
Association between 24 h Urinary Sodium and Potassium Excretion and Dietary Intake in Japanese Male Adolescent Football Players


Abstract
:1. Introduction
2. Materials and Methods
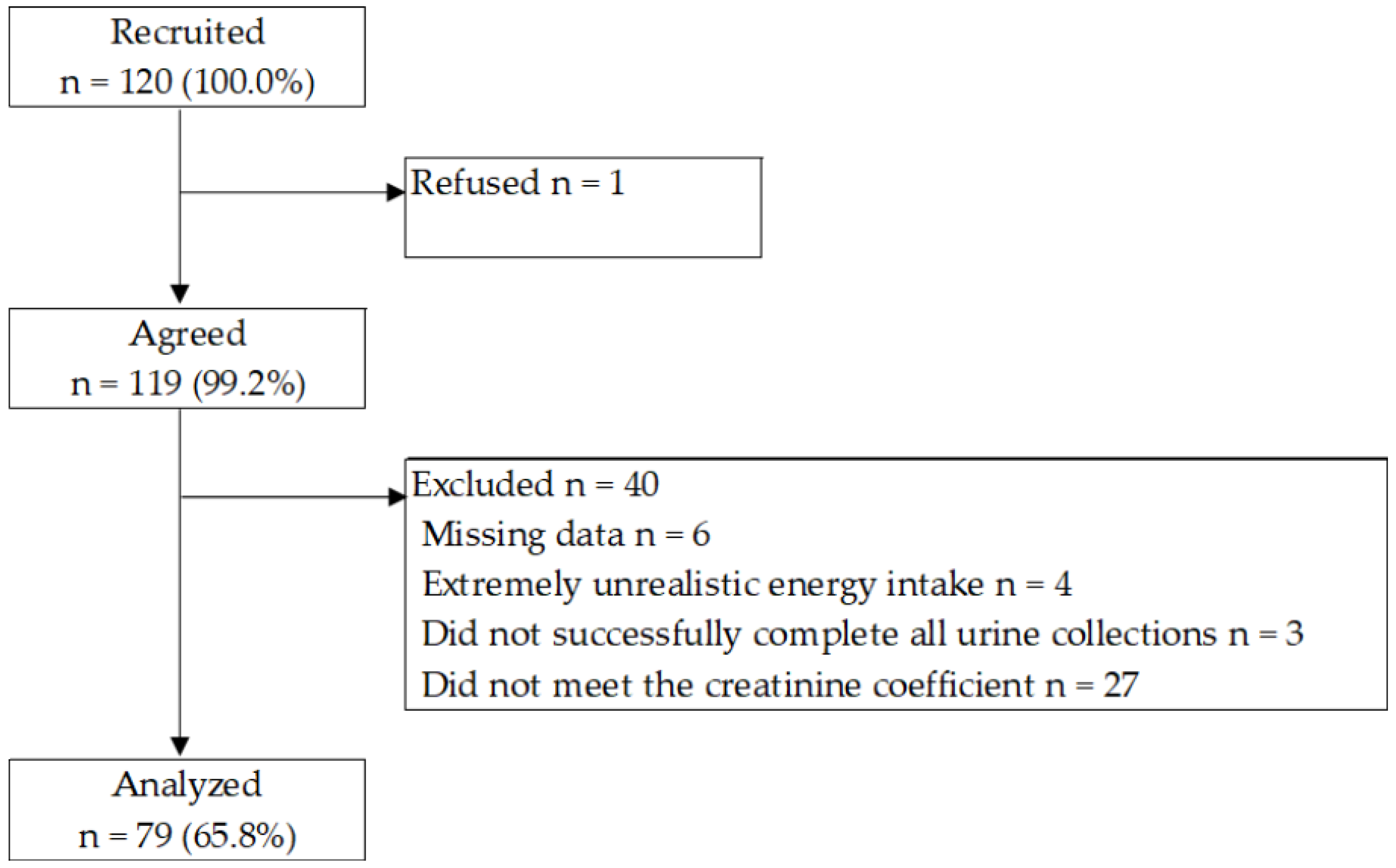
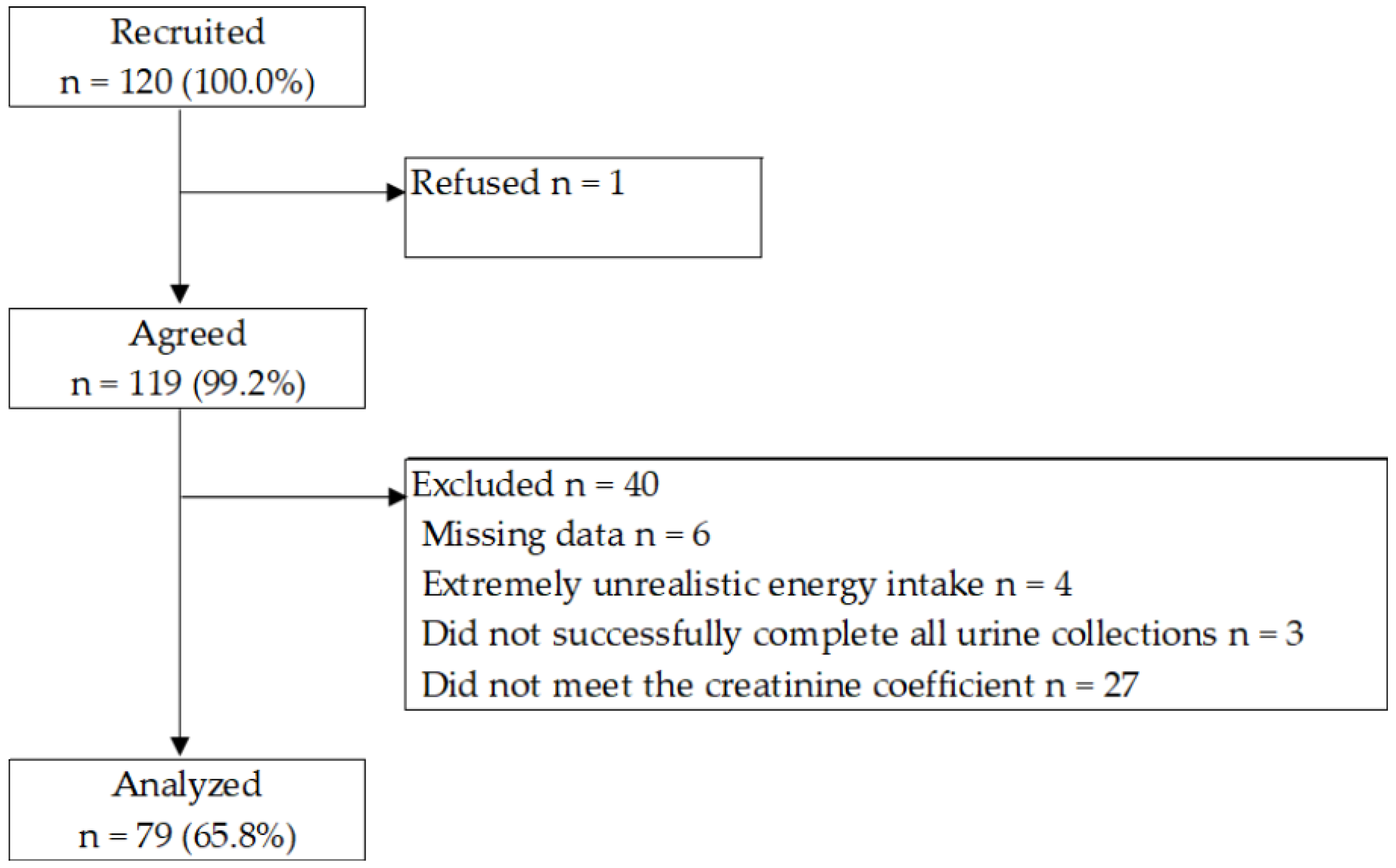
2.1. Participants
2.2. Twenty-Four-Hour Urine Collection
2.3. Dietary Assessment
2.4. Other Variables
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mohan, S.; Prabhakaran, D. Expert Meeting on Population Sodium Reduction Strategies for Prevention and Control of Noncommunicable Diseases in the South-East Asia Region-Background Review of Salt and Health: Situation in South-East Asia Region. 2013. Available online: https://apps.who.int/iris/handle/10665/312227 (accessed on 21 May 2021).
