
Satisfying Basic Psychological Needs among People with Complex Support Needs: A Self-Determination Theory-Guided Analysis of Primary Relatives’ Perspectives

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Data Sources and Participants
2.3. Procedures
2.4. Interview and Pilot
2.5. Data Analysis
3. Results
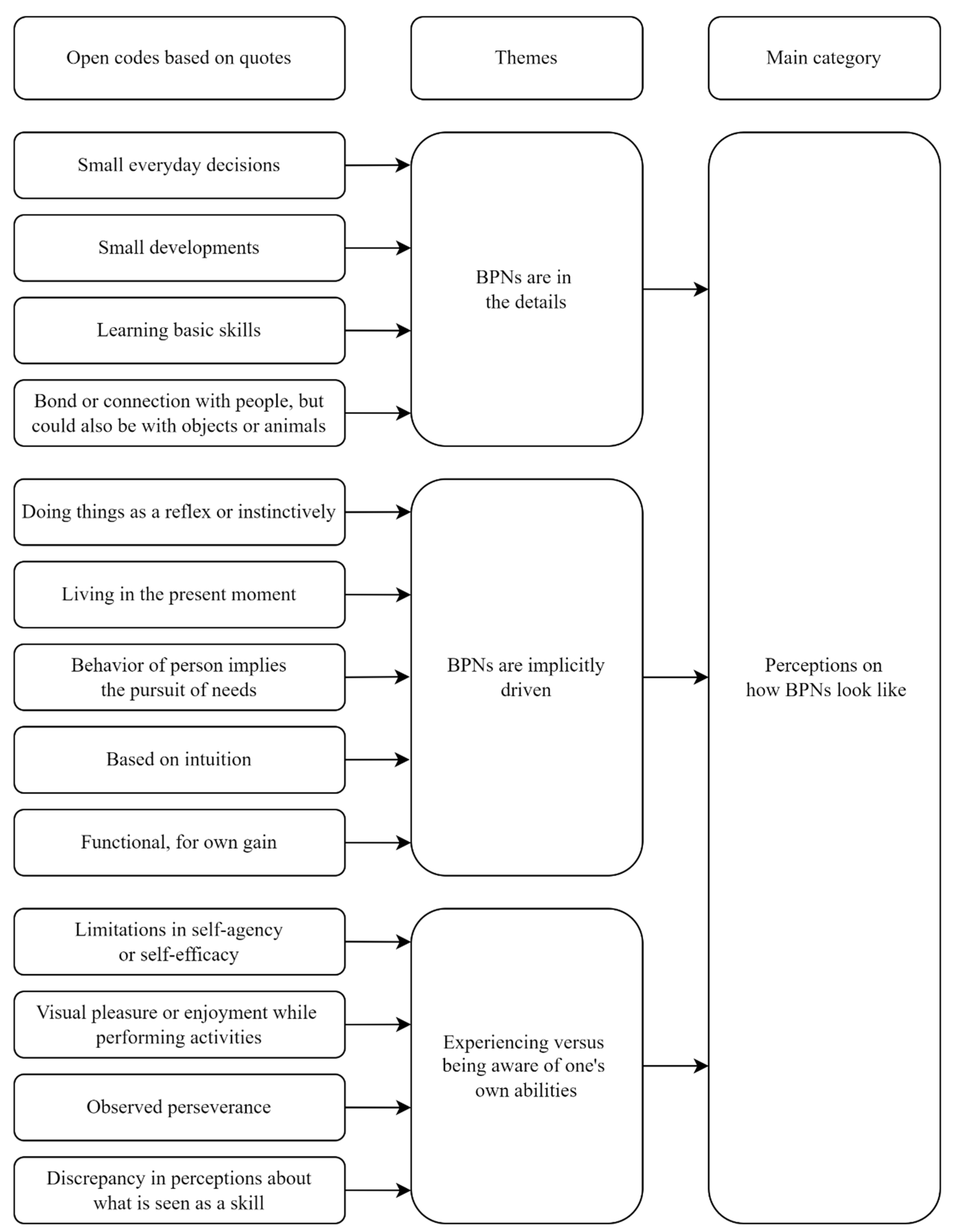
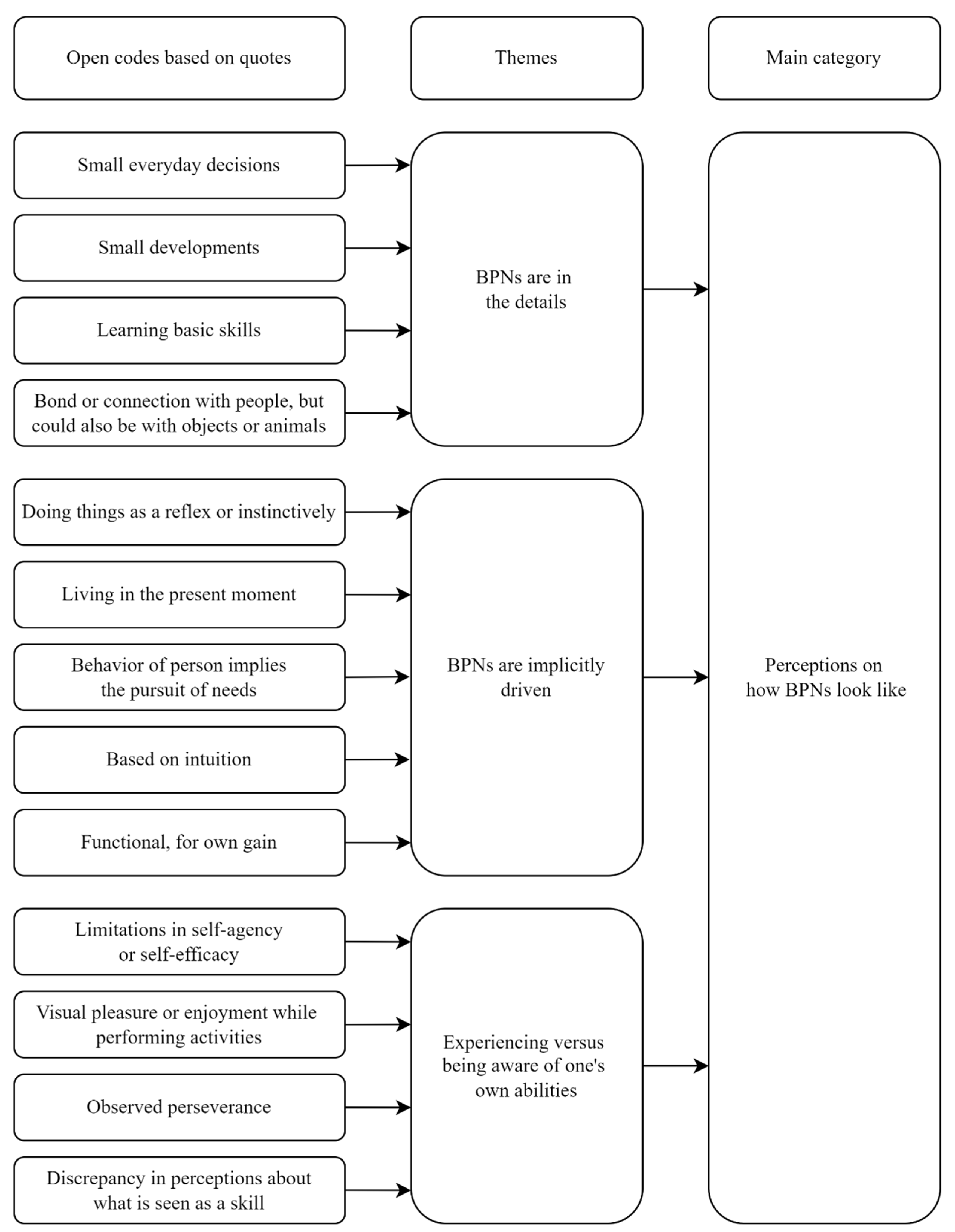
3.1. Primary Relatives’ Perceptions on What the BPNs of Family Members with Complex Support Needs Look Like
3.1.1. BPNs Are All in the Details
When people ask like “what can he do?” I say “he cannot do anything.” Of course we know jolly well what he can do. But I do not need to say to a stranger, like “well he can stand in a standing-frame”, because then they are like “right, he can take a few steps in a walking-frame, whatever”, you know. I just say it very darkly like, “well he cannot do anything.”
