
Treatment of Leptomeningeal Disease with Tepotinib in a Patient with Lung Adenocarcinoma Harboring MET Exon 14 Skipping Mutation Presenting with Extensive Metastasis Involving Duodenum


{kind=link}
{kind=link}
Abstract
1. Introduction and Clinical Significance
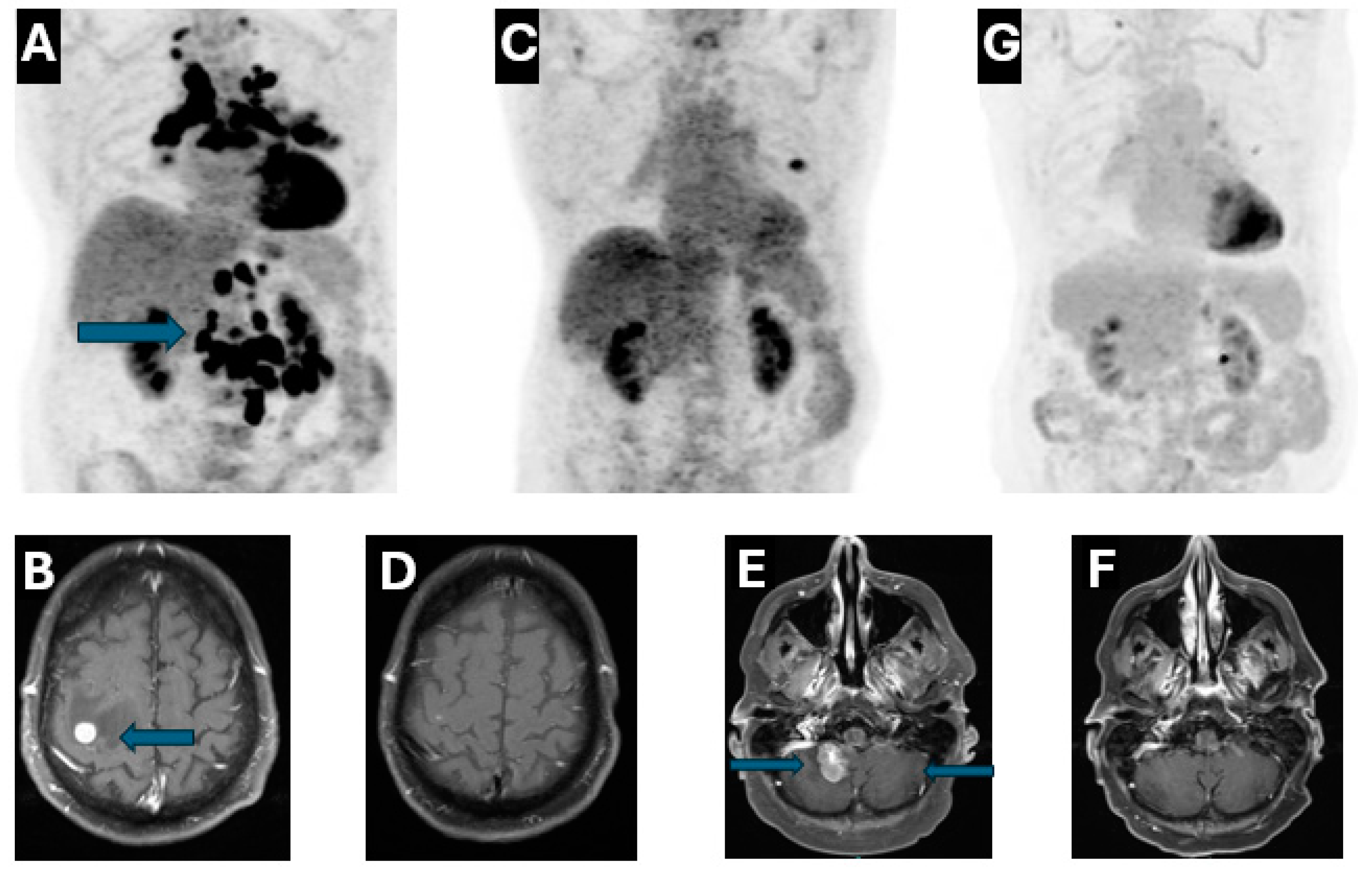
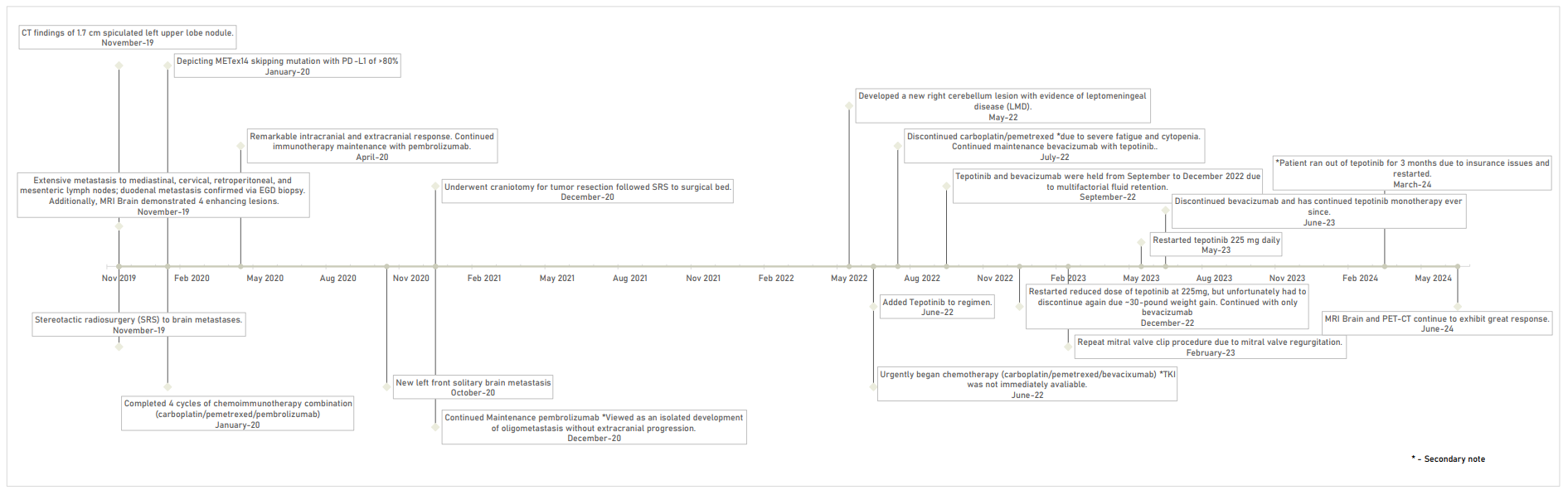
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| MET | Mesenchymal–epithelial transition |
| METex14 | Mesenchymal–epithelial transition exon 14 skipping mutation |
| NSCLC | Non-small cell lung cancer |
| TKIs | Tyrosine Kinase Inhibitors |
| LMD | Leptomeningeal Disease |
| ED | Emergency Department |
| CT | Computed Tomography |
| EGD | Esophagogastroduodenoscopy |
| PET | Positron Emission Tomography |
| MRI | Magnetic Resonance Imaging |
| NGS | Next-Generation Sequencing |
| PD-L1 | Programmed Death-Ligand 1 |
| BM | Brain Metastases |
| CNS | Central nervous system |
| EGFR | Epidermal Growth Factor Receptor |
References
- Socinski, M.A.; Pennell, N.A.; Davies, K.D. MET Exon 14 Skipping Mutations in Non–Small-Cell Lung Cancer: An Overview of Biology, Clinical Outcomes, and Testing Considerations. JCO Precis. Oncol. 2021, 5, 653–663. [Google Scholar] [CrossRef] [PubMed]
- Garassino, M.C.; Gadgeel, S.; Speranza, G.; Felip, E.; Esteban, E.; Dómine, M.; Hochmair, M.J.; Powell, S.F.; Bischoff, H.G.; Peled, N.; et al. Pembrolizumab Plus Pemetrexed and Platinum in Nonsquamous Non–Small-Cell Lung Cancer: 5-Year Outcomes From the Phase 3 KEYNOTE-189 Study. J. Clin. Oncol. 2023, 41, 1992–1998. [Google Scholar] [CrossRef] [PubMed]
- Reck, M.; Rodríguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csőszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Five-Year Outcomes with Pembrolizumab Versus Chemotherapy for Metastatic Non–Small-Cell Lung Cancer With PD-L1 Tumor Proportion Score ≥ 50%. J. Clin. Oncol. 2021, 39, 2339–2349. [Google Scholar] [CrossRef] [PubMed]
- Mazieres, J.; Paik, P.K.; Garassino, M.C.; Le, X.; Sakai, H.; Veillon, R.; Smit, E.F.; Cortot, A.B.; Raskin, J.; Viteri, S.; et al. Tepotinib Treatment in Patients with MET Exon 14–Skipping Non–Small Cell Lung Cancer: Long-term Follow-up of the VISION Phase 2 Nonrandomized Clinical Trial. JAMA Oncol. 2023, 9, 1260. [Google Scholar] [CrossRef]