- Thornton, S.N. Salt in health and disease-a delicate balance. N. Engl. J. Med. 2013, 368, 2531. [Google Scholar] [PubMed]
- Dyer, A.R.; Elliott, P.; Shipley, M. Urinary electrolyte excretion in 24 hours and blood pressure in the INTERSALT Study. II. estimates of electrolyte-blood pressure associations corrected for regression dilution bias. the INTERSALT Cooperative Research Group. Am. J. Epidemiol. 1994, 139, 940–951. [Google Scholar] [CrossRef] [PubMed]
- Aburto, N.J.; Hanson, S.; Gutierrez, H.; Hooper, L.; Elliott, P.; Cappuccio, F.P. Effect of increased potassium intake on cardiovascular risk factors and disease: Systematic review and meta-analyses. BMJ 2013, 346, f1378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lennon-Edwards, S.; Allman, B.R.; Schellhardt, T.A.; Ferreira, C.R.; Farquhar, W.B.; Edwards, D.G. Lower potassium intake is associated with increased wave reflection in young healthy adults. Nutr. J. 2014, 13, 39. [Google Scholar] [CrossRef] [Green Version]
- Okuda, M.; Asakura, K.; Sasaki, S.; Shinozaki, K. Twenty-four-hour urinary sodium and potassium excretion and associated factors in Japanese secondary school students. Hypertens. Res. 2016, 39, 524–529. [Google Scholar] [CrossRef]
- Tabara, Y.; Takahashi, Y.; Kumagai, K.; Setoh, K.; Kawaguchi, T.; Takahashi, M.; Muraoka, Y.; Tsujikawa, A.; Gotoh, N.; Terao, C.; et al. Descriptive epidemiology of spot urine sodium-to-potassium ratio clarified close relationship with blood pressure level: The Nagahama Study. J. Hypertens. 2015, 33, 2407–2413. [Google Scholar] [CrossRef]
- Grimes, C.A.; Riddell, L.J.; Campbell, K.J.; Beckford, K.; Baxter, J.R.; He, F.J.; Nowson, C.A. Dietary intake and sources of sodium and potassium among Australian schoolchildren: Results from the cross-sectional salt and other nutrients in children (SONIC) Study. BMJ Open 2017, 7, e016639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Craigie, A.M.; Lake, A.A.; Kelly, S.A.; Adamson, A.J.; Mathers, J.C. Tracking of obesity-related behaviours from childhood to adulthood: A systematic review. Maturitas 2011, 70, 266–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, L.; Krupp, D.; Remer, T. Salt, fruit and vegetable consumption and blood pressure development: A longitudinal investigation in healthy children. Br. J. Nutr. 2014, 111, 662–671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, X.; Wang, Y. Tracking of blood pressure from childhood to adulthood: A systematic review and meta-regression analysis. Circulation 2008, 117, 3171–3180. [Google Scholar] [CrossRef] [Green Version]
- Ministry of Health, Labour and Welfare. Dietary Reference Intakes for Japanese; Ministry of Health, Labour and Welfare: Tokyo, Japan, 2015; p. 2014. (In Japanese) [Google Scholar]
- Collins, A.C.; Ward, K.D.; Mirza, B.; Slawson, D.L.; McClanahan, B.S.; Vukadinovich, C. Comparison of nutritional intake in US adolescent swimmers and non-athletes. Health 2012, 4, 873–880. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Temme, E.H.M.; Kesteloot, H. Alcohol drinkers overreport their energy intake in the BIRNH Study: Evaluation by 24-hour urinary excretion of cations. Belgian Interuniversity Research on Nutrition and Health. J. Am. College Nutr. 2001, 20, 510–519. [Google Scholar] [CrossRef]
- Ekelund, U.; Yngve, A.; Westerterp, K.; Sjöström, M. Energy expenditure assessed by heart rate and doubly labeled water in young athletes. Med. Sci. Sports Exerc. 2002, 34, 1360–1366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagashima, Y.; Horikawa, A.; Koita, A.; Miyaki, M.; Iguchi, M.; Tanaka, A. Validity and reproducibility of a self-administered diet history questionnaire (dhq) answered by junior athletes and their mothers. Jpn. J. Sports Nutr. 2020, 13, 25–39. [Google Scholar]
- Liu, K.; Cooper, R.; McKeever, J.; McKeever, P.; Byington, R.; Soltero, I.; Stamler, R.; Gosch, F.; Stevens, E.; Stamler, J. Assessment of the association between habitual salt intake and high blood pressure: Methodological problems. Am. J. Epidemiol. 1979, 110, 219–226. [Google Scholar] [CrossRef]
- Huang, Y.; Van Horn, L.; Tinker, L.F.; Neuhouser, M.L.; Carbone, L.; Mossavar-Rahmani, Y.; Thomas, F.; Prentice, R.L. Measurement error corrected sodium and potassium intake estimation using 24-hour urinary excretion. Hypertension 2014, 63, 238–244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haff, G.G.; Triplett, N.T. Essentials of Strength Training and Conditioning, 4th ed.; Human Kinetics Publishers: Champaign, IL, USA, 2015. [Google Scholar]
- Yamori, Y.; Nara, Y.; Kihara, M.; Mano, M.; Horie, R. Simple method for sampling consecutive 24-hour urine for epidemiological and clinical studies. Clin. Exp. Hypertens. A 1984, 6, 1161–1167. [Google Scholar] [CrossRef]
- HO/PAHO Regional Expert Group for Cardiovascular Disease; Pan American Health Organization; World Health Organization. Protocol for Population Level Sodium Determination in 24-Hour Urine Samples. 2010. Available online: https://apps.who.int/iris/bitstream/handle/10665/340732/WHO-EURO-2021-2333-42088-57949-eng.pdf?sequence=1 (accessed on 21 May 2021).
