


Cognitive Impairment in Celiac Disease Patients: Scoping Review Exploring Psychological Triggers in a Chronic Condition


Abstract
1. Introduction
- Typical CD: The classic manifestation of CD with full expression of gluten-sensitive enteropathy associated with malabsorption, and positive duodenal biopsy and serology for Endomysial (IgA) and Tissue Transglutaminase antibodies (tTG).
- Atypical CD: Full expression of gluten-sensitive enteropathy found in association with non-gastrointestinal symptoms.
- Silent CD: Patients presenting a normal biopsy but positive serology.
- Refractory CD: Patients with severe mucosal injury but do not respond to a GFD.
2. Materials and Methods
- To summarize the current evidence on the features of CD-associated cognitive impairments.
- To identify gaps and limits in the literature that may require further research.
- To identify relevant research questions, particularly, the determinants of future approaches.
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Article Selection and Data Extraction
2.4. Statistical Analysis
3. Results
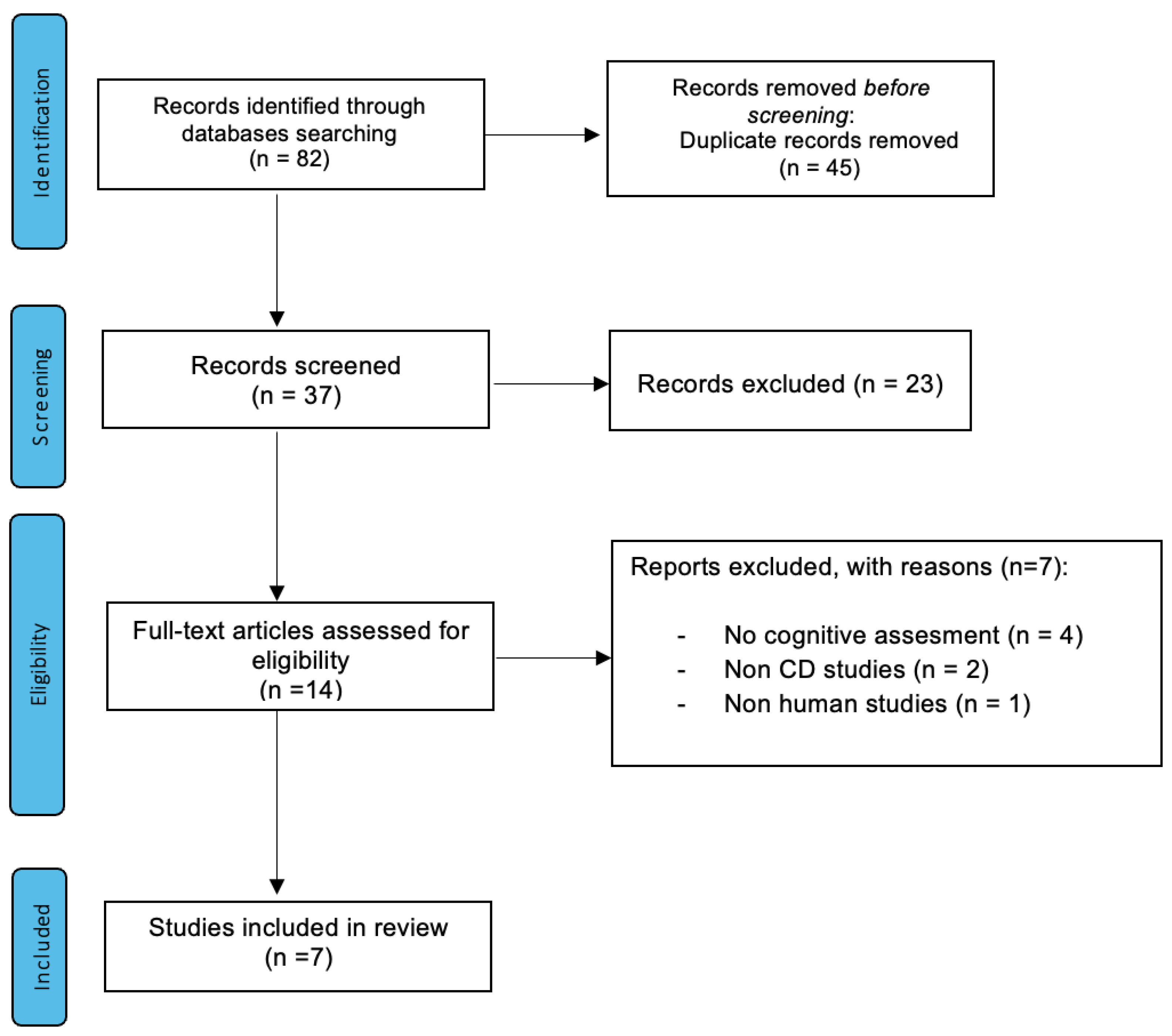
3.1. Search Results
3.2. Characteristics of Included Articles/Studies
3.3. Source of Articles/Studies
3.4. Type of Articles/Studies
3.5. Cognitive Modification in CD

{kind=link}
| Authors | Topic | Sample Size | Target Sample | Tests | Outcomes |
|---|---|---|---|---|---|
| Casella et al. (2012) [15] | C.I. + GFD + EMOT. FEATURES | n° 18 | Patients aged ≥65 at the time of CD diagnosis All tested t-Tg or i-GA antibodies and villous atrophy (MARSH III in 16 patients, MARSH I-II in 2 patients) | -MMSE -TMT (A, B, B-A) -Rey list -Verbal Fluency -Verbal span -Short story test -Digit symbol -Semantic memory -Episodic memory -Ideo-motor apraxia -Bucco-facial apraxia -GDS | “Raw score” significantly lower in CD than controls for: -Mini Mental Test Examination (p = 0.02), -Trial making test (p = 0.001), -Semantic fluency (p = 0.03), -Digit Symbol Test (p = 0.007), -Ideo-motor apraxia (p < 0.001), -Bucco-facial apraxia (p < 0.002). “Equivalent score” lower in CD than controls for: -Semantic memory (p < 0.01), -Ideo-motor apraxia (p = 0.007). Barthel Index of functional performance was similar in the 2 groups. |
| Lichtwark et al. (2014) [16] | C.I. + GFD + EMOT. FEATURES | n° 11 | CD diagnosed patients (MARSH III or MARSH I and II + antibodies positivity) GFD less than 4 weeks prior to the enrollment Excellent adherence to diet Mean age = 30 (Age range = 22–39) | -SCIT -TMT A&B-ROCF COWAT -RAVLT -Grooved Pegboard Task -WTAR -STPI (anxiety and depression subscales) | At week 52: MARSH improved significantly (p = 0.001) Tissue transglutaminase decreased from mean of 58.4 at baseline to 16.8 U/mL at week 52 (p = 0.025). Significant improvement at: -verbal fluency, -attention, -motor functions. Improvement showed strong correlation with improvements in Marsh scores and tissue transglutaminase antibody levels (r = 0.377–0.735; all p< 0.05). Cognition was impaired in people with untreated CD. |