3.1.2. BPNs Are Implicitly Driven
What other people think and if they want something too… It just is not there. It is not that she says “that is not important to me”, she just does not see it like that. It just does not exist for her. In fact a tremendously autonomous person. Yeah, autonomous to the core.
A relationship with his support workers, well there you see that it is kind of a family relationship. That he can just be himself (with them) and that they know him and that he has that attachment. That is, the more often he sees people, the more he can just be himself and find his own way in it.
3.1.3. Experiencing versus Being Aware of One’s Own Abilities
If you let (name of daughter) help you bake a cake or something … she is only able to put two or three things in a pan, but later she will tell someone else that she can bake, that she always does that, which is partly due to her getting a lot of positive feedback like “gosh how good of you (name of daughter),” you know? So (she thinks) “I can do that.” But that does not touch reality.
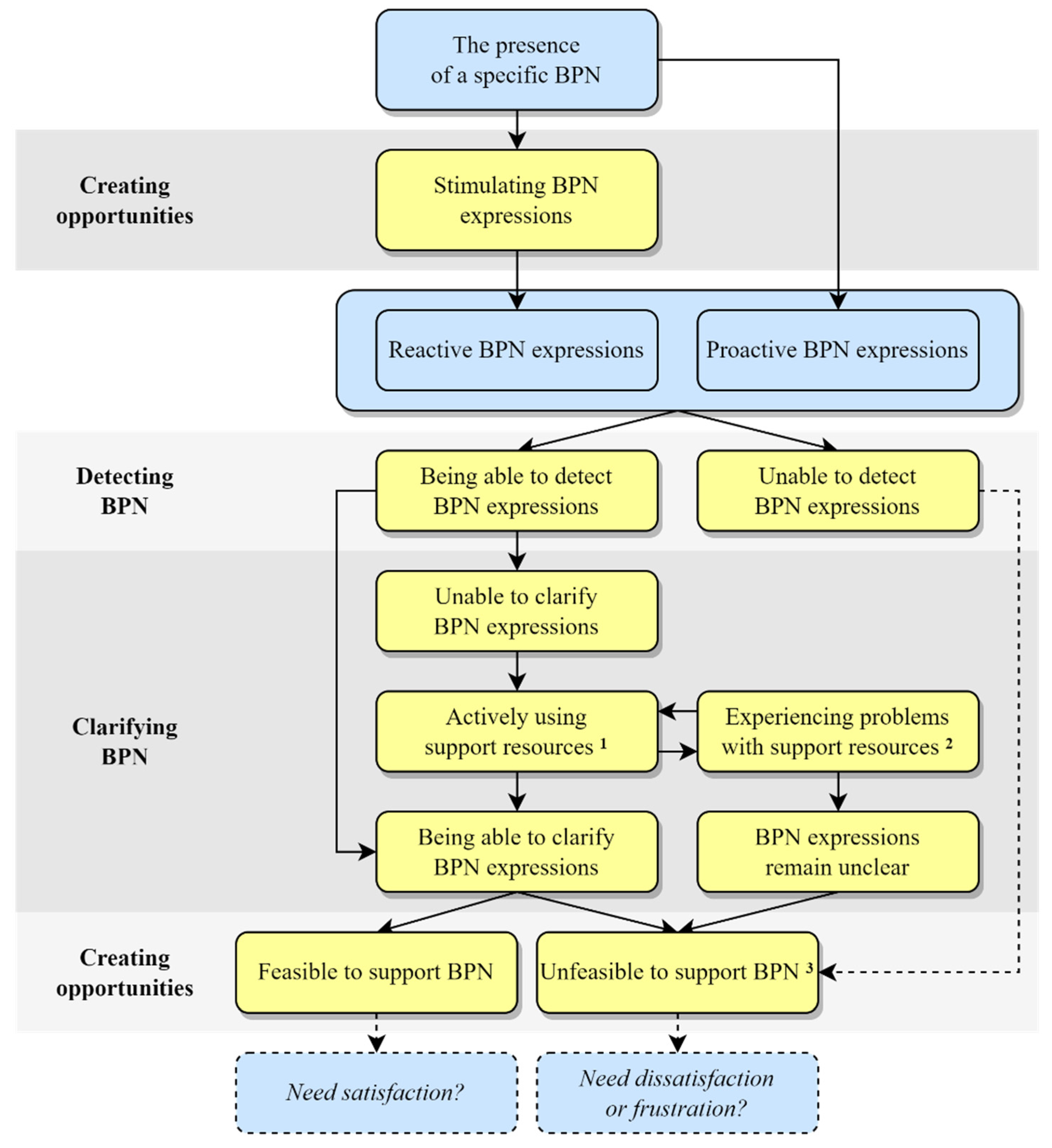
3.2. Primary Relatives’ Perceptions on How Support Processes for the BPNs of Family Members with Complex Support Needs Work
3.2.1. Detecting BPNs
You have to look carefully at his behavior because, for example, if he is at his care-organization performing daytime activities, and he is bored there, then he will start to show difficult behavior, so to speak. Then he will no longer participate, or then he is more difficult for this support workers to handle. Yes, then you can see from his behavior that he is not feeling comfortable in his own skin and that he actually does not agree with what is happening.
3.2.2. Clarifying BPNs
If she cannot make clear what she wants, yeah nice idea autonomy, but I do not think you can do anything with it then … she can then only influence the things she can directly reach herself, she can grab, she can organize … Everything for which she dependents on other people, and that is a lot considering her developmental age, she needs communication for that.
