
Intersectional Differences in Health Care Outcomes among Patients with Musculoskeletal Disorders in Germany

Abstract
1. Introduction
2. Materials and Methods
2.1. Data
2.2. Variables
2.3. Analysis
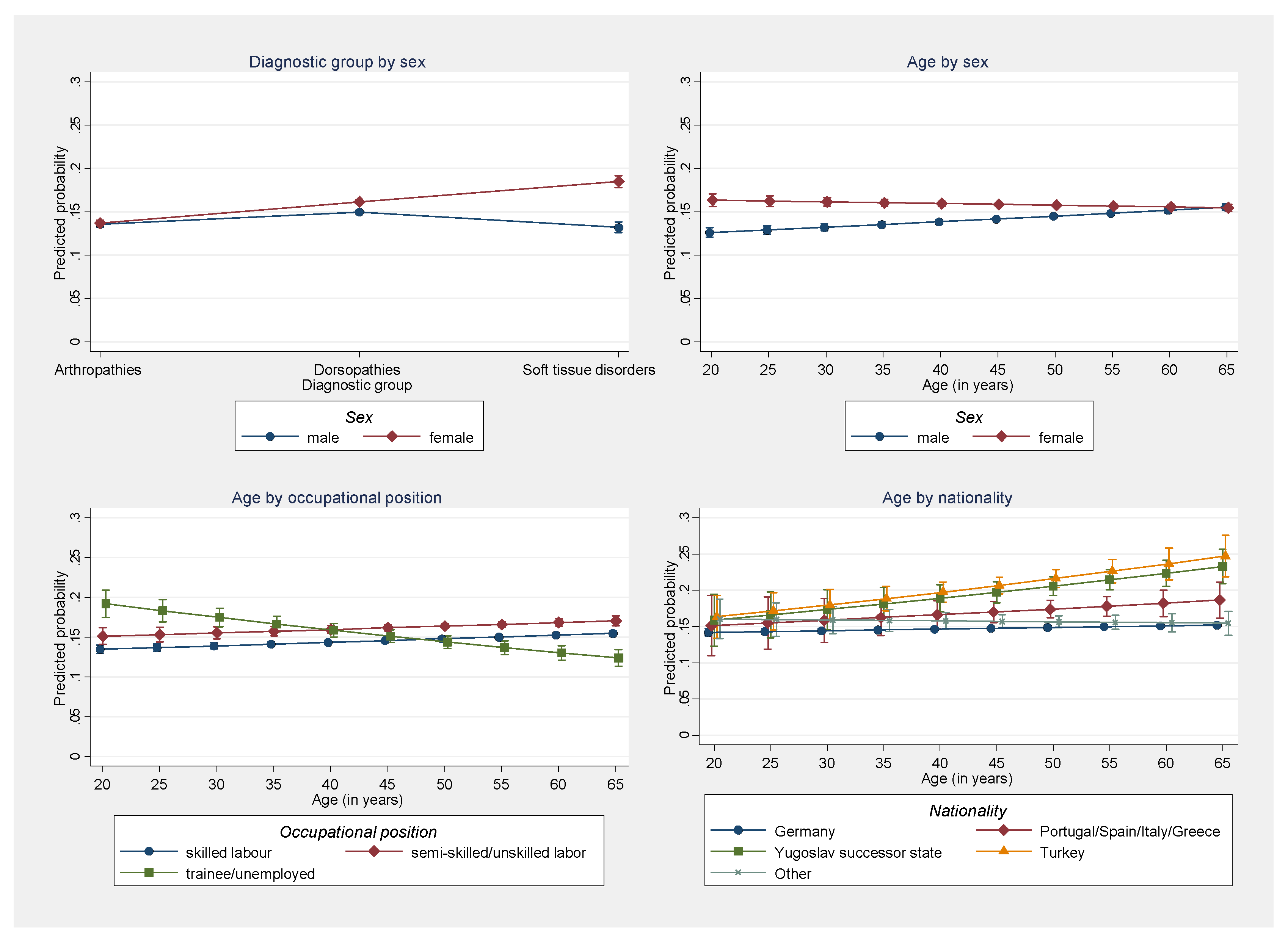
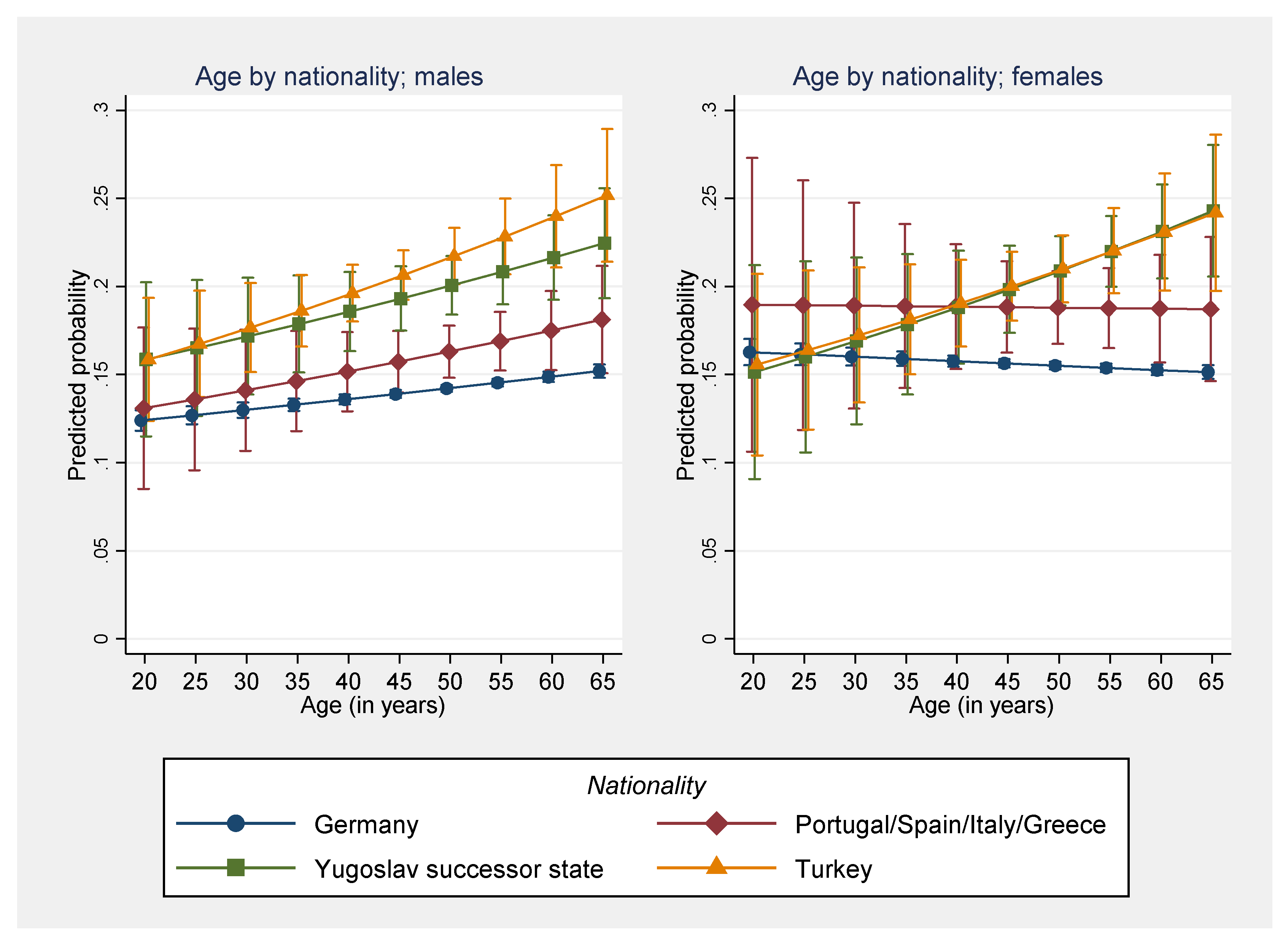
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hoy, D.G.; Smith, E.; Cross, M.; Sanchez-Riera, L.; Blyth, F.M.; Buchbinder, R.; Woolf, A.D.; Driscoll, T.; Brooks, P.; March, L.M. Reflecting on the global burden of musculoskeletal conditions: Lessons learnt from the global burden of disease 2010 study and the next steps forward. Ann. Rheum. Dis. 2015, 74, 4–7. [Google Scholar] [CrossRef]
- Palazzo, C.; Ravaud, J.F.; Papelard, A.; Ravaud, P.; Poiraudeau, S. The burden of musculoskeletal conditions. PLoS ONE 2014, 9, e90633. [Google Scholar] [CrossRef] [PubMed]
- Federal Statistical Office. Hospital Statistics—Diagnostic Data of the Hospital Patients (Fachserie 12 Reihe 6.2.1); Federal Statistical Office/Statistisches Bundesamt: Wiesbaden, Germany, 2019. [Google Scholar]
- Hammond, A. Rehabilitation in musculoskeletal diseases. Best Pract. Res. Clin. Rheumatol. 2008, 22, 435–449. [Google Scholar] [CrossRef] [PubMed]
- Goodman, S.M.; Parks, M.L.; McHugh, K.; Fields, K.; Smethurst, R.; Figgie, M.P.; Bass, A.R. Disparities in outcomes for African Americans and whites undergoing total knee arthroplasty: A systematic literature review. J. Rheumatol. 2016, 43, 765–770. [Google Scholar] [CrossRef]
- Brzoska, P.; Voigtländer, S.; Spallek, J.; Razum, O. Utilization and effectiveness of medical rehabilitation in foreign nationals residing in Germany. Eur. J. Epidemiol. 2010, 25, 651–660. [Google Scholar] [CrossRef] [PubMed]
- Kelly, U.A. Integrating intersectionality and biomedicine in health disparities research. Adv. Nurs. Sci. 2009, 32, E42–E56. [Google Scholar] [CrossRef] [PubMed]
