
Cross-Cultural Adaptation and Psychometric Properties of the SF-8 Questionnaire in Tanzanian Swahili for Injury Population

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Instrument
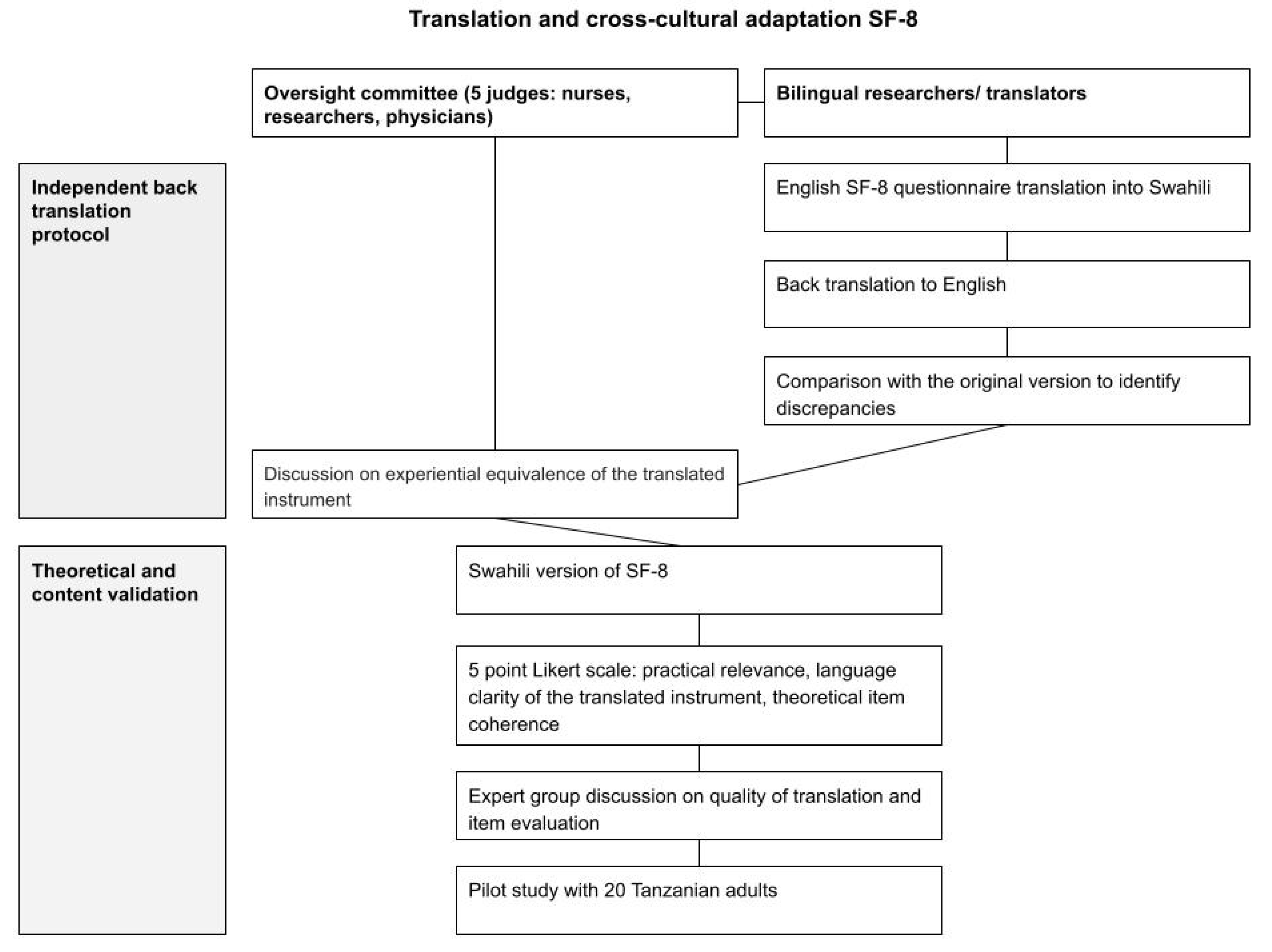
2.3. Translation and Cross-Cultural Adaptation
2.4. Data Collection
2.5. Data Analysis
2.6. Evidence of Validity
2.6.1. Evidence of Validity Based on Content
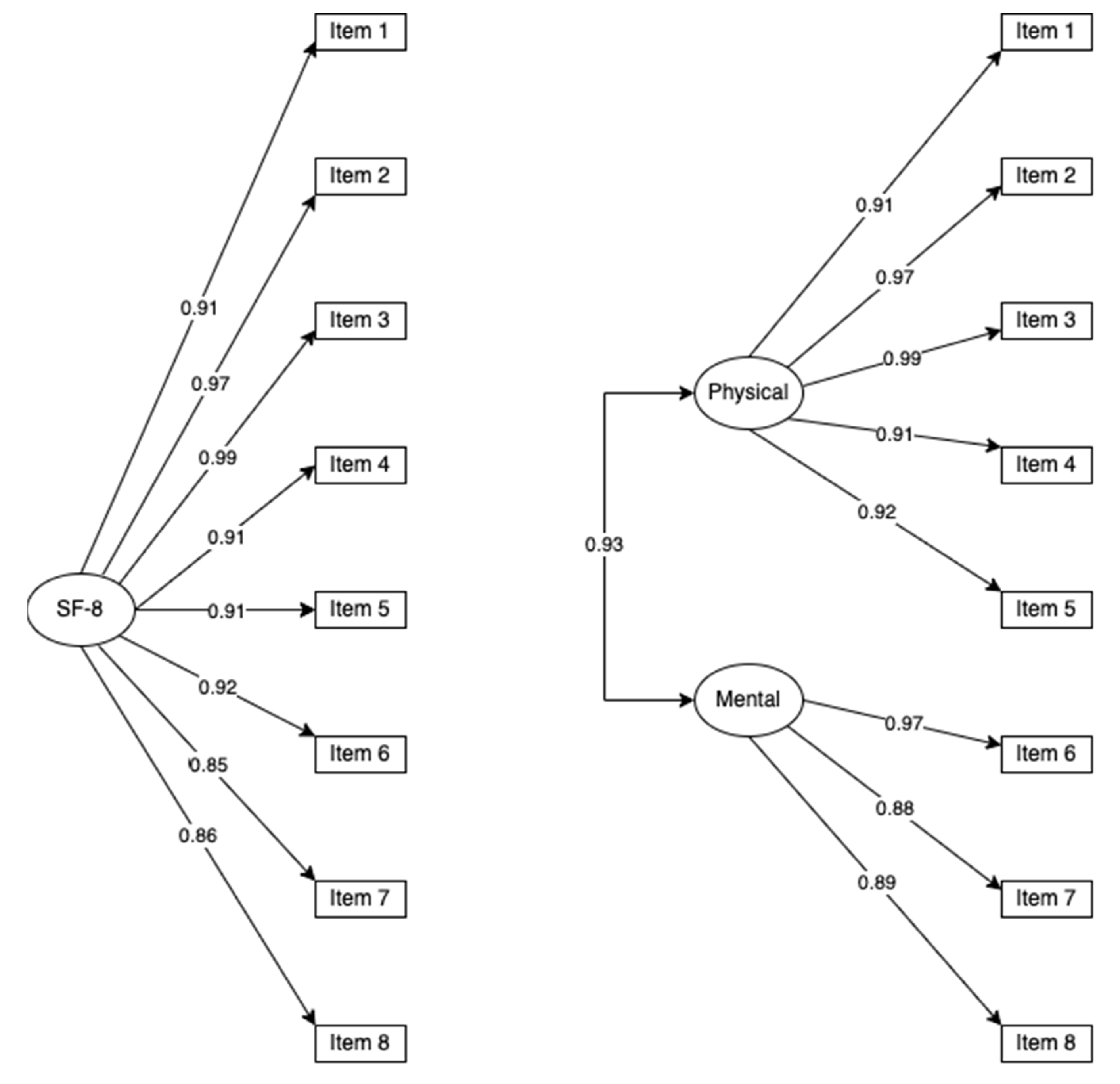
2.6.2. Evidence of Validity Based on Internal Structure
2.6.3. Evidence of Validity Based on Relation to Other Variables
2.7. Multigroup Invariance Analysis
2.8. Evidence of Reliability
3. Results
3.1. Sample Characteristics
3.2. Evidence of Validity Based on Content
3.3. Evidence of Validity Based on Internal Structure
3.4. Reliability Evidence
3.5. Evidence of Validity Based on Relation to Other Variables
3.6. Multi Groups Invariance Evidence
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| SF-8 Items | CVC Score |
|---|---|
| SF-1 | 0.87 |
| SF-2 | 0.87 |
| SF-3 | 0.93 |
| SF-4 | 0.80 |
| SF-5 | 0.93 |
| SF-6 | 0.80 |
| SF-7 | 0.80 |
| SF-8 | 0.80 |
References
- Revicki, D.A.; Kleinman, L.; Cella, D. A history of health-related quality of life outcomes in psychiatry. Dialogues Clin. Neurosci. 2014, 16, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Vallès, J.; Guilera, M.; Briones, Z.; Gomar, C.; Canet, J.; Alonso, J.; ARISCAT Group. Validity of the Spanish 8-item short-form generic health-related quality-of-life questionnaire in surgical patients: A population-based study. Anesthesiology 2010, 112, 1164–1174. [Google Scholar] [CrossRef] [PubMed]
