
Different Methods in HPV Genotyping of Anogenital and Oropharyngeal Lesions: Comparison between VisionArray® Technology, Next Generation Sequencing, and Hybrid Capture Assay

 , ,
, , 
Abstract
1. Introduction
2. Methods and Materials
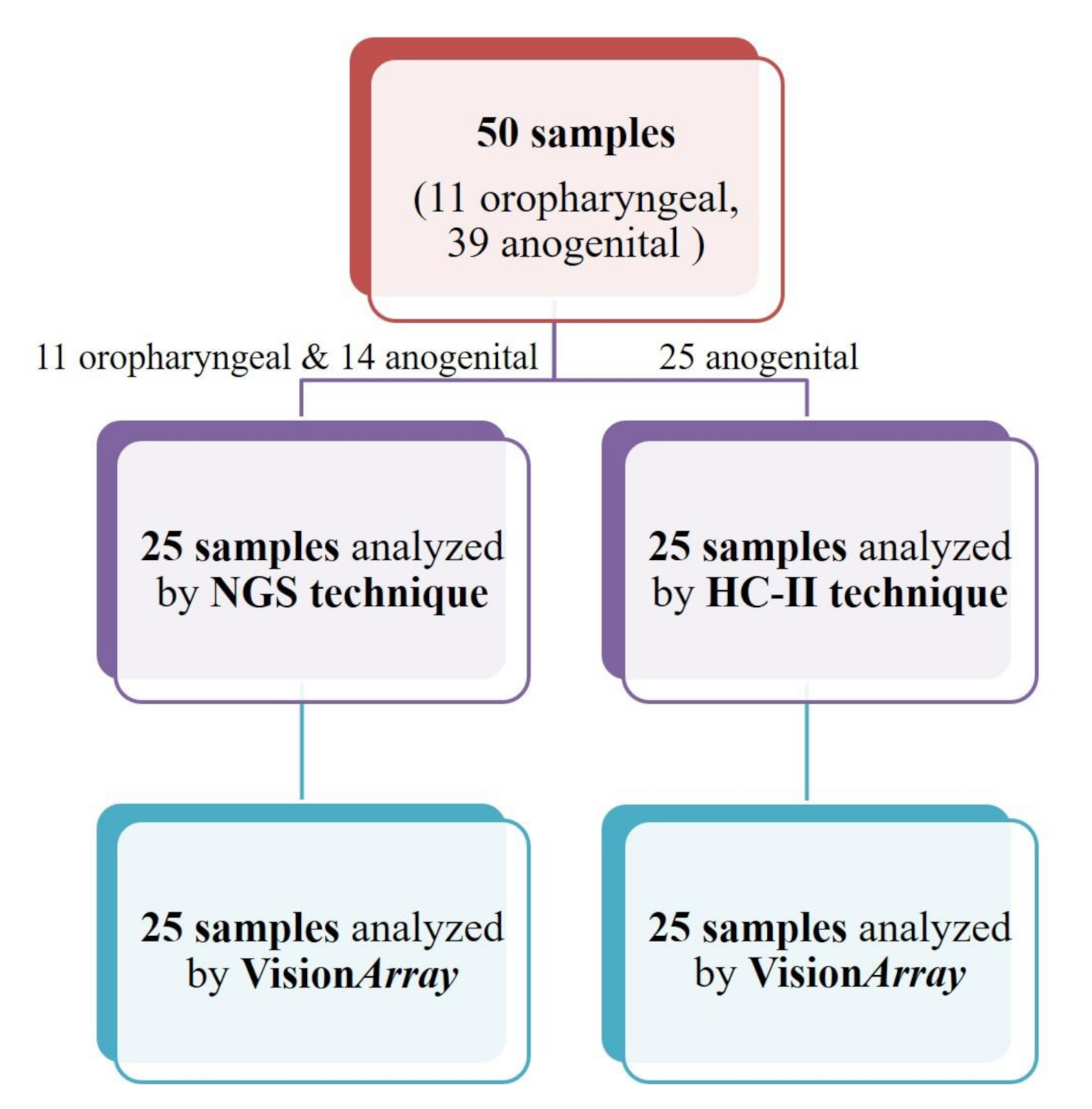
2.1. Sample Collection
2.2. DNA Extraction
2.3. Next Generation Sequencing
2.4. Hybrid Capture II
2.5. VisionArray® HPV Chips
2.6. Statistical Analysis
3. Results
3.1. Next Generation Sequencing and VisionArray® HPV Chips Analysis Comparison
3.1.1. Discrepant Results
3.1.2. Statistical Measures of Performance
3.2. Hybrid Capture II High-Risk HPV DNA Analysis and VisionArray® HPV Chips Analysis Comparison
3.2.1. Discrepant Results
3.2.2. Statistical Measures of Performance
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Schiller, J.T.; Day, P.M.; Kines, R.C. Current understanding of the mechanism of HPV infection. Gynecol. Oncol. 2010, 118, S12–S17. [Google Scholar] [CrossRef] [PubMed]
- de Martel, C.; Ferlay, J.; Franceschi, S.; Vignat, J.; Bray, F.; Forman, D.; Plummer, M. Global burden of cancers attributable to infections in 2008: A review and synthetic analysis. Lancet Oncol. 2012, 13, 607–615. [Google Scholar] [CrossRef]
- Forman, D.; de Martel, C.; Lacey, C.J.; Soerjomataram, I.; Lortet-Tieulent, J.; Bruni, L.; Vignat, J.; Ferlay, J.; Bray, F.; Plummer, M.; et al. Global burden of human papillomavirus and related diseases. Vaccine 2012, 30 (Suppl. 5), F12–F23. [Google Scholar] [CrossRef] [PubMed]
- zur Hausen, H. The search for infectious causes of human cancers: Where and why (Nobel lecture). Angew. Chem. Int. Ed. Engl. 2009, 48, 5798–5808. [Google Scholar] [CrossRef]
- Munoz, N.; Bosch, F.X.; de Sanjose, S.; Herrero, R.; Castellsague, X.; Shah, K.V.; Snijders, P.J.; Meijer, C.J. Epidemiologic classification of human papillomavirus types associated with cervical cancer. N. Engl. J. Med. 2003, 348, 518–527. [Google Scholar] [CrossRef]
- de Sanjose, S.; Diaz, M.; Castellsague, X.; Clifford, G.; Bruni, L.; Munoz, N.; Bosch, F.X. Worldwide prevalence and genotype distribution of cervical human papillomavirus DNA in women with normal cytology: A meta-analysis. Lancet Infect. Dis. 2007, 7, 453–459. [Google Scholar] [CrossRef]
- Bouvard, V.; Baan, R.; Straif, K.; Grosse, Y.; Secretan, B.; El Ghissassi, F.; Benbrahim-Tallaa, L.; Guha, N.; Freeman, C.; Galichet, L.; et al. A review of human carcinogens--Part B: Biological agents. Lancet Oncol. 2009, 10, 321–322. [Google Scholar] [CrossRef]
- Jacobs, M.V.; de Roda Husman, A.M.; van den Brule, A.J.; Snijders, P.J.; Meijer, C.J.; Walboomers, J.M. Group-specific differentiation between high- and low-risk human papillomavirus genotypes by general primer-mediated PCR and two cocktails of oligonucleotide probes. J. Clin. Microbiol. 1995, 33, 901–905. [Google Scholar] [CrossRef]
