
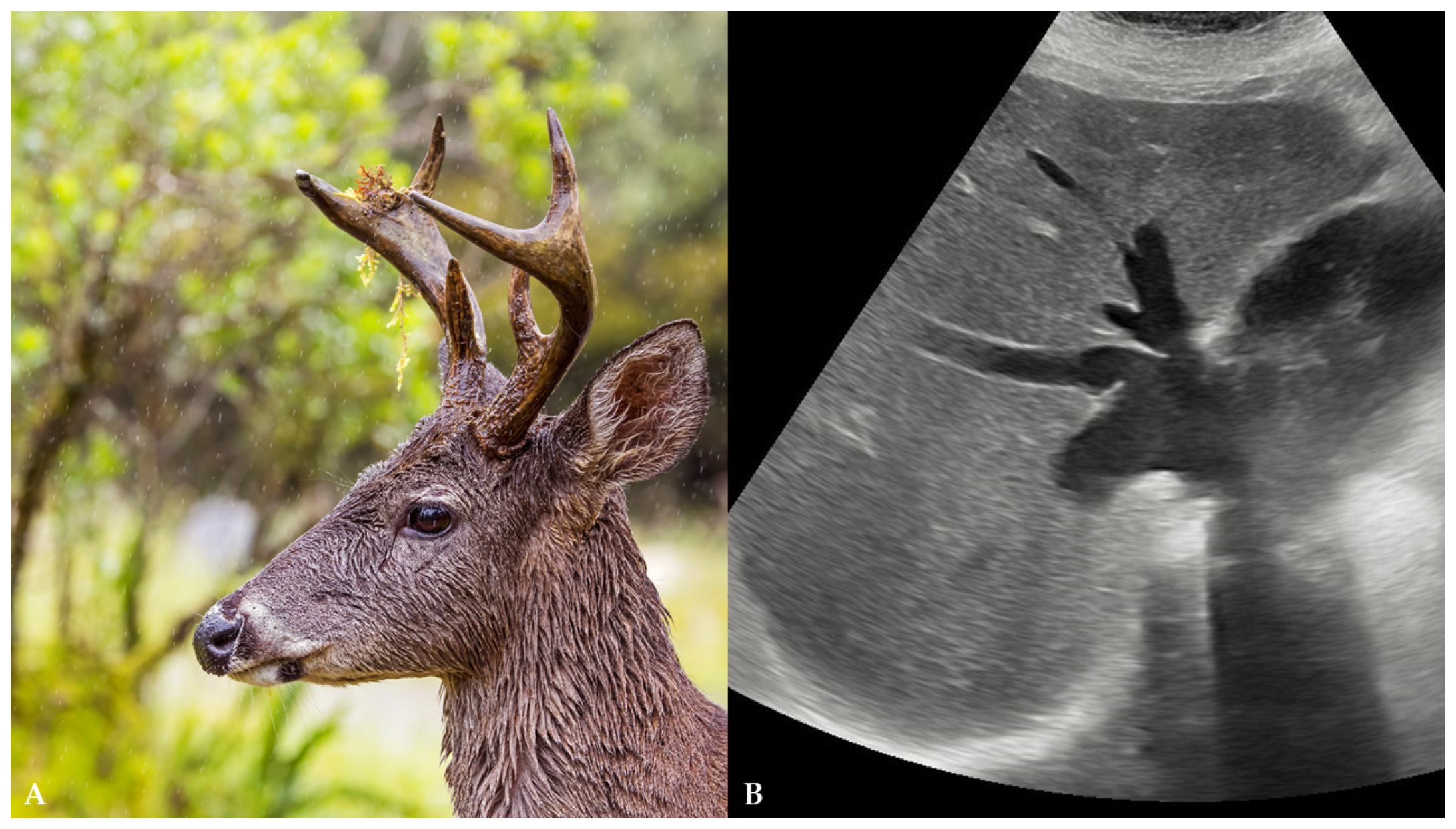
Deer Horn Sign in Congestive Hepatopathy Due to Heart Failure

 , , , ,
, , , ,
Abstract
1. Introduction and Clinical Significance
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ramanathan, S.; Sheikh, A. Playboy Bunny Sign. Abdom. Radiol. 2019, 44, 1938–1939. [Google Scholar] [CrossRef] [PubMed]
- Xiang, H.; Han, J.; Ridley, W.E.; Ridley, L.J. Playboy Bunny and Moose Head Sign: Hepatic Veins in Congestive Heart Failure. J. Med. Imag. Rad. Onc. 2018, 62, 99–100. [Google Scholar] [CrossRef] [PubMed]
- Hokama, A.; Arakaki, S.; Shibata, D.; Maeshiro, T.; Kinjo, F.; Fujita, J. “Playboy Bunny” Sign of Congestive Heart Failure. WestJEM 2011, 12, 433–434. [Google Scholar] [CrossRef] [PubMed]
- Akdemir, R.; Yildiz, A.; Bulur, S.; Kaya, A.; Bilir, C.; Uyan, C. Deer Horn Image in the Liver Associated with Giant Right Atrium. Am. J. Geriatr. Cardiol. 2007, 16, 200–201. [Google Scholar] [CrossRef] [PubMed]
- Vijay, J.; Naganur, S. Bunny Image and Deer Horn Sign in Heart Failure; A Clue Not to Miss! Heart Fail. J. India 2023, 1, 67. [Google Scholar] [CrossRef]
- Wells, M.L.; Venkatesh, S.K. Congestive hepatopathy. Abdom. Radiol. 2018, 43, 2037–2051. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Wang, C.; Dong, H.W.; Qi, J.; Rao, C.; Li, Q.; He, K. Inferior vena cava diameter in patients with chronic heart failure and chronic kidney disease: A retrospective study. Eur. J. Med. Res. 2025, 30, 30. [Google Scholar] [CrossRef] [PubMed]
- Brancatelli, G.; Vilgrain, V.; Federle, M.P.; Hakime, A.; Lagalla, R.; Iannaccone, R.; Valla, D. Budd-Chiari syndrome: Spectrum of imaging findings. AJR Am. J. Roentgenol. 2007, 188, W168–W176. [Google Scholar] [CrossRef] [PubMed]
