
Assessment of the National Test Strategy on the Development of the COVID-19 Pandemic in Denmark



Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Testing Stages
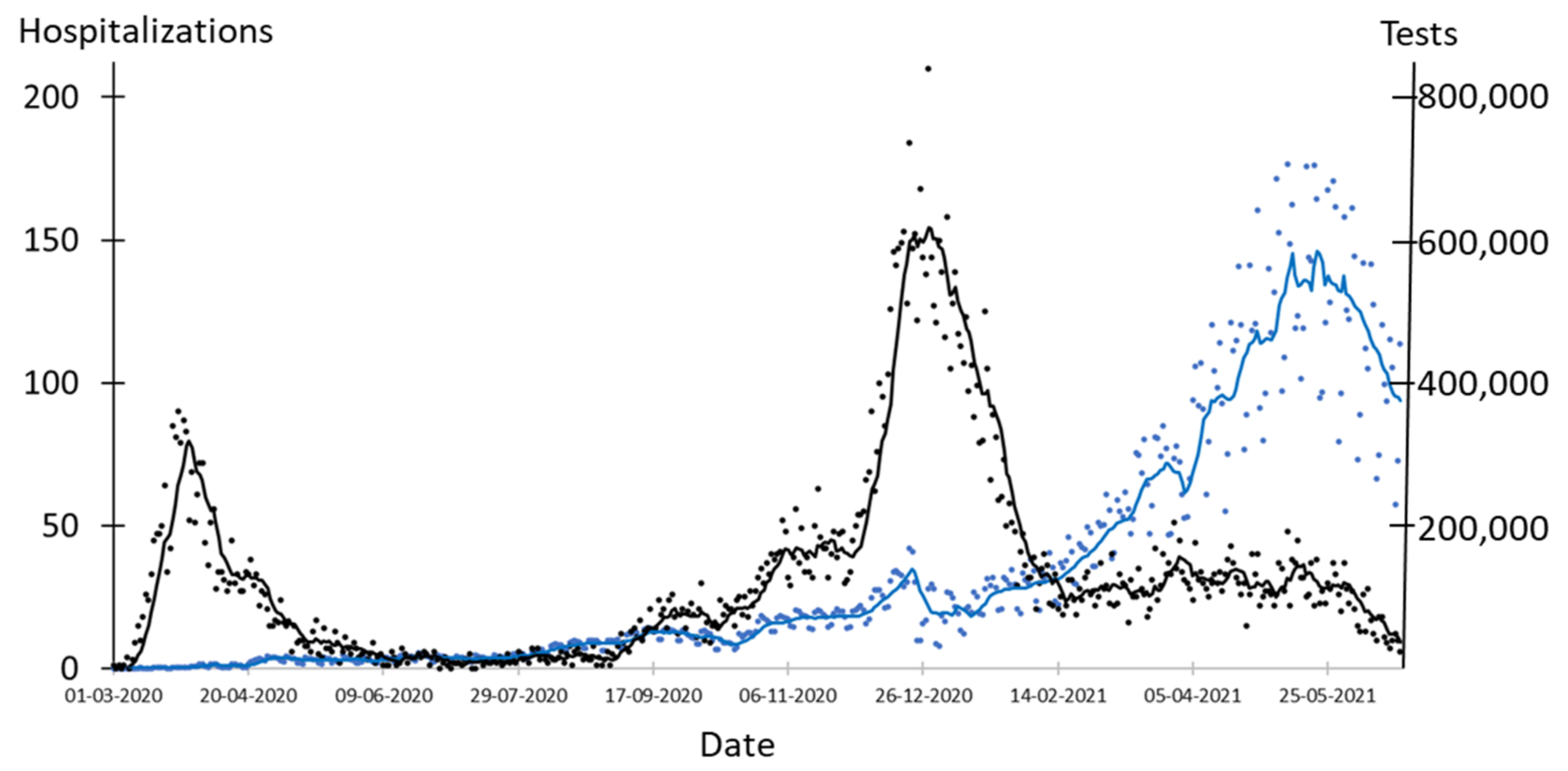
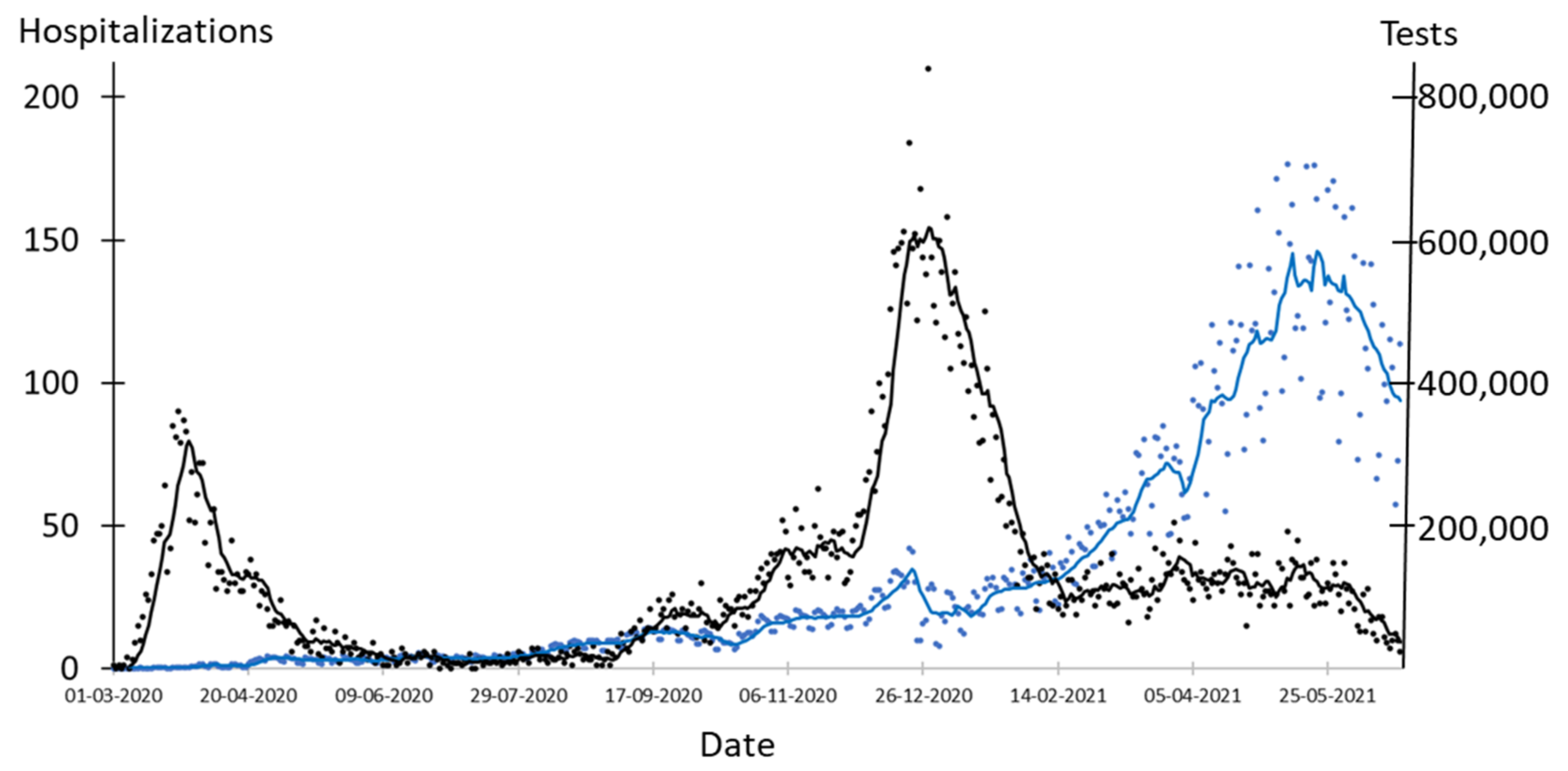
- Stage 1 (27 May 2020 to 6 December 2020): Danish society was open with relatively few changes in restrictions, although compulsory facemasks in public transport were introduced on 22 August and in all indoor facilities with public assess on 29 October [17,18]. During this stage, testing increased from 14,781 tests per day to 69,215 tests per day. Self-reported concerns about the pandemic were at a high level and increasing support to measures implemented by authorities to keep distance and lower the number of contacts was reported [19,20].
