | 35 | 32 (3.23) | 26 | |
| WORKING MEMORY | |||||||||||||||
| Digit span (auditory) | 7 | n/a | 6 | 5 | 6 | 3 | 1 | 2 | 4 | 4 | 7 | 6 | 4.4 (1.96) | 3 | |
| Matching span (auditory) | 7 | n/a | 7 | 6 | 7 | 6 | 3 | 4 | 5 | 5 | 6 | 7 | 5.6 (1.35) | 7 | |
| Verbal span (auditory–picture) | 12 | n/a | 6 | 5 | 4 | 2 | 3 | 5 | 3 | 3 | 3 | 4 | 3.8 (1.23) | 4 | |
| Corsi blocks (Visuospatial span) | (max forward or back) | 9 | 5 | 5 | 6 | 5 | 5 | 5 | 6 | 5 | 4 | 6 | 5.2 (0.63) | 6 | |
| scaled score | 10 (3.0) | 10 | 13 | 15 | 7 | 8 | 8 | 13 | 6 | 5 | 14 | 9.9 (3.60) | 8 | ||
References
- Code, C.; Petheram, B. Delivering for aphasia. Int. J. Speech-Lang. Pathol. 2011, 13, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, C.; Gittins, M.; Tyson, S.; Vail, A.; Conroy, P.; Paley, L.; Bowen, A. Prevalence of aphasia and dysarthria among inpatient stroke survivors: Describing the population, therapy provision and outcomes on discharge. Aphasiology 2020, 35, 950–960. [Google Scholar] [CrossRef]
- Dronkers, N. A new brain region for coordinating speech articulation. Nature 1996, 384, 159–161. [Google Scholar] [CrossRef] [PubMed]
- Mumby, K. An Investigation of Apraxia of Speech and Grammar in Connected Speech Following Stroke. Ph.D. Thesis, The University of Manchester, Manchester, UK, 2008. Available online: https://www.librarysearch.manchester.ac.uk/permalink/44MAN_INST/1r887gn/alma992983072351601631 (accessed on 18 July 2023).
- Molloy, J.; Jagoe, C. Use of diverse diagnostic criteria for acquired apraxia of speech: A scoping review. Int. J. Lang. Commun. Disord. 2019, 54, 875–893. [Google Scholar] [CrossRef]
- Code, C. Contemporary issues in apraxia of speech. Aphasiology 2021, 35, 391–396. [Google Scholar] [CrossRef]
- Brady, M.C.; Kelly, H.; Godwin, J.; Enderby, P.; Campbell, P. Speech and language therapy for aphasia following stroke. Cochrane Database Syst. Rev. 2016, 6, CD000425. [Google Scholar] [CrossRef]
- West, C.; Hesketh, A.; Bowen, A. Interventions for apraxia of speech following stroke. Cochrane Database Syst. Rev. 2005, 4, CD004298. [Google Scholar] [CrossRef]
- Biedermann, B.; Fieder, N.; Nickels, L. Spoken Word Production: Processes and Potential Breakdown. In Handbook of Communication Disorders. Theoretical, Empirical, and Applied Linguistics Perspectives; Bar-On, A., Ravid, D., Eds.; De Gruyter Mouton: Berlin, Germany; Boston, MA, USA, 2015; pp. 155–177. [Google Scholar]
- Duffy, J. Motor Speech Disorders: Substrates, Differential Diagnosis and Management, 2nd ed.; Elsevier: Amsterdam, The Netherlands; Mosby: St. Louis, MO, USA, 2005; pp. 307–334. [Google Scholar]
- Basilakos, A.; Yourganov, G.; den Ouden, D.; Fogerty, D.; Rorden, C.; Feenaughty, L.; Fridrikssona, J. A Multivariate Analytic Approach to the Differential Diagnosis of Apraxia of Speech. J. Speech Lang. Hear. Res. 2017, 60, 3369–3681. [Google Scholar] [CrossRef]
- Whitworth, A.; Webster, J.; Howard, D. Assessment and Intervention in Aphasia; Psychology Press: East Sussex, UK, 2005. [Google Scholar]
- Hernández-Sacristán, C.; Rosell-Clari, V.; Serra-Alegre, E.; Quiles-Climent, J. On natural metalinguistic abilities in aphasia: A preliminary study. Aphasiology 2012, 26, 199–219. [Google Scholar] [CrossRef]
- Rigaudeau-McKenna, B. Metalinguistic awareness in a case of early-adolescent dysphasia. Clin. Linguist. Phon. 1998, 12, 281–304. [Google Scholar] [CrossRef]
- Caplan, D.; Waters, G. On the Nature of the Phonological Output Planning Processes Involved in Verbal Rehearsal—Evidence from Aphasia. Brain Lang. 1995, 48, 191–220. [Google Scholar] [CrossRef] [PubMed]