We are working with pictograms, but that is still too challenging for him, but we do offer it to him. I notice myself in practice that I hardly do it, and because it just, yeah, is a fair amount of work and you do not get a response back. So that is pretty difficult … Signs, I did do them in the beginning … When he was only nine months old he got a hearing aid so then I had to use sign language too, but yeah, you can also do sign language to a cat, but they also will not understand it and (name of son) does not understand it either … With (name of son), the level is just too low to use signs. And he would never be able to make a sign back because he does not have the motor skills at all.
3.2.3. Creating Opportunities
I think he has had a walking-frame since he was three and he only now is starting to enjoy it and taking steps in it, but that is a matter of practice, practice, practice. Putting him in it every day at school … And well, yeah, he has his standing-frame, he stands in it every day at school, he practices with that, that is improving too, so yeah, he is developing in that. Just in teeny tiny steps.
If I sing a song when he cries, and I sing a certain song, then he is quiet, and if (name support worker) does that then he is not quiet. So that is well, then you just notice that he so to say, well, has a preference, does feel connected, right, to me, thankfully.
I think the only thing we can go on is, is she acting happy, yes or no. And since she generally behaves as quite happy, shows happiness, we assume that apparently as far as she is concerned the world is okay. But what she would have wanted to do, other than what she is doing now, or how she would have wanted to live her life, I have no idea.
There are also very difficult moments. For example, right before an operation and then say ”I do not want to” (through using her speech computer). You know, she could not say that before. On one hand it is great, but now I have to do something with it.
3.2.4. Tentative Conceptual Framework of BPN Support
4. Discussion
4.1. Implications for Practice
4.2. Limitations and Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chu, S.-Y. Perspectives of Taiwanese families: A preliminary study on promoting self-determination skills of young children with disabilities. Early Child. Educ. J. 2018, 46, 673–681. [Google Scholar] [CrossRef]
- TOP 10 EMB Onderzoeksagenda: De Belangrijkste Vragen van Ouders Aan Onderzoekers. Available online: https://aw-emb.nl/media/EMB_TOP_10_Onderzoeksagenda.pdf (accessed on 20 December 2021).