- Beitz, J. Quality-of-life end points in oncology drug trials. Oncology 1999, 13, 1439–1442. [Google Scholar] [PubMed]
- Badia, X.; Herdman, M. The importance of health-related quality-of-life data in determining the value of drug therapy. Clin. Ther. 2001, 23, 168–175. [Google Scholar] [CrossRef]
- Polinder, S.; Haagsma, J.A.; van Klaveren, D.; Steyerberg, E.W.; van Beeck, E.F. Health-related quality of life after TBI: A systematic review of study design, instruments, measurement properties, and outcome. Popul. Health Metr. 2015, 13, 4. [Google Scholar] [CrossRef] [PubMed]
- Fairbairn, K.; May, K.; Yang, Y.; Balasundar, S.; Hefford, C.; Abbott, J.H. Mapping Patient-Specific Functional Scale (PSFS) Items to the International Classification of Functioning, Disability and Health (ICF). Phys. Ther. 2012, 92, 310–317. [Google Scholar] [CrossRef] [PubMed]
- Chandran, A.; Hyder, A.A.; Peek-Asa, C. The Global Burden of Unintentional Injuries and an Agenda for Progress. Epidemiol. Rev. 2010, 32, 110–120. [Google Scholar] [CrossRef] [PubMed]
- Institute for Health Metrics and Evaluation. GBD Results Tool|GHDx [Internet]. GBD Results Tool. 2021. Available online: http://ghdx.healthdata.org/gbd-results-tool (accessed on 23 March 2021).
- Turner-Bowker, D.M.; Bayliss, M.S.; Ware, J.E., Jr.; Kosinski, M. Usefulness of the SF-8 Health Survey for comparing the impact of migraine and other conditions. Qual. Life Res. 2003, 12, 1003–1012. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E.; Kosinki, M.; Dewey, J.; Gandek, B. How to Score and Interpret Single-Item Health Status Measures: A Manual for Users of the SF-8 Health Survey; QualityMetric Inc.: Boston, MA, USA, 2001. [Google Scholar]