- Fama, M.; Snider, S.; Henderson, M.; Hayward, W.; Friedman, R.; Turkeltaub, P. The Subjective Experience of Inner Speech in Aphasia Is a Meaningful Reflection of Lexical Retrieval. J. Speech Lang. Hear. Res. 2019, 62, 106–122. [Google Scholar] [CrossRef] [PubMed]
- Fama, M.; Lemonds, E.; Levinson, G. The Subjective Experience of Word-Finding Difficulties in People with Aphasia: A Thematic Analysis of Interview Data. Am. J. Speech-Lang. Pathol. 2022, 31, 3–11. [Google Scholar] [CrossRef]
- Johansson, M.B.; Carlsson, M.; Sonnander, K. Communication difficulties and the use of communication strategies: From the perspective of individuals with aphasia. Int. J. Lang. Commun. Disord. 2012, 47, 144–155. [Google Scholar] [CrossRef] [PubMed]
- Nickels, L. Spoken Word Production and Its Breakdown in Aphasia; Psychology Press: East Sussex, UK, 1997. [Google Scholar]
- Nickels, L. The autocue? Self-generated phonemic cues in the treatment of a disorder of reading and naming. Cogn. Neuropsychol. 1992, 9, 155–182. [Google Scholar] [CrossRef]
- DeDe, G.; Parris, D.; Waters, G. Teaching self-cues: A treatment approach for verbal naming. Aphasiology 2003, 17, 465–480. [Google Scholar] [CrossRef]
- Tkaczyk, V. How to turn interior monologues inside out: Epistemologies, methods, and research tools in the long twentieth century. Sound Stud. 2020, 6, 130–152. [Google Scholar] [CrossRef]
- Whiteside, S.; Inglis, A.; Dyson, L.; Roper, A.; Harbottle, A.; Ryder, J.; Cowell, P.; Varley, R. Error reduction therapy in reducing struggle and grope behaviours in apraxia of speech. Neuropsychol. Rehabil. 2012, 22, 267–294. [Google Scholar] [CrossRef]
- Van der Merwe, A. Self-correction in apraxia of speech: The effect of treatment. Aphasiology 2007, 21, 658–669. [Google Scholar] [CrossRef]
- Choe, Y.-K.; Azuma, T.; Mathy, P.; Liss, J.; Edgar, J. The effect of home computer practice on naming in individuals with nonfluent aphasia and verbal apraxia. J. Med. Speech-Lang. Pathol. 2007, 15, 407–421. [Google Scholar]
- Barrow, R. Listening to the voice of living life with aphasia: Anne’s story. Int. J. Lang. Commun. Disord. 2008, 43, 30–46. [Google Scholar] [CrossRef] [PubMed]
- Douglas, J.T. My experience of living with nonfluent/agrammatic variant primary progressive aphasia: Challenges, compensatory strategies and adaptations. Int. J. Lang. Commun. Disord. 2023, 58, 542–554. [Google Scholar] [CrossRef] [PubMed]
- Barnes, R.; Warren, J. Shouting from far away: Three poems about living with speechlessness. Pract. Neurol. 2023, 23, 176–177. [Google Scholar] [CrossRef] [PubMed]
- Haley, K.; Shafer, J.; Harmon, T.; Jacks, A. Recovering with Acquired Apraxia of Speech: The First 2 Years. Am. J. Speech-Lang. Pathol. 2016, 25, S687–S696. [Google Scholar] [CrossRef]
- Brown, K.; Worrall, L.; Davidson, B.; Howe, T. Snapshots of success: An insider perspective on living successfully with aphasia. Aphasiology 2010, 24, 1267–1295. [Google Scholar] [CrossRef]
- Wray, F.; Clarke, D. Longer-term needs of stroke survivors with communication difficulties living in the community: A systematic review and thematic synthesis of qualitative studies. BMJ Open 2017, 7, e017944. [Google Scholar] [CrossRef]
- National Clinical Guideline for Stroke for the UK and Ireland; Intercollegiate Stroke Working Party: London, UK, 2023; Available online: www.strokeguideline.org (accessed on 12 July 2023).