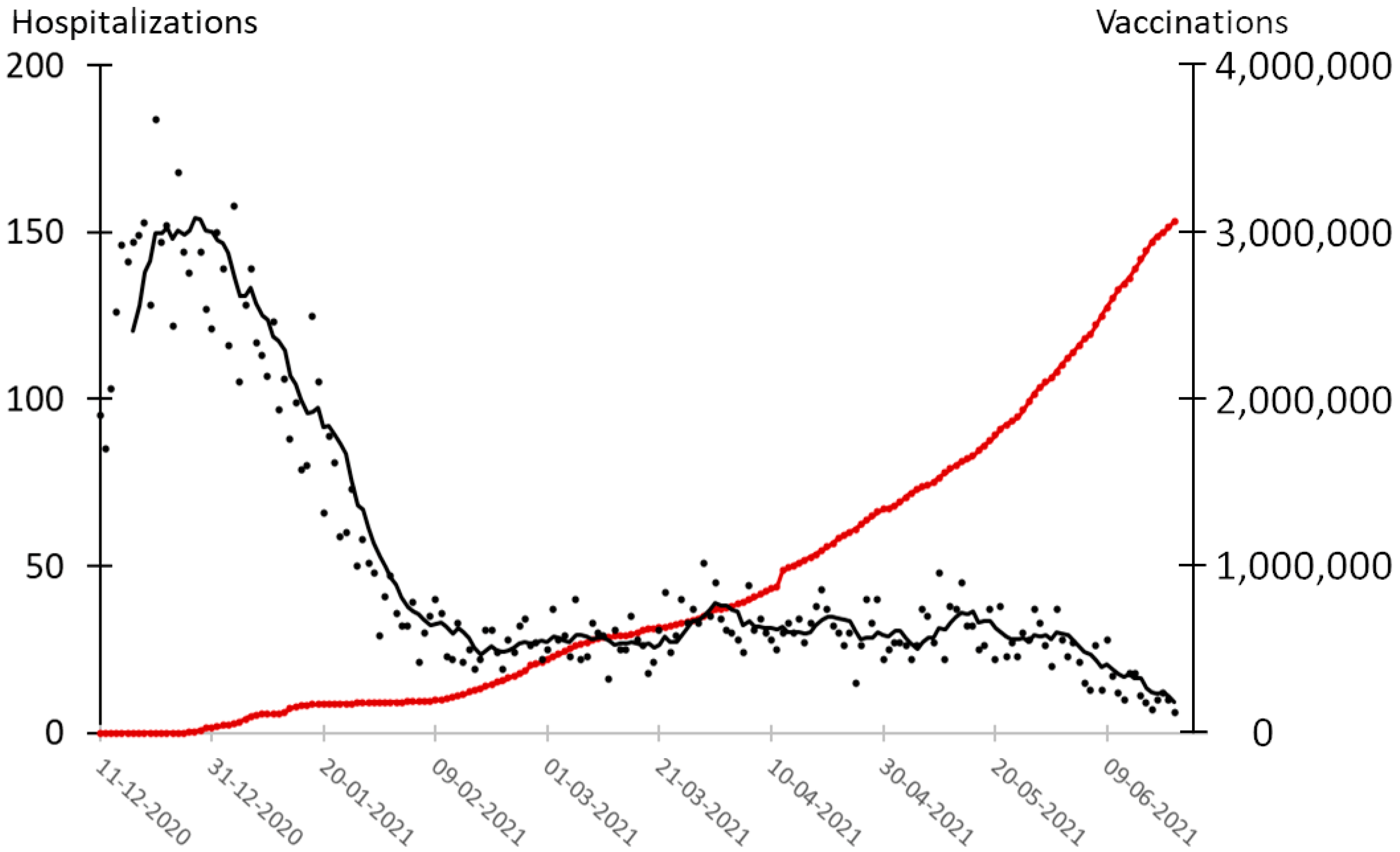
- Stage 2 (11 December 2020 to 28 February 2021): A winter lockdown with severe restrictions was implemented [21]. Hospitalizations peaked at 210 on 28 December 2020 and testing increased from 102,431 tests per day to 143,001 tests per day. Vaccinations started on 27 December and reached 7.3% of the population; most comprised elderly on 28 February [6,22]. Awareness of social distancing and of reducing the number of contacts was high and increased during this period [20]. The population was concerned, and the support for following advice from authorities was high [19].
