
A Retrospective Study of the Effects of Traumatic Brain Injury on Auditory Function: From a Clinical Perspective

Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Data Collection
2.3. Statistical Analysis
3. Results
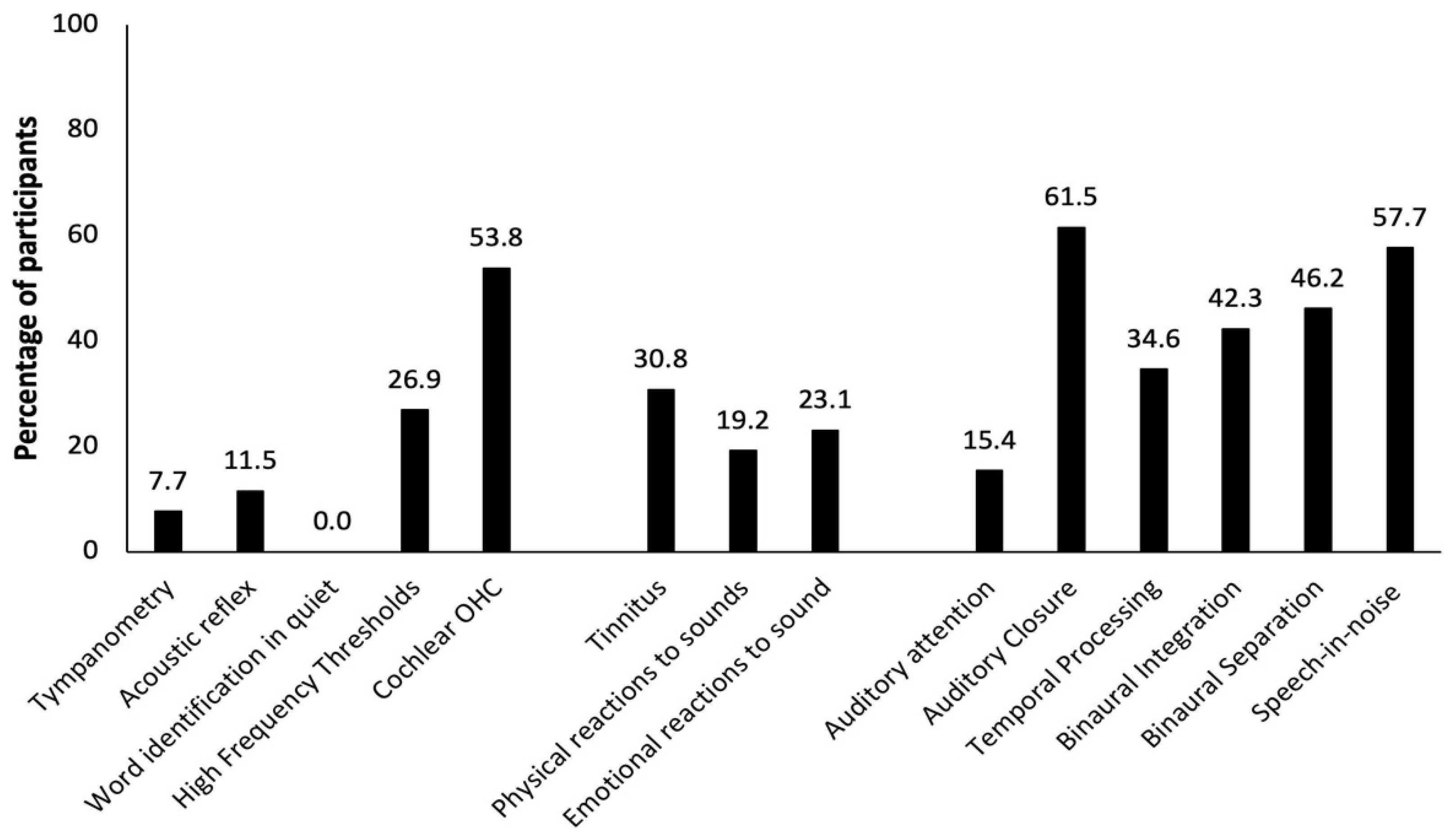
3.1. Auditory Dysfunction in TBI Participants
3.2. Relation between TBIs and Auditory Dysfunction
4. Discussion
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Analysis | Sub-Categories | No. of TBIs Sustained | Type of TBIs Sustained | ||
|---|---|---|---|---|---|
| Single (n = 16) | Multiple (n = 10) | Blunt Force (n = 20) | Blast Force (n = 6) | ||
| Reason for visit | Physician’s referral | 4 | 3 | 5 | 5 |
| Hearing difficulties | 12 | 7 | 15 | 1 | |
| Auditory issues prior to TBI | Yes (middle ear infections as a child) | - | 3 | 3 | - |
| No | 15 | 6 | 16 | 5 | |
| Unknown | 1 | 1 | 1 | 1 | |
| Type of Injury | Explosions | 2 | 4 | - | 6 |
| Motor Vehicle Accidents (MVA) | 6 | 3 | 9 | - | |
| Falls | 4 | - | 4 | - | |
| Assault and contact sports | 2 | 2 | 4 | - | |
| Unknown | 2 | - | 2 | - | |
| Degree of Severity (for multiple TBIs, the most severe injury is listed) | Mild | 7 | - | 7 | - |
| Moderate | 4 | 2 | 4 | 2 | |
| Severe | 1 | 3 | 3 | 1 | |
| Unknown | 4 | 5 | 6 | 3 | |
| Specifics of Injury (on blunt force trauma) | Whiplash | - | - | 9 | - |
| Blow to the back of the head | - | - | 5 | - | |
| Blow to the side of the head | - | - | 3 | - | |
| Hit from the top of the head (neck compression component) | - | - | 1 | - | |
| Hit on the forehead | - | - | 1 | - | |
| Unknown | - | - | 1 | - | |
| Time since injury (time since the most severe injury for multiple TBIs) | 1 year or less | 4 | - | 4 | - |
| Between 2 to 5 years | 4 | - | 4 | - | |
| 6 years or more | 6 | 8 | 9 | 5 | |
| Unknown | 2 | 2 | 3 | 1 | |
| Cognition pre-injury | Learning Impairment | 3 | 1 | 2 | 1 |
