Abstract
Mpox, a zoonotic viral disease, has emerged as a global concern due to outbreaks in both endemic and non-endemic regions in 2022. Rodents, including African squirrels and Gambian pouched rats, are suspected key reservoirs, with human infections occurring through direct contact with infected animals or bushmeat consumption. Previously confined to rural Africa, mpox has spread via international travel and the exotic pet trade. Human-to-human transmission occurs mainly via respiratory droplets and direct contact with bodily fluids or lesions. The virus has a double-stranded DNA genome within a lipid envelope. Despite lower mutation rates in DNA viruses, mpox has developed mutations, particularly in genes like F8L, G9R, and F13L, facilitating viral replication and immune evasion. The virus targets immune cells such as monocytes and macrophages, weakening host defenses and prolonging infection. Immunocompromised individuals are at higher risk of severe complications. Although generally self-limiting, severe cases may require antiviral treatment. This article briefly summarizes the therapeutic and preventive strategies, and public health measures to combat zoonotic threats.
Keywords:
mpox; smallpox; DNA virus; zoonotic diseases; transmission; immune interaction; public health 1. Introduction
Mpox, formerly known as monkeypox, is a zoonotic viral disease that spreads from animals to humans and is caused by the mpox virus, Orthopoxvirus monkeypox (MPXV). It belongs to a family of viruses that also includes variola, the virus responsible for smallpox. Mpox is mainly transmitted to humans through direct contact with infected animals, such as rodents, but it can also spread from person to person through respiratory droplets or through contact with bodily fluids [1,2,3]. Symptoms of the disease can vary widely, including fever, headache, body aches, swollen lymph nodes, and a distinctive rash that develops in later stages [4]. While most people recover without complications, some may experience severe symptoms, particularly those who are immunocompromised, leading to higher risks of complications, such as bacterial infections, encephalitis, and pneumonia [3,5].
Mpox has primarily been endemic in regions like Central Africa, especially the Democratic Republic of the Congo (DRC) [6] due to the Congo Basin rainforest where repeated spillovers occur when people hunt or sell bushmeat [7]. The ability of the virus to spread through both animal-to-human and human-to-human contact has amplified concerns, particularly given its capacity to cause severe complications in some individuals. The global outbreak of mpox in 2022 in the era of the COVID-19 pandemic highlights the urgent need for enhanced awareness, better surveillance systems, and more effective strategies to prevent and control outbreaks. A better understanding of epidemiology, symptoms, viral mutations, human cell interaction, transmission, treatment, and public health management strategies of the mpox virus will improve the effective measures for prevention and response in the future.
2. Epidemiology and Viral Structure
Mpox was first identified in monkeys in Copenhagen, Denmark, in 1958. It was recognized in humans for the first time in 1970 in the DRC. Over the next few decades, cases of mpox were reported primarily in Central and West Africa. However, between 1970 and 2021, cases remained sporadic, with limited spread to non-endemic regions. In 2022, a global outbreak led the World Health Organization to classify mpox as an “evolving threat of moderate public health concern” [2,6]. The 2022 outbreak involved thousands of cases in multiple countries, including the UK, Singapore, Israel, and the U.S., and was often linked to travel to endemic areas or contact with infected individuals.
The number of suspected cases (rather than laboratory-confirmed) has increased significantly, from more than 14 thousand cases in 2023 to more than 94 thousand in early 2024–2025 [8]. The limited access to diagnosis, vaccination and care favors persistent transmission and larger outbreaks [6]. Understanding the biology of the mpox virus is important to explain its persistence and pathogenic potential. At the molecular level, Mpox belongs to the genus orthopoxvirus in the Poxviridae family and shares many structural features with smallpox. The virus consists of four main components: a brick-shaped core, a double-stranded DNA genome, two lateral bodies, and an outer lipoprotein envelope [9]. Mpox is a relatively large DNA virus, measuring about 220–450 nanometers long and 140–260 nanometers wide [10]. The virus’s DNA genome has about 196,858 base pairs and approximately 180 different proteins [11] (Figure 1). The virus also carries a DNA-dependent RNA polymerase [12].
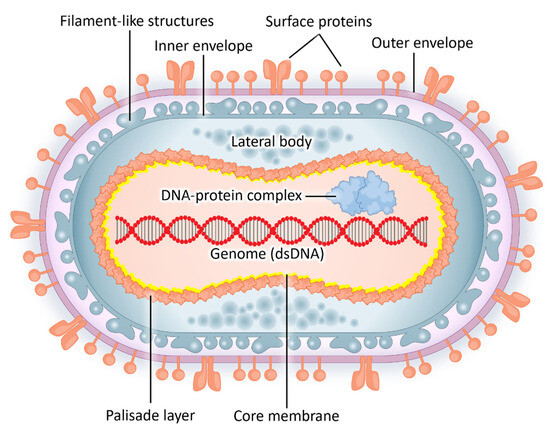
Figure 1.
