
Epidemiological Monitoring of COVID-19 in a Brazilian City: The Interface between the Economic Policies, Commercial Behavior, and Pandemic Control



Abstract
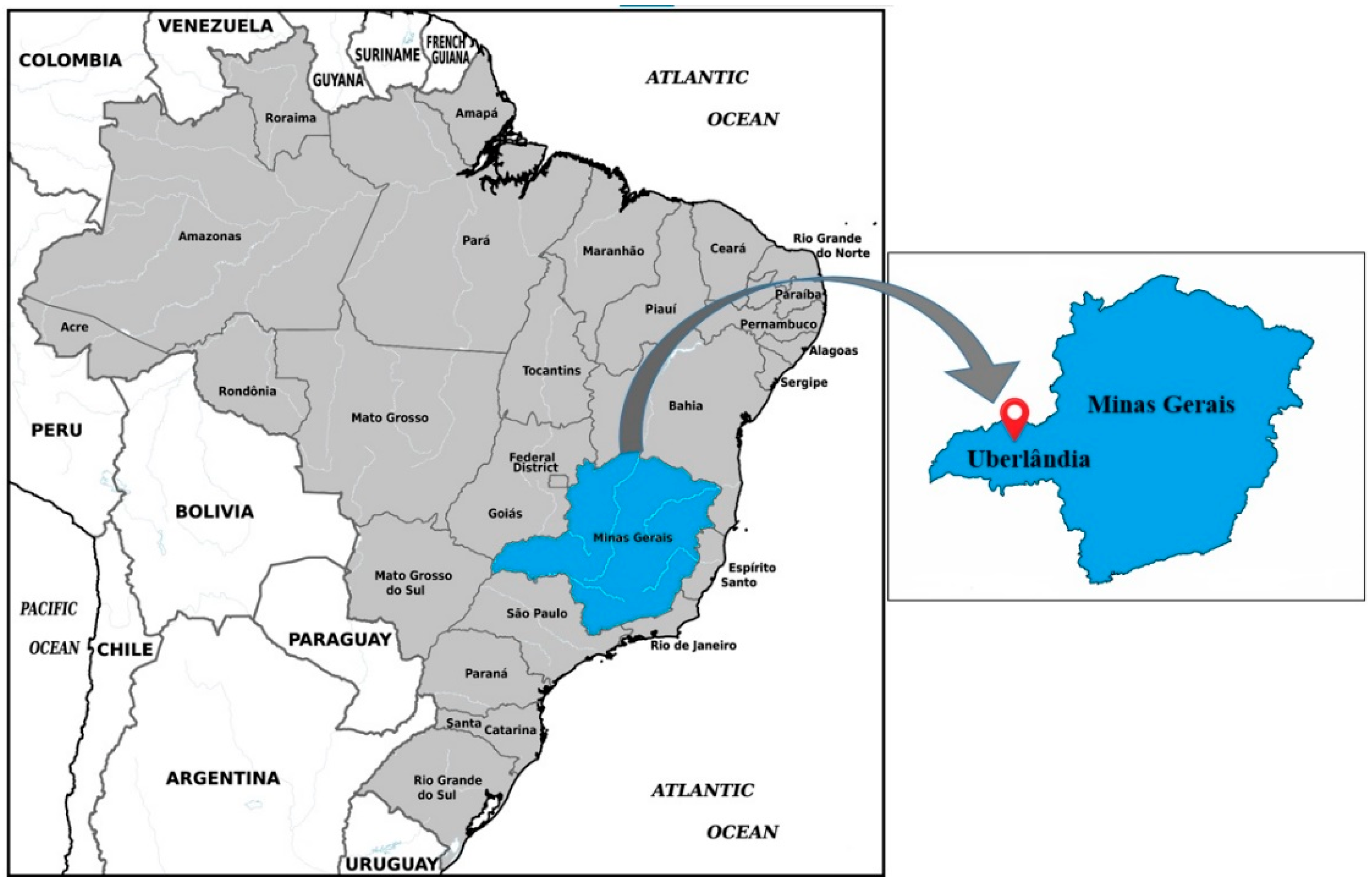
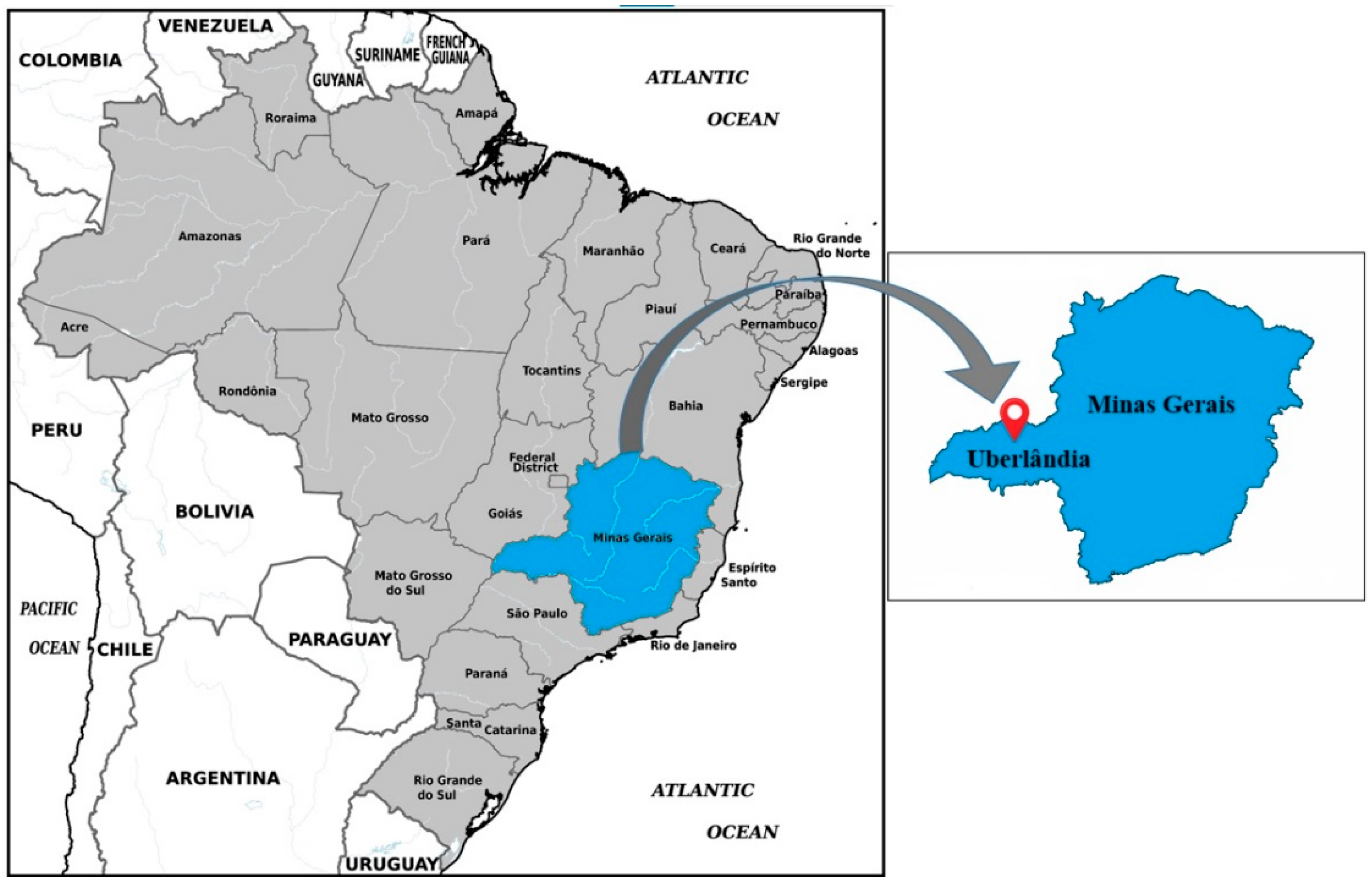
:1. Introduction
2. Materials and Methods
- Rigid: Agriculture, livestock, and related areas services; manufacturing of food and beverage products; food services; financial services (banking and insurance); production chain and essential accessory activities; construction; factories; energy; steel industry; health; communication and press; transport; vehicles; post offices; water and sewage treatment; hotels; legal activities; higher education and public transport.