| Unknown | 1 | 5 | 6 | 2 | |
| Excellent | 12 | 4 | 12 | 3 | |
| Cognition post-injury | Slow processing speed | 8 | 3 | 9 | 2 |
| Disoriented | 1 | 2 | 1 | 1 | |
| Difficulty concentrating | 7 | 5 | 7 | 4 | |
| Some memory issues | 4 | 2 | 6 | - | |
| Unknown | 3 | 3 | 7 | 2 | |
| Other sensory disturbances | Vision/Light sensitivity | 10 | 4 | 13 | 2 |
| Smell | 3 | - | 3 | 1 | |
| None | - | 2 | 1 | 3 | |
| Unknown | 4 | 1 | 4 | - | |
| Otoscopy Results | Normal both ears | 15 | 9 | 19 | 5 |
| Abnormal both ears | 1 | - | 1 | - | |
| Unknown | - | 1 | - | 1 | |
| Tympanometry | Within normal limits | 12 | 5 | 16 | 1 |
| Abnormal | 1 | 1 | 2 | - | |
| Unknown | 3 | 4 | 2 | 5 | |
| Acoustic Reflex | Normal both ears | 9 | 4 | 12 | 1 |
| Elevated or absent in either ear | 1 | 2 | 3 | - | |
| Unknown | 6 | 4 | 5 | 5 | |
| Cochlear Hair Cells Functions (DPOAE) | Normal | 3 | 1 | 4 | - |
| Abnormal | 7 | 8 | 10 | 5 | |
| Unknown | 6 | 1 | 6 | 1 | |
References
- Gold, E.M.; Su, D.; López-Velázquez, L.; Haus, D.L.; Perez, H.; Lacuesta, G.A.; Anderson, A.J.; Cummings, B.J. Functional Assessment of Long-Term Deficits in Rodent Models of Traumatic Brain Injury. Regen. Med. 2013, 8, 483–516. [Google Scholar] [CrossRef]
- Cernak, I.; Wang, Z.; Jiang, J.; Bian, X.; Savic, J. Ultrastructural and Functional Characteristics of Blast Injury-Induced Neurotrauma. J. Trauma Acute Care Surg. 2001, 50, 695–706. [Google Scholar] [CrossRef] [PubMed]
- Dang, B.; Chen, W.; He, W.; Chen, G. Rehabilitation Treatment and Progress of Traumatic Brain Injury Dysfunction. Neural Plast. 2017, 1–6. [Google Scholar] [CrossRef]
- McAllister, T.W. Neurobiological Consequences of Traumatic Brain Injury. Dialogues Clin. Neurosci. 2011, 13, 287. [Google Scholar] [PubMed]
- Teasdale, G.; Jennett, B. Assessment of Coma and Impaired Consciousness. Lancet 1974, 304, 81–84. [Google Scholar] [CrossRef]