The brick-shaped mpox virus, measuring about 220–450 nanometers long and 140–260 nanometers wide, is the largest known DNA virus. A lipid membrane envelops it and contains lateral bodies within a core area, along with a double-stranded DNA genome.
3. Human Cell Interaction and Viral Transmission
The capacity of the mpox virus for adaptation has made it a pathogen of growing concern, especially with the increased frequency of human-to-human transmission in recent outbreaks. The interaction between MPXV and human cells begins with viral entry. The virus primarily enters the body through broken skin, respiratory pathways, or mucous membranes such as the eyes, nose, or mouth. Once inside the host, MPXV targets various cell types, including macrophage, dendritic, and endothelial cells [13].
MPXV’s entry into human cells is facilitated by viral surface proteins that bind to host cell receptors (Figure 2). The evidence suggests that MPXV utilizes various attachment proteins to mediate cell entry [13,14]. After binding to the host cell, the virus can enter through macropinocytosis (the engulfment of extracellular content in vesicles known as macropinosomes) or membrane fusion. Once inside the cytoplasm, MPXV starts replication. The virus is then released either through cell lysis or via exocytosis, allowing it to infect neighboring cells. Mpox has a unique ability to manipulate the human immune system to prolong infection. The virus produces various proteins, such as H3L and NF-κB. H3L is a key protein that binds to chromatin, leading to altered gene expression and cellular damage. NF-κB disrupts the host’s cellular functions and natural antiviral defense and promotes viral survival by inhibiting the expression of antiviral genes [15,16]. Mpox also targets natural killer (NK) cells and monocytes, which are essential components of the innate immune system.
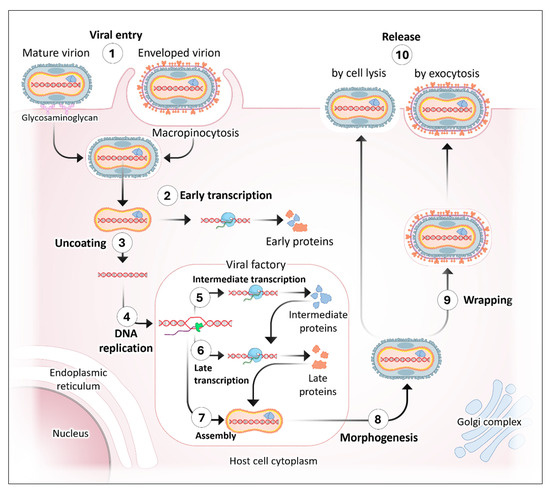
Figure 2.
The life cycle of mpox. The mpox virus infects and replicates within host cells through the following steps: 1. Virion Entry: The virus can attach to and enter a host cell in the form of either a mature virus or an extracellular enveloped virus. The surface membrane protein of the virus binds to glycosaminoglycans on the host cell surface. This attachment activates the host cell’s macropinocytosis, allowing the virus to be internalized. 2. Early Transcription and Translation: Once inside, some of the viral DNA is immediately transcribed and translated to produce early proteins. These include growth factors, immune response modulators, and factors essential for DNA replication. 3. Uncoating: After the virus enters the cell, the uncoating process occurs, shedding the outer membranes and releasing the viral core into the cytoplasm. 4. DNA Replication: Most of the viral DNA replicates to form concatemeric DNA. This replication occurs in a localized cytoplasmic region known as the viral factory. 5. Intermediate Gene Transcription and Translation: Within the viral factory, the newly replicated viral DNA undergoes intermediate transcription and translation, generating intermediate proteins, including transcription factors required for late transcription. 6. Late Gene Transcription and Translation: Also taking place in the viral factory, the progeny viral DNA undergoes late transcription and translation, producing late proteins that contribute to the viral assembly process. 7. Assembly: The viral DNA is organized into a single genome and packaged into the core along with proteins needed for early transcription. 8. Morphogenesis: The assembled core moves out of the viral factory region, acquires an outer membrane, and becomes a mature virus. 9. Wrapping: A portion of the total virus particles produced is further wrapped in trans-Golgi/late endosomal double membranes to form an intracellular enveloped virus. 10. Release: The intracellular enveloped virus migrates to the cell periphery on microtubules and is released via exocytosis, becoming a cell-associated enveloped virus. The mature virus generally remains within the cell, except in rare cases of cell lysis.