- Holbrook, J.T.; Patterson, K.Y.; Bodner, J.E.; Douglas, L.W.; Veillon, C.; Kelsay, J.L.; Mertz, W.; Smith, J.C. Sodium and potassium intake and balance in adults consuming self-selected diets. Am. J. Clin. Nutr. 1984, 40, 786–793. [Google Scholar] [CrossRef] [PubMed]
- Tasevska, N.; Runswick, S.A.; Bingham, S.A. Urinary potassium is as reliable as urinary nitrogen for use as a recovery biomarker in dietary studies of free living individuals. J. Nutr. 2006, 136, 1334–1340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sasaki, S.; Yanagibori, R.; Amano, K. Self-Administered Diet History Questionnaire developed for health education: A relative validation of the test-version by comparison with 3-day diet record in women. J. Epidemiol. 1998, 8, 203–215. [Google Scholar] [CrossRef] [Green Version]
- Sasaki, S.; Yanagibori, R.; Amano, K. Validity of a Self-Administered Diet History Questionnaire for assessment of sodium and potassium: Comparison with single 24-hour urinary excretion. Jpn. Circ. J. 1998, 62, 431–435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kobayashi, S.; Honda, S.; Murakami, K.; Sasaki, S.; Okubo, H.; Hirota, N.; Notsu, A.; Fukui, M.; Date, C. Both comprehensive and brief self-administered diet history questionnaires satisfactorily rank nutrient intakes in Japanese adults. J. Epidemiol. 2012, 22, 151–159. [Google Scholar] [CrossRef] [Green Version]
- Science and Technology Agency Standard. Tables of Food Composition in Japan, 5th revised and enlarged ed.; Printing Bureau of the Ministry of Finance: Tokyo, Japan, 2005. (In Japanese) [Google Scholar]
- Sasaki, S.; Katagiri, A.; Tsuji, T.; Shimoda, T.; Amano, K. Self-reported rate of eating correlates with body mass index in 18-y-old Japanese women. Int. J. Obes. Relat. Metab. Disord. 2003, 27, 1405–1410. [Google Scholar] [CrossRef] [Green Version]
- Intersalt Cooperative Research Group. Intersalt: An international study of electrolyte excretion and blood pressure. Results for 24 h urinary sodium and potassium excretion. BMJ 1988, 297, 319–328. [Google Scholar] [CrossRef] [Green Version]
- Campanozzi, A.; Avallone, S.; Barbato, A.; Iacone, R.; Russo, O.; De Filippo, G.; D’Angelo, G.; Pensabene, L.; Malamisura, B.; Cecere, G.; et al. High sodium and low potassium intake among italian children: Relationship with age, body mass and blood pressure. PLoS ONE 2015, 10, e0121183. [Google Scholar]
- Gonçalves, C.; Abreu, S.; Padrão, P.; Pinho, O.; Graça, P.; Breda, J.; Santos, R.; Moreira, P. Sodium and potassium urinary excretion and dietary intake: A cross-sectional analysis in adolescents. Food Nutr. Res. 2016, 60, 29442. [Google Scholar] [CrossRef] [Green Version]
- WHO [Guideline]. Potassium Intake for Adults and Children. 2012. Available online: https://www.who.int/publications/i/item/9789241504829 (accessed on 21 May 2021).
- WHO. Diet, Nutrition and the Prevention of Chronic Diseases; World Health Organization Technical Report Series; WHO: Geneva, Switzerland, 2003; Volume 916, pp. 1–149. Available online: http://whqlibdoc.who.int/trs/WHO_TRS_916.pdf (accessed on 24 October 2021).