- Wang, K.K.; Yang, Z.; Zhu, T.; Shi, Y.; Rubenstein, R.; Tyndall, J.A.; Manley, G.T. An Update on Diagnostic and Prognostic Biomarkers for Traumatic Brain Injury. Expert Rev. Mol. Diagn. 2018, 18, 165–180. [Google Scholar] [CrossRef] [PubMed]
- Phillips, Y.Y. Primary Blast Injuries. Ann. Emerg. Med. 1986, 15, 1446–1450. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Explosions and Blast Injuries: A Primer for Clinicians. CDC Atlanta GA 2003. Available online: https://www.cdc.gov/masstrauma/preparedness/primer.pdf (accessed on 28 December 2021).
- Cernak, I. Understanding Blast-Induced Neurotrauma: How Far Have We Come? Concussion 2017, 2, 1–19. [Google Scholar] [CrossRef]
- Hunter, J.; Ch, M. Sections of Surgery and Pathology. Proc. R. Soc. Med. 1941, 34, 171–192. [Google Scholar]
- Hicks, R.R.; Fertig, S.J.; Desrocher, R.E.; Koroshetz, W.J.; Pancrazio, J.J. Neurological Effects of Blast Injury. J. Trauma Inj. Infect. Crit. Care 2010, 68, 1257–1263. [Google Scholar] [CrossRef]
- Kocsis, J.D.; Tessler, A. Pathology of Blast-Related Brain Injury. JRRD 2009, 46, 667. [Google Scholar] [CrossRef]
- Mirza, R.; Kirchner, D.B.; Dobie, R.A.; Crawford, J.; ACOEM Task Force on Occupational Hearing Loss. Occupational Noise-Induced Hearing Loss. J. Occup. Environ. Med. 2018, 60, 498–501. [Google Scholar] [CrossRef] [PubMed]
- Mao, H.; Chen, Y. Noise-Induced Hearing Loss: Updates on Molecular Targets and Potential Interventions. Neural Plast. 2021, 2021, 4784385. [Google Scholar] [CrossRef]
- Lew, H.L. Auditory Dysfunction in Traumatic Brain Injury. J. Rehabil. Res. Dev. 2007, 44, 921–928. [Google Scholar] [CrossRef]
- Simon, L.V.; Lopez, R.A.; King, K.C. Blunt Force Trauma. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. Available online: https://www.ncbi.nlm.nih.gov/books/NBK470338/ (accessed on 11 August 2021).