By integrating host-cell membrane proteins into its structure, mpox evades neutralizing antibodies and interferes with immune cell activation [17]. This prevents the proper production of cytokines, such as interferons and tumor necrosis factor (TNF), which are vital for an effective immune response and critical for initiating antiviral defenses. Additionally, mpox inhibits T-cell activation by hindering antigen presentation, thereby limiting cell stimulation and the production of the effector cytokines necessary for viral clearance [18]. Furthermore, MPXV downregulates major histocompatibility complex (MHC) molecules on infected cells, making it more difficult for T cells to recognize and destroy them [19]. The virus can also inhibit apoptosis that is normally triggered by infected cells to prevent viral replication [20]. This combination of immune evasion tactics allows MPXV to persist longer in the host, replicate efficiently, and spread to additional cells and tissues. These immune evasion strategies allow mpox to weaken the host’s defenses, prolong infection and increase the risk of complications such as secondary infections and severe disease progression. Recent outbreaks have shown that the virus may adapt and become more efficient at transmission among humans.
Mpox can be transmitted through several routes, from animal-to-animal, animal-to-human, and human-to-human (Figure 3). While scientists have long suspected rodents and other small animals in Africa as reservoir host, the official “reservoir host” remains unidentified [21,22]. African squirrels, Gambian pouched rats, and primates have been implicated as potential reservoirs. Recently, an international team of scientists suggested that the fire-footed rope squirrel (Funisciurus pyrropus) could be the reservoir host [21,22]. Animal-to-animal transmission occurs through bites, scratches, or close physical contact [23]. While animal-to-human transmission often results from activities such as hunting, skinning, or handling infected animals, human-to-human transmission primarily occurs through direct contact with infected bodily fluids or respiratory droplets. This transmission can include skin-to-skin contact, via respiratory droplets or other forms of close contact [24], and sexual transmission could also be an efficient route for human-to-human transmission [25]. In particular, sex workers in the Congo have been strongly affected by the outbreak of mpox as it drives away clients from those who are known to have the disease. The appearance of a new clade 1b strain showing increased transmissibility has compounded the problem in that many cases are not reported. Access to healthcare is also limited, further enhancing the spread. It has been proposed that decriminalization of sex workers be implemented to control the spread of mpox in these areas [26]. Healthcare settings are particularly vulnerable to human-to-human transmission, requiring strict precautions to prevent further spread. In humans, the viral incubation period is 10–14 days, and the infectious period begins when clinical signs first appear [23].
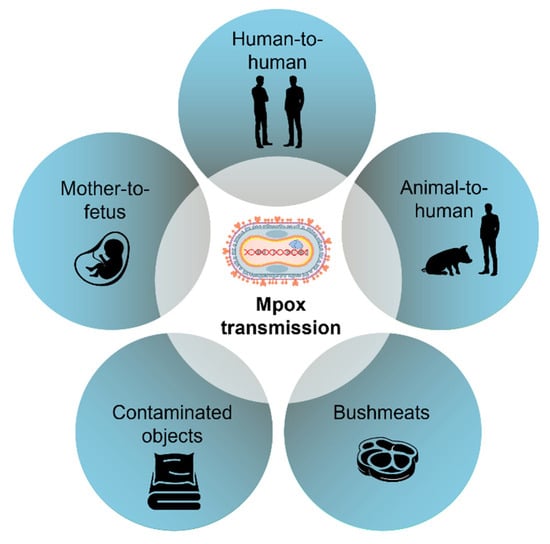
Figure 3.
The mpox virus spreads through direct contact with infected bodily fluids, respiratory droplets, skin-to-skin contact, or other forms of close physical interaction. Mpox virus can be transmitted from infected mothers to the fetus [27,28].
4. Symptoms and Treatment
Mpox typically begins with symptoms similar to those of the flu. Individuals often experience extreme fatigue, fever, chills, muscle aches, headaches, and swollen lymph nodes, particularly in the cervical, axillary, or pubic areas [2] (Figure 4). A few days after the onset of fever, a characteristic rash generally appears. This rash may begin on the face, hands, feet, chest, or genitals and can spread to other parts of the body. It usually progresses through several stages: starting as flat lesions, then developing into raised bumps, followed by fluid-filled blisters, and finally scabbing over. As the body heals, the scabs eventually fall off. The rash may be painful or itchy, and the illness typically lasts between two and four weeks.