| Longarini et al. (2019) [17] | C.I. + GFD + EMOT. FEATURES | n° 53 | Adults with symptoms and signs compatible with CD Mean age = 34 (Age range = 18–50) | -ACE-R -INECO -FAQ -BDI -STAI | 33 CD patients (66%) compared to healthy controls, CD cases and disease controls had: -impaired cognitive performance (p = 0.02 and p = 0.04, respectively), -functional impairment (p < 0.01), -higher depression (p < 0.01). CD patients compared to controls: -Similar cognitive performance, -Anxiety, -Nonsignificant lower depression scores compared with disease controls. Abnormal cognitive functions detected in adult NCD not disease-specific. Cognitive dysfunction was related to presence of prolonged symptoms due to a chronic disease. |
| Croall et al. (2020) [18] | C.I. + GFD + EMOT. FEATURES | n° 54 | NCD = 19 (Newly diagnosed CD); ECD = 35 (Established CD) Mean age = 44 (Age range = 18–70) | -ToPF -WAIS (Block design, vocabulary, matrix reasoning, similarities) -TMT -COWAT -Digit span -Story recall -CVLT -ROCF -Digit-symbol coding -SOIP -BDAE (verbal agility) -SF-36 (QOL) | NCD and ECD underperformed compared to controls, by comparable degrees in: -visual memory (overall model: p < 0.001), -verbal memory (p = 0.046). The ECD group underperformed only in visuo-constructive abilities (p = 0.050). QoL: NCD = lower vitality (p = 0.030), ECD = more bodily pain (p = 0.009). Dysfunction appears established at the point of diagnosis, after which it (predominantly) stabilizes. |
| Croall et al. (2020) [19] | C.I. + EMOT. FEATURES + NEURO IMAGING | n° 104 | 65% female, Mean age = 63 | -Digit span -Biobank’s fluid intelligence -TMT B-A -Pair matching task 6 questions exploring: -anxiety -depression -happiness with own health -suicidal thoughts -thoughts of self-harm | Compared with control individuals, participants with celiac disease had significant deficits in: -reaction time (p = 0.004). Significantly higher proportions had indications of: -anxiety (p = 0.025), -depression (p = 0.015), -thoughts of self-harm (p = 0.025), -health-related unhappiness (p = 0.010). White matter changes in the brains of participants with celiac disease. |
| Fisicaro et al. (2021) [20] | C.I. + EMOT. FEATURES + TMS | n° 15 | 15 right-handed, neurologically asymptomatic, de novo CD patients Mean age 34.1 | -MOCA -HDRS -TMS | -MoCA and HDRS scored significantly worse in CD patients. -iSP and cSP significantly shorter in duration in CD, positive correlation between the MoCA and iSP -Intracortical and interhemispheric motor disinhibition observed in CD, suggesting the involvement of GABA-mediated cortical and callosal circuitries. |