- Young, L.A.; Rule, G.T.; Bocchieri, R.T.; Burns, J.M. Biophysical Mechanisms of Traumatic Brain Injuries. Semin. Neurol. 2015, 35, 5–11. [Google Scholar]
- Faul, M.; Xu, L.; Wald, M.M.; Coronado, V.G. Traumatic Brain Injury in the United States; Emergency Department Visits, Hospitalizations, and Deaths 2002–2006 Atlanta (GA). Cent. Dis. Control Prev. Natl. Cent. Inj. Prev. Control 2010, 17–21. [Google Scholar]
- Das, M.; Mayilsamy, K.; Mohapatra, S.S.; Mohapatra, S. Mesenchymal Stem Cell Therapy for the Treatment of Traumatic Brain Injury: Progress and Prospects. Rev. Neurosci. 2019, 30, 839–855. [Google Scholar] [CrossRef] [PubMed]
- Haydel, M.J.; Burns, B. Blunt Head Trauma. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Trakimas, D.R.; Knoll, R.M.; Ishai, R.; Lee, D.J.; Jung, D.H.; Nadol, J.B.; Remenschneider, A.K.; Kozin, E.D. Otopathology of Unilateral Cochlear Implantation in Patients with Bilateral Temporal Bone Fracture. Otol. Neurotol. 2019, 40, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Zehnder, A.; Merchant, S.N. Transverse Fracture of the Temporal Bone. Otol. Neurotol. 2004, 25, 852–853. [Google Scholar] [CrossRef]
- Lubner, R.J.; Knoll, R.M.; Trakimas, D.R.; Bartholomew, R.A.; Lee, D.J.; Walters, B.; Nadol, J.B.; Remenschneider, A.K.; Kozin, E.D. Long-term Cochlear Implantation Outcomes in Patients Following Head Injury. Laryngoscope Investig. Otolaryngol. 2020, 5, 485–496. [Google Scholar] [CrossRef] [PubMed]
- Rao, D.P.; McFaull, S.; Thompson, W.; Jayaraman, G.C. Trends in Self-Reported Traumatic Brain Injury among Canadians, 2005–2014: A Repeated Cross-Sectional Analysis. CMAJ Open 2017, 5, 301–307. [Google Scholar] [CrossRef]
- Roebuck-Spencer, T.; Cernich, A. Epidemiology and Societal Impact of Traumatic Brain Injury. In Handbook on the Neuropsychology of Traumatic Brain Injury; Springer: New York, NY, USA, 2014; pp. 3–23. [Google Scholar]
- Oleksiak, M.; Smith, B.M.; Andre, J.R.S.; Caughlan, C.M.; Steiner, M. Audiological Issues and Hearing Loss among Veterans with Mild Traumatic Brain Injury. J. Rehabil. Res. Dev. 2012, 49, 995–1003. [Google Scholar] [CrossRef]
- Assi, H.; Moore, R.D.; Ellemberg, D.; Hébert, S. Sensitivity to Sounds in Sport-Related Concussed Athletes: A New Clinical Presentation of Hyperacusis. Sci. Rep. 2018, 8, 9921. [Google Scholar] [CrossRef]
- Bergemalm, P.-O.; Borg, E. Peripheral and Central Audiological Sequelae of Closed Head Injury: Function, Activity, Participation and Quality of Life. Audiol. Med. 2005, 3, 185–198. [Google Scholar] [CrossRef]
- Hoover, E.C.; Souza, P.E.; Gallun, F.J. Auditory and Cognitive Factors Associated with Speech-in-Noise Complaints Following Mild Traumatic Brain Injury. J. Am. Acad. Audiol. 2017, 28, 325–339. [Google Scholar] [CrossRef] [PubMed]
- Kraus, N.; Lindley, T.; Colegrove, D.; Krizman, J.; Otto-Meyer, S.; Thompson, E.C.; White-Schwoch, T. The Neural Legacy of a Single Concussion. Neurosci. Lett. 2017, 646, 21–23. [Google Scholar] [CrossRef] [PubMed]