- Tokuda, Y.; Okubo, T.; Ohde, S.; Jacobs, J.; Takahashi, O.; Omata, F.; Yanai, H.; Hinohara, S.; Fukui, T. Assessing Items on the SF-8 Japanese Version for Health-Related Quality of Life: A Psychometric Analysis Based on the Nominal Categories Model of Item Response Theory. Value Health 2009, 12, 568–573. [Google Scholar] [CrossRef] [PubMed]
- Roberts, B.; Browne, J.; Ocaka, K.F.; Oyok, T.; Sondorp, E. The reliability and validity of the SF-8 with a conflict-affected population in northern Uganda. Health Qual. Life Outcomes 2008, 6, 108. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Sane, H.; Kulkarni, P.; Yadav, J.; Gokulchandran, N.; Biju, H.; Badhe, P. Cell therapy attempted as a novel approach for chronic traumatic brain injury—A pilot study. SpringerPlus 2015, 4, 26. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Cha, E.-S.; Kim, K.H.; Erlen, J.A. Translation of scales in cross-cultural research: Issues and techniques. J. Adv. Nurs. 2007, 58, 386–395. [Google Scholar] [CrossRef] [PubMed]
- American Educational Research Association, Association AP, National Council on Measurment in Education. Standards for Educational and Psychological Testing; Amer Educational Research Assn: Washington, DC, USA, 2014. [Google Scholar]
- R: The R Project for Statistical Computing. 2021. Available online: https://www.r-project.org/ (accessed on 15 December 2021).