- Kersey, J.; Evans, W.; Mullen, K.; Askren, A.; Cavanaugh, R.; Wallace, S.; Hula, W.; Walsh Dickey, M.; Terhorst, L.; Skidmore, E. Metacognitive Strategy Training Is Feasible for People with Aphasia. Occup. Ther. J. Res. 2021, 41, 309–318. [Google Scholar] [CrossRef]
- Nichol, L.; Hill, A.; Wallace, S.; Pitt, R.; Baker, C.; Rodriguez, A. Self-management of aphasia: A scoping review. Aphasiology 2019, 33, 903–942. [Google Scholar] [CrossRef]
- Holland, A. The value of “communication strategies” in the treatment of aphasia. Aphasiology 2021, 35, 984–994. [Google Scholar] [CrossRef]
- MacKenzie, S.; Mumby, K. (Eds.) Perspectives on Spirituality in Speech and Language Therapy; J & R Press: Havant, UK, 2022. [Google Scholar]
- Glaser, B.; Strauss, A. The Discovery of Grounded Theory: Strategies for Qualitative Research; Aldine: New York, NY, USA, 1967. [Google Scholar]
- Mumby, K.; Bowen, A.; Hesketh, A. Apraxia of speech: How reliable are speech and language therapists’ diagnoses? Clin. Rehabil. 2007, 21, 760–767. [Google Scholar] [CrossRef]
- McNeil, M.; Pratt, S.; Fossett, T. The Differential Diagnosis of Apraxia of Speech. In Speech Motor Control in Normal and Disordered Speech; Maassen, B., Kent, R., Peters, H., van Lieshout, P., Hulstijn, W., Eds.; Oxford University Press: Oxford, UK, 2004; pp. 389–413. [Google Scholar]
- Goodglass, H.; Kaplan, E.; Barresi, B. Boston Diagnostic Aphasia Examination, 3rd ed.; Pro-Ed: Austin, TX, USA, 2001. [Google Scholar]
- Pound, C.; Parr, S.; Lindsay, J.; Woolf, C. Beyond Aphasia: Therapies for Living with Communication Disability; Winslow: Oxon, UK, 2000. [Google Scholar]
- Simmons-Mackie, N.; Kagan, A.; O’Neill Christie, C.; Huijbregts, M.; McEwen, S.; Willems, J. Communicative access and decision making for people with aphasia: Implementing sustainable healthcare systems change. Aphasiology 2007, 21, 39–66. [Google Scholar] [CrossRef]
- Attride-Stirling, J. Thematic networks: An analytic tool for qualitative research. Qual. Res. 2001, 1, 385–405. [Google Scholar] [CrossRef]
- Mumby, K.; Whitworth, A. Adjustment processes in chronic aphasia after stroke: Exploring multiple perspectives in the context of a community-based intervention. Aphasiology 2013, 27, 462–489. [Google Scholar] [CrossRef]
- Simmons-Mackie, N.; Damico, J. Qualitative methods in aphasia research: Ethnography. Aphasiology 1999, 13, 681–687. [Google Scholar] [CrossRef]
- Moran-Ellis, J.; Alexander, V.; Cronin, A.; Dickinson, M.; Fielding, J.; Sleney, J.; Thomas, H. Triangulation and integration: Processes, claims and implications. Qual. Res. 2006, 6, 45–59. [Google Scholar] [CrossRef]
- Mumby, K.; Roddam, H. Aphasia and Spirituality: The feasibility of assessment and intervention using WELLHEAD and SHALOM. Aphasiology 2021, 35, 925–949. [Google Scholar] [CrossRef]
- Miller, N. Apraxia of Speech. In The Characteristics of Aphasia; Code, C., Ed.; Taylor and Francis: London, UK, 1989; pp. 131–154. [Google Scholar]
- Harmon, T.; McDonald, E.; Steele, K. Effects of cognitive and social demands on linguistic production for people with moderate, mild, or no aphasia. Aphasiology 2023. [Google Scholar] [CrossRef]
- Kuptsova, S.; Dragoy, O.; Ivanova, M. Switching attention deficits in post-stroke individuals with different aphasia types. Aphasiology 2023, 37, 260–287. [Google Scholar] [CrossRef]
- Laures-Gore, J.; DuBay, M.; Duff, M.; Buchanan, T. Identifying behavioral measures of stress in individuals with aphasia. J. Speech Lang. Hear. Res. 2010, 53, 1394–1400. [Google Scholar] [CrossRef]
- Manning, M.; MacFarlane, S.; Hickey, A.; Galvin, R.; Franklin, S. Regulating emotional responses to aphasia to re-engage in life: A qualitative interview study. Int. J. Lang. Commun. Disord. 2022, 57, 352–365. [Google Scholar] [CrossRef]