- Pfannstiel, M.A. State of the Art von Maßnahmen und Instrumenten zum Management der Patienten- und Mitarbeiterdiversität im Krankenhaus. In Dienstleistungsmanagement im Krankenhaus II. Prozesse, Produktivität, Diversität; Bounken, R.B., Pfannstiel, M.A., Reutschl, A.J., Eds.; Springer Gabler: Wiesbaden, Germany, 2014; pp. 381–427. [Google Scholar]
- Truong, M.; Paradies, Y.; Priest, N. Interventions to improve cultural competency in healthcare: A systematic review of reviews. BMC Health Serv. Res. 2014, 14, 99. [Google Scholar] [CrossRef] [PubMed]
- Saha, S.; Beach, M.C.; Cooper, L.A. Patient centeredness, cultural competence and healthcare quality. J. Natl. Med. Assoc. 2008, 100, 1275–1285. [Google Scholar] [CrossRef]
- Brzoska, P.; Yilmaz-Aslan, Y. Trends in health care outcomes among patients with musculoskeletal disorders in Germany undergoing rehabilitation. An intersectionality perspective. In Proceedings of the 14th World Congress of the International Society of Physical and Rehabilitation Medicine, Orlando, FL, USA, 4–9 March 2020. [Google Scholar]
- Bengel, J.; Koch, U. Grundlagen der Rehabilitationswissenschaften: Themen, Strategien und Methoden der Rehabilitationsforschung; Springer: Berlin, Germany, 2000. [Google Scholar]
- Gerdes, N.; Zwingmann, C.; Jäckel, W.H. The system of rehabilitation Germany. In Research in Rehabilitation; Jäckel, W.H., Bengel, J., Herdt, J., Eds.; Schattauer: Stuttgart, Germany, 2006; pp. 3–19. [Google Scholar]
- Deutsche Rentenversicherung Bund. Der Ärztliche Reha-Entlassungsbericht. Leitfaden zum Einheitlichen Entlassungsbericht in der medizinischen Rehabilitation der Gesetzlichen Rentenversicherung 2007; Deutsche Rentenversicherung Bund: Berlin, Germany, 2007. [Google Scholar]
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics; Pearson: Boston, MA, USA, 2012. [Google Scholar]
- Colella, T.J.; Gravely, S.; Marzolini, S.; Grace, S.L.; Francis, J.A.; Oh, P.; Scott, L.B. Sex bias in referral of women to outpatient cardiac rehabilitation? A meta-analysis. Eur. J. Prev. Cardiol. 2015, 22, 423–441. [Google Scholar] [CrossRef]