- Rossi, G.; Marchioni, A.; Romagnani, E.; Bertolini, F.; Longo, L.; Cavazza, A.; Barbieri, F. Primary Lung Cancer Presenting with Gastrointestinal Tract Involvement: Clinicopathologic and Immunohistochemical Features in a Series of 18 Consecutive Cases. J. Thorac. Oncol. 2007, 2, 115–120. [Google Scholar] [CrossRef]
- Offin, M.; Luo, J.; Guo, R.; Lyo, J.K.; Falcon, C.; Dienstag, J.; Wilkins, O.; Chang, J.; Rudin, C.M.; Riely, G.; et al. CNS Metastases in Patients with MET Exon 14–Altered Lung Cancers and Outcomes with Crizotinib. JCO Precis. Oncol. 2020, 4, 871–876. [Google Scholar] [CrossRef]
- Neves, A.; Mendonça, I.; da Cunha Marques, J.A.; Costa, J.; Almeida, J.S.; Marques, J.A.D.C.; Almeida, J.S., Sr. Gastric Metastasis from Lung Adenocarcinoma: An Uncommon Presentation. Cureus, 2023; 15, Epub ahead of print. [Google Scholar] [CrossRef]
- Khasraw, M.; Yalamanchili, P.; Santhanagopal, A.; Wu, C.; Salas, M.; Meng, J.; Karnoub, M.; Esker, S.; Felip, E. Clinical Management of Patients with Non-Small Cell Lung Cancer, Brain Metastases, and Actionable Genomic Alterations: A Systematic Literature Review. Adv. Ther. 2024, 41, 1815–1842. [Google Scholar] [CrossRef]
- Ozcan, G.; Singh, M.; Vredenburgh, J.J. Leptomeningeal Metastasis from Non–Small Cell Lung Cancer and Current Landscape of Treatments. Clin. Cancer Res. 2023, 29, 11–29. [Google Scholar] [CrossRef]
- Pierret, T.; Giaj-Levra, N.; Toffart, A.-C.; Alongi, F.; Moro-Sibilot, D.; Gobbini, E. Immunotherapy in NSCLC Patients with Brain and Leptomeningeal Metastases. Front. Oncol. 2022, 12, 787080. [Google Scholar] [CrossRef]
- Catalano, M.; Marini, A.; Ferrari, K.; Voltolini, L.; Cianchi, F.; Comin, C.E.; Castiglione, M.; Roviello, G.; Mini, E. Gastric and colonic metastasis from NSCLC: A very unusual case report. Medicine 2022, 101, e28249. [Google Scholar] [CrossRef] [PubMed]
- Shih-Chun, C.; Shih-Chiang, H.; Chun-Yi, T.; Shan-Yu, W.; Keng-Hao, L.; Jun-Te, H.; Ta-Sen, Y.; Chun-Nan, Y. Non-small cell lung cancer with gastric metastasis and repeated gastrointestinal bleeding: A rare case report and literature review. Thorac. Cancer 2021, 12, 560–563. [Google Scholar] [CrossRef] [PubMed]
- Paik, P.K.; Felip, E.; Veillon, R.; Sakai, H.; Cortot, A.B.; Garassino, M.C.; Mazieres, J.; Viteri, S.; Senellart, H.; Van Meerbeeck, J.; et al. Tepotinib in Non–Small-Cell Lung Cancer with MET Exon 14 Skipping Mutations. N. Engl. J. Med. 2020, 383, 931–943. [Google Scholar] [CrossRef] [PubMed]