- Stage 3 (6 April 2021–21 June 2021): Schools, other educational institutions, and small businesses such as hairdressers, tattoo hops, massage parlors, and others were reopened [23]. Malls were reopened on 21 April and many indoor facilities such as restaurants and museums opened on 6 May for guests that had been vaccinated or had a negative COVID-19 test not older than 72 h [24]. The requirement for facemasks was abandoned on 14 June [25]. This period includes the most extensive level of mass testing with an average of 466,861 tests per day corresponding to 8049 tests per day per 100,000 persons. By the end of May, all citizens above 65 years had been offered a COVID-19 vaccine, and 37.4% of the population had received the first dose [3,15]. On 21 June 2021, 53% of the population had received the first dose. Awareness of social distancing and of reducing the number of contacts was low and decreased during this period [20]. Adherence to self-isolation was low. The population was not that worried and reported decreasing will to follow advice from authorities [19].
3.2. Effect of Testing on Hospitalizations
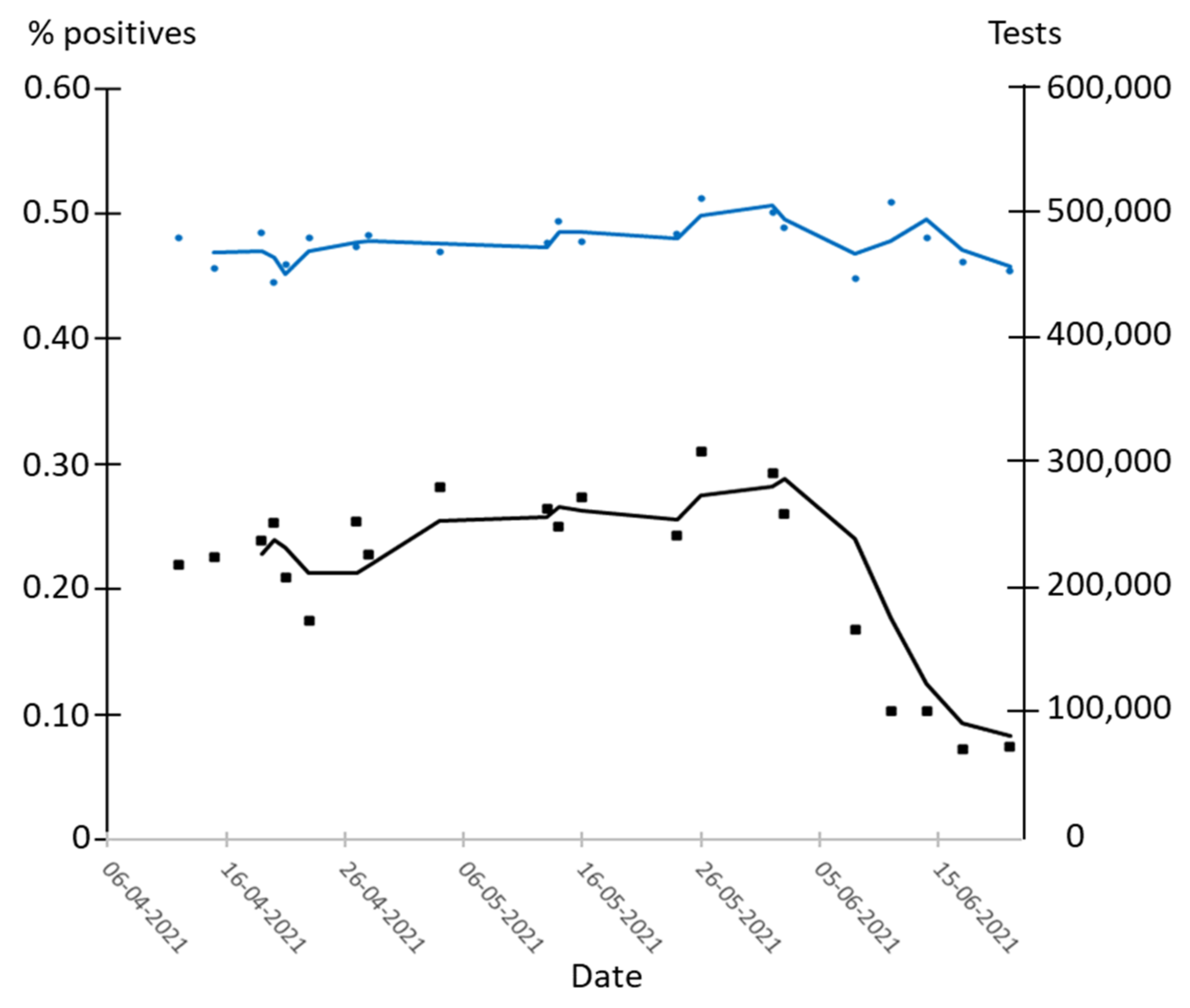