- Anthoine, E.; Moret, L.; Regnault, A.; Sébille, V.; Hardouin, J.-B. Sample size used to validate a scale: A review of publications on newly-developed patient reported outcomes measures. Health Qual. Life Outcomes 2014, 12, 176. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Nieto, R. Contributions to Statistical Analysis: The Coefficients of Proportional Variance, Content Validity and Kappa; BookSurge Publishing: Charleston, SC, USA, 2002. [Google Scholar]
- De Vellis, R.F. Scale Development: Theory and Applications, 2nd ed.; Sage Publications: Thousand Oaks, CA, USA, 2003. [Google Scholar]
- Kline, R.B. Principles and Practice of Structural Equation Modeling, 3rd ed.; Methodology in the Social Sciences; The Guilford Press: New York, NY, USA, 2010. [Google Scholar]
- Byrne, B.M. Structural Equation Modeling with AMOS: Basic Concepts, Applications, and Programming; Routledge: London, UK, 2013. [Google Scholar]
- Hair, J.F.; Babin, B.; Anderson, R.E.; Tatham, R.L. SEM: Confirmatory Factor Analysis. In Multivariate Data Analysis, 6th ed.; Pearson Prentice Hall: Hoboken, NJ, USA, 2006; pp. 770–836. [Google Scholar]
- Nunnally, J.; Bernstein, I. Psychometric Theory, 3rd ed.; McGraw-Hill: New York, NY, USA, 1994. [Google Scholar]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Fawzi, M.C.S.; Ngakongwa, F.; Liu, Y.; Rutayuga, T.; Siril, H.; Somba, M.; Kaaya, S.F. Validating the Patient Health Questionnaire-9 (PHQ-9) for screening of depression in Tanzania. Neurol. Psychiatry Brain Res. 2018, 31, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The Patient Health Questionnaire-2: Validity of a two-item depression screener. Med. Care 2001, 41, 1284–1292. [Google Scholar] [CrossRef] [PubMed]
- Svetina, D.; Rutkowski, L.; Rutkowski, D. Multiple-Group Invariance with Categorical Outcomes Using Updated Guidelines: An Illustration Using M plus and the lavaan/semTools Packages. Struct. Equ. Model. A Multidiscip. J. 2019, 27, 1–20. [Google Scholar] [CrossRef]
- Roach, K.E. Measurement of Health Outcomes: Reliability, Validity and Responsiveness. JPO J. Prosthet. Orthot. 2006, 18, 8–12. [Google Scholar] [CrossRef]
- Lohr, K.N.; Aaronson, N.K.; Alonso, J.; Burnam, M.A.; Patrick, D.L.; Perrin, E.B.; Roberts, J.S. Evaluating quality-of-life and health status instruments: Development of scientific review criteria. Clin. Ther. 1996, 18, 979–992. [Google Scholar] [CrossRef]


| Characteristic | N | N = 1434 |
|---|---|---|
| Age 1 | 1434 | 38.44 (±16.37) |
| Sex | 1427 | |
| Male | 1162 (81%) | |
| Female | 265 (19%) | |
| Marital status | 1422 | |
| Married | 763 (54%) | |
| Not married | 659 (46%) | |
| Occupation | 1421 | |
| Self-employed | 926 (65%) | |
| Employed | 339 (24%) | |
| Other | 102 (7%) | |
| Unemployed | 54 (4%) | |
| Education | 1401 | |
| Primary | 891 (64%) | |
| Secondary | 407 (29%) | |
| University | 103 (7%) | |
| Mechanism of injury | 1433 | |
| Road traffic injury | 909 (63%) | |
| Fall | 237 (17%) | |
| Assault | 198 (14%) | |
| Other | 89 (6%) | |
| Injury severity | 1252 | |
| Mild | 986 (79%) | |
| Moderate | 219 (17%) | |
| Severe | 47 (4%) | |
| Traumatic Brain Injury | 825 | 260 (32%) |
| SF-8 1 Factor Model | SF-8 2 Factor Model | |
|---|---|---|
| Reliability | ||
| Cronbach’s Alpha (CI 95%) | 0.971 (0.968, 0.973) | Physical = 0.964 (0.960, 0.966) |
| Mental = 0.933 (0.926, 0.938) | ||