- Webster, J.L.; Dunford, E.K.; Neal, B.C. A systematic survey of the sodium contents of processed foods. Am. J. Clin. Nutr. 2010, 91, 413–420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministry of Health, Labour and Welfare. Healthy Japan. Volume 21. Available online: https://www.mhlw.go.jp/www1/topics/kenko21_11/b1.html (accessed on 21 August 2021).
- Ministry of Education, Culture, Sports, Science and Technology; Ministry of Health, Labour and Welfare; Ministry of Agriculture, Forestry and Fisheries. Dietary Guidelines, Partially Revised in 2016. Dietary Guidelines for Japanese. Available online: https://www.maff.go.jp/e/index.html (accessed on 20 October 2021).
- Ballew, C.; Kuester, S.; Gillespie, C. Beverage choices affect adequacy of children’s nutrient intakes. Arch. Pediatr. Adolesc. Med. 2000, 154, 1148–1152. [Google Scholar] [CrossRef] [Green Version]
- Kristjansdottir, A.G.; Thorsdottir, I.; De Bourdeaudhuij, I.; Due, P.; Wind, M.; Klepp, K.I. Determinants of fruit and vegetable intake among 11-year-old schoolchildren in a country of traditionally low fruit and vegetable consumption. Int. J. Behav. Nutr. Phys. Act. 2006, 3, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministry of Health, Labour and Welfare. The National Health and Nutrition Survey in Japan. 1997. Available online: https://www.mhlw.go.jp/toukei/kouhyo/indexkk_14_4.html (accessed on 21 August 2021).
- Ministry of Health, Labour and Welfare. The National Health and Nutrition Survey in Japan. 2015. Available online: https://www.mhlw.go.jp/bunya/kenkou/eiyou/h27-houkoku.html (accessed on 21 May 2021).
- Lucko, A.M.; Doktorchik, C.; Woodward, M.; Cogswell, M.; Neal, B.; Rabi, D.; Anderson, C.; He, F.J.; MacGregor, G.A.; L’Abbe, M.L.; et al. Percentage of Ingested sodium excreted in 24-hour urine collections: A systematic review and meta-analysis. J. Clin. Hypertens. 2018, 20, 1220–1229. [Google Scholar] [CrossRef] [Green Version]