- van den Brule, A.J.; Pol, R.; Fransen-Daalmeijer, N.; Schouls, L.M.; Meijer, C.J.; Snijders, P.J. GP5+/6+ PCR followed by reverse line blot analysis enables rapid and high-throughput identification of human papillomavirus genotypes. J. Clin. Microbiol. 2002, 40, 779–787. [Google Scholar] [CrossRef]
- Davies, P.; Kornegay, J.; Iftner, T. Current methods of testing for human papillomavirus. Best Pract. Res. Clin. Obstet. Gynaecol. 2001, 15, 677–700. [Google Scholar] [CrossRef]
- Gravitt, P.E.; Peyton, C.L.; Apple, R.J.; Wheeler, C.M. Genotyping of 27 human papillomavirus types by using L1 consensus PCR products by a single-hybridization, reverse line blot detection method. J. Clin. Microbiol. 1998, 36, 3020–3027. [Google Scholar] [CrossRef]
- Human papillomavirus vaccines: WHO position paper, May 2017-Recommendations. Vaccine 2017, 35, 5753–5755. [CrossRef] [PubMed]
- Franceschi, S.; Herrero, R.; Clifford, G.M.; Snijders, P.J.; Arslan, A.; Anh, P.T.; Bosch, F.X.; Ferreccio, C.; Hieu, N.T.; Lazcano-Ponce, E.; et al. Variations in the age-specific curves of human papillomavirus prevalence in women worldwide. Int. J. Cancer 2006, 119, 2677–2684. [Google Scholar] [CrossRef] [PubMed]
- Rischin, D.; Young, R.J.; Fisher, R.; Fox, S.B.; Le, Q.T.; Peters, L.J.; Solomon, B.; Choi, J.; O’Sullivan, B.; Kenny, L.M.; et al. Prognostic significance of p16INK4A and human papillomavirus in patients with oropharyngeal cancer treated on TROG 02.02 phase III trial. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2010, 28, 4142–4148. [Google Scholar] [CrossRef]
- Ang, K.K.; Harris, J.; Wheeler, R.; Weber, R.; Rosenthal, D.I.; Nguyen-Tan, P.F.; Westra, W.H.; Chung, C.H.; Jordan, R.C.; Lu, C.; et al. Human papillomavirus and survival of patients with oropharyngeal cancer. N. Engl. J. Med. 2010, 363, 24–35. [Google Scholar] [CrossRef]
- Manos, M.M.; Ting, Y.; Wright, D.K.; Lewis, J.; Broker, T.R.; Wolinsky, S.M. The use of polymerase chain reaction amplification for the detection of genital human papillomaviruses. Cancer Cells 1989, 7, 209–214. [Google Scholar]
- Coutlee, F.; Gravitt, P.; Kornegay, J.; Hankins, C.; Richardson, H.; Lapointe, N.; Voyer, H.; Franco, E. Use of PGMY primers in L1 consensus PCR improves detection of human papillomavirus DNA in genital samples. J. Clin. Microbiol. 2002, 40, 902–907. [Google Scholar] [CrossRef]
- Snijders, P.J.; van den Brule, A.J.; Schrijnemakers, H.F.; Snow, G.; Meijer, C.J.; Walboomers, J.M. The use of general primers in the polymerase chain reaction permits the detection of a broad spectrum of human papillomavirus genotypes. J. Gen. Virol. 1990, 71 Pt 1, 173–181. [Google Scholar] [CrossRef]