| Lanza et al. (2021) [21] | C.I. + EMOT. FEATURES + TMS | n° 15 | 15 right-handed, neurologically asymptomatic, de novo CD patients Mean age 34.1 | -MOCA -HDRS -TMS | Central cholinergic functioning not affected in de novo CD patients compared to healthy controls. Statistically significant difference in MoCA, but no overt cognitive impairment in CD patients. |
3.6. Effects of Gluten-Free Diet
3.7. Emotional Features
3.8. Neuroimaging and TMS
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Caio, G.; Volta, U.; Sapone, A.; Leffler, D.A.; De Giorgio, R.; Catassi, C.; Fasano, A. Celiac disease: A comprehensive current review. BMC Med. 2019, 17, 142. [Google Scholar] [CrossRef] [PubMed]
- Ludvigsson, J.F.; Leffler, D.A.; Bai, J.C.; Biagi, F.; Fasano, A.; Green, P.H.R.; Hadjivassiliou, M.; Kaukinen, K.; Kelly, C.P.; Leonard, J.N.; et al. The Oslo definitions for coeliac disease and related terms. Gut 2013, 62, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Mustalahti, K.; Catassi, C.; Reunanen, A.; Fabiani, E.; Heier, M.; McMillan, S.; Murray, L.; Metzger, M.-H.; Gasparin, M.; Bravi, E.; et al. The prevalence of celiac disease in Europe: Results of a centralized, international mass screening project. Ann. Med. 2010, 42, 587–595. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.E.; Lee, H.E.; Wu, T.-T. Histologic evaluation in the diagnosis and management of celiac disease: Practical challenges, current best practice recommendations and beyond. Hum. Pathol. 2022, 132, 20–30. [Google Scholar] [CrossRef] [PubMed]
- Mandile, R.; Maglio, M.; Mosca, C.; Marano, A.; Discepolo, V.; Troncone, R.; Auricchio, R. Mucosal Healing in Celiac Disease: Villous Architecture and Immunohistochemical Features in Children on a Long-Term Gluten Free Diet. Nutrients 2022, 14, 3696. [Google Scholar] [CrossRef] [PubMed]
- Ascher, H.; Holm, K.; Kristiansson, B.; Maki, M. Different features of coeliac disease in two neighbouring countries. Arch. Dis. Child. 1993, 69, 375–380. [Google Scholar] [CrossRef] [PubMed]
- Rubio-Tapia, A.; Hill, I.D.; Kelly, C.P.; Calderwood, A.H.; Murray, J.A. American College of Gastroenterology ACG clinical guidelines: Diagnosis and management of celiac disease. Am. J. Gastroenterol. 2013, 108, 656–676. [Google Scholar] [CrossRef]
- Raiteri, A.; Granito, A.; Giamperoli, A.; Catenaro, T.; Negrini, G.; Tovoli, F. Current guidelines for the management of celiac disease: A systematic review with comparative analysis. WJG 2022, 28, 154–176. [Google Scholar] [CrossRef] [PubMed]
- Pantic, N.; Pantic, I.; Jevtic, D.; Mogulla, V.; Oluic, S.; Durdevic, M.; Nordin, T.; Jecmenica, M.; Milovanovic, T.; Gavrancic, T.; et al. Celiac Disease and Thrombotic Events: Systematic Review of Published Cases. Nutrients 2022, 14, 2162. [Google Scholar] [CrossRef] [PubMed]