- Baker, L.B. Sweating rate and sweat sodium concentration in athletes: A review of methodology and intra/interindividual variability. Sports Med. 2017, 47 (Suppl. 1), 111–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peniamina, R.; Skeaff, S.; Haszard, J.J.; McLean, R. Comparison of 24-h diet records, 24-h urine, and duplicate diets for estimating dietary intakes of potassium, sodium, and iodine in children. Nutrients 2019, 11, 2927. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charlton, K.; Schutte, A.; Wepener, L.; Corso, B.; Kowal, P.; Ware, L. Correcting for intra-individual variability in sodium excretion in spot urine samples does not improve the ability to predict 24 h urinary sodium excretion. Nutrients 2020, 12, 2026. [Google Scholar] [CrossRef]
- Consolazio, C.F.; Matoush, L.O.; Nelson, R.A.; Harding, R.S.; Canham, J.E. Excretion of sodium, potassium, magnesium and iron in human sweat and the relation of each to balance and requirements. J. Nutr. 1963, 79, 407–415. [Google Scholar] [CrossRef] [PubMed]
- Hinton, P.S.; Sanford, T.C.; Davidson, M.M.; Yakushko, O.F.; Beck, N.C. Nutrient Intakes and dietary behaviors of male and female collegiate athletes. Int. J. Sport Nutr. Exerc. Metab. 2004, 14, 389–405. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Variable | All (n = 79) | |
|---|---|---|
| Mean | SD | |
| Age, years | 13.0 | 0.8 |
| School grade, n (%) | ||
| Grade 7 | 30 (38.0) | |
| Grade 8 | 28 (35.4) | |
| Grade 9 | 21 (26.6) | |
| Physical activity level, n (%) a | ||
| Level III (high) | 16 (20.3) | |
| Level IV (very high) | 63 (79.7) | |
| Sports activities, h/week | 20.1 | 3.5 |
| Systolic blood pressure, mmHg | 117.1 | 12.6 |
| Diastolic blood pressure, mmHg | 63.0 | 8.3 |
| Body height, cm | 157.2 | 9.8 |
| Body mass, kg | 45.7 | 9.0 |
| BMI, kg/m2 | 18.4 | 2.1 |
| Body fat percentage, % | 12.7 | 4.1 |