- Fontaine, V.; Mascaux, C.; Weyn, C.; Bernis, A.; Celio, N.; Lefevre, P.; Kaufman, L.; Garbar, C. Evaluation of combined general primer-mediated PCR sequencing and type-specific PCR strategies for determination of human papillomavirus genotypes in cervical cell specimens. J. Clin. Microbiol. 2007, 45, 928–934. [Google Scholar] [CrossRef]
- Cullen, M.; Boland, J.F.; Schiffman, M.; Zhang, X.; Wentzensen, N.; Yang, Q.; Chen, Z.; Yu, K.; Mitchell, J.; Roberson, D.; et al. Deep sequencing of HPV16 genomes: A new high-throughput tool for exploring the carcinogenicity and natural history of HPV16 infection. Papillomavirus Res. 2015, 1, 3–11. [Google Scholar] [CrossRef]
- Lee, J.Y.; Cutts, R.J.; White, I.; Augustin, Y.; Garcia-Murillas, I.; Fenwick, K.; Matthews, N.; Turner, N.C.; Harrington, K.; Gilbert, D.C.; et al. Next Generation Sequencing Assay for Detection of Circulating HPV DNA (cHPV-DNA) in Patients Undergoing Radical (Chemo)Radiotherapy in Anal Squamous Cell Carcinoma (ASCC). Front. Oncol. 2020, 10, 505. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Unger, E.R.; Rajeevan, M.S. Universal human papillomavirus typing by whole genome sequencing following target enrichment: Evaluation of assay reproducibility and limit of detection. BMC Genom. 2019, 20, 231. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Unger, E.R.; Batra, D.; Sheth, M.; Steinau, M.; Jasinski, J.; Jones, J.; Rajeevan, M.S. Universal Human Papillomavirus Typing Assay: Whole-Genome Sequencing following Target Enrichment. J. Clin. Microbiol. 2017, 55, 811–823. [Google Scholar] [CrossRef] [PubMed]
- Montgomery, N.D.; Parker, J.S.; Eberhard, D.A.; Patel, N.M.; Weck, K.E.; Sharpless, N.E.; Hu, Z.; Hayes, D.N.; Gulley, M.L. Identification of Human Papillomavirus Infection in Cancer Tissue by Targeted Next-generation Sequencing. Appl. Immunohistochem. Mol. Morphol. 2016, 24, 490–495. [Google Scholar] [CrossRef] [PubMed]
- Kocjan, B.J.; Bzhalava, D.; Forslund, O.; Dillner, J.; Poljak, M. Molecular methods for identification and characterization of novel papillomaviruses. Clin. Microbiol. Infect. 2015, 21, 808–816. [Google Scholar] [CrossRef] [PubMed]
- Chandrani, P.; Kulkarni, V.; Iyer, P.; Upadhyay, P.; Chaubal, R.; Das, P.; Mulherkar, R.; Singh, R.; Dutt, A. NGS-based approach to determine the presence of HPV and their sites of integration in human cancer genome. Br. J. Cancer 2015, 112, 1958–1965. [Google Scholar] [CrossRef] [PubMed]