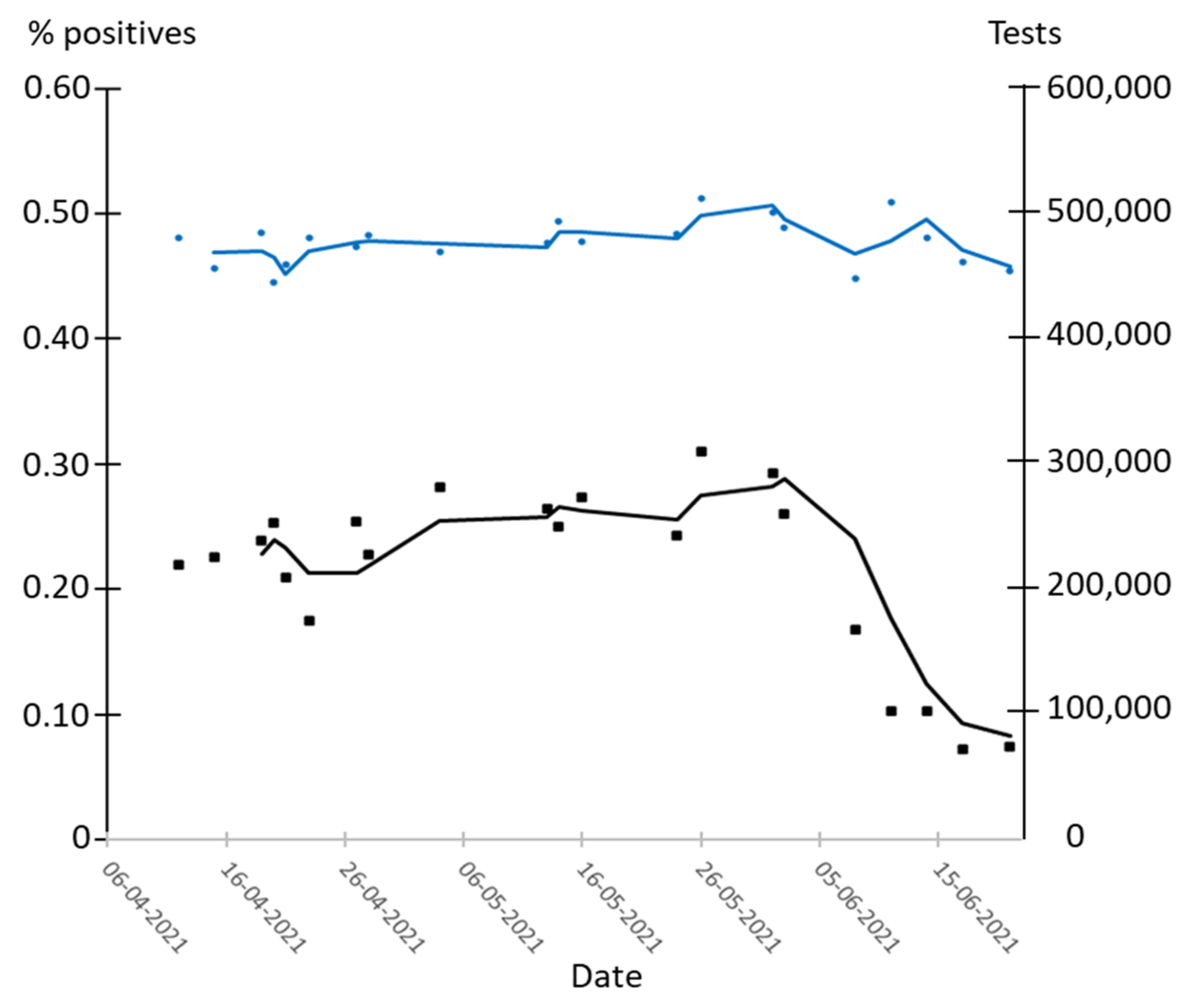
3.3. Effect of Testing on Percentage of Positive Tests
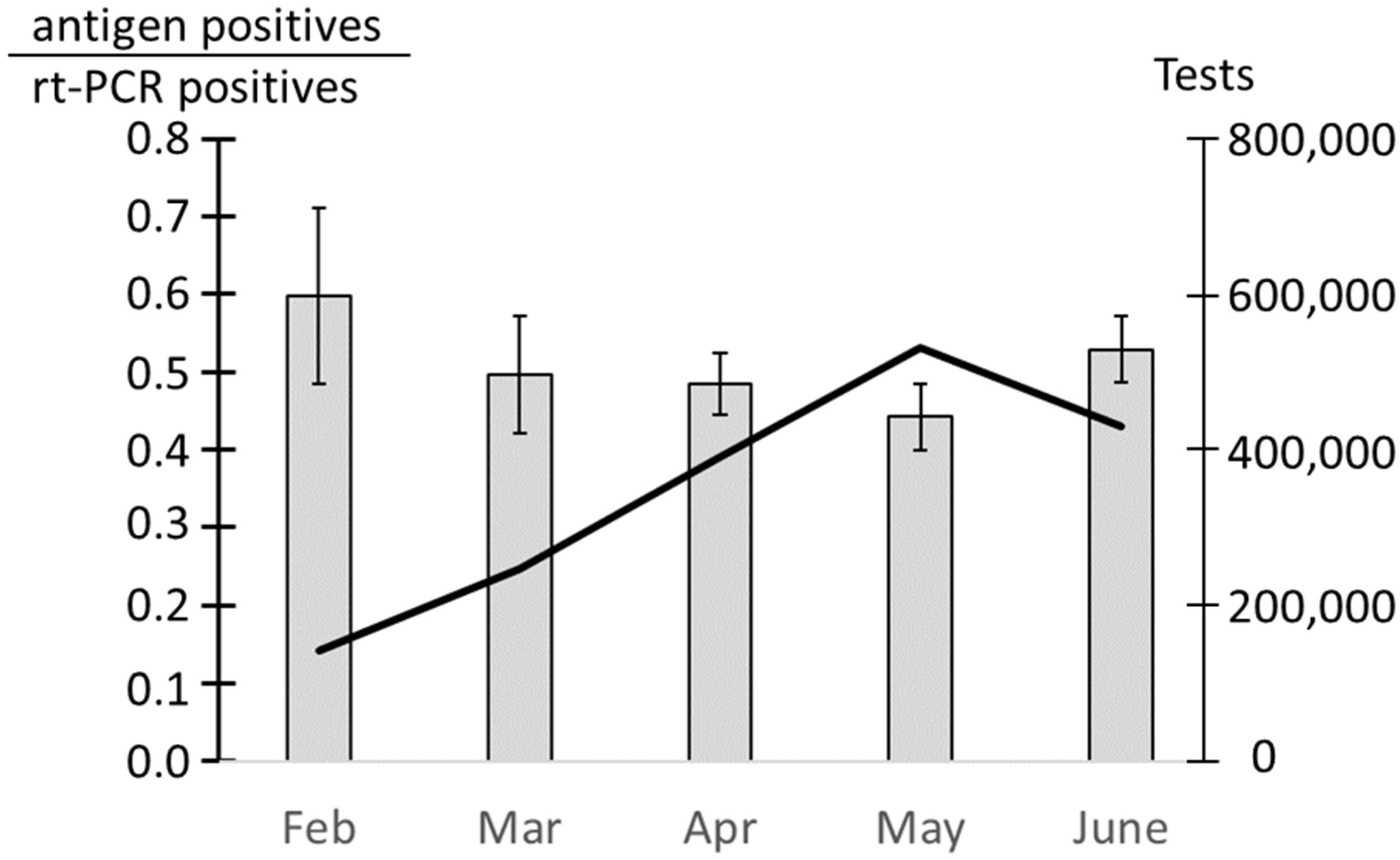
3.4. Ratio between Positive Antigen Tests and Rt-PCR Tests
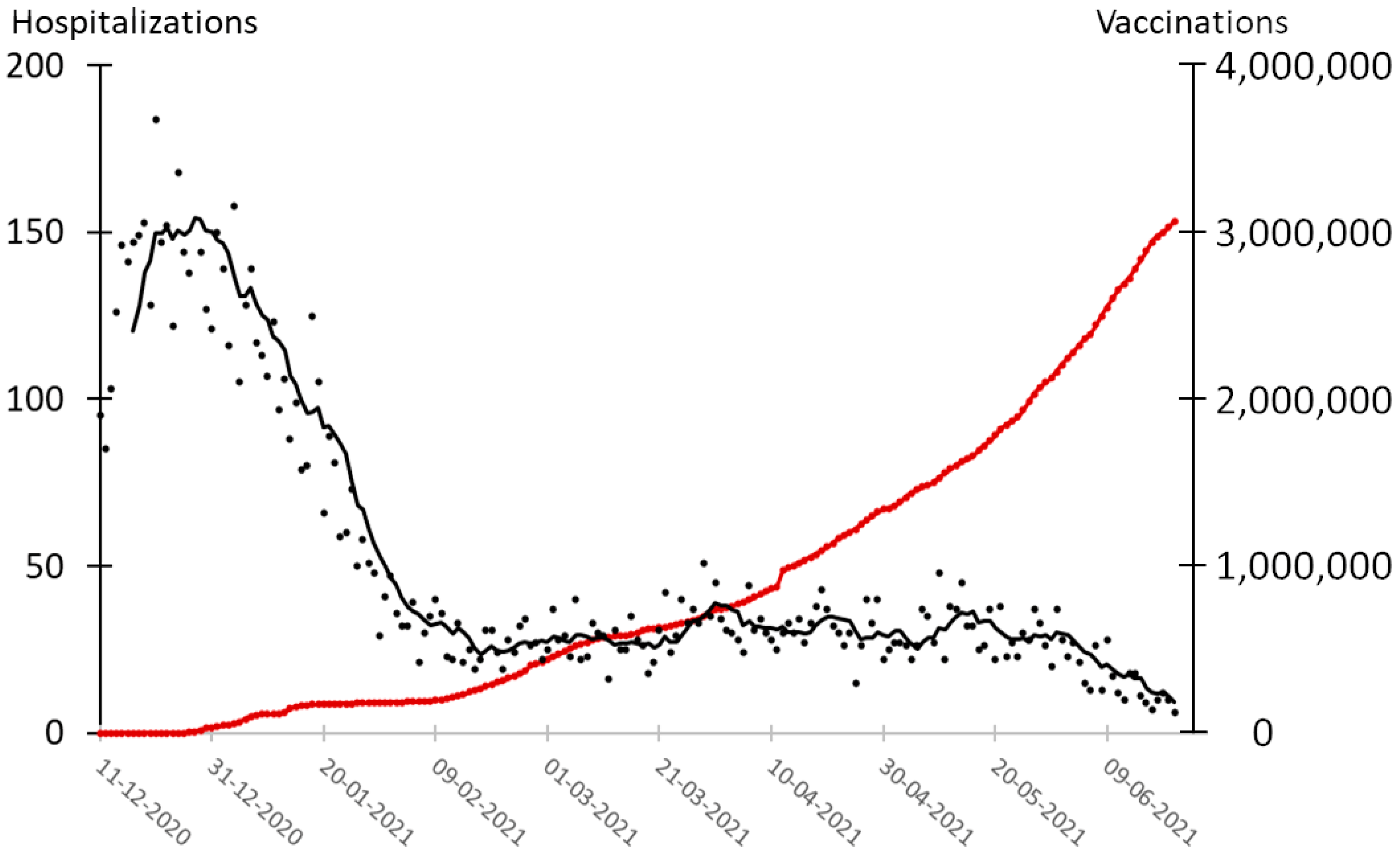
3.5. Vaccination and Hospitalizations Correlated
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Peto, J. COVID-19 Mass Testing Facilities Could End the Epidemic Rapidly. BMJ 2020, 368, 1163. [Google Scholar] [CrossRef] [Green Version]
- Gill, M.; Gray, M. Mass Testing for COVID-19 in the UK. BMJ 2020, 371, 4436. [Google Scholar] [CrossRef]
- Statens Serum Institut. Første Dansker Testet Positiv for COVID-19. Available online: https://www.ssi.dk/aktuelt/nyheder/2020/02_27_foerste-tilfaelde-af-ny-coronavirus-i-dk (accessed on 28 June 2021).
- The Danish Ministry of Health. Teststrategi Skal Sikre at Flest Muligt Testes for COVID-19. Available online: https://sum.dk/nyheder/2020/marts/teststrategi-skal-sikre-at-flest-muligt-testes-for-COVID-19 (accessed on 28 June 2021).
