A Modified Technique for Fabricating Customized Angled Dual Abutments for Implants with Severe Angulations

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
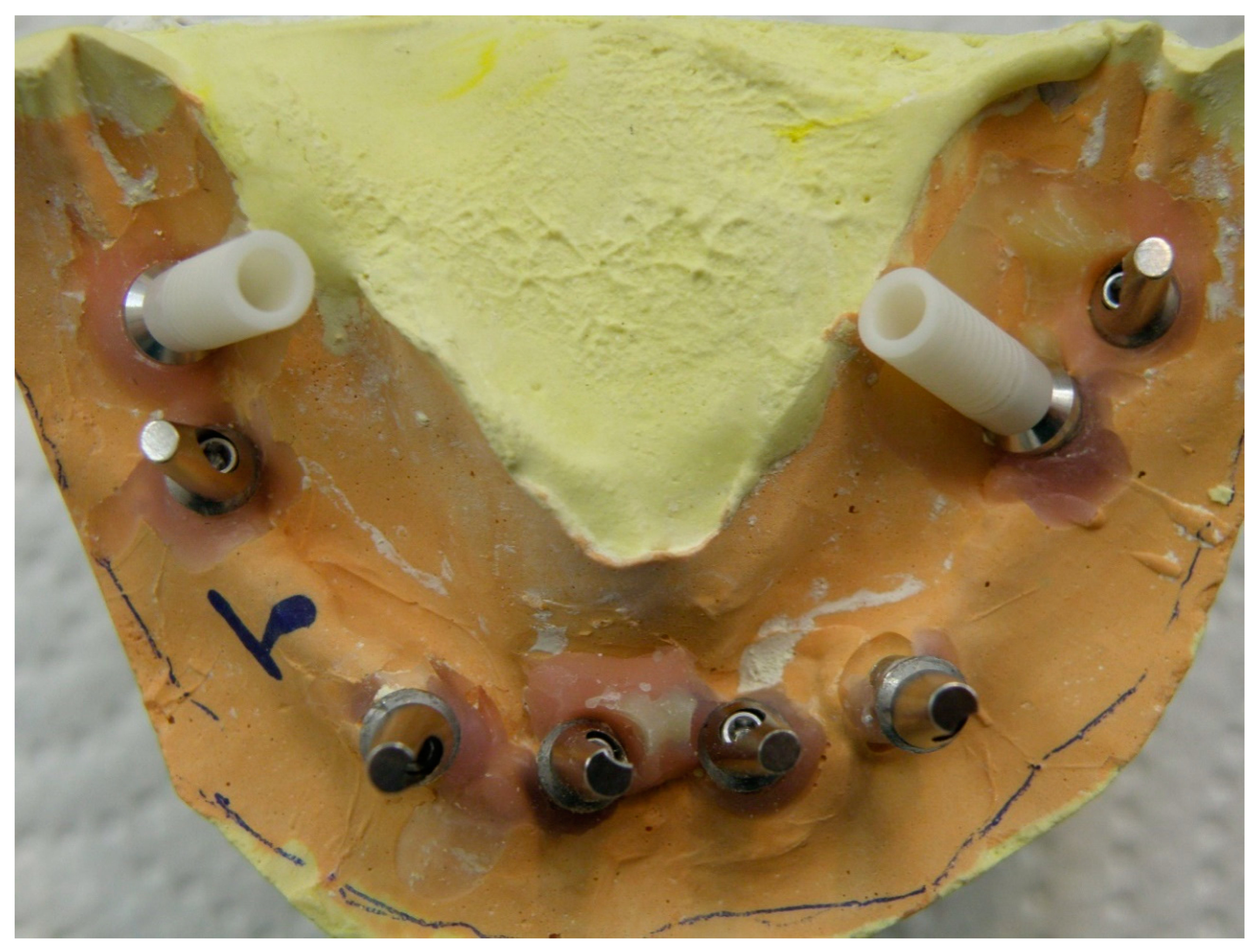
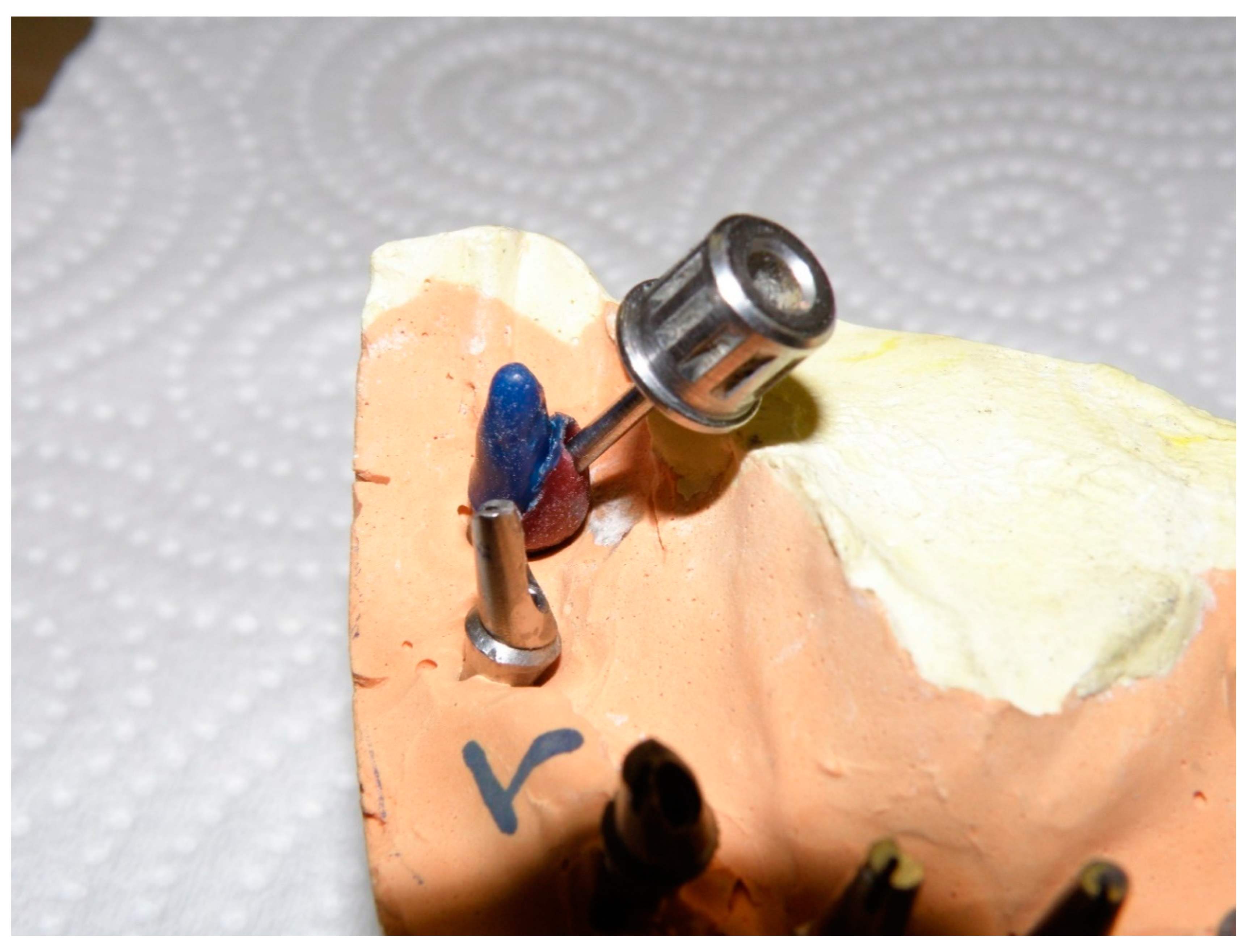
2. Technique Report
3. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Berroeta, E.; Zabalegui, I.; Donovan, T.; Chee, W. Dynamic abutment: A method of redirecting screw access for implant-supported restorations: Technical details and a clinical report. J. Prosthet. Dent. 2015, 113, 516–519. [Google Scholar] [CrossRef] [PubMed]
- Grunder, U.; Gracis, S.; Capelli, M. Influence of the 3-D bone-to-implant relationship on esthetics. Int. J. Periodontics Restor. Dent. 2005, 25, 113–119. [Google Scholar]
- Tarnow, D.P.; Cho, S.C.; Wallace, S.S. The effect of inter-implant distance on theheight of inter-implant bone crest. J. Periodontol. 2000, 71, 546–549. [Google Scholar] [CrossRef]
- Grossmann, Y.; Madjar, D. Prosthetic treatment for severely misaligned implants: A clinical report. J. Prosthet. Dent. 2002, 88, 259–262. [Google Scholar] [CrossRef] [PubMed]
- Eger, D.E.; Gunsolley, J.C.; Feldman, S. Comparison of angled and standard abutments and their effect on clinical outcomes: A preliminary report. Int. J. Oral Maxillofac. Implant. 2000, 15, 819–823. [Google Scholar]
- Malo, P.; Rangert, B.; Nobre, M. All-on-four immediate-function concept with Branemark system implants for completely edentulous mandibles: A retrospective clinical study. Clin. Implant. Dent. Relat. Res. 2003, 5, 2–9. [Google Scholar] [CrossRef] [PubMed]