- Maes, B.; Nijs, S.; Vandesande, S.; Van Keer, I.; Arthur-Kelly, M.; Dind, J.; Goldbart, J.; Petitpierre, G.; Van der Putten, A.A.J. Looking back, looking forward: Methodological challenges and future directions in research on persons with profound intellectual and multiple disabilities. J. Appl. Res. Intellect. Disabil. 2021, 34, 250–262. [Google Scholar] [CrossRef] [PubMed]
- Nakken, H.; Vlaskamp, C. A need for a taxonomy for profound intellectual and multiple disabilities. J. Policy Pract. Intellect. Disabil. 2007, 4, 83–87. [Google Scholar] [CrossRef]
- Luijkx, J.; Van der Putten, A.A.J.; Vlaskamp, C. Time use of parents raising children with severe or profound intellectual and multiple disabilities. Child Care Health Dev. 2017, 43, 518–526. [Google Scholar] [CrossRef] [PubMed]
- Tadema, A.C.; Vlaskamp, C. The time and effort in taking care for children with profound intellectual and multiple disabilities: A study on care load and support. Br. J. Learn. Disabil. 2010, 38, 41–48. [Google Scholar] [CrossRef]
- Vandesande, S.; Bosmans, G.; Maes, B. Can I be your safe haven and secure base? A parental perspective on parent-child attachment in young children with a severe or profound intellectual disability. Res. Dev. Disabil. 2019, 93, 103452. [Google Scholar] [CrossRef]
- Wehmeyer, M.L.; Shogren, K.A.; Little, T.D.; Lopez, S.J. (Eds.) Introduction to the self-determination construct. In Development of Self-Determination through the Life-Course; Springer: Dordrecht, The Netherlands, 2017; pp. 3–16. [Google Scholar]
- Wehmeyer, M.L. Self-determination in adolescents and adults with intellectual and developmental disabilities. Curr. Opin. Psychiatry 2020, 33, 81–85. [Google Scholar] [CrossRef]
- United Nations. Convention on the Rights of Persons with Disabilities; United Nations Headquarters: New York, NY, USA, 2006; Available online: https://www.un.org/disabilities/documents/convention/convention_accessible_pdf.pdf (accessed on 3 December 2019).
- Ryan, R.M.; Deci, E.L. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am. Psychol. 2000, 55, 68–78. [Google Scholar] [CrossRef]
- Adams, N.; Little, T.D.; Ryan, R.M. Self-determination theory. In Development of Self-Determination through the Life-Course; Wehmeyer, M.L., Shogren, K.A., Little, T.D., Lopez, S.J., Eds.; Springer: Dordrecht, The Netherlands, 2017; pp. 47–54. [Google Scholar]
- Shogren, K.A.; Wehmeyer, M.L.; Palmer, S.B. Causal agency theory. In Development of Self-Determination through the Life-Course; Wehmeyer, M.L., Shogren, K.A., Little, T.D., Lopez, S.J., Eds.; Springer: Dordrecht, The Netherlands, 2017; pp. 55–67. [Google Scholar]
- Deci, E.L.; Ryan, R.M. The “what” and “why” of goal pursuits: Human needs and the self-determination of behavior. Psychol. Inq. 2000, 11, 227–268. [Google Scholar] [CrossRef]
- Ryan, R.M.; Deci, E.L. Intrinsic and extrinsic motivations: Classic definitions and new directions. Contemp. Educ. Psychol. 2000, 25, 54–67. [Google Scholar] [CrossRef]
- Ryan, R.M.; Deci, E.L. Self-regulation and the problem of human autonomy: Does psychology need choice, self-determination, and will? J. Pers. 2006, 74, 1557–1586. [Google Scholar] [CrossRef] [PubMed]
- White, R.W. Motivation reconsidered: The concept of competence. Psychol. Rev. 1959, 66, 297–333. [Google Scholar] [CrossRef] [PubMed]
- Baumeister, R.F.; Leary, M.R. The need to belong: Desire for interpersonal attachments as a fundamental human motivation. Psychol. Bull. 1995, 117, 497–529. [Google Scholar] [CrossRef] [PubMed]
- Vansteenkiste, M.; Ryan, R.M.; Soenens, B. Basic psychological need theory: Advancements, critical themes, and future directions. Motiv. Emot. 2020, 44, 1–31. [Google Scholar] [CrossRef] [Green Version]
- Frielink, N.; Schuengel, C.; Embregts, P.J.C.M. Autonomy support, need satisfaction, and motivation for support among adults with intellectual disability: Testing a self-determination theory model. Am. J. Intellect. Dev. Disabil. 2018, 123, 33–49. [Google Scholar] [CrossRef] [Green Version]
