
Normative Values for Femoral Length, Tibial Length, and the Femorotibial Ratio in Adults Using Standing Full-Length Radiography


Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Radiographic Protocol
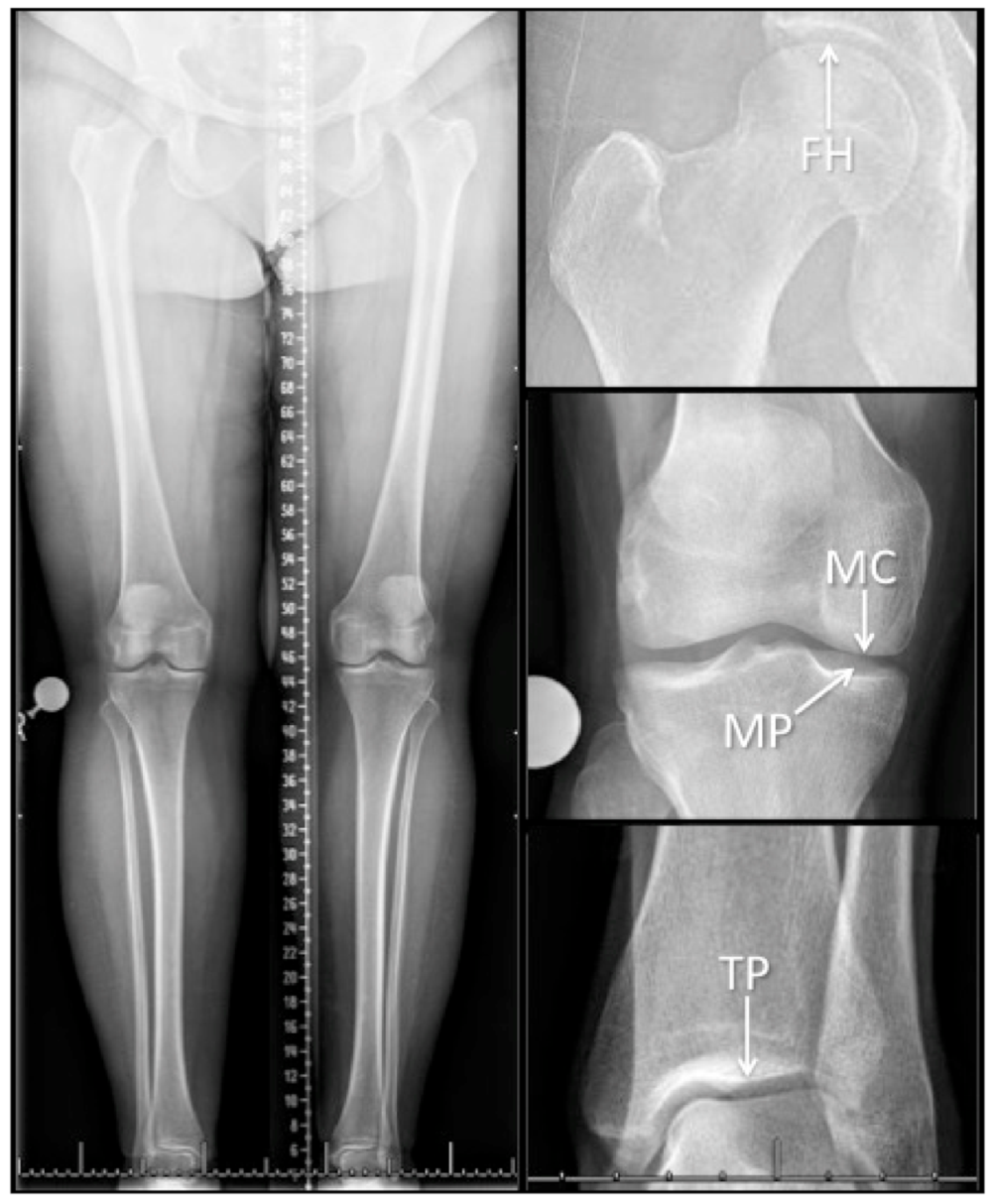
2.3. Limb Measurement
2.4. Statistical Analysis
3. Results
3.1. Measurement Method Reliability
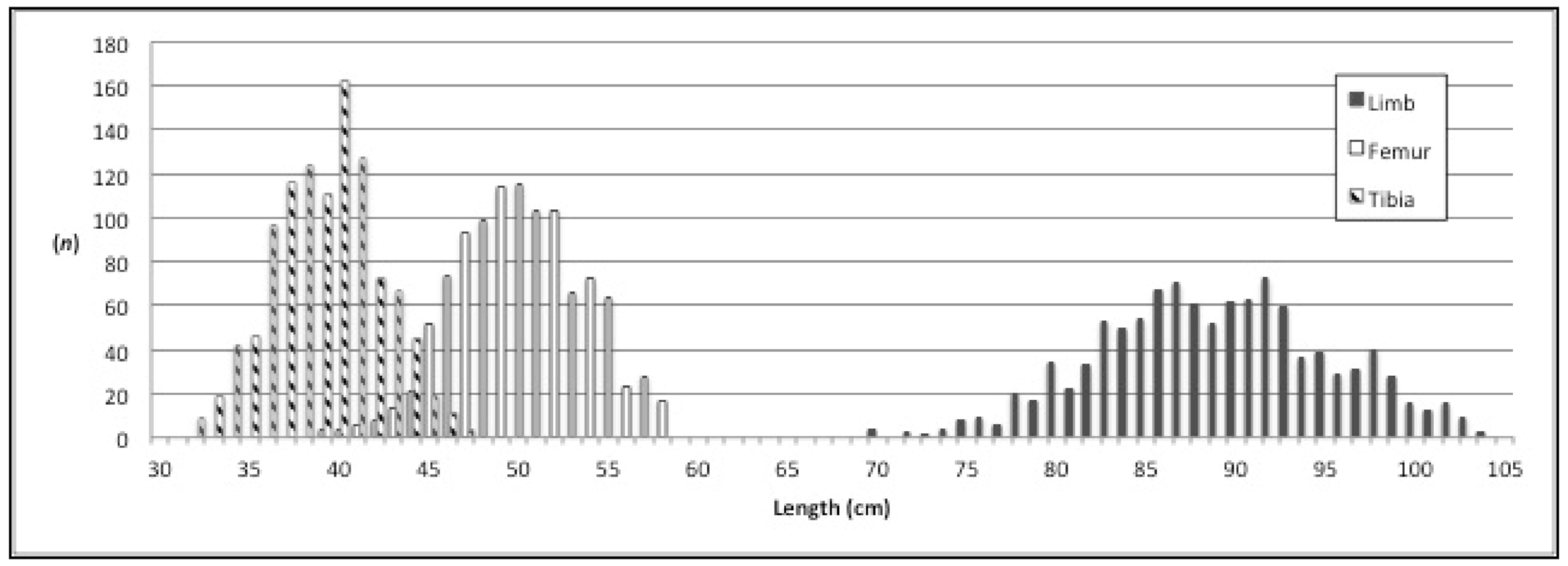
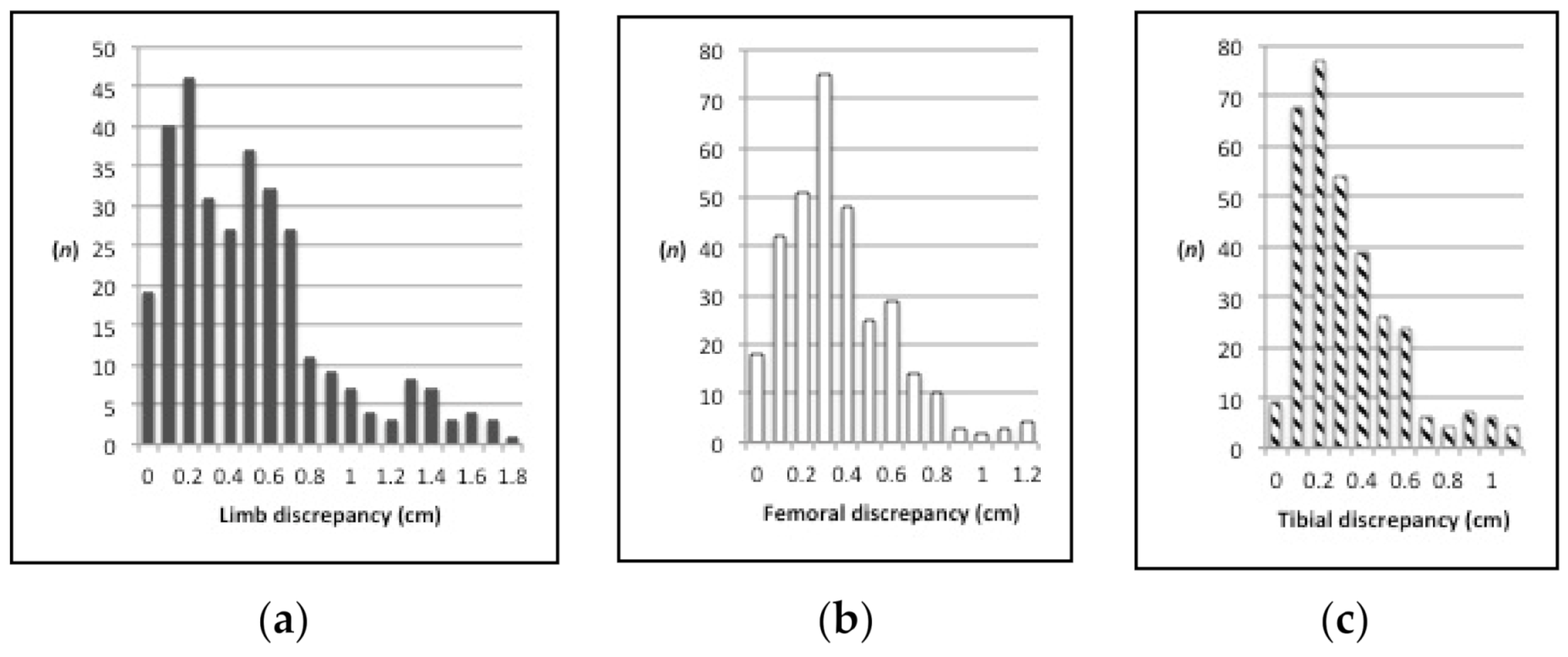
3.2. Limb Length
3.3. Femoral Length
3.4. Tibial Length
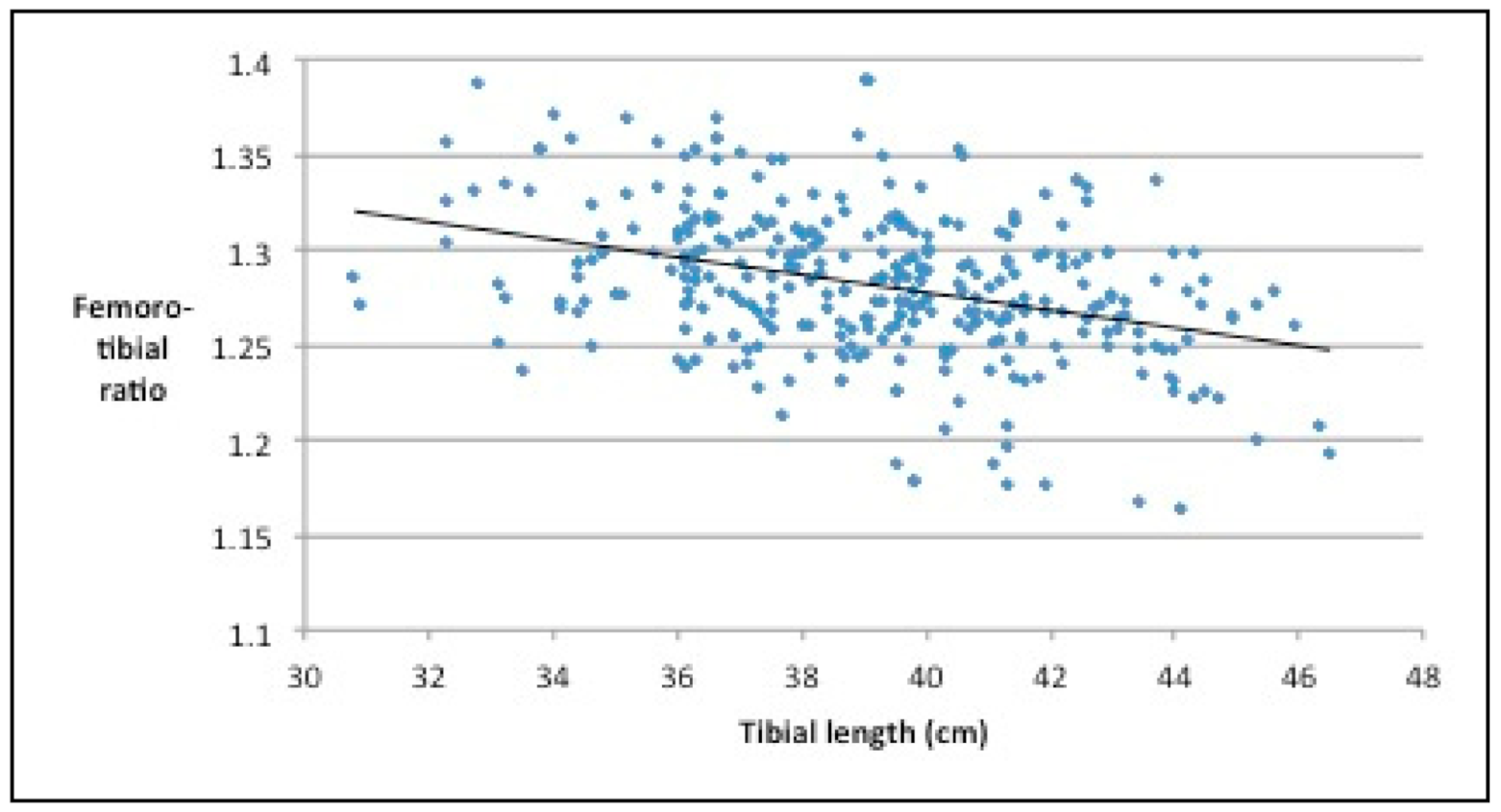
3.5. Femorotibial Ratio
4. Discussion
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Strecker, W.; Keppler, P.; Gebhard, F.; Kinzl, L. Length and torsion of the lower limb. J. Bone Jt. Surg. Br. 1997, 79, 1019–1023. [Google Scholar] [CrossRef]
- Guggenberger, R.; Pfirrmann, C.W.; Koch, P.P.; Buck, F.M. Assessment of lower limb length and alignment by biplanar linear radiography: Comparison with supine CT and upright full-length radiography. Am. J. Roentgenol. 2014, 202, W161–W167. [Google Scholar] [CrossRef] [PubMed]