- Sethi, A.; Kaus, T.; Sochor, P.; Axmann-Krcmar, D. Evolution of theconcept of angulated abutments in implant dentistry: 14-year clinical data. Implant. Dent. 2002, 11, 41–51. [Google Scholar] [CrossRef] [PubMed]
- Cavallaro, J., Jr.; Greenstein, G. Angled implant abutments: A practical application of available knowledge. J. Am. Dent. Assoc. 2011, 142, 150–158. [Google Scholar] [CrossRef]
- Ha, C.Y.; Lim, Y.J.; Kim, M.J.; Choi, J.H. The influence of abutment angulation onscrew loosening of implants in the anterior maxilla. Int. J. Oral Maxillofac. Implant. 2011, 26, 45–55. [Google Scholar]
- Guichet, D.L.; Yoshinobu, D.; Caputo, A.A. Effect of splinting and interproximal contact tightness on load transfer by implant restorations. J. Prosthet. Dent. 2002, 87, 528–535. [Google Scholar] [CrossRef]
- Grossmann, Y.; Finger, I.M.; Block, M.S. Indications for splinting implant restorations. J. Oral Maxillofac. Surg. 2005, 63, 1642–1652. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.M.; Leu, L.J.; Wang, J.; Lin, L.D. Effects of prosthesis materials and prosthesis splinting on periimplant bone stress around implants in poor quality bone: A numeric analysis. Int. J. Oral Maxillofac. Implant. 2002, 17, 231–237. [Google Scholar]
- Nematollahi, F.; Beyabanaki, E.; Alikhasi, M. Cement Selection for Cement-Retained Implant-Supported Prostheses: A Literature Review. J. Prosthodont. 2016, 25, 599–606. [Google Scholar] [CrossRef] [PubMed]
- Lundgren, D.; Laurell, L. Biomechanical aspects of fixed bridgework supported by natural teeth and endosseous implants. Periodontology 2000 1994, 4, 23–40. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.S.; Kum, Y.L.; Bae, J.M. Biomechanical comparison of axial and tilted implants for mandibular full arch fixed prosthesis. Int. J. Oral Maxillofac. Implant. 2011, 26, 976–984. [Google Scholar]