- Thompson, E.C.; Krizman, J.; White-Schwoch, T.; Nicol, T.; LaBella, C.R.; Kraus, N. Difficulty Hearing in Noise: A Sequela of Concussion in Children. Brain Inj. 2018, 32, 763–769. [Google Scholar] [CrossRef] [PubMed]
- Vander Werff, K.R.; Rieger, B. Auditory and Cognitive Behavioral Performance Deficits and Symptom Reporting in Postconcussion Syndrome Following Mild Traumatic Brain Injury. J. Speech Lang. Hear. Res. 2019, 62, 2501–2518. [Google Scholar] [CrossRef]
- Clifford, R.E.; Baker, D.; Risbrough, V.B.; Huang, M.; Yurgil, K.A. Impact of TBI, PTSD, and Hearing Loss on Tinnitus Progression in a US Marine Cohort. Mil. Med. 2019, 184, 839–846. [Google Scholar] [CrossRef]
- Swan, A.A.; Nelson, J.T.; Swiger, B.; Jaramillo, C.A.; Eapen, B.C.; Packer, M.; Pugh, M.J. Prevalence of Hearing Loss and Tinnitus in Iraq and Afghanistan Veterans: A Chronic Effects of Neurotrauma Consortium Study. Hear. Res. 2017, 349, 4–12. [Google Scholar] [CrossRef]
- Gallun, F.J.; Diedesch, A.C.; Kubli, L.R.; Walden, T.C.; Folmer, R.L.; Lewis, M.S.; McDermott, D.J.; Fausti, S.A.; Leek, M.R. Performance on Tests of Central Auditory Processing by Individuals Exposed to High-Intensity Blasts. J. Rehabil. Res. Dev. 2012, 49, 1005–1025. [Google Scholar] [CrossRef]
- Gallun, F.J.; Papesh, M.A.; Lewis, M.S. Hearing Complaints among Veterans Following Traumatic Brain Injury. Brain Inj. 2017, 31, 1183–1187. [Google Scholar] [CrossRef] [PubMed]
- Saunders, G.H.; Frederick, M.T.; Arnold, M.; Silverman, S.; Chisolm, T.H.; Myers, P. Auditory Difficulties in Blast-Exposed Veterans with Clinically Normal Hearing. J. Rehabil. Res. Dev. 2015, 52, 343–360. [Google Scholar] [CrossRef]
- Kraus, N.; Thompson, E.C.; Krizman, J.; Cook, K.; White-Schwoch, T.; LaBella, C.R. Auditory Biological Marker of Concussion in Children. Sci. Rep. 2016, 6, 39009. [Google Scholar] [CrossRef]
- Vander Werff, K.R.; Rieger, B. Impaired Auditory Processing and Neural Representation of Speech in Noise among Symptomatic Post-Concussion Adults. Brain Inj. 2019, 33, 1320–1331. [Google Scholar] [CrossRef] [PubMed]
- Flood, G.M.; Dumas, H.M.; Haley, S.M. Central Auditory Processing and Social Functioning Following Brain Injury in Children. Brain Inj. 2005, 19, 1019–1026. [Google Scholar] [CrossRef]
- Fligor, B.J.; Cox, L.C.; Nesathurai, S. Subjective Hearing Loss and History of Traumatic Brain Injury Exhibits Abnormal Brainstem Auditory Evoked Response: A Case Report. Arch. Phys. Med. Rehabil. 2002, 83, 141–143. [Google Scholar] [CrossRef] [PubMed]
- Mott, F.W. The Microscopic Examination of the Brains of Two Men Dead of Commotio Cerebri (Shell Shock) without Visible External Injury. Br. Med. J. 1917, 2, 612–615. [Google Scholar] [CrossRef][Green Version]