- The Danish Ministry of Health. Alle Borgere får Mulighed for at Blive Testet for COVID-19. Available online: https://sum.dk/nyheder/2020/maj/alle-borgere-faar-mulighed-for-at-blive-testet-for-COVID-19- (accessed on 1 November 2021).
- Ritchie, H.; Ortiz-Ospina, E.; Beltekian, D.; Mathieu, E.; Hasell, J.; Macdonald, B.; Giattino, C.; Appel, C.; Rodés-Guirao, L.; Roser, M. Coronavirus Pandemic (COVID-19). Our World Data 2020. [Google Scholar]
- The Danish Ministry of Health. Regeringen Tilpasser Teststrategi til Gradvis Genåbning af Samfundet. Available online: https://sum.dk/nyheder/2021/marts/regeringen-tilpasser-teststrategi-til-gradvis-genaabning-af-samfundet (accessed on 28 June 2021).
- Pavelka, M.; Van-Zandvoort, K.; Abbott, S.; Sherratt, K.; Majdan, M.; Group, C.C.; Analýz, I.Z.; Jarčuška, P.; Krajčí, M.; Flasche, S.; et al. The Impact of Population-Wide Rapid Antigen Testing on SARS-CoV-2 Prevalence in Slovakia. Science 2021, 372, 635–641. [Google Scholar] [CrossRef]
- Holt, E. COVID-19 Testing in Slovakia. Lancet Infect. Dis 2021, 21, 32. [Google Scholar] [CrossRef]
- Kahanec, M.; Lafférs, L.; Schmidpeter, B. The Impact of Repeated Mass Antigen Testing for COVID-19 on the Prevalence of the Disease. J. Popul. Econ. 2021, 34, 1105–1140. [Google Scholar] [CrossRef]