- Colbert, J.D.; Martin, B.J.; Haykowsky, M.J.; Hauer, T.L.; Austford, L.D.; Arena, R.A.; Knudtson, M.L.; Meldrum, D.A.; Aggarwal, S.G.; Stone, J.A. Cardiac rehabilitation referral, attendance and mortality in women. Eur. J. Prev. Cardiol. 2015, 22, 979–986. [Google Scholar] [CrossRef]
- Cossette, S.; Maheu-Cadotte, M.A.; Mailhot, T.; Fontaine, G.; Cournoyer, A.; Cournoyer, C.; Guertin, M.C.; Juneau, M. Sex-and gender-related factors associated with cardiac rehabilitation enrollment: A secondary analysis among systematically referred patients. J. Cardiopulm. Rehabil. Prev. 2019, 39, 259–265. [Google Scholar] [CrossRef]
- Supervía, M.; Medina-Inojosa, J.R.; Yeung, C.; Lopez-Jimenez, F.; Squires, R.W.; Pérez-Terzic, C.M.; Brewer, L.C.; Leth, S.E.; Thomas, R.J. Cardiac rehabilitation for women: A systematic review of barriers and solutions. Mayo Clin. Proc. 2017, 92, 565–577. [Google Scholar] [CrossRef]
- Gary, K.W.; Arango-Lasprilla, J.C.; Stevens, L.F. Do racial/ethnic differences exist in post-injury outcomes after TBI? A comprehensive review of the literature. Brain Inj. 2009, 23, 775–789. [Google Scholar] [CrossRef] [PubMed]
- Flores, L.E.; Verduzco-Gutierrez, M.; Molinares, D.; Silver, J.K. Disparities in health care for Hispanic patients in physical medicine and rehabilitation in the United States: A narrative review. Am. J. Phys. Med. Rehabil. 2020, 99, 338–347. [Google Scholar] [CrossRef]
- Castellanos, L.R.; Viramontes, O.; Bains, N.K.; Zepeda, I.A. Disparities in cardiac rehabilitation among individuals from racial and ethnic groups and rural communities—A systematic review. J. Racial Ethn. Health Disparities 2019, 6, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Resurrección, D.M.; Moreno-Peral, P.; Gomez-Herranz, M.; Rubio-Valera, M.; Pastor, L.; Caldas de Almeida, J.M.; Motrico, E. Factors associated with non-participation in and dropout from cardiac rehabilitation programmes: A systematic review of prospective cohort studies. Eur. J. Cardiovasc. Nurs. 2019, 18, 38–47. [Google Scholar] [CrossRef] [PubMed]