- Falk, H.; Laurell, L.; Lundgren, D. Occlusal interferences and cantilever joint stress in implant-supported prostheses occluding with complete dentures. Int. J. Oral Maxillofac. Implant. 1990, 5, 70–77. [Google Scholar]
- Lundgren, D.; Falk, H.; Laurell, L. Influence of number and distribution of occlusal cantilever contacts on closing and chewing forces in dentitions with implant-supported fixed prostheses occluding with complete dentures. Int. J. Oral Maxillofac. Implant. 1989, 4, 277–283. [Google Scholar]





© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saboury, A.; Beyabanaki, E. A Modified Technique for Fabricating Customized Angled Dual Abutments for Implants with Severe Angulations. Prosthesis 2020, 2, 246-251. https://doi.org/10.3390/prosthesis2040022
Saboury A, Beyabanaki E. A Modified Technique for Fabricating Customized Angled Dual Abutments for Implants with Severe Angulations. Prosthesis. 2020; 2(4):246-251. https://doi.org/10.3390/prosthesis2040022
Chicago/Turabian StyleSaboury, Aboulfazl, and Elaheh Beyabanaki. 2020. "A Modified Technique for Fabricating Customized Angled Dual Abutments for Implants with Severe Angulations" Prosthesis 2, no. 4: 246-251. https://doi.org/10.3390/prosthesis2040022
APA StyleSaboury, A., & Beyabanaki, E. (2020). A Modified Technique for Fabricating Customized Angled Dual Abutments for Implants with Severe Angulations. Prosthesis, 2(4), 246-251. https://doi.org/10.3390/prosthesis2040022