- Nowak, R.G.; Ambulos, N.P.; Schumaker, L.M.; Mathias, T.J.; White, R.A.; Troyer, J.; Wells, D.; Charurat, M.E.; Bentzen, S.M.; Cullen, K.J. Genotyping of high-risk anal human papillomavirus (HPV): Ion torrent-next generation sequencing vs. linear array. Virol. J. 2017, 14, 112. [Google Scholar] [CrossRef]
- Nilyanimit, P.; Chansaenroj, J.; Poomipak, W.; Praianantathavorn, K.; Payungporn, S.; Poovorawan, Y. Comparison of Four Human Papillomavirus Genotyping Methods: Next-generation Sequencing, INNO-LiPA, Electrochemical DNA Chip, and Nested-PCR. Ann. Lab. Med. 2018, 38, 139–146. [Google Scholar] [CrossRef]
- Flores-Miramontes, M.G.; Torres-Reyes, L.A.; Alvarado-Ruiz, L.; Romero-Martinez, S.A.; Ramirez-Rodriguez, V.; Balderas-Pena, L.M.; Vallejo-Ruiz, V.; Pina-Sanchez, P.; Cortes-Gutierrez, E.I.; Jave-Suarez, L.F.; et al. Human papillomavirus genotyping by Linear Array and Next-Generation Sequencing in cervical samples from Western Mexico. Virol. J. 2015, 12, 161. [Google Scholar] [CrossRef]
- Dias, T.C.; Longatto-Filho, A.; Campanella, N.C. Human papillomavirus genotyping as a tool for cervical cancer prevention: From commercially available human papillomavirus DNA test to next-generation sequencing. Future Sci. OA 2020, 6, FSO603. [Google Scholar] [CrossRef]
- Barzon, L.; Militello, V.; Lavezzo, E.; Franchin, E.; Peta, E.; Squarzon, L.; Trevisan, M.; Pagni, S.; Dal Bello, F.; Toppo, S.; et al. Human papillomavirus genotyping by 454 next generation sequencing technology. J. Clin. Virol. 2011, 52, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Arroyo, L.S.; Smelov, V.; Bzhalava, D.; Eklund, C.; Hultin, E.; Dillner, J. Next generation sequencing for human papillomavirus genotyping. J. Clin. Virol. 2013, 58, 437–442. [Google Scholar] [CrossRef] [PubMed]
- Arroyo Muhr, L.S.; Hultin, E.; Bzhalava, D.; Eklund, C.; Lagheden, C.; Ekstrom, J.; Johansson, H.; Forslund, O.; Dillner, J. Human papillomavirus type 197 is commonly present in skin tumors. Int. J. Cancer 2015, 136, 2546–2555. [Google Scholar] [CrossRef]
- de Roda Husman, A.M.; Walboomers, J.M.; van den Brule, A.J.; Meijer, C.J.; Snijders, P.J. The use of general primers GP5 and GP6 elongated at their 3’ ends with adjacent highly conserved sequences improves human papillomavirus detection by PCR. J. Gen. Virol. 1995, 76 Pt 4, 1057–1062. [Google Scholar] [CrossRef]
- Lee, S.H.; Vigliotti, V.S.; Vigliotti, J.S.; Pappu, S. Validation of human papillomavirus genotyping by signature DNA sequence analysis. BMC Clin. Pathol. 2009, 9, 3. [Google Scholar] [CrossRef] [PubMed]
- Craig, S.G.; Anderson, L.A.; Schache, A.G.; Moran, M.; Graham, L.; Currie, K.; Rooney, K.; Robinson, M.; Upile, N.S.; Brooker, R.; et al. Recommendations for determining HPV status in patients with oropharyngeal cancers under TNM8 guidelines: A two-tier approach. Br. J. Cancer 2019, 120, 827–833. [Google Scholar] [CrossRef]