- Schalock, R.L.; Verdugo, M.A. Handbook on Quality of Life for Human Service Practitioners; American Association on Mental Retardation: Washington, DC, USA, 2002; pp. 11–30. [Google Scholar]
- Vicente, E.V.; Verdugo, M.A.; Gómez-Vela, M.; Fernández-Pulido, R.; Wehmeyer, M.L.; Guillén, V.M. Personal characteristics and school contextual variables associated with student self-determination in Spanish context. J. Intellect. Dev. Disabil. 2019, 44, 23–34. [Google Scholar] [CrossRef]
- Carter, E.W.; Owens, L.; Trainor, A.A.; Sun, Y.; Swedeen, B. Self-determination skills and opportunities of adolescents with severe intellectual and developmental disabilities. Am. J. Intellect. Dev. Disabil. 2009, 114, 179–192. [Google Scholar] [CrossRef]
- Wehmeyer, M.L.; Abery, B.H.; Zhang, D.; Ward, K.; Willis, D.; Hossain, W.A.; Balcazar, F.; Ball, A.; Bacon, A.; Calkins, C.; et al. Personal self-determination and moderating variables that impact efforts to promote self-determination. Exceptionality 2011, 19, 19–30. [Google Scholar] [CrossRef]
- Wehmeyer, M.L.; Shogren, K.A. Applications of the self-determination construct to disability. In Development of Self-Determination through the Life-Course; Wehmeyer, M.L., Shogren, K.A., Little, T.D., Lopez, S.J., Eds.; Springer: Dordrecht, The Netherlands, 2017; pp. 111–123. [Google Scholar]
- Pelleboer-Gunnink, H.A.; Van Oorsouw, W.M.W.J.; Van Weeghel, J.; Embregts, P.J.C.M. Stigma research in the field of intellectual disabilities: A scoping review on the perspective of care providers. Int. J. Dev. Disabil. 2021, 67, 168–187. [Google Scholar] [CrossRef] [Green Version]
- Martínez-Tur, V.; Moliner, C.; Peñarroja, V.; Gracia, E.; Peiró, J.M. From service quality in organisations to self-determination at home. J. Intellect. Disabil. Res. 2015, 59, 882–890. [Google Scholar] [CrossRef]
- Wehmeyer, M.L. Self-determination and individuals with severe disabilities: Re-examining meanings and misinterpretations. Res. Pract. Persons Severe Disabil. 2005, 30, 113–120. [Google Scholar] [CrossRef]
- Lifshitz, H.; Klein, P.S.; Cohen, S.F. Effects of MISC intervention on cognition, autonomy, and behavioral functioning of adult consumers with severe intellectual disability. Res. Dev. Disabil. 2010, 31, 881–894. [Google Scholar] [CrossRef] [PubMed]
- Dollar, C.A.; Fredrick, L.D.; Alberto, P.A.; Luke, J.K. Using simultaneous prompting to teach independent living and leisure skills to adults with severe intellectual disabilities. Res. Dev. Disabil. 2012, 33, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Moreno, J.; Saldaña, D. Use of a computer-assisted program to improve metacognition in persons with severe intellectual disabilities. Res. Dev. Disabil. 2005, 26, 341–357. [Google Scholar] [CrossRef]
- Roche, L.; Sigafoos, J.; Lancioni, G.E.; O’Reilly, M.F.; Green, V.A. Microswitch technology for enabling self-determined responding in children with profound and multiple disabilities: A systematic review. Augment. Altern. Comm. 2015, 31, 246–258. [Google Scholar] [CrossRef]
- Kruithof, K.; Willems, D.; Van Etten-Jamaludin, F.; Olsman, E. Parents’ knowledge of their child with profound intellectual and multiple disabilities: An interpretative synthesis. J. Appl. Res. Intellect. Disabil. 2020, 33, 1141–1150. [Google Scholar] [CrossRef]
- Deci, E.L.; Ryan, R.M. Self-determination research: Reflections and future directions. In Handbook of Self-Determination Research; University of Rochester Press: Rochester, NY, USA, 2002; pp. 431–441. [Google Scholar]
- Bowen, G.A. Grounded theory and sensitizing concepts. Int. J. Qual. Methods 2006, 5, 12–23. [Google Scholar] [CrossRef]
- Charmaz, K. Constructing Grounded Theory: A Practical Guide through Qualitative Analysis; Sage: London, UK, 2006. [Google Scholar]
- Hall, S.A.; Rossetti, Z. The roles of adult siblings in the lives of people with severe intellectual and developmental disabilities. J. Appl. Res. Intellect. Disabil. 2018, 31, 423–434. [Google Scholar] [CrossRef]
- NVivo Qualitative Data Analysis Software; Version 12; QSR International Pty Ltd.: Melbourne, Australia, 2018.