- Richards, H.; Emslie, C. The ‘doctor’ or the ‘girl from the University’? Considering the influence of professional roles on qualitative interviewing. Fam. Pract. 2000, 17, 71–75. [Google Scholar] [CrossRef] [PubMed]
- McCall, J.; DeMarco, A.; Mandal, A.; Fama, M.; van der Stelt, C.; Lacey, E.; Laks, A.; Snider, S.; Friedman, R.; Turkeltaub, P. Listening to Yourself and Watching Your Tongue: Distinct Abilities and Brain Regions for Monitoring Semantic and Phonological Speech Errors. J. Cogn. Neurosci. 2023, 35, 1169–1194. [Google Scholar] [CrossRef] [PubMed]
- Lawton, M.; Haddock, G.; Conroy, P.; Serrant, L.; Sage, K. People with aphasia’s perception of the therapeutic alliance in aphasia rehabilitation post stroke: A thematic analysis. Aphasiology 2018, 32, 1397–1417. [Google Scholar] [CrossRef]
- Tichborne, B.; Liu, F.; Bose, A. Subjective Experience of Word Production Difficulties in Aphasia: A Metaphor Analysis of Autobiographical Accounts. Aphasiology 2023, 1–33. [Google Scholar] [CrossRef]
- Kay, J.; Lesser, R.; Coltheart, M. PALPA: Psycholinguistic Assessments of Language Processing in Aphasia; Lawrence Erlbaum: Hove, UK, 1992. [Google Scholar]
- Bishop, D. Test for the Reception of Grammar (TROG); Medical Research Council: Oxford, UK, 1989. [Google Scholar]
- Marshall, J.; Black, M.; Byng, S. Reversible Sentence Comprehension Test, in Sentence Processing Pack; Bicester: Winslow, UK, 1999. [Google Scholar]
| Rough Timeline | A Summary from Scattered Hand-Written Notes during Recovery from Viral Encephalitis, of Which These Are a Few Excerpts about Metalinguistic Aspects. |
|---|---|
| Early perceptions: | Difficulty with lexical access—needing to use circumlocution. Aware of some semantic paraphasias when they occurred, and others several minutes or even hours later. Some paraphasias were mixed—semantic paraphasias closely related phonetically to the target. Some phonemic errors, usually spotted and corrected at the time just after saying them—as if the internal checking process was inefficient and some errors were escaping that would normally have been corrected prior to production. Spelling errors—alterations in ability to remember spellings of longer irregular words—needing to use a dictionary more often. Sometimes forgetting the meanings of less frequent words I had previously known. Some difficulty constructing complex sentences—I would set off and then have to abandon the thread partway and restart using a different structure (especially when tired). A sense of ‘blank’ where there used to be internal verbalizations. |
| A few months later (retrospective comments shown in brackets): | Sometimes aware of a paraphasia a day or so afterwards! (Like an old-fashioned vending machine where the coin has been inserted but it does not deliver the chocolate bar until you have hit the machine in desperation, turned to go, and then there is a clunk—the transaction had been registered but the mechanism took a long time to respond.) Noticing most often lexical errors seemed to be combined phonologically and semantically related to the target. The interaction between different levels of production—sometimes I would not initiate speech at all because I perceived in advance that the multisyllabic word I wanted was beyond my grasp in the complexity of the grammar I wanted to embark on. This I experienced as utter derailment and it felt like profound failure as if linguistic demands ‘conspired together against me’. (To a conversation partner I seemed unusually quiet, even taciturn, I think.) I had retained the ability for silent rehearsal, yet at this stage in my recovery it prevented me from initiating much. I set myself challenges and became expert at masking my difficulties for limited periods. Written language was extremely tiring on screen, although handwritten notes helped reduce the ‘noise’ of the technology. I still find it harder to read on screen than when printed out, so I have strategically used more printing where possible. |