- Brzoska, P.; Sauzet, O.; Yilmaz-Aslan, Y.; Widera, T.; Razum, O. Satisfaction with rehabilitative health care services among German and non-German nationals residing in Germany: A cross-sectional study. BMJ Open 2017, 7, e015520. [Google Scholar] [CrossRef] [PubMed]
- Brzoska, P. Disparities in health care outcomes between immigrants and the majority population in Germany: A trend analysis, 2006–2014. PLoS ONE 2018, 13, e0191732. [Google Scholar] [CrossRef]
- Handtke, O.; Schilgen, B.; Mösko, M. Culturally competent healthcare—A scoping review of strategies implemented in healthcare organizations and a model of culturally competent healthcare provision. PLoS ONE 2019, 14, e0219971. [Google Scholar] [CrossRef] [PubMed]
- Berens, E.M.; Vogt, D.; Messer, M.; Hurrelmann, K.; Schaeffer, D. Health literacy among different age groups in Germany: Results of a cross-sectional survey. BMC Public Health 2016, 16, 1151. [Google Scholar] [CrossRef]
- Yilmaz-Aslan, Y.; Brzoska, P.; Bluhm, M.; Aslan, A.; Razum, O. Illness perceptions in Turkish migrants with diabetes: A qualitative study. Chronic Illn. 2014, 10, 107–121. [Google Scholar] [CrossRef]
- Schultz, W.M.; Kelli, H.M.; Lisko, J.C.; Varghese, T.; Shen, J.; Sandesara, P.; Quyyumi, A.A.; Taylor, H.A.; Gulati, M.; Harold, J.G.; et al. Socioeconomic status and cardiovascular outcomes: Challenges and interventions. Circulation 2018, 137, 2166–2178. [Google Scholar] [CrossRef] [PubMed]
- Kangovi, S.; Barg, F.K.; Carter, T.; Levy, K.; Sellman, J.; Long, J.A.; Grande, D. Challenges faced by patients with low socioeconomic status during the post-hospital transition. J. Gen. Intern. Med. 2014, 29, 283–289. [Google Scholar] [CrossRef] [PubMed]