- Ambulos, N.P., Jr.; Schumaker, L.M.; Mathias, T.J.; White, R.; Troyer, J.; Wells, D.; Cullen, K.J. Next-Generation Sequencing-Based HPV Genotyping Assay Validated in Formalin-Fixed, Paraffin-Embedded Oropharyngeal and Cervical Cancer Specimens. J. Biomol. Tech. 2016, 27, 46–52. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Conway, C.; Chalkley, R.; High, A.; Maclennan, K.; Berri, S.; Chengot, P.; Alsop, M.; Egan, P.; Morgan, J.; Taylor, G.R.; et al. Next-generation sequencing for simultaneous determination of human papillomavirus load, subtype, and associated genomic copy number changes in tumors. J. Mol. Diagn. 2012, 14, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Eklund, C.; Forslund, O.; Wallin, K.L.; Dillner, J. Global improvement in genotyping of human papillomavirus DNA: The 2011 HPV LabNet International Proficiency Study. J. Clin. Microbiol. 2014, 52, 449–459. [Google Scholar] [CrossRef]


{kind=link}
| Sample | Sex | Age | Sample Type | Site Region |
|---|---|---|---|---|
| S1 | M | 43 | FrB | Anogenital-Anus |
| S2 | M | 45 | FrB | Anogenital-Anus |
| S3 | F | 34 | FrB | Anogenital-Anus |
| S4 | M | 61 | FFPE | Oropharyngeal-Lymph node |
| S5 | M | 67 | FFPE | Oropharyngeal-Tonsil |
| S6 | F | 24 | FrB | Anogenital-Cervix |
| S7 | M | 57 | FFPE | Oropharyngeal-Lymph node |
| S8 | F | 60 | FFPE | Anogenital-Anus |
| S9 | F | 43 | FrB | Anogenital-Anus |
| S10 | M | 41 | FFPE | Oropharyngeal-Tonsil |
| S11 | F | 48 | FrB | Anogenital-Anus |
| S12 | F | 20 | FrB | Anogenital-Anus |
| S13 | M | 53 | FrB | Anogenital-Anus |
| S14 | F | 66 | FFPE | Oropharyngeal-Tonsil |
| S15 | F | 69 | FFPE | Oropharyngeal-Tonsil |
| S16 | M | 66 | FFPE | Oropharyngeal-Tongue |
| S17 | M | 70 | FrB | Anogenital-Anus |
| S18 | F | 63 | FFPE | Oropharyngeal-Tonsil |
| S19 | F | 39 | FrB | Anogenital-Anus |
| S20 | F | 44 | FrB^ | Anogenital-Cervix |
| S21 | F | 28 | FFPE | Anogenital-Anus |
| S22 | M | 55 | FFPE | Oropharyngeal-Lymph node |
| S23 | M | 28 | FrB | Anogenital-Anus |
| S24 | M | 42 | FFPE | Oropharyngeal-Tongue |
| S25 | F | 53 | FFPE | Oropharyngeal-Tonsil |
| S26 | F | 19 | FrB | Anogenital-Cervix |
| S27 | F | 61 | FrB | Anogenital-Cervix |
| S28 | F | 32 | FrB | Anogenital-Cervix |
| S29 | F | 61 | FrB | Anogenital-Cervix |
| S30 | F | 39 | FrB | Anogenital-Cervix |
| S31 | F | 46 | FrB | Anogenital-Cervix |
| S32 | F | 30 | FrB | Anogenital-Cervix |
| S33 | F | 33 | FrB | Anogenital-Cervix |
| S34 | F | 46 | FrB | Anogenital-Cervix |
| S35 | F | 31 | FrB | Anogenital-Cervix |
| S36 | F | 49 | FrB | Anogenital-Cervix |
| S37 | F | 45 | FrB | Anogenital-Cervix |
| S38 | F | 46 | FrB | Anogenital-Cervix |