- Glaser, B.G.; Strauss, A.L. The Discovery of Grounded Theory: Strategies for Qualitative Research; Aldine: New York, NY, USA, 1967. [Google Scholar]
- Corbin, J.; Strauss, A. Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory, 3rd ed.; Sage: Thousand Oaks, CA, USA, 2008. [Google Scholar]
- Bühler, K. Die Geistige Entwicklung des Kindes [The Spiritual Development of the Child], 4th ed.; Gustav Fischer: Jena, Germany, 1924. [Google Scholar]
- Ainsworth, M.D.S.; Blehar, M.C.; Waters, E.; Wall, S. Patterns of Attachment: Observations in the Strange Situation and at Home; Lawrence Erlbaum Associates: Hillsdale, MI, USA, 1978. [Google Scholar]
- Embregts, P.J.C.M.; Negenman, A.; Habraken, J.M.; De Boer, M.E.; Frederiks, B.J.M.; Hertogh, C.M.P.M. Restraint interventions in people with moderate to profound intellectual disabilities: Perspectives of support staff and family members. J. Appl. Res. Intellect. Disabil. 2019, 32, 172–183. [Google Scholar] [CrossRef] [Green Version]
- De Geus-Neelen, K.C.J.M.; Van Oorsouw, W.M.W.J.; Embregts, P.J.C.M. Individueel wonen. Een kans op meer keuzemogelijkheden en minder vrijheidsbeperking voor mensen met een ernstige verstandelijke beperking en gedragsproblemen? [Individual living. A chance of more choice opportunities and less restrictive interventions for people with severe intellectual disabilities and challenging behaviour?]. Orthop. Onderz. Prakt. 2014, 53, 477–492. [Google Scholar]
- De Geus-Neelen, K.C.J.M.; Van Oorsouw, W.M.W.J.; Hendriks, L.A.H.C.; Embregts, P.J.C.M. Perceptions of staff and family of the quality of life of people with severe to profound intellectual disability. J. Intellect. Dev. Disabil. 2019, 44, 42–50. [Google Scholar] [CrossRef] [Green Version]
- Dean, E.E.; Kirby, A.V.; Hagiwara, M.; Shogren, K.A.; Ersan, D.T.; Brown, S. Family role in the development of self-determination for youth with intellectual and developmental disabilities: A scoping review. Intellect. Dev. Disabil. 2021, 59, 315–334. [Google Scholar] [CrossRef] [PubMed]
- Vandesande, S.; Bosmans, G.; Sterkenburg, P.; Schuengel, C.; Maes, B. The Attachment Strengths and Needs Interview for parents of children with severe or profound intellectual disabilities: An acceptability and feasibility study. J. Intellect. Dev. Disabil. 2021, 47, 118–130. [Google Scholar] [CrossRef]
- Anderson, E.E.; Boyd, B.; Qureskhi, N.K.; Stirling, J.M.; McCarthy, V.; Kuczewski, M.G. Operation homefront: Meeting clerkship competencies with home visits to families of children with special needs. Acad. Pediatr. 2019, 19, 170–176. [Google Scholar] [CrossRef] [PubMed]
- Skarsaune, S.K.N.; Hanisch, H.M.; Gjermestad, A. Self-Determination: What can we learn from persons with profound intellectual and multiple disabilities? Scand. J. Disabil. Res. 2021, 23, 317–327. [Google Scholar] [CrossRef]
- Scott, H.M.; Havercamp, S.M. Comparisons of self and proxy report on health-related factors in people with intellectual disability. J. Appl. Res. Intellect. Disabil. 2018, 31, 927–936. [Google Scholar] [CrossRef]
- Janssen, C.G.C.; Voorman, J.M.; Becher, J.G.; Dallmeijer, A.J.; Schuengel, C. Course of health-related quality of life in 9–16-year-old children with cerebral palsy: Associations with gross motor abilities and mental health. Disabil. Rehabil. 2010, 32, 344–351. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Participants | Family Members with Complex Support Needs | ||||||