- Intermediate: Activities of the rigid phase; recreation and leisure activities; rent; curricular and extracurricular teaching; activities related to cultural and environmental heritage; travel agency; sports activities and social clubs; publicity; professional, scientific, and technical activities; sales representatives; photographic activities; beauty and aesthetic salons; jewelry and costume jewelry; driver training; duty-free stores; design and decoration; books and stationery; agricultural products; sporting goods, electronic games, weapons, and fireworks; antiques; department and varieties; other ancillary activities.
- Flexible: Activities of the rigid and intermediate phases; events; recreation and leisure activities; movie theaters; other personal service activities.
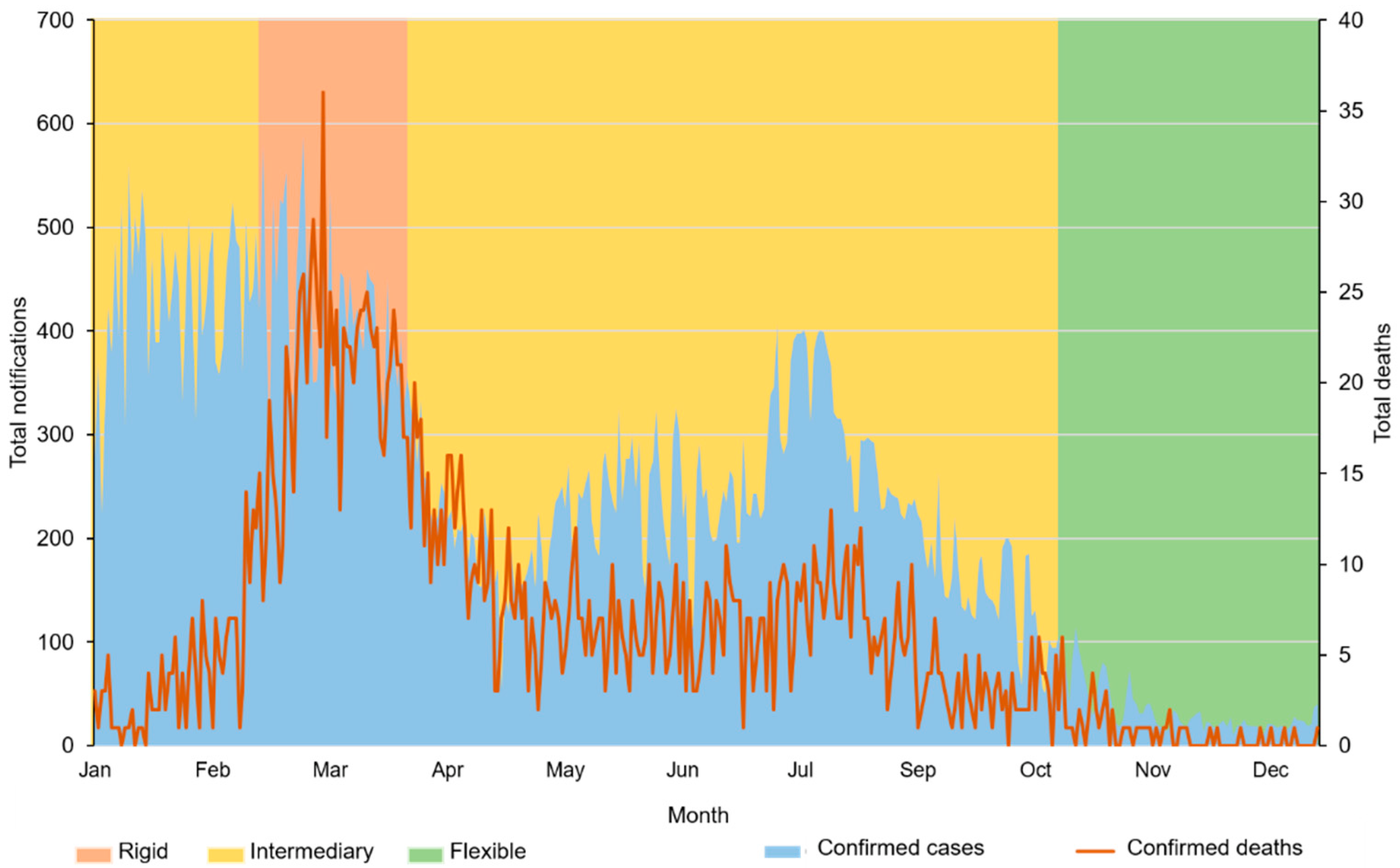
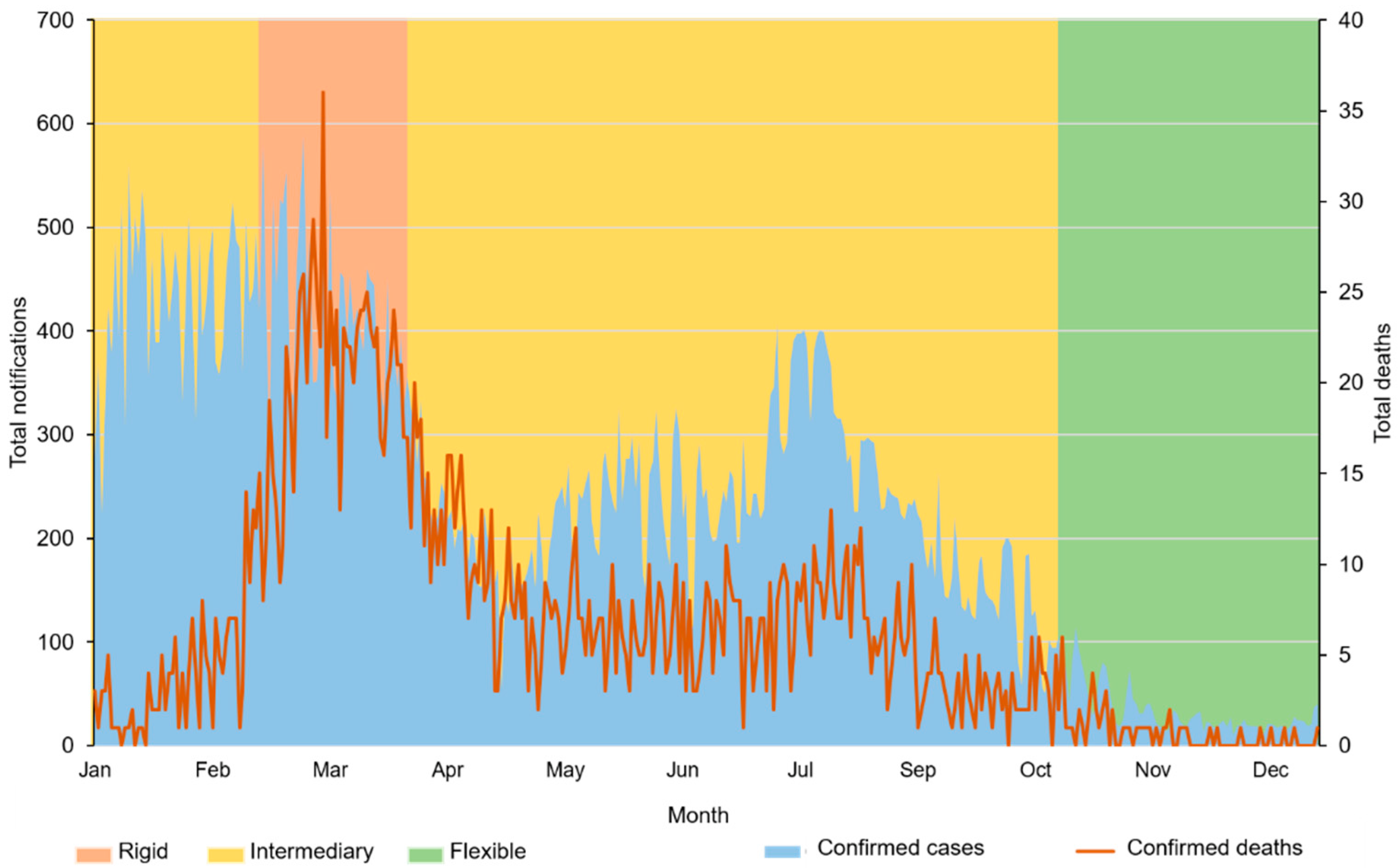
3. Results
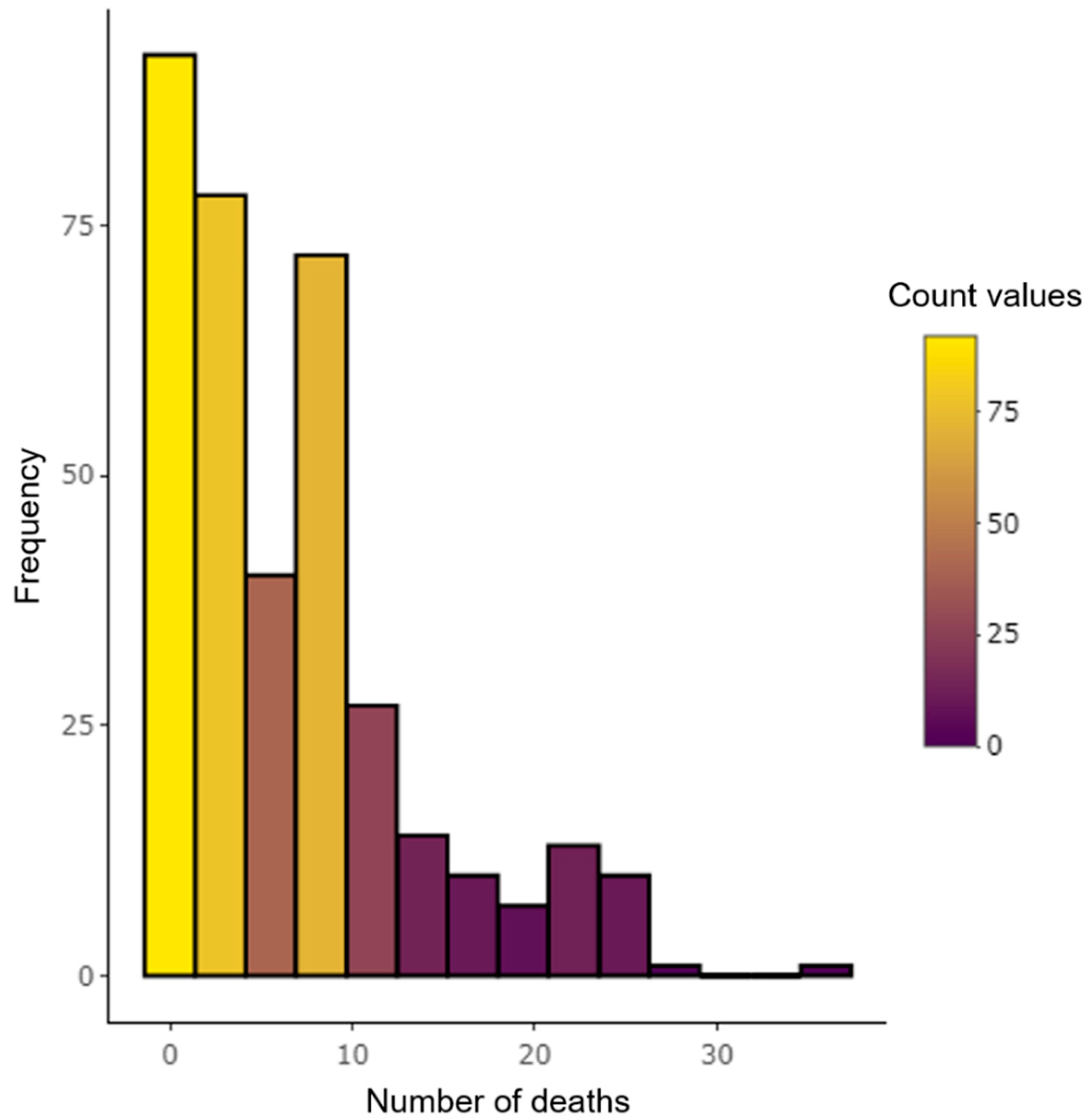
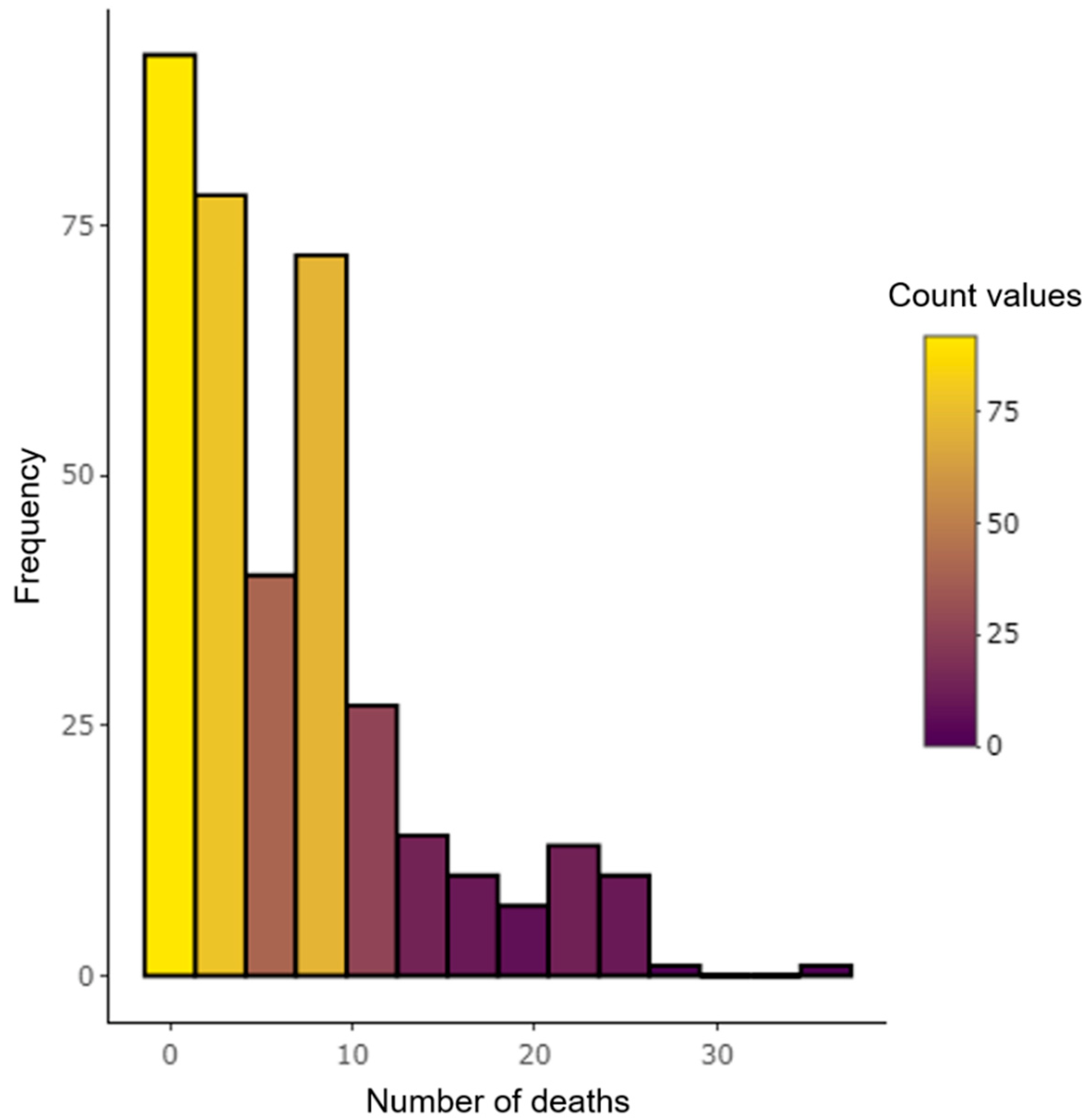
3.1. Behavior of Cases and Deaths
3.2. Profile of Hospitalized Individuals
3.3. Selecting The Regression Model for Multivariate Analysis of Deaths
3.4. Applying the Poisson Model
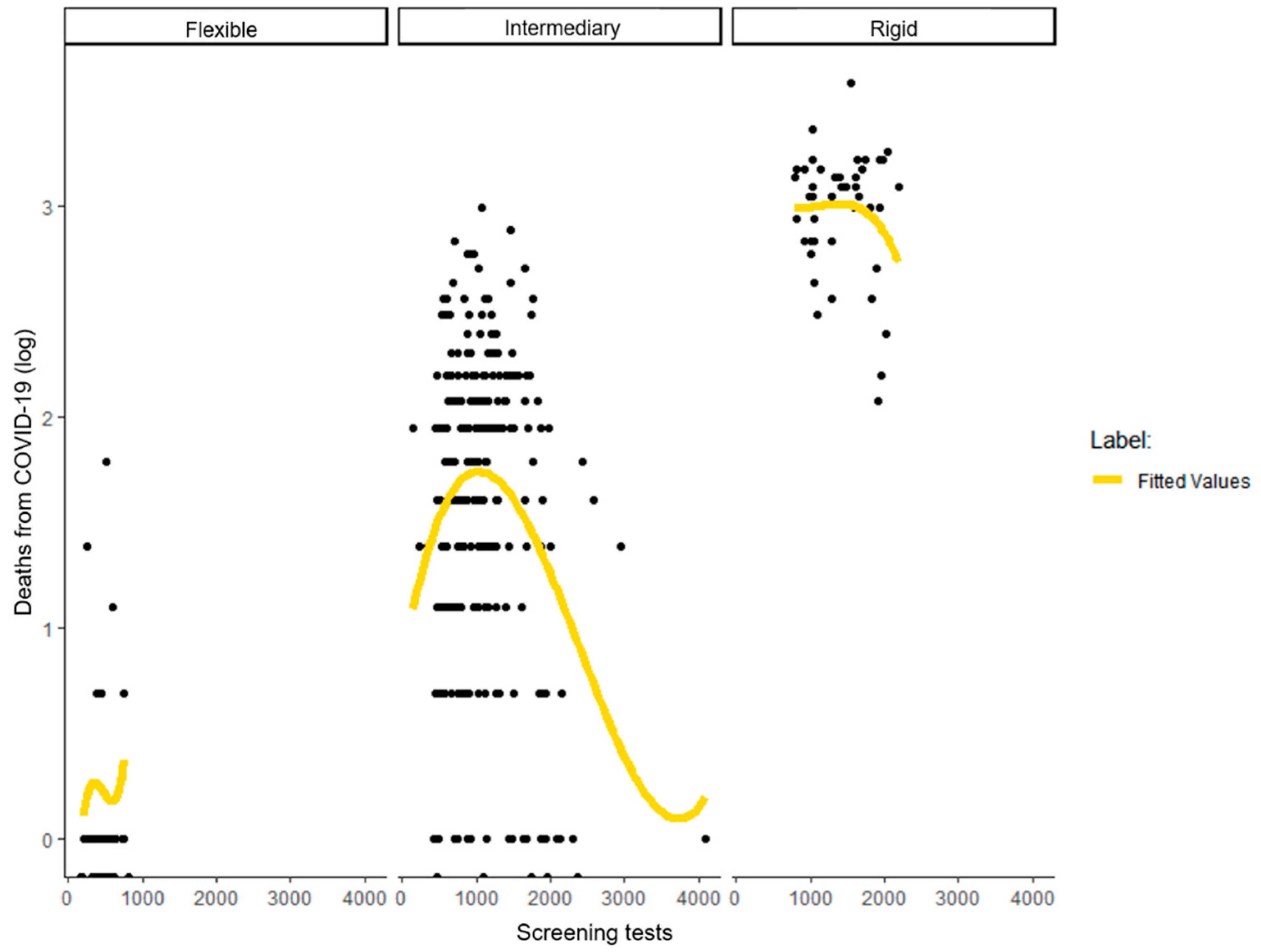
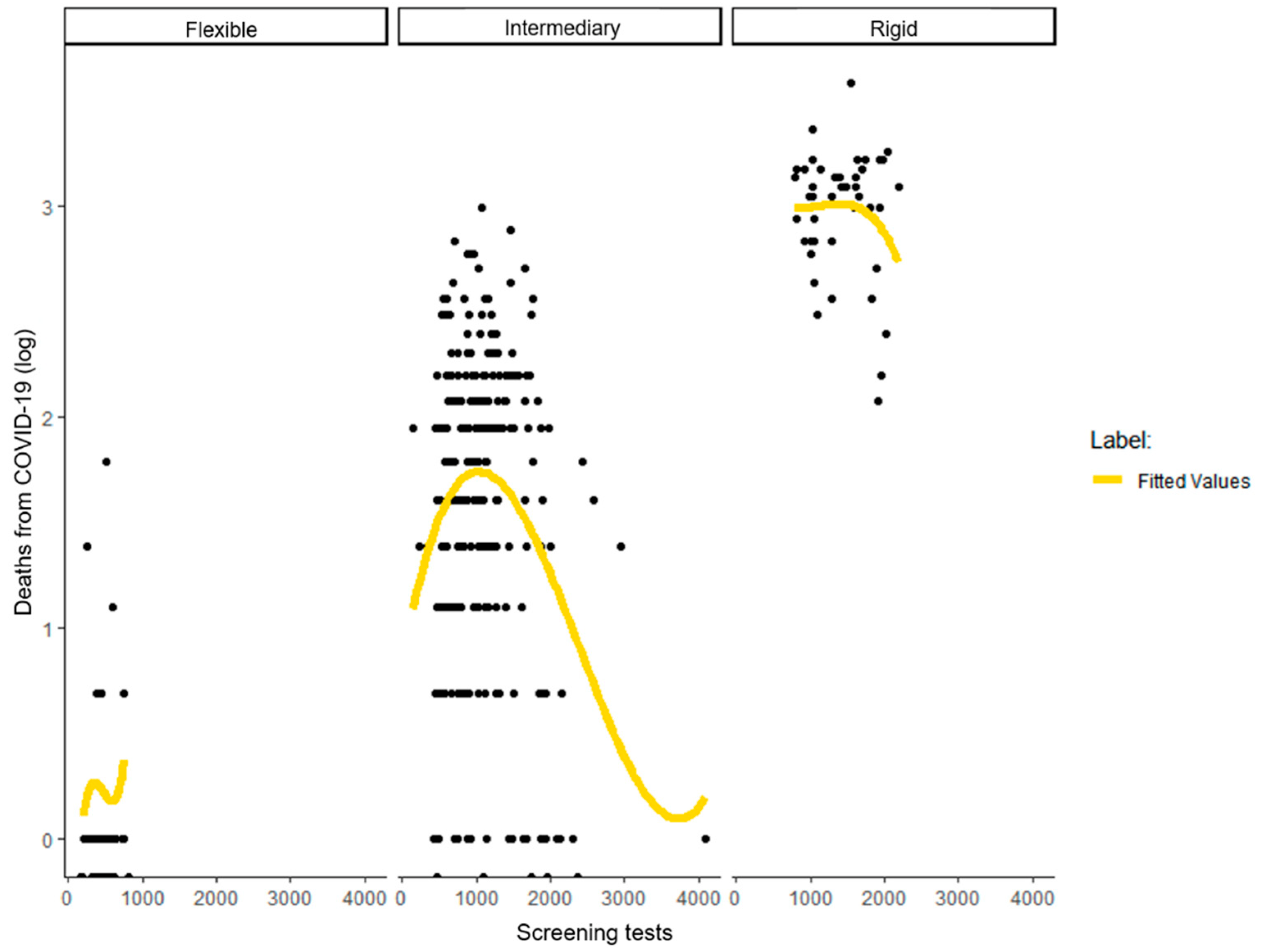
3.5. Applying Univariate Regressions to Correlate Screening Tests and Deaths
4. Discussion
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Umakanthan, S.; Sahu, P.; Ranade, A.V.; Bukelo, M.M.; Rao, J.S.; Abrahao-Machado, L.F.; Dhananjaya, K.V. Origin, transmission, diagnosis and management of coronavirus disease 2019 (COVID-19). Postgrad. Med. J. 2020, 96, 753–758. [Google Scholar] [PubMed]