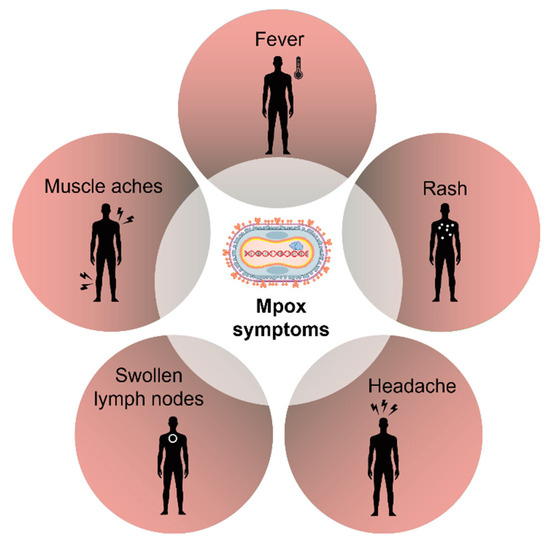
Figure 4.
The mpox infections typically present rash and flu-like symptoms, such as fever, headache, and body ache, and some individuals may also develop lymphadenopathy.
In certain cases, especially among immunocompromised individuals [29], mpox can have atypical manifestations of sepsis, widespread rash, hemorrhagic complications, extensive confluent skin lesions (lesions merge to form large lesions), and necrotic lesions (tissue death, causing blackening, damaged skin that may become gangrenous), and severe lymphadenopathy. Additional complications may include ocular or periorbital infections, pulmonary complications, encephalitis, and myocarditis [30]. Prompt medical attention is important for anyone experiencing serious symptoms or who is considered at higher risk of complications.
Currently, there is no specific antiviral treatment for mpox. Therefore, management primarily focuses on symptomatic care, including pain relief, fever reduction, and maintaining hydration. In severe cases, antiviral medications such as tecovirimat (TPOXX), cidofovir, and brincidofovir may be prescribed [31]. Although these drugs are approved for smallpox, and there is no FDA approval, they are used off-label for mpox. Hospitalization may be required for patients with complications, such as pneumonia or encephalitis, and isolation is crucial to prevent the spread of the virus. Most cases of mpox are self-limiting, with recovery occurring within 2–4 weeks. However, in rare cases, as mentioned earlier, the disease can lead to severe complications and even death, particularly in immunocompromised individuals or those with pre-existing health conditions [3]. In February 2023, the U.S. Centers for Disease Control and Prevention (CDC) shared temporary guidelines for treating severe cases of mpox [32]. These severe cases are more common in people with HIV. The guidelines include the use of certain medications and treatments that were originally designed to protect against smallpox. These are called medical countermeasures (MCMs) and include the previously mentioned antiviral medications, along with trifluridine eye drops and Vaccinia Immune Globulin Intravenous (VIGIV) [33].
4.1. Vaccines for Mpox
Although mpox-specific vaccines have not been developed, existing smallpox vaccines have demonstrated cross-protection due to their close genetic relationship with the variola virus (which causes smallpox) (Table 1).

Table 1.
The summary of clinical trials of vaccines used for mpox prevention and treatment with the types, applications, and approval status.
4.2. Clinical Trial Findings on Tecovirimat for Mpox
The results of two clinical trials, PALM007 (Democratic Republic of the Congo) [35] and STOMP [36], revealed that while tecovirimat (TPOXX) was safe, it did not accelerate the healing of mpox lesions compared with a placebo. In the PALM007 trial, 597 people with mpox were treated at hospitals in the DRC. All patients received supportive care (like fluids, nutrition, and infection treatment) and were randomly given either tecovirimat or a placebo. The study showed that tecovirimat was well-tolerated and caused no serious side effects. However, it was no better than a placebo, and supportive care was equally effective. Researchers pointed out that basic care, such as good nutrition, hydration, and close monitoring, is likely to help patients recover quicker. More research is needed to understand other confounding factors that may influence the results.
4.3. Severe Mpox in People with Advanced HIV
People with advanced HIV are at higher risk for severe mpox and death from the infection. To help guide care, the CDC published Interim Clinical Considerations for Severe Manifestations of mpox which includes interim clinical recommendations for managing severe mpox in these patients [32]. The CDC and National Institutes of Health (NIH) are working together on a study called VIRISMAP (Virologic and Immunologic Characteristics of Severe Mpox in People with Advanced HIV). The goal is to better understand how the mpox virus spreads in people with advanced HIV and what immune system factors may lead to more severe illness. This research could help improve treatment and prevention for those most at risk. The study includes U.S. adults (18+) with HIV and low CD4+ helper T-cell counts who were hospitalized with confirmed or likely mpox. During their hospital stay, doctors collect medical data and lab samples to learn more about how mpox affects this vulnerable group.