- Chan, S.S.; Colecchia, A.; Duarte, R.F.; Bonifazi, F.; Ravaioli, F.; Bourhis, J.H. Imaging in Hepatic Veno-Occlusive Disease/Sinusoidal Obstruction Syndrome. Biol. Blood Marrow Transplant. 2020, 26, 1770–1779. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Blood Test | Value | Reference Value |
|---|---|---|
| Glucose | 8.3 | 4.4–6.4 mmol/L |
| AST | 89 | 11–34 U/L |
| ALT | 73 | 8–41 U/L |
| GGT | 42 | 9–35 U/L |
| Total bilirubin | 41 | 3–20 μmol/L |
| Creatinine | 110 | 49–90 μmol/L |
| Alfa-amylase | 112 | 23–91 U/L |
| Lipase | 118 | 13–60 U/L |
| CRP | 99 | <5 mg/L |
| NT-proBNP | 14235.8 | <125 ng/L |
| High-sensitivity troponin I | 22.1 | 15.6 ng/L for those older than 20 years of age |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferenc, T.; Matković, A.; Svetec, J.; Brkić, F.; Bratić, T.; Perić, V.; Vidjak, V. Deer Horn Sign in Congestive Hepatopathy Due to Heart Failure. Reports 2025, 8, 79. https://doi.org/10.3390/reports8020079
Ferenc T, Matković A, Svetec J, Brkić F, Bratić T, Perić V, Vidjak V. Deer Horn Sign in Congestive Hepatopathy Due to Heart Failure. Reports. 2025; 8(2):79. https://doi.org/10.3390/reports8020079
Chicago/Turabian StyleFerenc, Thomas, Andro Matković, Jelena Svetec, Filip Brkić, Tomica Bratić, Vitorio Perić, and Vinko Vidjak. 2025. "Deer Horn Sign in Congestive Hepatopathy Due to Heart Failure" Reports 8, no. 2: 79. https://doi.org/10.3390/reports8020079
APA StyleFerenc, T., Matković, A., Svetec, J., Brkić, F., Bratić, T., Perić, V., & Vidjak, V. (2025). Deer Horn Sign in Congestive Hepatopathy Due to Heart Failure. Reports, 8(2), 79. https://doi.org/10.3390/reports8020079