| Fat-free mass, kg | 37.2 | 6.6 |
| FFMI, kg/m2 | 14.9 | 1.1 |
| Variable | All (n = 79) | |
|---|---|---|
| Mean | SD | |
| Sodium, mmol/L | 170.8 | 35.1 |
| Sodium, mmol/day | 143.2 | 44.7 |
| Potassium, mmol/L | 51.8 | 14.7 |
| Potassium, mmol/day | 42.8 | 14.2 |
| Na/K ratio, molar ratio | 3.6 | 1.2 |
| Volume output, mL/day | 857.1 | 214.4 |
| Creatinine excretion, mg/L | 132.6 | 37.4 |
| Variable | All (n = 79) | |
|---|---|---|
| Mean | SD | |
| Dietary intake | ||
| Energy, kcal/day | 3194 | 717 |
| Protein, g/day | 104.4 | 26.9 |
| Protein, g/kg BM | 2.4 | 0.7 |
| Protein, % of energy | 13.1 | 1.7 |
| Fat, g/day | 95.6 | 26.6 |
| Fat, g/kg BM | 2.2 | 0.7 |
| Fat, % of energy | 27.1 | 5.3 |
| Carbohydrate, g/day | 464.8 | 124.4 |
| Carbohydrate, g/kg BM | 10.4 | 3.0 |
| Carbohydrate, % of energy | 58.0 | 6.4 |
| Grains, g/day | 833.8 | 269.8 |
| Potatoes, g/day | 34.4 | 22.5 |
| Vegetables, g/day | 304.6 | 194.5 |
| Fruit, g/day | 170.6 | 149.3 |
| Fishes and shellfishes, g/day | 67.7 | 45.6 |
| Milk and dairy products, g/day | 364.2 | 204.9 |
| Seasoning, g/day | 20.6 | 20.6 |
| Estimated dietary intake | ||
| Salt intake, g/day a | 9.7 | 3.0 |
| Salt intake exceed 8.0 g/day, n (%) a,b | 58 (73.4) | |
| Potassium intake, mg/day a | 2172 | 719 |
| Potassium intake not meet 2600 mg/day, n (%) a,b | 58 (73.4) | |
| Urinary Sodium | Urinary Potassium | Urinary Na/K Ratio | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Model 1 | Model 1 | Model 2 a | Model 3 a | Model 1 | Model 2 b | Model 3 b | ||||||||
| β | p | β | p | β | p | β | p | β | p | β | p | β | p | |
| Protein | 0.209 | 0.065 | 0.034 | 0.766 | - | - | - | - | −0.107 | 0.350 | - | - | - | - |
| Fat | 0.097 | 0.396 | 0.093 | 0.416 | - | - | - | - | −0.111 | 0.331 | - | - | - | - |
| Carbohydrate | 0.038 | 0.739 | 0.143 | 0.210 | - | - | - | - | −0.232 | 0.038 | −0.160 | 0.174 | - | - |