- Statens Serum Institut. Dagens COVID-19-Opgørelser—Dsownload Filerne her. Available online: https://covid19.ssi.dk/overvagningsdata/download-fil-med-overvaagningdata (accessed on 29 June 2021).
- Pedersen, R.K.; Berrig, C.; Ørskov, S.; Simonsen, L.; Andreasen, V. Effekten af COVID-19 screening i Danmark; Roskilde University: Roskilde, Denmark, 2021. [Google Scholar]
- Statens Serum Institut. Download fil Med Vaccinations Data for COVID-19. Available online: https://covid19.ssi.dk/overvagningsdata/download-fil-med-vaccinationsdata (accessed on 5 July 2021).
- Bravais, A. Analyse Mathématique sur les Probabilités des Erreurs de Situation D’un Point; Imprimerie Royale: Paris, France, 1844. [Google Scholar]
- The Danish Government. Aftale om Yderligere Genåbning i fase 2. Available online: https://www.regeringen.dk/nyheder/2020/aftale-om-yderligere-genaabning-i-fase-2/ (accessed on 29 June 2021).
- The Prime Minister’s Office. Pressemøde om COVID-19 den 11. Marts 2020. Available online: https://www.stm.dk/presse/pressemoedearkiv/pressemoede-om-COVID-19-den-11-marts-2020/ (accessed on 29 June 2021).