| Much later: | Words still feel fleeting. When I find one I like in my stream of verbal thoughts, I need to write it down or else I may not retrieve it when I choose to use it next. Despite the challenge, writing academically again has underpinned my recovery. Lengthy conversations were exhausting and still tax me. I have a sense of inefficiency within internal language processing. Now, even 8 years later, I still find that when I have too many competing demands on my cognitive processing (whether immediate or concerning reflection or planning), then I notice paraphasias creeping in again, although now I am able to laugh as I become ‘Mrs Malaprop’ again, and treat myself with a little rest, a little kindness. |
| Participant | AOS Severity | Oral Apraxia | Type of Aphasia (from BDAE) | Aphasia Severity | |
|---|---|---|---|---|---|
| Overall Severity (BDAE Severity 0–5 in Brackets) | Mean Centile from 4 BDAE Subtests (Mean from Full BDAE 2nd Edition in Brackets) | ||||
| L.D. | Mild | Mild | Broca’s | Moderate (2) | 41 (60) |
| B.G. | Mild | None | Broca’s | Mild (3) | 74 (66) |
| J.R. | Moderate | Moderate | Broca’s | Moderate (2) | 38 (56) |
| M.L. | Mild | None | Broca’s | Moderate (1) | 47 (54) |
| D.R. | Mild | None | Conduction | Moderate (2) | 24 (59) |
| B.S. | Moderate | None | Conduction | Moderate (2) | 31 (43) |
| C.E. | Moderate | Mild | Conduction | Moderate (2) | 25 (42) |
| R.G. | Moderate | None | Anomia | Mild (3) | 87 (76) |
| P.Y. | Mild | Mild | Anomia | Mild (4) | 95 (72) |
| A.S. | Mild | None | Anomia | Mild (3) | 77 (70) |
| B.J. | Mild | Mild | Anomia | Mild (4) | 79 (68) |
| Overarching Question | How Do You Communicate? |
|---|---|
| (1) Biographical information | What happened when you had your stroke? How has your life changed? |
| (2) Picture naming and repetition of polysyllabic words | (To elicit apraxic errors for discussion afterwards) |
| (3) Further questions for discussion | What methods do you use to communicate? |
| How do you communicate now? | |
| Are there any problems? | |
| You say ‘x’ is the main problem—did you notice when you did ‘y’ just now? | |
| Can you describe what it feels like? | |
| When are you most likely to make errors? (Time of day/month/year? Situation/activity?) | |
| What makes it better? |
| Themes | Subthemes | Sub-Subthemes | Description of Participant Perceptions | Examples * |
|---|---|---|---|---|
| What Participant identifies an error in their spoken communication | Nature of errors | Struggle | Extra effort required to achieve spoken production, in some cases requiring repeated attempts at the target |
|
| Distortion | Sounds are slurred or unrecognisable |
| ||
| Word finding | Trouble selecting the right word to convey the message, given the constraints on speech production |
| ||
| Rate | Fast delivery noted as associated with errors |
| ||
| Concurrent effects of errors | Frustration | Participants’ errors were compounded by frustration at lack of communication |
| |
| Common ground | Participants enthusiastically identified errors in videos of others that they equated with their own experience |
| ||
| When Participant explanation for when the error occurred | Mood | Fatigue | Some felt errors were more prevalent and worse when fatigued, including after lengthy periods communicating |
|
| Emotional state, humour | Heightened emotional states made errors more likely; humour and laughter helped defuse tension |
| ||
| Context | Time of day | Some participants felt they were better in the morning but experiences varied |
| |
| Situation | Situation in which the communication breakdown happened, such as increased stress, including social situation |
| ||