- Kellgren, J.H.; Lawrence, J.S. Radiological assessment of osteo-arthrosis. Ann. Rheum. Dis. 1957, 16, 494–502. [Google Scholar] [CrossRef] [PubMed]
- Sabharwal, S.; Zhao, C.; McKeon, J.; Melaghari, T.; Blacksin, M.; Wenekor, C. Reliability analysis for radiographic measurement of limb length discrepancy: Full-length standing anteroposterior radiograph versus scanogram. J. Pediatric Orthop. 2007, 27, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Cicchetti, D.V. Guidelines, criteria, and rules of thumb for evaluating normed and standardized assessment instruments in psychology. Psychol. Assess. 1994, 6, 284–290. [Google Scholar] [CrossRef]
- Herscovici, D., Jr.; Scaduto, J.M. Assessing leg length after fixation of comminuted femur fractures. Clin. Orthop. Relat. Res. 2014, 472, 2745–2750. [Google Scholar] [CrossRef] [PubMed]
- Vaidya, R.; Anderson, B.; Elbanna, A.; Colen, R.; Hoard, D.; Sethi, A. CT scanogram for limb length discrepancy in comminuted femoral shaft fractures following IM nailing. Injury 2012, 43, 1176–1181. [Google Scholar] [CrossRef] [PubMed]
- Ng, V.Y.; Kean, J.R.; Glassman, A.H. Limb-length discrepancy after hip arthroplasty. J. Bone Jt. Surg. Am. Vol. 2013, 95, 1426–1436. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, S.; Kernohan, G.; Fitzpatrick, C.; Hill, J.; Beverland, D. Perception of imposed leg length inequality in normal subjects. Hip. Int. 2010, 20, 505–511. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Men (n = 459) | Women (n = 294) | |
|---|---|---|
| Age group (n, %) | ||
| 15–29 years | 61 (13) | 44 (15) |
| 30–49 years | 153 (33) | 77 (26) |
| 50–69 years | 163 (36) | 99 (34) |
| 70+ years | 82 (18) | 74 (25) |
| Both limbs | 183 (40) | 141 (48) |
| measured (n, %) | ||
| Excluded limbs (n, %) | ||
| Open physes | 9 (3) | 3 (2) |
| Congenital/tumor | 2 (1) | 2 (1) |
| Previous fracture | 31 (11) | 15 (10) |
| Knee arthritis | 234 (85) | 133 (87) |
| Total | 276 (100) | 153 (100) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aitken, S.A. Normative Values for Femoral Length, Tibial Length, and the Femorotibial Ratio in Adults Using Standing Full-Length Radiography. Osteology 2021, 1, 86-91. https://doi.org/10.3390/osteology1020009
Aitken SA. Normative Values for Femoral Length, Tibial Length, and the Femorotibial Ratio in Adults Using Standing Full-Length Radiography. Osteology. 2021; 1(2):86-91. https://doi.org/10.3390/osteology1020009
Chicago/Turabian StyleAitken, Stuart A. 2021. "Normative Values for Femoral Length, Tibial Length, and the Femorotibial Ratio in Adults Using Standing Full-Length Radiography" Osteology 1, no. 2: 86-91. https://doi.org/10.3390/osteology1020009
APA StyleAitken, S. A. (2021). Normative Values for Femoral Length, Tibial Length, and the Femorotibial Ratio in Adults Using Standing Full-Length Radiography. Osteology, 1(2), 86-91. https://doi.org/10.3390/osteology1020009