- The Danish Ministry of Health Bekendtgørelse. Om Krav Om Mundbind m.v. i Kollektiv Trafik m.v.; Danish Ministry of Health: Copenhagen, Denmark, 2020; Volume 1221. [Google Scholar]
- The Danish Ministry of Health. Bekendtgørelse Om Krav Om Mundbind m.v. På Serveringssteder, i Detailhandlen, Kultur- Og Kirkeinstitutioner, Idræts- Og Foreningsfaciliteter Og På Uddannelsesinstitutioner i Forbindelse Med Håndtering Af COVID-19; Danish Ministry of Health: Copenhagen, Denmark, 2020; Volume 1534. [Google Scholar]
- Petersen, M.B.; Roepstorff, A. Danskernes Adfærd Og Holdninger Til Corona-Epidemien; The Hope Project; Aarhus University: Aarhus, DK, USA, 2021. [Google Scholar]
- Rasmussen, M.S.; Jørgensen, F.; Bor, A.; Petersen, M.B. Danskernes Smitteforebyggende Adfærd Og Opfattelser; The Hope Project; Aarhus University: Aarhus, Denmark, 2021. [Google Scholar]
- The Danish Ministry of Health. Udvidelse af Skærpede tiltag til i alt 69 Kommuner. Available online: https://sum.dk/nyheder/2020/december/udvidelse-af-skaerpede-tiltag-til-i-alt-69-kommuner (accessed on 29 June 2021).
- Danish Health Authority. Vaccinations Kalender. Available online: https://www.sst.dk/da/udgivelser/2021/vaccinationskalender (accessed on 29 June 2021).
- Nationalt Kommunikations Partnerskab. COVID-19 Genåbning af Danmark. Available online: http://coronasmitte.dk/nyt-fra-myndighederne/proces-for-tiltag-og-restriktioner/genaabning-af-danmark (accessed on 29 June 2021).
- The Danish Government. Rammeaftale om plan for Genåbning af Danmark. Available online: https://www.stm.dk/presse/pressemeddelelser/rammeaftale-om-plan-for-genaabning-af-danmark/ (accessed on 29 June 2021).
- The Danish Government. Aftale om Udfasning af Restriktioner fra 11. juni 2021. Available online: https://www.regeringen.dk/nyheder/2021/aftale-om-udfasning-af-restriktioner-fra-11-juni-2021/ (accessed on 29 June 2021).
- Cevik, M.; Tate, M.; Lloyd, O.; Maraolo, A.E.; Schafers, J.; Ho, A. SARS-CoV-2, SARS-CoV, and MERS-CoV Viral Load Dynamics, Duration of Viral Shedding, and Infectiousness: A Systematic Review and Meta-Analysis. Lancet Microbe 2021, 2, e13–e22. [Google Scholar] [CrossRef] [PubMed]
- Mallett, S.; Allen, A.J.; Graziadio, S.; Taylor, S.A.; Sakai, N.S.; Green, K.; Suklan, J.; Hyde, C.; Shinkins, B.; Zhelev, Z.; et al. At What Times during Infection Is SARS-CoV-2 Detectable and No Longer Detectable Using RT-PCR-Based Tests? A Systematic Review of Individual Participant Data. BMC Med. 2020, 18, 346. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Coronavirus Disease 2019 (COVID-19): Situation Report; WHO: Geneva, Switzerland, 2020; Volume 73. [Google Scholar]
- Meyerowitz, E.A.; Richterman, A.; Gandhi, R.T.; Sax, P.E. Transmission of SARS-CoV-2: A Review of Viral, Host, and Environmental Factors. Ann. Intern. Med. 2021, 174, 69–79. [Google Scholar] [CrossRef] [PubMed]
- Faes, C.; Abrams, S.; Van Beckhoven, D.; Meyfroidt, G.; Vlieghe, E.; Hens, N. Time between Symptom Onset, Hospitalisation and Recovery or Death: Statistical Analysis of Belgian COVID-19 Patients. Int. J. Environ. Res. Public Health 2020, 17, 7560. [Google Scholar] [CrossRef]
- Jørgensen, F.; Lindholdt, M.F.; Petersen, M.B. Befolkningens Selvrapporterede Overholdelse Af Anbefalingerne Om Selvisolation; The Hope Project; Aarhus University: Aarhus, Denmark, 2020. [Google Scholar]
- Engelbrecht, F.A.; Scholes, R.J. Test for Covid-19 Seasonality and the Risk of Second Waves. One Health 2021, 12, 100202. [Google Scholar] [CrossRef] [PubMed]
- Dinnes, J.; Deeks, J.J.; Berhane, S.; Taylor, M.; Adriano, A.; Davenport, C.; Dittrich, S.; Emperador, D.; Takwoingi, Y.; Cunningham, J.; et al. Rapid, Point-of-Care Antigen and Molecular-Based Tests for Diagnosis of SARS-CoV-2 Infection. Cochrane Database Syst. Rev. 2021, 3, CD013705. [Google Scholar] [CrossRef]
- Ledford, H. Six Months of COVID Vaccines: What 1.7 Billion Doses Have Taught Scientists. Nature 2021, 594, 164–167. [Google Scholar] [CrossRef]
- Haas, E.J.; Angulo, F.J.; McLaughlin, J.M.; Anis, E.; Singer, S.R.; Khan, F.; Brooks, N.; Smaja, M.; Mircus, G.; Pan, K.; et al. Impact and Effectiveness of MRNA BNT162b2 Vaccine against SARS-CoV-2 Infections and COVID-19 Cases, Hospitalisations, and Deaths Following a Nationwide Vaccination Campaign in Israel: An Observational Study Using National Surveillance Data. Lancet 2021, 397, 1819–1829. [Google Scholar] [CrossRef] [PubMed]
- Mercer, T.R.; Salit, M. Testing at Scale during the COVID-19 Pandemic. Nat. Rev. Genet. 2021, 22, 415–426. [Google Scholar] [CrossRef] [PubMed]
- Gorji, H.; Lunati, I.; Rudolf, F.; Vidondo, B.; Hardt, W.-D.; Jenny, P.; Engel, D.; Schneider, J.; Jamnicki, M.; Leuthold, R.; et al. Results from Canton Grisons of Switzerland Suggest Repetitive Testing Reduces SARS-CoV-2 Incidence (February-March 2021). medRxiv 2021. [Google Scholar] [CrossRef]
- Jun, S.-P.; Yoo, H.S.; Lee, J.-S. The Impact of the Pandemic Declaration on Public Awareness and Behavior: Focusing on COVID-19 Google Searches. Technol. Forecast. Soc. Chang. 2021, 166, 120592. [Google Scholar] [CrossRef]
- Bourassa, J.A.L.; Steven, M.; Lieberman, A.; Lori, A. What Tests to Use, When, Why—and Why Not? Pitfalls of Mass Testing for COVID-19. The Brookings Institution, 2020. Available online: https://www.brookings.edu/blog/usc-brookings-schaeffer-on-health-policy/2020/10/27/sars-cov-2-testing-what-tests-to-use-when-why-and-why-not/ (accessed on 28 June 2021).