| S39 | F | 70 | FrB | Anogenital-Cervix |
| S40 | F | 59 | FrB | Anogenital-Cervix |
| S41 | F | 48 | FrB | Anogenital-Cervix |
| S42 | F | 21 | FrB | Anogenital-Cervix |
| S43 | F | 40 | FrB | Anogenital-Cervix |
| S44 | F | 33 | FrB | Anogenital-Cervix |
| S45 | F | 32 | FrB | Anogenital-Cervix |
| S46 | F | 46 | FrB | Anogenital-Cervix |
| S47 | F | 46 | FrB | Anogenital-Cervix |
| S48 | F | 33 | FrB | Anogenital-Cervix |
| S49 | F | 41 | FrB | Anogenital-Cervix |
| S50 | F | 33 | FrB | Anogenital-Cervix |
| Sample | NGS | VisionArray® | Site Region |
|---|---|---|---|
| S1 | HPV11 | HPV11 | Anogenital-Anus |
| S2 | Neg | Neg | Anogenital-Anus |
| S3 | Neg | Neg | Anogenital-Anus |
| S4 * | NE | Neg | Oropharyngeal-Lymph node |
| S5 * | NE | HPV16+42 | Oropharyngeal-Tonsil |
| S6 * | HPV6+66 | HPV6+66+61+73+82+90 | Anogenital-Cervix |
| S7 * | NE | HPV16 | Oropharyngeal-Lymph node |
| S8 | HPV16 | HPV16 | Anogenital-Anus |
| S9 | HPV11 | HPV11 | Anogenital-Anus |
| S10 | Neg | Neg | Oropharyngeal-Tonsil |
| S11 | HPV6 | HPV6 | Anogenital-Anus |
| S12 | Neg | Neg | Anogenital-Anus |
| S13 | HPV33+54 | HPV33+54 | Anogenital-Anus |
| S14 | Neg | Neg | Oropharyngeal-Tonsil |
| S15 | HPV35 | HPV35 | Oropharyngeal-Tonsil |
| S16 | HPV33 | HPV33 | Oropharyngeal-Tongue |
| S17 | HPV6 | HPV6 | Anogenital-Anus |
| S18 | HPV16 | HPV16 | Oropharyngeal-Tonsil |
| S19 | Neg | Neg | Anogenital-Anus |
| S20 | Neg | Neg | Anogenital-Cervix |
| S21 * | Neg | HPV40 | Anogenital-Anus |
| S22 * | HPV35 | HPV35+34 | Oropharyngeal-Lymph node |
| S23 | HPV6+91 | HPV6+91 | Anogenital-Anus |
| S24 | Neg | Neg | Oropharyngeal-Tongue |
| S25 | HPV35 | HPV35 | Oropharyngeal-Tonsil |
| VisionArray® vs. NGS | Sensitivity | Specificity | Overall Accuracy | PPV | NPV | Concordance (Cohen’s κ) (95% CI) |
|---|---|---|---|---|---|---|
| Positive: HR+PHR+LR | 0.81 | 1.0 | 0.84 | 1.0 | 0.75 | 0.702 (0.44–0.97) |
| Positive: HR | 0.78 | 1.0 | 0.92 | 1.0 | 0.89 | 0.779 (0.55–1.0) |
| Positive: HR/PHR | 0.73 | 1.0 | 0.88 | 1.0 | 0.82 | 0.775 (0.56–0.99) |
| HR/PHR/LR | 0.81 | 1.0 | 0.84 | 1.0 | 0.75 | 0.818 (0.62–1.0) |
| Sample | HC | VisionArray® | Site Region |
|---|---|---|---|
| S26 * | Neg | HPV42 | Anogenital-Cervix |
| S27 * | Neg | HPV55 | Anogenital-Cervix |
| S28 * | Neg | HPV42 | Anogenital-Cervix |
| S29 | Neg | Neg | Anogenital-Cervix |
| S30 * | Neg | 16+42 | Anogenital-Cervix |
| S31 * | Neg | HPV6+11+53 | Anogenital-Cervix |
| S32 | Neg | Neg | Anogenital-Cervix |
| S33 | Neg | Neg | Anogenital-Cervix |
| S34 | Neg | Neg | Anogenital-Cervix |
| S35 | Neg | Neg | Anogenital-Cervix |
| S36 | Neg | Neg | Anogenital-Cervix |
| S37 | Neg | Neg | Anogenital-Cervix |