- de Melo Ghisi, G.L.; da Silva Chaves, G.S.L.; Britto, R.R.; Oh, P. Health literacy and coronary artery disease: A systematic review. Patient Educ. Couns. 2018, 101, 177–184. [Google Scholar] [CrossRef]
- Weber, L.; Zambrana, R.E.; Fore, M.E.; Parra-Medina, D. Racial and ethnic health inequities: An intersectional approach. In Handbook of the Sociology of Racial and Ethnic Relations; Springer: Berlin/Heidelberg, Germany, 2018; pp. 133–160. [Google Scholar]
- Koehn, S.; Neysmith, S.; Kobayashi, K.; Khamisa, H. Revealing the shape of knowledge using an intersectionality lens: Results of a scoping review on the health and health care of ethnocultural minority older adults. Ageing Soc. 2013, 33, 437–464. [Google Scholar] [CrossRef]
- Erdsiek, F.; Aksakal, T.; Mader, M.; Idris, M.; Yılmaz-Aslan, Y.; Razum, O.; Brzoska, P. Diversity-sensitive measures in German hospitals—Attitudes, implementation, and barriers according to administration managers. BMC Health Serv. Res. 2022, 22, 689. [Google Scholar] [CrossRef]
- Aksakal, T.; Erdsiek, F.; Yılmaz-Aslan, Y.; Mader, M.; Padberg, D.; Razum, O.; Brzoska, P. Umsetzungsstrategien einer diversitätssensiblen Gesundheitsversorgung und Unternehmensführung—Eine bundesweite postalische Befragung von Rehabilitationseinrichtungen. Die Rehabil. 2022, 62, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Aksakal, T.; Mader, M.; Annac, K.; Erdsiek, F.; Korn, M.; Padberg, D.; Idris, M.; Yilmaz-Aslan, Y.; Razum, O.; Brzoska, P. Entwicklung eines Instrumentenkatalogs und Handlungsleitfadens für Rehabilitationseinrichtungen und Rehabilitationsträger zur Umsetzung einer diversitätssensiblen Versorgung (DiversityKAT). Abschlussbericht. Universität Witten/Herdecke sowie Universität Bielefeld. 2021. Available online: https://www.deutsche-rentenversicherung.de/SharedDocs/Downloads/DE/Experten/reha_forschung/forschungsprojekte/abschlussbericht_diversitykat.pdf (accessed on 26 April 2023).