- de Brito, V.P.; Carrijo, A.M.M.; de Oliveira, S.V. Association of Diabetes Mellitus with COVID-19 severity and its potential mediating factors: A systematic review. Rev. Thema 2020, 18, 204–217. [Google Scholar]
- Prada, L.; Ferreira, J. COVID-19, diabetes and vaccines. Rev. Port. Diabetes 2020, 15, 131–138. [Google Scholar]
- Pires, L.N.; Carvalho, L.; Xavier, L.D.L. COVID-19 and inequality: The distribution of risk factors in Brazil. Exp. Find. 2020, 21, 1–4. [Google Scholar]
- Werneck, G.L.; Carvalho, M.S. The pandemic of COVID-19 in Brazil: Chronic of a health crisis foretold. Cad. Saúde Pública 2020, 36, e00068820. [Google Scholar] [CrossRef] [PubMed]
- Freitas, A.R.R.; Napimoga, M.; Donalisio, M.R. Assessing the severity of COVID-19. Epidemiol. Serv. Saúde 2020, 29, e2020119. [Google Scholar] [PubMed] [Green Version]
- Minas Gerais Secretary of Health. Coronavirus Epidemiological Bulletin. Available online: https://coronavirus.saude.mg.gov.br/boletim (accessed on 12 March 2022).
- Rosa, M.F.P.; da Silva, W.N.T.; de Carvalho, W.R.G.; de Oliveira, S.V. Epidemiology of COVID-19 in Uberlândia (MG): Preliminary Analysis of the Impact of Commercial Activities’s Openness. J. Health NPEPS 2020, 5. Available online: https://periodicos.unemat.br/index.php/jhnpeps/article/view/4844 (accessed on 12 March 2022).
- Aquino, E.M.; Silveira, I.H.; Pescarini, J.M.; Aquino, R.; Souza-Filho, J.A.D.; Rocha, A.D.S.; Lima, R.T.D.R.S. Social distancing measures in the control of the pandemic of COVID-19: Potential impacts and challenges in Brazil. Ciênc. Saúde Colet. 2020, 25, 2423–2446. [Google Scholar] [CrossRef]
- Domingues, C.M.A.S. Challenges for implementation of the COVID-19 vaccination campaign in Brazil. Cad. Saúde Pública 2021, 37, 1–5. [Google Scholar]
- Lima, E.J.D.F.; Almeida, A.M.; de Ávila Kfouri, R. Vaccines for COVID-19-the state of the art. Ver. Bras. Saúde Mater. Infant. 2021, 21, 13–19. [Google Scholar] [CrossRef]
- Uberlândia City Hall. Confronting Coronavirus: Decrees and Documents. Available online: https://www.uberlandia.mg.gov.br/prefeitura/secretarias/saude/coronavirus/decretos-e-documentos/ (accessed on 30 March 2022).