- Cooke, W.T.; Smith, W.T. Neurological disorders associated with adult coeliac disease. Brain 1966, 89, 683–722. [Google Scholar] [CrossRef] [PubMed]
- Hadjivassiliou, M.; Grünewald, R.A.; Davies-Jones, G.A.B. Gluten sensitivity as a neurological illness. J. Neurol. Neurosurg. Psychiatry 2002, 72, 560–563. [Google Scholar] [CrossRef] [PubMed]
- Volta, U.; De Giorgio, R.; Granito, A.; Stanghellini, V.; Barbara, G.; Avoni, P.; Liguori, R.; Petrolini, N.; Fiorini, E.; Montagna, P.; et al. Anti-ganglioside antibodies in coeliac disease with neurological disorders. Dig. Liver Dis. 2006, 38, 183–187. [Google Scholar] [CrossRef] [PubMed]
- Cervio, E.; Volta, U.; Verri, M.; Boschi, F.; Pastoris, O.; Granito, A.; Barbara, G.; Parisi, C.; Felicani, C.; Tonini, M.; et al. Sera of Patients with Celiac Disease and Neurologic Disorders Evoke a Mitochondrial-Dependent Apoptosis In Vitro. Gastroenterology 2007, 133, 195–206. [Google Scholar] [CrossRef]
- Hu, W.T.; Murray, J.A.; Greenaway, M.C.; Parisi, J.E.; Josephs, K.A. Cognitive Impairment and Celiac Disease. Arch. Neurol. 2006, 63, 1440. [Google Scholar] [CrossRef]
- Casella, S.; Zanini, B.; Lanzarotto, F.; Ricci, C.; Marengoni, A.; Romanelli, G.; Lanzini, A. Cognitive performance is impaired in coeliac patients on gluten free diet: A case–control study in patients older than 65 years of age. Dig. Liver Dis. 2012, 44, 729–735. [Google Scholar] [CrossRef] [PubMed]
- Lichtwark, I.T.; Newnham, E.D.; Robinson, S.R.; Shepherd, S.J.; Hosking, P.; Gibson, P.R.; Yelland, G.W. Cognitive impairment in coeliac disease improves on a gluten-free diet and correlates with histological and serological indices of disease severity. Aliment. Pharmacol. Ther. 2014, 40, 160–170. [Google Scholar] [CrossRef] [PubMed]
- Longarini, G.; Richly, P.; Temprano, M.; Costa, A.F.; Vázquez, H.; Moreno, M.L.; Niveloni, S.; López, P.; Smecuol, E.; Mazure, R.; et al. A Prospective Study on Cognitive Impairment in Middle-aged Adults with Newly Diagnosed Celiac Disease. J. Clin. Gastroenterol. 2019, 53, 290–294. [Google Scholar] [CrossRef] [PubMed]
- Croall, I.D.; Tooth, C.; Venneri, A.; Poyser, C.; Sanders, D.S.; Hoggard, N.; Hadjivassiliou, M. Cognitive Impairment in Coeliac Disease with Respect to Disease Duration and Gluten-Free Diet Adherence: A Pilot Study. Nutrients 2020, 12, 2028. [Google Scholar] [CrossRef]
- Croall, I.D.; Sanders, D.S.; Hadjivassiliou, M.; Hoggard, N. Cognitive Deficit and White Matter Changes in Persons with Celiac Disease: A Population-Based Study. Gastroenterology 2020, 158, 2112–2122. [Google Scholar] [CrossRef]