- Franke, L.M.; Perera, R.A.; Aygemang, A.A.; Marquardt, C.A.; Teich, C.; Sponheim, S.R.; Duncan, C.C.; Walker, W.C. Auditory Evoked Brain Potentials as Markers of Chronic Effects of Mild Traumatic Brain Injury in Mid-Life. Clin. Neurophysiol. 2021, 132, 2979–2988. [Google Scholar] [CrossRef]
- Munjal, S.K.; Panda, N.K.; Pathak, A. Relationship between Severity of Traumatic Brain Injury (TBI) and Extent of Auditory Dysfunction. Brain Inj. 2010, 24, 525–532. [Google Scholar] [CrossRef]
- Race, N.; Lai, J.; Shi, R.; Bartlett, E.L. Differences in Postinjury Auditory System Pathophysiology after Mild Blast and Nonblast Acute Acoustic Trauma. J. Neurophysiol. 2017, 118, 782–799. [Google Scholar] [CrossRef]
- Canadian Interorganizational Steering Group for Speech-Language Pathology and Audiology. Canadian Guidelines on Auditory Processing Disorder in Children and Adults: Assessment and Intervention; Canadian Interorganizational Steering Group for Speech-Language Pathology and Audiology: Ottawa, ON, Canada, 2012; pp. 1–83. [Google Scholar]
- Auditec. Tonal and Speech Materials for Auditory Perceptual Assessment: Nu-6, Ordered by Difficulty; Auditec: St. Louis, MO, USA, 2015. [Google Scholar]
- Keith, R.W. ACPT: Auditory Continuous Performance Test; Psychol. Corp: San Antonio, TX, USA, 1994. [Google Scholar]
- Keith, R.W. Auditory Continuous Performance Test Examiners Manual; Psychol. Corp: San Antonio, TX, USA, 1994. [Google Scholar]
- Keith, R.W. Random Gap Detection Test; Auditec: St. Louis, MO, USA, 2000. [Google Scholar]
- Musiek, F.E. Duration Pattern Sequence; Auditec: St. Louis, MO, USA, 2015. [Google Scholar]
- Musiek, F.E. Pitch (Frequency) Pattern Test; Auditec: St. Louis, MO, USA, 2015. [Google Scholar]
- Musiek, F.E. Frequency (Pitch) and Duration Pattern Tests. J. Am. Acad. Audiol. 1994, 5, 265–268. [Google Scholar] [PubMed]
- Auditec. Tonal and Speech Materials for Auditory Perceptual Assessment: Nu-6, 45% Time-Compressed; Auditec: St. Louis, MO, USA, 2015. [Google Scholar]
- Keith, R.W. Standardization of the Time Compressed Sentence Test. J. Educ. Audiol. 2002, 10, 15–20. [Google Scholar]
- Auditec. Tonal and Speech Materials for Auditory Perceptual Assessment: Nu-6, Low Pass FILTERED at 1000 Hz; Auditec: St. Louis, MO, USA, 2015. [Google Scholar]
- Cameron, S.; Dillon, H.; Newall, P. The Listening in Spatialized Noise Test: An Auditory Processing Disorder Study. J. Am. Acad. Audiol. 2006, 17, 306–320. [Google Scholar] [CrossRef]
- Cameron, S.; Brown, D.; Keith, R.; Martin, R.; Watson, C.; Dillon, H. Development of the North American Listening in Spatialized Noise–Sentences Test (NA LiSN-S): Sentence equivalence, normative data, and test-retest reliability studies. J. Am. Acad. Audiol. 2009, 20, 128–146. [Google Scholar] [CrossRef]
- Etymōtic Research. QuickSIN Speech-in-Noise Test, Version 1.3; Etymōtic Research: Elk Grove Village, IL, USA, 2005. [Google Scholar]