- Brazilian Institute of Geography and Statistics. Panorama of Cities and States. Available online: https://cidades.ibge.gov.br/brasil/mg/uberlandia/panorama (accessed on 13 March 2022).
- Brazilian Institute of Geography and Statistics. Panorama of Cities and States. Available online: https://cidades.ibge.gov.br/brasil/mg/panorama (accessed on 15 March 2022).
- Cameron, A.C.; Trivedi, P.K. Regression-based tests for overdispersion in the Poisson model. J. Econom. 1990, 46, 347–364. [Google Scholar] [CrossRef]
- Fávero, L.P.; Belfiore, P. Handbook of Data Analysis: Statistics and Multivariate Modeling with Excel®, SPSS® and Stata®, 1st ed.; Elsevier: Amsterdam, The Netherlands, 2017; ISBN 978-853-528-505-5. [Google Scholar]
- Ministry of Health. Resolution No. 510, Dated 7 April 2016, Which Provides on the Standards Applicable to Research in Human and Social Sciences. Available online: http://conselho.saude.gov.br/resolucoes/2016/Reso510.pdf (accessed on 13 March 2022).
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 13 March 2022).
- Uberlândia City Hall. Decree No. 18,523 of 27 February 2020 Establishing the COVID-19 Committee. Available online: http://docs.uberlandia.mg.gov.br/wp-content/uploads/2020/02/5817.pdf#page=02 (accessed on 29 March 2022).
- Uberlândia City Hall. Municipal Plan for the Operation of Economic Activities. Available online: https://www.uberlandia.mg.gov.br/prefeitura/secretarias/saude/coronavirus/plano-municipal-de-funcionamento-das-atividades-economicas (accessed on 12 March 2022).
- Uberlândia City Hall. Municipal Bulletin: Epidemiological Report. Available online: https://www.uberlandia.mg.gov.br/prefeitura/secretarias/saude/coronavirus/boletim-municipal-informe-epidemiologico/ (accessed on 1 April 2022).
- Ministry of Health. Coronavirus Panel. Available online: https://covid.saude.gov.br/ (accessed on 29 May 2022).
- Campos, I.S.; Aratani, V.F.; Cabral, K.B.; Limongi, J.E.; Oliveira, S.V.D. A vulnerability analysis for the management of and response to the COVID-19 epidemic in the second most populous state in Brazil. Front. Public Health 2021, 9, 331. [Google Scholar] [CrossRef] [PubMed]
- da Silva-Júnior, M.J.; Mendonça, K.S.; de Lima, C.A.; Pires, P.L.; Calegari, T.; de Oliveira, S.V. Analysis of the spatial-temporal dynamics of incidence, mortality and test rates (rapid and RT-PCR) of COVID-19 in the state of Minas Gerais, Brazil. SciELO 2020. preprints. [Google Scholar]
- Jonh Hopkins University and Medicine. COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU). Available online: https://coronavirus.jhu.edu/map.html (accessed on 29 May 2022).
- Xu, S.; Li, Y. Beware of the second wave of COVID-19. Lancet 2020, 395, 1321–1322. [Google Scholar] [CrossRef]
- Thomson, E.C.; Rosen, L.E.; Shepherd, J.G.; Spreafico, R.; da Silva Filipe, A.; Wojcechowskyj, J.A.; ISARIC4C Investigators. Circulating SARS-CoV-2 spike N439K variants maintain fitness while evading antibody-mediated immunity. Cell 2021, 184, 1171–1187.e20. [Google Scholar] [CrossRef] [PubMed]
- Pereira, G.; Wütrich, F. Local Actions to Address the COVID-19 Pandemic in South America. Oculum Ens. 2021, 18. [Google Scholar] [CrossRef]
- Hodgson, S.H.; Mansatta, K.; Mallett, G.; Harris, V.; Emary, K.R.; Pollard, A.J. What defines an efficacious COVID-19 vaccine? A review of the challenges assessing the clinical efficacy of vaccines against SARS-CoV-2. Lancet Infect. Dis. 2021, 21, 26–35. [Google Scholar] [CrossRef]
- Minas Gerais Secretary of Health. Vacinometer: Belo Horizonte. Available online: https://coronavirus.saude.mg.gov.br/vacinometro (accessed on 29 March 2022).
- Ministry of Health. National Operationalization Plan for Vaccination against COVID-19. Available online: https://www.gov.br/saude/pt-br/composicao/secovid/pno_edicoes/1a-edicao-pno-16-12-2020.pdf/view (accessed on 30 March 2022).