- Takamori, S.; Matsubara, T.; Fujishita, T.; Ito, K.; Toyozawa, R.; Seto, T.; Yamaguchi, M.; Okamoto, T. Dramatic intracranial response to tepotinib in a patient with lung adenocarcinoma harboring MET exon 14 skipping mutation. Thorac. Cancer 2021, 12, 978–980. [Google Scholar] [CrossRef]
- Chen, H.; Luo, Y.; Lin, M.; Chen, H.; Liu, M.; Wang, Y.; Li, S.; Yang, D.; Yang, Z. Clinical and pathological characteristics of 11 NSCLC patients with c-MET exon 14 skipping. Transl. Cancer Res. TCR 2022, 11, 880–887. [Google Scholar] [CrossRef]
- Ninomaru, T.; Okada, H.; Fujishima, M.; Irie, K.; Fukushima, S.; Hata, A. Lazarus Response to Tepotinib for Leptomeningeal Metastases in a Patient with MET Exon 14 Skipping Mutation–Positive Lung Adenocarcinoma: Case Report. JTO Clin. Res. Rep. 2021, 2, 100145. [Google Scholar] [CrossRef]
- Roth, K.G.; Mambetsariev, I.; Salgia, R. Prolonged survival and response to tepotinib in a non-small-cell lung cancer patient with brain metastases harboring MET exon 14 mutation: A research report. Cold Spring Harb. Mol. Case Stud. 2020, 6, a005785. [Google Scholar] [CrossRef]
- Yang, J.C.; Kim, S.-W.; Kim, D.-W.; Lee, J.-S.; Cho, B.C.; Ahn, J.-S.; Lee, D.H.; Kim, T.M.; Goldman, J.W.; Natale, R.B.; et al. Osimertinib in Patients with Epidermal Growth Factor Receptor Mutation–Positive Non–Small-Cell Lung Cancer and Leptomeningeal Metastases: The BLOOM Study. J. Clin. Oncol. 2020, 38, 538–547. [Google Scholar] [CrossRef]
- Garcia, J.; Hurwitz, H.I.; Sandler, A.B.; Miles, D.; Coleman, R.L.; Deurloo, R.; Chinot, O.L. Bevacizumab (Avastin®) in cancer treatment: A review of 15 years of clinical experience and future outlook. Cancer Treat. Rev. 2020, 86, 102017. [Google Scholar] [CrossRef]
- Friese-Hamim, M.; Clark, A.; Perrin, D.; Crowley, L.; Reusch, C.; Bogatyrova, O.; Zhang, H.; Crandall, T.; Lin, J.; Ma, J.; et al. Brain penetration and efficacy of tepotinib in orthotopic patient-derived xenograft models of MET-driven non-small cell lung cancer brain metastases. Lung Cancer 2022, 163, 77–86. [Google Scholar] [CrossRef]