- Killion, M.C.; Niquette, P.A.; Gudmundsen, G.I.; Revit, L.J.; Banerjee, S. Development of a Quick Speech-in-Noise Test for Measuring Signal-to-Noise Ratio Loss in Normal-Hearing and Hearing-Impaired Listeners. J. Acoust. Soc. Am. 2004, 116, 2395–2405. [Google Scholar] [CrossRef] [PubMed]
- Bench, J.; Kowal, Å.; Bamford, J. The Bkb (Bamford-Kowal-Bench) Sentence Lists for Partially-Hearing Children. Br. J. Audiol. 1979, 13, 108–112. [Google Scholar] [CrossRef]
- Etymōtic Research. Bamford-Kowal-Bench Speech-in-Noise Test. Version 1.03; Etymōtic Research: Elk Grove Village, IL, USA, 2005. [Google Scholar]
- Willeford, J.; Burleigh, J. Sentence Procedures in Central Testing. Handb. Clin. Audiol. 1994, 4, 256–268. [Google Scholar]
- Willeford, J.; Burleigh, J. Competing Sentences; Auditec: St. Louis, MO, USA, 2015. [Google Scholar]
- Katz, J. Staggered Spondaic Word Test. (SSW); Precision Acoustics, Inc.: Vancouver, WA, USA, 1986. [Google Scholar]
- Katz, J.; Basil, R.A.; Smith, J.M. LXVI A Staggered Spondaic Word Test for Detecting Central Auditory Lesions. Ann. Otol. Rhinol. Laryngol. 1963, 72, 908–917. [Google Scholar] [CrossRef]
- Musiek, F.E. Assessment of Central Auditory Dysfunction: The Dichotic Digit Test Revisited. Ear Hear. 1983, 4, 79–83. [Google Scholar] [CrossRef]
- Musiek, F.E. Dichotic Digits Test; Auditec: St. Louis, MO, USA, 2015. [Google Scholar]
- Estes, B.; Dennison, A.; Schiff, W.; Hertza, J. D-15Misophonia and Attention Disturbance Following Right Orbital Brain Injury. Arch. Clin. Neuropsychol. 2010, 25, 475–583. [Google Scholar]
- Attias, J.; Zwecker-Lazar, I.; Nageris, B.; Keren, O.; Groswasser, Z. Dysfunction of the Auditory Efferent System in Patients with Traumatic Brain Injuries with Tinnitus and Hyperacusis. J. Basic Clin. Physiol. Pharmacol. 2005, 16. [Google Scholar] [CrossRef] [PubMed]
- Monaghan, J.J.M.; Garcia-Lazaro, J.A.; McAlpine, D.; Schaette, R. Hidden Hearing Loss Impacts the Neural Representation of Speech in Background Noise. Curr. Biol. 2020, 30, 4710–4721. [Google Scholar] [CrossRef] [PubMed]
- Kohrman, D.; Wan, G.; Cassinotti, L.; Corfas, G. Hidden Hearing Loss: A Disorder with Multiple Etiologies and Mechanisms. Cold Spring Harb. Perspect. Med. 2020, 10, a035493. [Google Scholar] [CrossRef]
- Bryan, C.J. Multiple Traumatic Brain Injury and Concussive Symptoms among Deployed Military Personnel. Brain Inj. 2013, 27, 1333–1337. [Google Scholar] [CrossRef] [PubMed]
- Bryden, D.W.; Tilghman, J.I.; Hinds, S.R. Blast-Related Traumatic Brain Injury: Current Concepts and Research Considerations. J. Exp. Neurosci. 2019, 13, 1–11. [Google Scholar] [CrossRef]
- Greer, N.; Sayer, N.; Koeller, E.; Velasquez, T.; Wilt, T.J. Outcomes Associated with Blast Versus Nonblast-Related Traumatic Brain Injury in US Military Service Members and Veterans: A Systematic Review. J. Head Trauma Rehabil. 2018, 33, 16–29. [Google Scholar] [CrossRef]
- Belanger, H.G.; Proctor-Weber, Z.; Kretzmer, T.; Kim, M.; French, L.M.; Vanderploeg, R.D. Symptom Complaints Following Reports of Blast Versus Non-Blast Mild TBI: Does Mechanism of Injury Matter? Clin. Neuropsychol. 2011, 25, 702–715. [Google Scholar] [CrossRef]