| S38 | Neg | Neg | Anogenital-Cervix |
| S39 | Pos | HPV16 | Anogenital-Cervix |
| S40 | Pos | HPV35 | Anogenital-Cervix |
| S41 | Pos | HPV51 | Anogenital-Cervix |
| S42 | Pos | HPV56 | Anogenital-Cervix |
| S43 | Pos | HPV56 | Anogenital-Cervix |
| S44 | Pos | HPV16+39 | Anogenital-Cervix |
| S45 | Pos | HPV16+52+53 | Anogenital-Cervix |
| S46 | Pos | HPV16+54+56+66 | Anogenital-Cervix |
| S47 | Pos | HPV16+61 | Anogenital-Cervix |
| S48 | Pos | HPV16+18 | Anogenital-Cervix |
| S49 * | Pos | HPV40+42+44+54 | Anogenital-Cervix |
| S50 | Pos | HPV6+31 | Anogenital-Cervix |
| VisionArray® vs. HC II | Sensitivity | Specificity | Overall Accuracy | PPV | NPV | Concordance (Cohen’s κ) (95% CI) |
|---|---|---|---|---|---|---|
| Positive HR+PHR+LR | 0.71 | 1.0 | 0.80 | 1.0 | 0.62 | 0.606 (0.32–0.89) |
| Positive: HR | 0.92 | 0.92 | 0.92 | 0.92 | 0.92 | 0.84 (0.63–1.0) |
| Positive: HR/PHR | 0.85 | 0.92 | 0.88 | 0.92 | 0.85 | 0.76 (0.51–1.0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Acquaviva, G.; Visani, M.; Sanza, V.; De Leo, A.; Maloberti, T.; Pierotti, P.; Crucitti, P.; Collina, G.; Chiarelli Olivari, C.; Pession, A.; et al. Different Methods in HPV Genotyping of Anogenital and Oropharyngeal Lesions: Comparison between VisionArray® Technology, Next Generation Sequencing, and Hybrid Capture Assay. J. Mol. Pathol. 2021, 2, 29-41. https://doi.org/10.3390/jmp2010004
Acquaviva G, Visani M, Sanza V, De Leo A, Maloberti T, Pierotti P, Crucitti P, Collina G, Chiarelli Olivari C, Pession A, et al. Different Methods in HPV Genotyping of Anogenital and Oropharyngeal Lesions: Comparison between VisionArray® Technology, Next Generation Sequencing, and Hybrid Capture Assay. Journal of Molecular Pathology. 2021; 2(1):29-41. https://doi.org/10.3390/jmp2010004
Chicago/Turabian StyleAcquaviva, Giorgia, Michela Visani, Viviana Sanza, Antonio De Leo, Thais Maloberti, Paola Pierotti, Paola Crucitti, Guido Collina, Cecilia Chiarelli Olivari, Annalisa Pession, and et al. 2021. "Different Methods in HPV Genotyping of Anogenital and Oropharyngeal Lesions: Comparison between VisionArray® Technology, Next Generation Sequencing, and Hybrid Capture Assay" Journal of Molecular Pathology 2, no. 1: 29-41. https://doi.org/10.3390/jmp2010004
APA StyleAcquaviva, G., Visani, M., Sanza, V., De Leo, A., Maloberti, T., Pierotti, P., Crucitti, P., Collina, G., Chiarelli Olivari, C., Pession, A., Tallini, G., & de Biase, D. (2021). Different Methods in HPV Genotyping of Anogenital and Oropharyngeal Lesions: Comparison between VisionArray® Technology, Next Generation Sequencing, and Hybrid Capture Assay. Journal of Molecular Pathology, 2(1), 29-41. https://doi.org/10.3390/jmp2010004