| Modality | Spontaneous speech | Errors were more likely when saying something spontaneously rather than repeating an automatized phrase said many times. |
| |
| Repetition | Some participants found it easier to repeat speech than to initiate it themselves |
| ||
| Reading aloud | Some participants found having the words written down and reading them aloud improved production |
| ||
| Variability | Unpredictability | Linked with the subtheme of frustration, participants experienced unexpected communication breakdowns |
| |
| Where Participants’ sense of the language context in which the error occurred | Length | - | Difficulty related to how long the target spoken item is |
|
| Frequency | - | Difficulty related to how often the target is spoken |
| |
| Initiation | - | Extra difficulty starting an utterance or word |
| |
| Sounds | - | Specific types of speech sounds may cause more difficulty |
| |
| Grammar | - | Word class or order of words influence errors |
| |
| Order | - | Speech units are out of sequence (sounds or words) |
| |
| How Mechanisms underlying spoken errors | Awareness | Lexical factors | Participant knows they have accessed the word but can’t say it |
|
| Syllables | Awareness of syllable structure of the target word |
| ||
| Memory | Memory of events | Ability to refer to events or messages in the past |
| |
| Retaining items in planning for speech production | Avoiding decay or ‘disappearance’ of the items being processed before the message can be produced |
| ||
| Internal speech | - | Silent internal speech/hearing the word in your head or not |
| |
| Feedback | - | Sensory feedback affecting accuracy |
| |
| Concentration | - | Needing to concentrate to avoid errors, better without distractions such as noise |
| |
| Internal blackboard | - | Seeing the written word in your head |
| |
| Why Rationalization of why communication fails or improves | Physical explanation | - | Explanation based on the physical effects, e.g., of stroke |
|
| Missing link | - | Not catching part of the sequence of the production process; part of the neural mechanism disrupted |
| |
| Why communication is sometimes better (strategies for self- management) | Reading cue | Reading aloud to self to cue own speech |
| |
| Writing cue | Writing down the target word and then trying to say it |
| ||
| Slowing down | Reducing speech rate to reduce the number and severity of errors |
| ||
| Calming | Trying to be calm and relaxed |
| ||
| Other people | Educating others to react well; being with others |
| ||
| Substitution | Using a different word to convey the message |
| ||
| Preparation | Planning speech in advance for a given situation |
| ||
| Practice | Benefit of practising |
| ||
| Blame | Self-blame | Sense of failure |
| |
| Powerlessness | Lack of control and blame of others, circumstances |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mumby, K. Metalinguistic Awareness as Self-Management in People with Apraxia of Speech and Aphasia: Lived Experience from a Longitudinal Case Series. Disabilities 2023, 3, 426-454. https://doi.org/10.3390/disabilities3040028
Mumby K. Metalinguistic Awareness as Self-Management in People with Apraxia of Speech and Aphasia: Lived Experience from a Longitudinal Case Series. Disabilities. 2023; 3(4):426-454. https://doi.org/10.3390/disabilities3040028
Chicago/Turabian StyleMumby, Katharyn. 2023. "Metalinguistic Awareness as Self-Management in People with Apraxia of Speech and Aphasia: Lived Experience from a Longitudinal Case Series" Disabilities 3, no. 4: 426-454. https://doi.org/10.3390/disabilities3040028
APA StyleMumby, K. (2023). Metalinguistic Awareness as Self-Management in People with Apraxia of Speech and Aphasia: Lived Experience from a Longitudinal Case Series. Disabilities, 3(4), 426-454. https://doi.org/10.3390/disabilities3040028