- Michelon, C.M. Main variants of SARS-CoV-2 reported in Brazil. Rev. Bras. Anal. Clin. 2021, 53, 109–116. [Google Scholar]
- Da Silva, M.L.; Da Silva, R.A. Brazilian economy pre, during and post-pandemic COVID-19: Impacts and reflections. In COVID-19 Socieconomic Observatory; Federal University of Santa Maria: Santa Maria, Brazil, 2020; pp. 1–11. [Google Scholar]
- Gebhard, C.; Regitz-Zagrosek, V.; Neuhauser, H.K.; Morgan, R.; Klein, S.L. Impact of sex and gender on COVID-19 outcomes in Europe. Biol. Sex Differ. 2021, 76, 428–455. [Google Scholar] [CrossRef]
- Mukherjee, S.; Pahan, K. Is COVID-19 gender-sensitive? J. Neuroimmune Pharmacol. 2021, 16, 38–47. [Google Scholar] [CrossRef]
- Gallo Marin, B.; Aghagoli, G.; Lavine, K.; Yang, L.; Siff, E.J.; Chiang, S.S.; Michelow, I.C. Predictors of COVID-19 severity: A literature review. Rev. Med. Virol. 2021, 31, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.D.; Ding, M.; Dong, X.; Zhang, J.J.; Kursat Azkur, A.; Azkur, D.; Akdis, C.A. Risk factors for severe and critically ill COVID-19 patients: A review. Allergy 2021, 76, 428–455. [Google Scholar] [CrossRef] [PubMed]
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, transmission, diagnosis, and treatment of coronavirus disease 2019 (COVID-19): A review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef]
- Rello, J.; Belliato, M.; Dimopoulos, M.A.; Giamarellos-Bourboulis, E.J.; Jaksic, V.; Martin-Loeches, I.; Dimopoulos, G. Update in COVID-19 in the intensive care unit from the 2020 HELLENIC Athens International symposium. Anaesth. Crit. Care Pain Med. 2020, 39, 723–730. [Google Scholar] [CrossRef] [PubMed]
- McCullough, P.A.; Kelly, R.J.; Ruocco, G.; Lerma, E.; Tumlin, J.; Wheelan, K.R.; Risch, H.A. Pathophysiological basis and rationale for early outpatient treatment of SARS-CoV-2 (COVID-19) infection. Am. J. Med. 2021, 134, 16–22. [Google Scholar] [CrossRef]
- Silva, L.F.D.; Cursino, E.G.; Brandão, E.D.S.; Góes, F.G.B.; Depianti, J.R.B.; Silva, L.J.D.; Aguiar, R.C.B.D. The path from suspicion to diagnosis of people with COVID-19. Rev. Gaúcha Enferm. 2021, 42, e20200282. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Specification | Total | Daily Average | CI (95%) |
|---|---|---|---|---|
| Confirmed cases | - | 86,585 | 237.22 | ±15.49 |
| Confirmed deaths | - | 2450 | 6.71 | ±0.68 |
| Hospitalizations | ICU | 52,997 | 145.20 | ±9.51 |
| Nursery | 65,963 | 180.72 | ±13.57 | |
| Tests | - | 365,512 | 1001.40 | ±53.84 |
| Sex | Male | 68,518 | 187.72 | ±12.74 |
| Female | 50,500 | 138.36 | ±10.30 | |
| Age | 0–5 | 1886 | 5.17 | ±0.41 |
| 6–12 | 497 | 1.36 | ±0.13 | |
| 13–39 | 17,200 | 47.12 | ±3.36 | |
| 40–59 | 46,106 | 126.32 | ±9.29 | |
| 60–69 | 24,440 | 66.96 | ±5.83 | |
| 70–79 | 17,392 | 47.65 | ±3.37 | |
| 80+ | 11,526 | 31.58 | ±2.18 | |
| Phases of the municipal plan | Flexible | 77 * | - | - |
| Intermediary | 244 * | - | - | |
| Rigid | 44 * | - | - |
| Models | Degrees of Freedom | LogLik | Chi-Square | p-Value |
|---|---|---|---|---|
| Poisson | 16 | −750.43 | ||
| Negative binomial | 17 | −750.44 | 0.0098 | 0.9212 |
| Parameter | State | Coefficient |
|---|---|---|
| Intercept | - | −0.5421 *** |
| (0.1403) | ||
| Phases of the municipal plan | Intermediary | 1.1016 *** |
| (0.1735) | ||
| Rigid | 0.9978 *** | |
| (0.2308) | ||
| Confirmed cases | - | 0.0001 |
| Type of hospitalization | (0.0004) | |
| ICU | −0.0133 | |
| (0.0075) | ||
| Nursery | −0.0149 * | |
| (0.0076) | ||
| Screening tests performed | - | −0.0001 ** |
| (0.0000) | ||
| Sex | Male | 0.0119 |
| (0.0064) | ||
| Female | 0.0092 | |
| (0.0066) | ||
| Age | 0–5 | −0.0020 |
| (0.0084) | ||
| 6–12 | 0.0110 | |
| (0.0169) | ||
| 13–39 | 0.0138 ** | |
| (0.0053) | ||
| 40–59 | 0.0032 | |
| (0.0040) | ||
| 60–69 | 0.0103 * | |
| (0.0046) | ||
| 70–79 | 0.0080 | |
| (0.0043) | ||
| 80 or more | 0.0034 | |
| (0.0051) | ||
| Indicators | Values | |
| N | 365 | |
| AIC | 1532.8649 | |
| BIC | 1595.2633 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Brito, V.P.; Carrijo, A.M.M.; Martins, M.V.T.; de Oliveira, S.V. Epidemiological Monitoring of COVID-19 in a Brazilian City: The Interface between the Economic Policies, Commercial Behavior, and Pandemic Control. World 2022, 3, 344-356. https://doi.org/10.3390/world3020019
de Brito VP, Carrijo AMM, Martins MVT, de Oliveira SV. Epidemiological Monitoring of COVID-19 in a Brazilian City: The Interface between the Economic Policies, Commercial Behavior, and Pandemic Control. World. 2022; 3(2):344-356. https://doi.org/10.3390/world3020019
Chicago/Turabian Stylede Brito, Veronica Perius, Alice Mirane Malta Carrijo, Marcos Vinicius Teixeira Martins, and Stefan Vilges de Oliveira. 2022. "Epidemiological Monitoring of COVID-19 in a Brazilian City: The Interface between the Economic Policies, Commercial Behavior, and Pandemic Control" World 3, no. 2: 344-356. https://doi.org/10.3390/world3020019
APA Stylede Brito, V. P., Carrijo, A. M. M., Martins, M. V. T., & de Oliveira, S. V. (2022). Epidemiological Monitoring of COVID-19 in a Brazilian City: The Interface between the Economic Policies, Commercial Behavior, and Pandemic Control. World, 3(2), 344-356. https://doi.org/10.3390/world3020019