- Fisicaro, F.; Lanza, G.; D’Agate, C.C.; Ferri, R.; Cantone, M.; Falzone, L.; Pennisi, G.; Bella, R.; Pennisi, M. Intracortical and Intercortical Motor Disinhibition to Transcranial Magnetic Stimulation in Newly Diagnosed Celiac Disease Patients. Nutrients 2021, 13, 1530. [Google Scholar] [CrossRef]
- Lanza, G.; Fisicaro, F.; D’Agate, C.C.; Ferri, R.; Cantone, M.; Falzone, L.; Pennisi, G.; Bella, R.; Hadjivassiliou, M.; Pennisi, M. Preserved central cholinergic functioning to transcranial magnetic stimulation in de novo patients with celiac disease. PLoS ONE 2021, 16, e0261373. [Google Scholar] [CrossRef] [PubMed]
- Edwards George, J.B.; Aideyan, B.; Yates, K.; Voorhees, K.N.; O’Flynn, J.; Sweet, K.; Avery, K.; Ehrlich, A.; Bast, A.; Leffler, D.A. Gluten-induced Neurocognitive Impairment: Results of a Nationwide Study. J. Clin. Gastroenterol. 2022, 56, 584–591. [Google Scholar] [CrossRef] [PubMed]
- Yelland, G.; Bruce, K.; Robinson, S.; Smith, J. Validity of a screening tool for detecting subtle cognitive impairment in the middle-aged and elderly. CIA 2014, 2014, 2165–2176. [Google Scholar] [CrossRef]
- Cardo, A.; Churruca, I.; Lasa, A.; Navarro, V.; Vázquez-Polo, M.; Perez-Junkera, G.; Larretxi, I. Nutritional Imbalances in Adult Celiac Patients Following a Gluten-Free Diet. Nutrients 2021, 13, 2877. [Google Scholar] [CrossRef] [PubMed]
- Hallert, C.; Grant, C.; Grehn, S.; Grännö, C.; Hultén, S.; Midhagen, G.; Ström, M.; Svensson, H.; Valdimarsson, T. Evidence of poor vitamin status in coeliac patients on a gluten-free diet for 10 years: Vitamin status in treated coeliac patients. Aliment. Pharmacol. Ther. 2002, 16, 1333–1339. [Google Scholar] [CrossRef]
- Smith, A.D.; Refsum, H.; Bottiglieri, T.; Fenech, M.; Hooshmand, B.; McCaddon, A.; Miller, J.W.; Rosenberg, I.H.; Obeid, R. Homocysteine and Dementia: An International Consensus Statement1. JAD 2018, 62, 561–570. [Google Scholar] [CrossRef]
- Zmijewski, M.A. Vitamin D and Human Health. IJMS 2019, 20, 145. [Google Scholar] [CrossRef]
- Fava, G.A.; Sonino, N. Psychosomatic Medicine: Emerging Trends and Perspectives. Psychother. Psychosom. 2000, 69, 184–197. [Google Scholar] [CrossRef]
- Porcelli, P.; Sonino, N. Fattori Psicologici Che Influenzano le Malattie: Una Nuova Classificazione per il DSM-5; Giovanni Fioriti: Roma, Italy, 2008; ISBN 978-88-87319-98-9. [Google Scholar]
- Fond, G.; Loundou, A.; Hamdani, N.; Boukouaci, W.; Dargel, A.; Oliveira, J.; Roger, M.; Tamouza, R.; Leboyer, M.; Boyer, L. Anxiety and depression comorbidities in irritable bowel syndrome (IBS): A systematic review and meta-analysis. Eur. Arch. Psychiatry Clin. Neurosci. 2014, 264, 651–660. [Google Scholar] [CrossRef]