5. Public Health Importance and Challenges in Mpox Studies
The primary preventive measures for mpox include avoiding contact with infected individuals and animals, as well as refraining from using objects that have been used by anyone infected [37]. Maintaining good hygiene practices and using personal protective equipment (PPE) in healthcare settings are essential to prevent human-to-human transmission. Pregnant women, children under the age of 8, and immunocompromised individuals should not care for sick individuals or animals. Additional prevention strategies for mpox should focus primarily on vaccination, as the smallpox vaccine provides cross-protection against the virus. However, since smallpox was eradicated and vaccination stopped, more people are now at risk [37]. During outbreaks, vaccines are given to high-risk groups like healthcare workers and travelers to areas where mpox is common [38]. Newer vaccines, such as the modified vaccinia Ankara (MVA) vaccine, are safer for people with weak immune systems and help improve protection [39].
Mpox research faces many challenges that limit our understanding and ability to control disease effectively. In endemic regions, especially Central and West Africa, poor disease monitoring and limited testing lead to underreporting of cases. There is also a lack of long-term data on how the virus spreads, how often people are reinfected, and how long immunity lasts after infection or vaccination. Scientists have not yet confirmed the natural animal host, although rodents are suspected. Clinical studies often involve small groups of patients, especially those outside large outbreaks, making it difficult to apply results to broader populations. The limited number of quality clinical trials has contributed to the lack of understanding of the safety and effectiveness of mpox treatments and vaccines. Recent outbreaks have shown unusual symptoms, such as genital sores, that have not yet been fully understood. Drugs, such as tecovirimat (TPOXX) and vaccines like JYNNEOS and ACAM2000 also need further research to better understand their long-term effectiveness and side effects (Table 2).
Table 2.
Partial list of clinical trials of drugs used to treat mpox with the mechanisms of action, and approval status.
On an immunological level, researchers are still learning how the virus behaves inside the body and how it avoids the immune system. The ability to track virus mutations is limited because of a lack of real-time genetic monitoring. Those who have previously received smallpox vaccines should have some residual protection against mpox. Individuals who were immunized prior to 1975 showed that 89.6% had anti-MPXV IgG antibody and 70.1% had neutralizing antibody [40]. However, it is unclear how much protection people obtain from previous mpox infections. Social issues also add to the problem. Misinformation makes it harder for people to get care. In many regions, public health efforts do not fully include local knowledge or community involvement. Finally, the underfunding of mpox research hinders preparedness for outbreaks.
6. Conclusions
Mpox has reemerged as a global health threat, although less contagious and deadly than smallpox, its genetic adaptation, immune evasion and wide transmission routes complicate control efforts. The FDA has approved the JYNNEOS and ACAM2000 smallpox/mpox vaccines representing important preventive progress on of mpox. The WHO has granted emergency use of MVA-BN (non-replicating) and LC16mB (minimally replicating) smallpox and mpox vaccines. Considering the high transmission capabilities of the mpox virus, a “One Health” approach that considers human, animal, and environmental health is important for preventing future outbreaks. Improved surveillance, better vaccines, and more effective treatments will be essential in controlling mpox. The rise of mpox in 2022 as a global health issue highlights the need to improve how we track and respond to infectious diseases. Since the virus can adapt, avoid the immune system, and spread between people, better testing, targeted vaccination, and continuous genomic surveillance are needed. This article summarizes current knowledge on viral characteristics, epidemiology, host-cell interactions, and potential therapeutic strategies, emphasizing the integration of structural biology, clinical findings, and public health perspectives as a key strength. However, limited long-term clinical evidence and incomplete understanding of virus–host interactions support the need of public health initiatives must also focus on education, rapid case identification, and international cooperation to mitigate future outbreaks and safeguard vulnerable populations.
Author Contributions
M.S.Z.: Conceptualization; Writing—original draft; R.C.S.: Conceptualization; Writing—original draft; D.R.: Writing—original draft; E.L.: Writing—original draft; S.M.G.A.: Writing—original draft; S.T.: Writing—original draft; J.C.L.-A.: Writing—review & editing; N.S.A.: Writing—review & editing; Visualization; M.S.R.: Writing—review & editing. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- The European Centre for Disease Prevention and Control. Rapid Risk Assessment on the Monkeypox Outbreak; The European Centre for Disease Prevention and Control: Solna, Sweden, 2022; Available online: https://www.ecdc.europa.eu/en/news-events/ecdc-releases-first-update-its-rapid-risk-assessment-monkeypox-outbreak (accessed on 4 July 2025).