- Hoffer, M.E.; Balaban, C.; Gottshall, K.; Balough, B.J.; Maddox, M.R.; Penta, J.R. Blast Exposure: Vestibular Consequences and Associated Characteristics. Otol. Neurotol. 2010, 31, 232–236. [Google Scholar] [CrossRef]
- Hoffer, M.E.; Balaban, C. Traumatic Brain Injury and Blast Exposures: Auditory and Vestibular Pathology. In Textbook of Tinnitus; Møller, A.R., Langguth, B., De Ridder, D., Kleinjung, T., Eds.; Springer: New York, NY, USA, 2011; pp. 517–520. [Google Scholar] [CrossRef]
- Gutierrez-Cadavid, J. Imaging of Head Trauma. In Imaging of Head Trauma, in Imaging of the Nervous System; Latchaw, R.E., Kucharczyk, J., Moseley, M.E., Eds.; Elsevier Mosby: Philadelphia, PA, USA, 2005; pp. 869–904. [Google Scholar]

| Several vs. One TBI | Blast vs. Blunt Force TBI | |||||
|---|---|---|---|---|---|---|
| Auditory Dysfunction | OR | CI | p | OR | CI | p |
| Cochlear outer hair cells function | 5.143 | 0.819–32.303 | 0.081 | 8 | 0.12–523.32 | 0.530 |
| Tinnitus | 4.333 | 0.742–25.295 | 0.103 | 3 | 0.4516–19.929 | 0.256 |
| Physical reactions to sounds | 0.389 | 0.0372–4.061 | 0.430 | 0.750 | 0.067–8.382 | 0.815 |
| Misophonia | 0.244 | 0.024–2.489 | 0.234 | 0.600 | 0.056–6.442 | 0.673 |
| Auditory Closure | 0.455 | 0.089–2.318 | 0.343 | 1.333 | 0.196–9.083 | 0.769 |
| Temporal processing | 1.467 | 0.282–7.627 | 0.649 | 2.333 | 0.362–15.054 | 0.373 |
| Auditory Attention | 0.482 | 0.043–5.401 | 0.554 | 1.133 | 0.097–13.441 | 0.921 |
| Binaural Integration | 0.857 | 0.172–4.267 | 0.851 | 1.500 | 0.239–9.383 | 0.664 |
| Binaural Separation | 1.286 | 0.264–6.276 | 0.756 | 1.222 | 0.197–7.595 | 0.829 |
| Speech-in-noise | 5.143 | 0.819–32.302 | 0.081 | 5.000 | 0.492–50.833 | 0.174 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
White, M.; Duquette-Laplante, F.; Jutras, B.; Bursch, C.; Koravand, A. A Retrospective Study of the Effects of Traumatic Brain Injury on Auditory Function: From a Clinical Perspective. NeuroSci 2022, 3, 52-62. https://doi.org/10.3390/neurosci3010004
White M, Duquette-Laplante F, Jutras B, Bursch C, Koravand A. A Retrospective Study of the Effects of Traumatic Brain Injury on Auditory Function: From a Clinical Perspective. NeuroSci. 2022; 3(1):52-62. https://doi.org/10.3390/neurosci3010004
Chicago/Turabian StyleWhite, Mira, Fauve Duquette-Laplante, Benoît Jutras, Caryn Bursch, and Amineh Koravand. 2022. "A Retrospective Study of the Effects of Traumatic Brain Injury on Auditory Function: From a Clinical Perspective" NeuroSci 3, no. 1: 52-62. https://doi.org/10.3390/neurosci3010004
APA StyleWhite, M., Duquette-Laplante, F., Jutras, B., Bursch, C., & Koravand, A. (2022). A Retrospective Study of the Effects of Traumatic Brain Injury on Auditory Function: From a Clinical Perspective. NeuroSci, 3(1), 52-62. https://doi.org/10.3390/neurosci3010004