| Omega McDonald | 0.958 | Physical = 0.940 |
| Mental = 0.839 | ||
| Composite Reliability | 0.968 | Physical = 0.979 |
| Mental = 0.941 | ||
| CFA | ||
| χ2 (df)/p-value | 261.070 (20)/0.000 | 226.599 (19)/0.000 |
| RMSEA (CI 95%) | 0.092 (0.082, 0.100) | 0.087 (0.077, 0.098) |
| TLI | 0.989 | 0.990 |
| CFI | 0.992 | 0.993 |
| NFI | 0.989 | 0.990 |
| Average extracted variance | 0.841 | Physical = 0.888 |
| Mental = 0.833 |
| SF-8 Items | PHQ Item 1 | PHQ Item 2 |
|---|---|---|
| SF-1 | 0.598 | 0.532 |
| SF-2 | 0.615 | 0.638 |
| SF-3 | 0.697 | 0.677 |
| SF-4 | 0.652 | 0.631 |
| SF-5 | 0.573 | 0.530 |
| SF-6 | 0.681 | 0.716 |
| SF-7 | 0.685 | 0.718 |
| SF-8 | 0.727 | 0.750 |
| 1-factor model | 0.490 | 0.450 |
| 2-factors Physical | 0.509 | 0.403 |
| 2-factors Mental | 0.472 | 0.492 |
| Invariance | χ2 | df | RMSEA (90% CI) | CFI | ΔCFI | TLI | |
|---|---|---|---|---|---|---|---|
| By sex | Form | 293.225 | 40 | 0.094 (0.084–0.100) | 0.991 | 0.988 | |
| Loadings | 214.060 | 47 | 0.071 (0.061–0.080) | 0.994 | 0.001 | 0.993 | |
| Variance | 211.273 | 46 | 0.071 (0.061–0.081) | 0.994 | >0.001 | 0.993 | |
| By age | Form | 261.224 | 40 | 0.088 (0.078–0.098) | 0.992 | 0.989 | |
| Loadings | 200.747 | 47 | 0.068 (0.058–0.077) | 0.995 | 0.003 | 0.994 | |
| Variance | 198.102 | 46 | 0.068 (0.058–0.078) | 0.995 | >0.001 | 0.994 |
| Invariance | χ2 | df | RMSEA (90% CI) | CFI | ΔCFI | TLI | |
|---|---|---|---|---|---|---|---|
| By sex | Form | 254.507 | 38 | 0.089 (0.079–0.100) | 0.993 | 0.989 | |
| Loadings | 203.989 | 44 | 0.071 (0.062–0.082) | 0.995 | 0.002 | 0.993 | |
| Variance | 198.311 | 42 | 0.072 (0.062–0.083) | 0.995 | >0.001 | 0.993 | |
| By age | Form | 223.189 | 38 | 0.083 (0.072–0.093) | 0.994 | 0.991 | |
| Loadings | 195.686 | 44 | 0.069 (0.060–0.079) | 0.995 | 0.001 | 0.993 | |
| Variance | 190.199 | 42 | 0.070 (0.060–0.081) | 0.995 | >0.001 | 0.993 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pestillo de Oliveira, L.; Malheiros Caruzzo, N.; Sakita, F.; Mmbaga, B.T.; Boshe, J.; Tupetz, A.; Staton, C.A.; Nickenig Vissoci, J.R. Cross-Cultural Adaptation and Psychometric Properties of the SF-8 Questionnaire in Tanzanian Swahili for Injury Population. Disabilities 2022, 2, 428-438. https://doi.org/10.3390/disabilities2030030
Pestillo de Oliveira L, Malheiros Caruzzo N, Sakita F, Mmbaga BT, Boshe J, Tupetz A, Staton CA, Nickenig Vissoci JR. Cross-Cultural Adaptation and Psychometric Properties of the SF-8 Questionnaire in Tanzanian Swahili for Injury Population. Disabilities. 2022; 2(3):428-438. https://doi.org/10.3390/disabilities2030030
Chicago/Turabian StylePestillo de Oliveira, Leonardo, Nayara Malheiros Caruzzo, Francis Sakita, Blandina T. Mmbaga, Judith Boshe, Anna Tupetz, Catherine A. Staton, and Joao Ricardo Nickenig Vissoci. 2022. "Cross-Cultural Adaptation and Psychometric Properties of the SF-8 Questionnaire in Tanzanian Swahili for Injury Population" Disabilities 2, no. 3: 428-438. https://doi.org/10.3390/disabilities2030030
APA StylePestillo de Oliveira, L., Malheiros Caruzzo, N., Sakita, F., Mmbaga, B. T., Boshe, J., Tupetz, A., Staton, C. A., & Nickenig Vissoci, J. R. (2022). Cross-Cultural Adaptation and Psychometric Properties of the SF-8 Questionnaire in Tanzanian Swahili for Injury Population. Disabilities, 2(3), 428-438. https://doi.org/10.3390/disabilities2030030