| Grains | 0.078 | 0.495 | 0.076 | 0.504 | - | - | - | - | −0.157 | 0.167 | - | - | - | - |
| Potatoes | 0.110 | 0.336 | 0.014 | 0.903 | - | - | - | - | −0.111 | 0.334 | - | - | - | - |
| Vegetables | 0.009 | 0.936 | 0.230 | 0.041 | 0.224 | 0.039 | 0.140 | 0.195 | −0.278 | 0.013 | −0.256 | 0.023 | −0.062 | 0.372 |
| Fruit | 0.029 | 0.797 | 0.161 | 0.156 | - | - | - | - | −0.272 | 0.016 | −0.250 | 0.027 | −0.145 | 0.526 |
| Fishes and shellfishes | 0.133 | 0.241 | −0.102 | 0.369 | - | - | - | - | 0.119 | 0.295 | - | - | - | - |
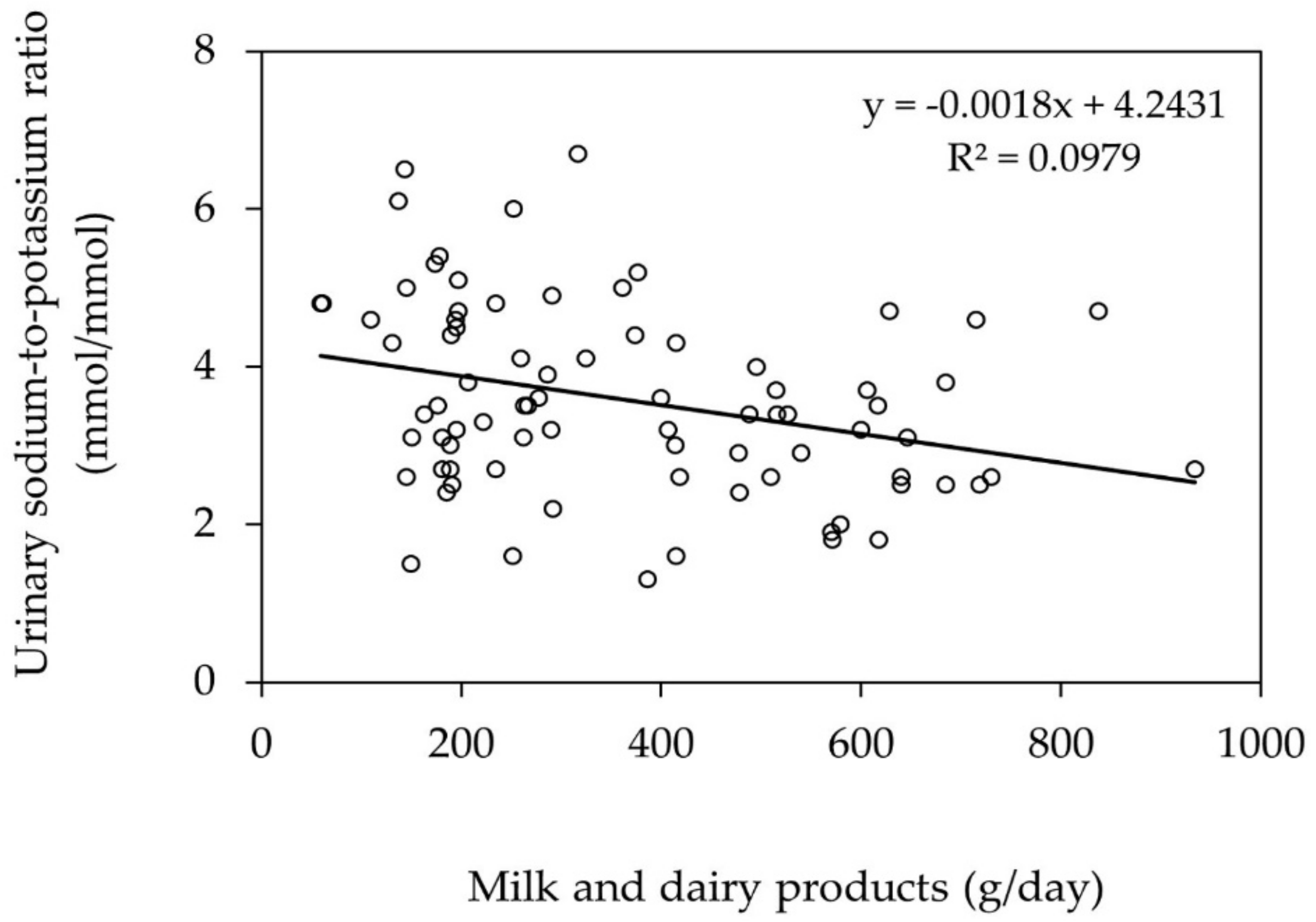
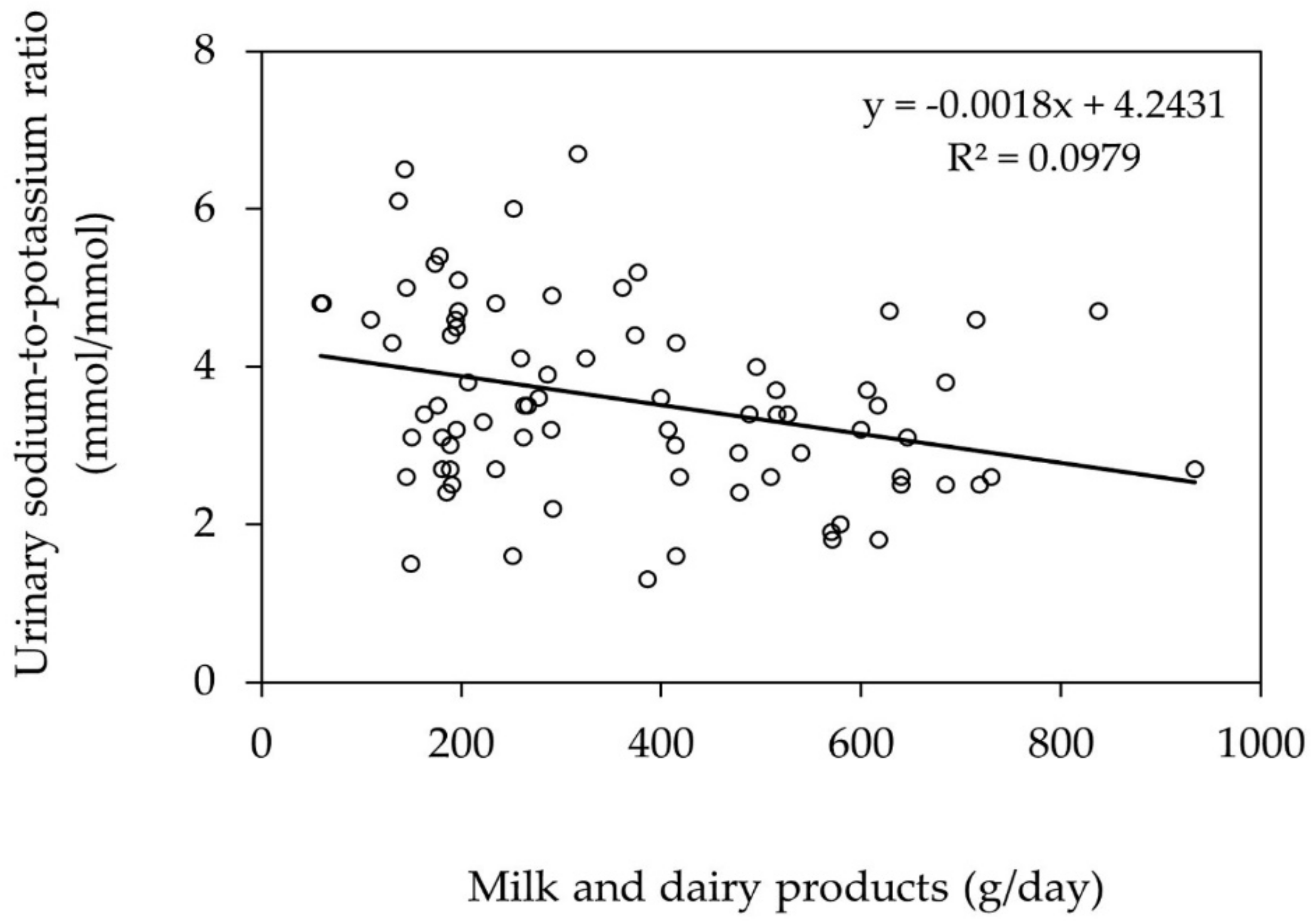
| Milk and dairy products | 0.007 | 0.953 | 0.304 | 0.007 | 0.303 | 0.005 | 0.252 | 0.021 | −0.317 | 0.004 | −0.298 | 0.008 | −0.254 | 0.026 |
| Seasoning | −0.051 | 0.658 | 0.051 | 0.656 | - | - | - | - | −0.117 | 0.306 | - | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nagashima, Y.; Horikawa, A.; Mori, M. Association between 24 h Urinary Sodium and Potassium Excretion and Dietary Intake in Japanese Male Adolescent Football Players. Adolescents 2021, 1, 461-472. https://doi.org/10.3390/adolescents1040035
Nagashima Y, Horikawa A, Mori M. Association between 24 h Urinary Sodium and Potassium Excretion and Dietary Intake in Japanese Male Adolescent Football Players. Adolescents. 2021; 1(4):461-472. https://doi.org/10.3390/adolescents1040035
Chicago/Turabian StyleNagashima, Yosuke, Akiko Horikawa, and Mari Mori. 2021. "Association between 24 h Urinary Sodium and Potassium Excretion and Dietary Intake in Japanese Male Adolescent Football Players" Adolescents 1, no. 4: 461-472. https://doi.org/10.3390/adolescents1040035
APA StyleNagashima, Y., Horikawa, A., & Mori, M. (2021). Association between 24 h Urinary Sodium and Potassium Excretion and Dietary Intake in Japanese Male Adolescent Football Players. Adolescents, 1(4), 461-472. https://doi.org/10.3390/adolescents1040035