- Hu, X.; Deng, Q.; Li, J.; Chen, J.; Wang, Z.; Zhang, X.; Fang, Z.; Li, H.; Zhao, Y.; Yu, P.; et al. Development and Clinical Application of a Rapid and Sensitive Loop-Mediated Isothermal Amplification Test for SARS-CoV-2 Infection. mSphere 2020, 5, e00808-20. [Google Scholar] [CrossRef]
- Simon, A.E.; Wu, A.W.; Lavori, P.W.; Sugarman, J. Preventive Misconception: Its Nature, Presence, and Ethical Implications for Research. Am. J. Prev. Med. 2007, 32, 370–374. [Google Scholar] [CrossRef]
- Cao, S.; Gan, Y.; Wang, C.; Bachmann, M.; Wei, S.; Gong, J.; Huang, Y.; Wang, T.; Li, L.; Lu, K.; et al. Post-Lockdown SARS-CoV-2 Nucleic Acid Screening in Nearly Ten Million Residents of Wuhan, China. Nat. Commun. 2020, 11, 5917. [Google Scholar] [CrossRef]
- Li, Z.; Liu, F.; Cui, J.; Peng, Z.; Chang, Z.; Lai, S.; Chen, Q.; Wang, L.; Gao, G.F.; Feng, Z. Comprehensive Large-Scale Nucleic Acid-Testing Strategies Support China’s Sustained Containment of COVID-19. Nat. Med. 2021, 27, 740–742. [Google Scholar] [CrossRef] [PubMed]
- Xing, Y.; Wong, G.W.K.; Ni, W.; Hu, X.; Xing, Q. Rapid Response to an Outbreak in Qingdao, China. N. Engl. J. Med. 2020, 383, e129. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Stage | Dates | Average Daily Tests per 100,000 Inhabitants | Average Daily Hospitalizations | Correlation 7 Days Delay | Correlation 14 Days Delay | Correlation 21 Days Delay |
|---|---|---|---|---|---|---|
| All | 27 May 2020–21 June 2021 | 2722 | 34 | 0.02 (0.66) | 0.00 (0.99) | −0.02 (0.74) |
| 0 | 01 March 2020–26 May 2020 | 114 | 28 | −0.61 (0.00) | −0.71 (0.00) | −0.66 (0.00) |
| 1 | 27 May 2020–06 December 2020 | 652 | 16 | 0.87 (0.00) | 0.83 (0.00) | 0.81 (0.00) |
| 2 | 11 December 2020–28 February 2021 | 1949 | 83 | −0.22 (0.06) | −0.06 (0.65) | 0.07 (0.61) |
| 3 | 06 April 2021–21 June 2021 | 8049 | 27 | 0.16 (0.19) | −0.06 (0.63) | −0.24 (0.07) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Busk, P.K.; Kristiansen, T.B.; Engsig-Karup, A. Assessment of the National Test Strategy on the Development of the COVID-19 Pandemic in Denmark. Epidemiologia 2021, 2, 540-552. https://doi.org/10.3390/epidemiologia2040037
Busk PK, Kristiansen TB, Engsig-Karup A. Assessment of the National Test Strategy on the Development of the COVID-19 Pandemic in Denmark. Epidemiologia. 2021; 2(4):540-552. https://doi.org/10.3390/epidemiologia2040037
Chicago/Turabian StyleBusk, Peter Kamp, Thomas Birk Kristiansen, and Allan Engsig-Karup. 2021. "Assessment of the National Test Strategy on the Development of the COVID-19 Pandemic in Denmark" Epidemiologia 2, no. 4: 540-552. https://doi.org/10.3390/epidemiologia2040037
APA StyleBusk, P. K., Kristiansen, T. B., & Engsig-Karup, A. (2021). Assessment of the National Test Strategy on the Development of the COVID-19 Pandemic in Denmark. Epidemiologia, 2(4), 540-552. https://doi.org/10.3390/epidemiologia2040037