- Apea, V.; Titanji, B.K.; Dakin, F.H.; Hayes, R.; Smuk, M.; Kawu, H.; Waters, L.; Levy, I.; Kuritzkes, D.R.; Gandhi, M.; et al. International healthcare workers’ experiences and perceptions of the 2022 multi-country mpox outbreak. PLoS Glob Public Health 2025, 5, e0003704. [Google Scholar] [CrossRef]
- The Centers for Disease Control and Prevention. Clinical Considerations for Mpox in Immunocompromised People; The Centers for Disease Control and Prevention: Atlanta, GA, USA, 2024. Available online: https://www.cdc.gov/mpox/hcp/clinical-care/immunocompromised-people.html (accessed on 4 July 2025).
- Wawina-Bokalanga, T.; Merritt, S.; Kinganda-Lusamaki, E.; Jansen, D.; Halbrook, M.; O’Toole, Á.; Pukuta-Simbu, E.; Vakaniaki, E.H.; Ola-Mpumbe, R.; Kwete-Mbokama, P.; et al. Epidemiology and phylogenomic characterisation of two distinct mpox outbreaks in Kinshasa, DR Congo, involving a new subclade Ia lineage: A retrospective, observational study. Lancet 2025, 406, 63–75. [Google Scholar] [CrossRef]
- Levitt, C.V.; Tran, Q.K.; Hraky, H.; Mazer-Amirshahi, M.; Pourmand, A. Emergency department approach to monkeypox. World J. Emerg. Med. 2023, 14, 341–348. [Google Scholar] [CrossRef]
- Olawade, D.B.; Wada, O.Z.; Fidelis, S.C.; Oluwole, O.S.; Alisi, C.S.; Orimabuyaku, N.F.; Clement David-Olawade, A. Strengthening Africa’s response to Mpox (monkeypox): Insights from historical outbreaks and the present global spread. Sci. One Health 2024, 3, 100085. [Google Scholar] [CrossRef] [PubMed]
- Hutin, Y.J.; Williams, R.J.; Malfait, P.; Pebody, R.; Loparev, V.N.; Ropp, S.L.; Rodriguez, M.; Knight, J.C.; Tshioko, F.K.; Khan, A.S.; et al. Outbreak of human monkeypox, Democratic Republic of Congo, 1996 to 1997. Emerg Infect Dis 2001, 7, 434–438. [Google Scholar] [CrossRef] [PubMed]
- United Nations Children’s Fund. Democratic Republic of the Congo Humanitarian Situation Report No. 7 (Mpox), 31 March 2025; United Nations Children’s Fund: New York, NY, USA, 2025; Available online: https://www.unicef.org/documents/democratic-republic-congo-humanitarian-situation-report-no-7-mpox-31-march-2025?utm_source=chatgpt.com (accessed on 4 July 2025).
- Karagoz, A.; Tombuloglu, H.; Alsaeed, M.; Tombuloglu, G.; AlRubaish, A.A.; Mahmoud, A.; Smajlovic, S.; Cordic, S.; Rabaan, A.A.; Alsuhaimi, E. Monkeypox (mpox) virus: Classification, origin, transmission, genome organization, antiviral drugs, and molecular diagnosis. J. Infect. Public Health 2023, 16, 531–541. [Google Scholar] [CrossRef] [PubMed]
- Sagdat, K.; Batyrkhan, A.; Kanayeva, D. Exploring monkeypox virus proteins and rapid detection techniques. Front. Cell Infect. Microbiol. 2024, 14, 1414224. [Google Scholar] [CrossRef]
- Lu, J.; Xing, H.; Wang, C.; Tang, M.; Wu, C.; Ye, F.; Yin, L.; Yang, Y.; Tan, W.; Shen, L. Mpox (formerly monkeypox): Pathogenesis, prevention, and treatment. Signal Transduct. Target. Ther. 2023, 8, 458. [Google Scholar] [CrossRef]
- Abduljalil, J.M.; Elfiky, A.A.; Elgohary, A.M. Exploration of natural compounds against the human mpox virus DNA-dependent RNA polymerase in silico. J. Infect. Public Health 2023, 16, 996–1003. [Google Scholar] [CrossRef]
- Meem, S.S.; Proma, A.Y.; Bhuiyan, M.A.; Dewan, S.M.R. The pressing need for study on the effects of Mpox on the progression of vascular inflammation: A well-timed call. Health Sci. Rep. 2024, 7, e2223. [Google Scholar] [CrossRef]