|---|---|---|---|---|---|---|---|
| Participant Pseudonym | Relationship | Primary Caregiver(s) of Family Member with Complex Support Needs | Primary Caregiver(s) of Others Next to Family Member with Complex Support Needs | Gender | Age Group (Years) | Other Health Issues 1 | Living Arrangement |
| R1 | Mother | √ | √ | Male | Middle childhood (6–12) | √ | Family home |
| R2 | Both parents | √ | √ | Male | Middle childhood (6–12) | √ | Family home |
| R3 | Mother | √ | × | Female | Adult (21+) | √ | Family home |
| R4 | Mother | √ | √ | Female | Adolescence (13–21) | √ | Family home |
| R5 | Mother | √ | √ | Female | Adolescence (13–21) | √ | Family home |
| R6 | Both parents | √ | √ | Male | Middle childhood (6–12) | √ | Family home |
| R7 | Sister | × | - | Male | Adult (21+) | √ | Group home |
| R8 | Sister | √ | × | Female | Adult (21+) | × | Family home |
| R9 | Mother | √ | √ | Female | Adolescence (13–21) | × | Family home |
| No. | Semi-Structured Interview Questions |
|---|---|
| 1. | What does autonomy 1 mean to you/What do you understand by it/How would you describe it? |
| 2. | What do you think autonomy means for (name family member)/What would (name family member) understand by this? |
| 3. | Can you tell me what changes there have been in the need for autonomy from birth to now, and how did you notice that? |
| 4. | How do you notice in (name family member) that he/she feels supported in his/her need for autonomy? |
| 5. | How do you notice in (name family member) that he/she does not feel supported in his/her need for autonomy? |
| 6. | How do you notice when (name family member) needs (more) autonomy? |
| 7. | What do you do to support or stimulate the need for autonomy? |
| 8. | What could healthcare professionals do to support or stimulate the need for autonomy/What possibilities do you see for this? |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Tuyll van Serooskerken, J.M.; Willemen, A.M.; de la Croix, A.; Embregts, P.J.C.M.; Schuengel, C. Satisfying Basic Psychological Needs among People with Complex Support Needs: A Self-Determination Theory-Guided Analysis of Primary Relatives’ Perspectives. Disabilities 2022, 2, 330-347. https://doi.org/10.3390/disabilities2020024
van Tuyll van Serooskerken JM, Willemen AM, de la Croix A, Embregts PJCM, Schuengel C. Satisfying Basic Psychological Needs among People with Complex Support Needs: A Self-Determination Theory-Guided Analysis of Primary Relatives’ Perspectives. Disabilities. 2022; 2(2):330-347. https://doi.org/10.3390/disabilities2020024
Chicago/Turabian Stylevan Tuyll van Serooskerken, Jacqueline M., Agnes M. Willemen, Anne de la Croix, Petri J. C. M. Embregts, and Carlo Schuengel. 2022. "Satisfying Basic Psychological Needs among People with Complex Support Needs: A Self-Determination Theory-Guided Analysis of Primary Relatives’ Perspectives" Disabilities 2, no. 2: 330-347. https://doi.org/10.3390/disabilities2020024
APA Stylevan Tuyll van Serooskerken, J. M., Willemen, A. M., de la Croix, A., Embregts, P. J. C. M., & Schuengel, C. (2022). Satisfying Basic Psychological Needs among People with Complex Support Needs: A Self-Determination Theory-Guided Analysis of Primary Relatives’ Perspectives. Disabilities, 2(2), 330-347. https://doi.org/10.3390/disabilities2020024