- Rostami-Nejad, M.; Taraghikhah, N.; Ciacci, C.; Pourhoseingholi, M.A.; Barzegar, F.; Rezaei-Tavirani, M.; Aldulaimi, D.; Zali, M.R. Anxiety Symptoms in Adult Celiac Patients and the Effect of a Gluten-Free Diet: An Iranian Nationwide Study. Inflamm. Intest. Dis. 2020, 5, 42–47. [Google Scholar] [CrossRef]
- Mawdsley, J.E. Psychological stress in IBD: New insights into pathogenic and therapeutic implications. Gut 2005, 54, 1481–1491. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, S.M.; Gramling, S.E.; Mancini, T. The influence of life stress, personality, and learning history on illness behavior. J. Behav. Ther. Exp. Psychiatry 1994, 25, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Porcelli, P.; De Carne, M.; Todarello, O. Prediction of Treatment Outcome of Patients with Functional Gastrointestinal Disorders by the Diagnostic Criteria for Psychosomatic Research. Psychother. Psychosom. 2004, 73, 166–173. [Google Scholar] [CrossRef] [PubMed]

| (a) | ||||
| Characteristics of Articles/Studies | Number | % | ||
| Platform Publication: Journal (=6) | Nutrients | 2 | 28.6% | |
| PLOS ONE | 1 | 14.3% | ||
| Digestive and Liver Disease | 1 | 14.3% | ||
| Alimentary Pharmacology & Therapeutics | 1 | 14.3% | ||
| Journal of Clinical Gastroenterology | 1 | 14.3% | ||
| Gastroenterology | 1 | 14.3% | ||
| First Author’ Country | Italy | 3 | 42.8% | |
| UK | 2 | 28.6% | ||
| Australia | 1 | 14.3% | ||
| Argentina | 1 | 14.3% | ||
| Publication or posted date | May 2021 | 2 | 28.6% | |
| 2020 | 3 | 42.8% | ||
| July 2014 | 1 | 14.3% | ||
| September 2012 | 1 | 14.3% | ||
| (b) | ||||
| Characteristics of Articles/Studies | Main Topic | Secondary Topic | n° | % |
| Case control = 6 | Cognitive impairment = 6 | Emotional Features GFD Neuroimaging/TMS | 6/6 3/6 3/6 | 100% 50% 50% |
| Cohort study = 1 | Cognitive impairment = 1 | GFD Emotional Features | 1/1 1/1 | 100% 100% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caruso, A.; Di Giacomo, D. Cognitive Impairment in Celiac Disease Patients: Scoping Review Exploring Psychological Triggers in a Chronic Condition. Gastrointest. Disord. 2023, 5, 87-101. https://doi.org/10.3390/gidisord5010009
Caruso A, Di Giacomo D. Cognitive Impairment in Celiac Disease Patients: Scoping Review Exploring Psychological Triggers in a Chronic Condition. Gastrointestinal Disorders. 2023; 5(1):87-101. https://doi.org/10.3390/gidisord5010009
Chicago/Turabian StyleCaruso, Alberto, and Dina Di Giacomo. 2023. "Cognitive Impairment in Celiac Disease Patients: Scoping Review Exploring Psychological Triggers in a Chronic Condition" Gastrointestinal Disorders 5, no. 1: 87-101. https://doi.org/10.3390/gidisord5010009
APA StyleCaruso, A., & Di Giacomo, D. (2023). Cognitive Impairment in Celiac Disease Patients: Scoping Review Exploring Psychological Triggers in a Chronic Condition. Gastrointestinal Disorders, 5(1), 87-101. https://doi.org/10.3390/gidisord5010009