- Kataria, R.; Kaur, S.; Kaundal, R. Deciphering the complete human-monkeypox virus interactome: Identifying immune responses and potential drug targets. Front. Immunol. 2023, 14, 1116988. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.L.; Chung, C.S.; Heine, H.G.; Chang, W. Vaccinia virus envelope H3L protein binds to cell surface heparan sulfate and is important for intracellular mature virion morphogenesis and virus infection in vitro and in vivo. J. Virol. 2000, 74, 3353–3365. [Google Scholar] [CrossRef] [PubMed]
- Parnian, R.; Heydarifard, F.; Mousavi, F.S.; Heydarifard, Z.; Zandi, M. Innate Immune Response to Monkeypox Virus Infection: Mechanisms and Immune Escape. J. Innate Immun. 2024, 16, 413–424. [Google Scholar] [CrossRef] [PubMed]
- Fang, D.; Liu, Y.; Dou, D.; Su, B. The unique immune evasion mechanisms of the mpox virus and their implication for developing new vaccines and immunotherapies. Virol. Sin. 2024, 39, 709–718. [Google Scholar] [CrossRef]
- Branda, F.; Romano, C.; Ciccozzi, M.; Giovanetti, M.; Scarpa, F.; Ciccozzi, A.; Maruotti, A. Mpox: An Overview of Pathogenesis, Diagnosis, and Public Health Implications. J. Clin. Med. 2024, 13, 2234. [Google Scholar] [CrossRef]
- Griffin, B.D.; Corredor, J.C.; Pei, Y.; Nagy, E. Downregulation of Cell Surface Major Histocompatibility Complex Class I Expression Is Mediated by the Left-End Transcription Unit of Fowl Adenovirus 9. Viruses 2021, 13, 2211. [Google Scholar] [CrossRef]
- Lum, F.M.; Torres-Ruesta, A.; Tay, M.Z.; Lin, R.T.P.; Lye, D.C.; Renia, L.; Ng, L.F.P. Monkeypox: Disease epidemiology, host immunity and clinical interventions. Nat. Rev. Immunol. 2022, 22, 597–613. [Google Scholar] [CrossRef]
- Elsheikh, R.; Makram, A.M.; Vasanthakumaran, T.; Tomar, S.; Shamim, K.; Tranh, N.D.; Elsheikh, S.S.; Van, N.T.; Huy, N.T. Monkeypox: A comprehensive review of a multifaceted virus. Infect. Med. 2023, 2, 74–88. [Google Scholar] [CrossRef]
- Qiu, J. An animal source of mpox emerges—And it’s a squirrel. Nature 2025, 640, 575–576. [Google Scholar] [CrossRef]
- Reynolds, M.G.; Carroll, D.S.; Karem, K.L. Factors affecting the likelihood of monkeypox’s emergence and spread in the post-smallpox era. Curr. Opin. Virol. 2012, 2, 335–343. [Google Scholar] [CrossRef]
- Zaucha, G.M.; Jahrling, P.B.; Geisbert, T.W.; Swearengen, J.R.; Hensley, L. The pathology of experimental aerosolized monkeypox virus infection in cynomolgus monkeys (Macaca fascicularis). Lab. Investig. 2001, 81, 1581–1600. [Google Scholar] [CrossRef]
- McCollum, A.M.; Shelus, V.; Hill, A.; Traore, T.; Onoja, B.; Nakazawa, Y.; Doty, J.B.; Yinka-Ogunleye, A.; Petersen, B.W.; Hutson, C.L.; et al. Epidemiology of Human Mpox—Worldwide, 2018–2021. MMWR Morb. Mortal. Wkly. Rep. 2023, 72, 68–72. [Google Scholar] [CrossRef]
- Adebisi, Y.A.; Ezema, S.M.; Bolarinwa, O.; Bassey, A.E.; Ogunkola, I.O. Sex Workers and the Mpox Response in Africa. J. Infect. Dis. 2024, 230, 786–788. [Google Scholar] [CrossRef] [PubMed]
- Sampson, M.M.; Magee, G.; Schrader, E.A.; Dantuluri, K.L.; Bukhari, A.; Passaretti, C.; Temming, L.; Leonard, M.; Philips, J.B.; Weinrib, D. Mpox (Monkeypox) Infection During Pregnancy. Obs. Gynecol. 2023, 141, 1007–1010. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, D.A.; Pittman, P.R. Mpox (Monkeypox) in Pregnancy: Viral Clade Differences and Their Associations with Varying Obstetrical and Fetal Outcomes. Viruses 2023, 15, 1649. [Google Scholar] [CrossRef] [PubMed]