- Passaro, A.; Wang, J.; Wang, Y.; Lee, S.-H.; Melosky, B.; Shih, J.-Y.; Azuma, K.; Juan-Vidal, O.; Cobo, M.; Felip, E.; et al. Amivantamab plus chemotherapy with and without lazertinib in EGFR-mutant advanced NSCLC after disease progression on osimertinib: Primary results from the phase III MARIPOSA-2 study. Ann. Oncol. 2024, 35, 77–90. [Google Scholar] [CrossRef] [PubMed]
- Planchard, D.; Jänne, P.A.; Cheng, Y.; Yang, J.C.-H.; Yanagitani, N.; Kim, S.-W.; Sugawara, S.; Yu, Y.; Fan, Y.; Geater, S.L.; et al. Osimertinib with or without Chemotherapy in EGFR -Mutated Advanced NSCLC. N. Engl. J. Med. 2023, 389, 1935–1948. [Google Scholar] [CrossRef] [PubMed]
- Nishio, M.; Kato, T.; Toyozawa, R.; Hida, T. Management of Peripheral Edema in Patients with MET Exon 14-Mutated Non-small Cell Lung Cancer Treated with Small Molecule MET Inhibitors. Targ. Oncol. 2022, 17, 597–604. [Google Scholar] [CrossRef]
- Chen, M.F.; Harada, G.; Liu, D.; DeMatteo, R.; Falcon, C.; Wilhelm, C.; Kris, M.G.; Drilon, A.; Gutgarts, V. Brief Report: Tyrosine Kinase Inhibitors for Lung Cancers That Inhibit MATE-1 Can Lead to “False” Decreases in Renal Function. J. Thorac. Oncol. 2024, 19, 153–159. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shugarts, J.; Amado, A.; Praska, T.; Camou, M.; Niu, J. Treatment of Leptomeningeal Disease with Tepotinib in a Patient with Lung Adenocarcinoma Harboring MET Exon 14 Skipping Mutation Presenting with Extensive Metastasis Involving Duodenum. Reports 2025, 8, 96. https://doi.org/10.3390/reports8020096
Shugarts J, Amado A, Praska T, Camou M, Niu J. Treatment of Leptomeningeal Disease with Tepotinib in a Patient with Lung Adenocarcinoma Harboring MET Exon 14 Skipping Mutation Presenting with Extensive Metastasis Involving Duodenum. Reports. 2025; 8(2):96. https://doi.org/10.3390/reports8020096
Chicago/Turabian StyleShugarts, Jacquelyn, Aida Amado, Taylor Praska, Monica Camou, and Jiaxin Niu. 2025. "Treatment of Leptomeningeal Disease with Tepotinib in a Patient with Lung Adenocarcinoma Harboring MET Exon 14 Skipping Mutation Presenting with Extensive Metastasis Involving Duodenum" Reports 8, no. 2: 96. https://doi.org/10.3390/reports8020096
APA StyleShugarts, J., Amado, A., Praska, T., Camou, M., & Niu, J. (2025). Treatment of Leptomeningeal Disease with Tepotinib in a Patient with Lung Adenocarcinoma Harboring MET Exon 14 Skipping Mutation Presenting with Extensive Metastasis Involving Duodenum. Reports, 8(2), 96. https://doi.org/10.3390/reports8020096