- Thornhill, J.P.; Barkati, S.; Walmsley, S.; Rockstroh, J.; Antinori, A.; Harrison, L.B.; Palich, R.; Nori, A.; Reeves, I.; Habibi, M.S.; et al. Monkeypox Virus Infection in Humans across 16 Countries—April–June 2022. N. Engl. J. Med. 2022, 387, 679–691. [Google Scholar] [CrossRef]
- Miller, M.J.; Cash-Goldwasser, S.; Marx, G.E.; Schrodt, C.A.; Kimball, A.; Padgett, K.; Noe, R.S.; McCormick, D.W.; Wong, J.M.; Labuda, S.M.; et al. Severe Monkeypox in Hospitalized Patients—United States, August 10–October 10, 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 1412–1417. [Google Scholar] [CrossRef]
- Fox, T.; Gould, S.; Princy, N.; Rowland, T.; Lutje, V.; Kuehn, R. Therapeutics for treating mpox in humans. Cochrane Database Syst. Rev. 2023, 3, CD015769. [Google Scholar] [CrossRef]
- Rao, A.K.; Schrodt, C.A.; Minhaj, F.S.; Waltenburg, M.A.; Cash-Goldwasser, S.; Yu, Y.; Petersen, B.W.; Hutson, C.; Damon, I.K. Interim Clinical Treatment Considerations for Severe Manifestations of Mpox—United States, February 2023. MMWR Morb Mortal. Wkly. Rep. 2023, 72, 232–243. [Google Scholar] [CrossRef]
- Saldana, C.S.; Kelley, C.F.; Aldred, B.M.; Cantos, V.D. Mpox and HIV: A Narrative Review. Curr. HIV/AIDS Rep. 2023, 20, 261–269. [Google Scholar] [CrossRef]
- Raadsen, M.P.; Dahlke, C.; Fathi, A.; Hardtke, S.; Klüver, M.; Krähling, V.; Gerresheim, G.K.; Mayer, L.; Mykytyn, A.Z.; Weskamm, L.M.; et al. Safety, immunogenicity, and optimal dosing of a modified vaccinia Ankara-based vaccine against MERS-CoV in healthy adults: A phase 1b, double-blind, randomised placebo-controlled clinical trial. Lancet Infect. Dis. 2025, 25, 231–242. [Google Scholar] [CrossRef]
- Ali, R.; Alonga, J.; Biampata, J.L.; Kombozi Basika, M.; Maljkovic Berry, I.; Bisento, N.; Blum, E.; Bonnett, T.; Cone, K.; Crozier, I.; et al. Tecovirimat for Clade I MPXV Infection in the Democratic Republic of Congo. N. Engl. J. Med. 2025, 392, 1484–1496. [Google Scholar] [CrossRef]
- Chenchula, S.; Atal, S.; Ghanta, M.K.; Uppugunduri, C.R.; Karunakaran, S.; Amerneni, K.C.; Sarma, P.; Prakash, S.; Amerneni, L.S.; Padmavathi, R.; et al. Emerging variants of Mpox virus and tecovirimat resistance: Genomic insights and implications for treatment strategies. Virology 2025, 608, 110532. [Google Scholar] [CrossRef]
- The Centers for Disease Control and Prevention. Preventing Mpox; The Centers for Disease Control and Prevention: Atlanta, GA, USA, 2024. Available online: https://www.cdc.gov/mpox/prevention/index.html (accessed on 4 July 2025).
- Bisanzio, D.; Davis, A.E.; Talbird, S.E.; Van Effelterre, T.; Metz, L.; Gaudig, M.; Mathieu, V.O.; Brogan, A.J. Targeted preventive vaccination campaigns to reduce Ebola outbreaks: An individual-based modeling study. Vaccine 2023, 41, 684–693. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Gu, Z.; Sheng, S.; Song, R.; Jin, R. The Current State and Progress of Mpox Vaccine Research. China CDC Wkly. 2024, 6, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Matusali, G.; Petruccioli, E.; Cimini, E.; Colavita, F.; Bettini, A.; Tartaglia, E.; Sbarra, S.; Meschi, S.; Lapa, D.; Francalancia, M.; et al. Evaluation of Cross-Immunity to the Mpox Virus Due to Historic Smallpox Vaccination. Vaccines 2023, 11, 1541. [Google Scholar] [CrossRef] [PubMed]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).