- Latham, C.L.; Hogan, M.; Ringl, K. Nurses supporting nurses: Creating a mentoring program for staff nurses to improve the workforce environment. Nurs. Adm. Q. 2008, 32, 27–39. [Google Scholar] [CrossRef] [PubMed]
- Hayward, L.M.; Canali, A.; Hill, A. Interdisciplinary peer mentoring: A model for developing culturally competent health care professionals. J. Phys. Ther. Educ. 2005, 19, 28–40. [Google Scholar] [CrossRef]
- Statistisches Bundesamt. Bevölkerung und Erwerbstätigkeit. Bevölkerung mit Migrationshintergrund. Ergebnisse des Mikrozensus 2021 (Fachserie 1 Reihe 2.2); Statistisches Bundesamt: Wiesbaden, Germany, 2022. [Google Scholar]



{kind=link}
{kind=link}
| Improvement in Health Condition after Rehabilitation (n, %) | Total | p-Value | ||
|---|---|---|---|---|
| Yes | No | |||
| Sex (n, %) | <0.01 | |||
| Male | 129,345 (51.0%) | 22,392 (49.7%) | 151,737 (50.8%) | |
| Female | 124,213 (49.0%) | 22,667 (50.3%) | 146,880 (49.2%) | |
| Age (mean, sd) | 50.3 (8.8) | 50.2 (8.8) | 50.3 (8.8) | <0.01 |
| Nationality (n, %) | <0.01 | |||
| Germany | 238,324 (94.0%) | 41,348 (91.8%) | 279,672 (93.7%) | |
| Portugal/Spain/Italy/Greece | 2931 (1.2%) | 649 (1.4%) | 3580 (1.2%) | |
| Yugoslav successor state | 3022 (1.2%) | 826 (1.8%) | 3848 (1.3%) | |
| Turkey | 3369 (1.3%) | 1080 (2.4%) | 4449 (1.5%) | |
| Other | 5912 (2.3%) | 1156 (2.6%) | 7068 (2.4%) | |
| Occupational position (n, %) | <0.01 | |||
| Skilled labor | 191,032 (75.3%) | 32,128 (71.3%) | 223,160 (74.7%) | |
| Semi-skilled/unskilled labor | 46,228 (18.2%) | 10,179 (22.6%) | 56,407 (18.9%) | |
| Trainee/unemployed | 16,298 (6.4%) | 2752 (6.1%) | 19,050 (6.4%) | |
| Type of employment (n, %) | <0.01 | |||
| Fulltime | 174,270 (68.7%) | 29,691 (65.9%) | 203,961 (68.3%) | |
| Part-time | 43,267 (17.1%) | 7883 (17.5%) | 51,150 (17.1%) | |
| Unemployed | 16,046 (6.3%) | 4201 (9.3%) | 20,247 (6.8%) | |
| Other | 19,975 (7.9%) | 3284 (7.3%) | 23,259 (7.8%) | |
| Occupation (n, %) | <0.01 | |||
| Manual | 76,993 (30.4%) | 14,299 (31.7%) | 91,292 (30.6%) | |
| Services | 59,649 (23.5%) | 11,437 (25.4%) | 71,086 (23.8%) | |
| Technical/professional | 38,746 (15.3%) | 6495 (14.4%) | 45,241 (15.2%) | |
| Administrative | 40,963 (16.2%) | 6922 (15.4%) | 47,885 (16.0%) | |
| Other | 37,207 (14.7%) | 5906 (13.1%) | 43,113 (14.4%) | |
| Diagnosis (n, %) | <0.01 | |||
| Arthropathies | 62,033 (24.5%) | 9823 (21.8%) | 71,856 (24.1%) | |
| Dorsopathies | 173,488 (68.4%) | 31,354 (69.6%) | 204,842 (68.6%) | |
| Soft tissue disorders | 18,037 (7.1%) | 3882 (8.6%) | 21,919 (7.3%) | |
| Marital status (n, %) | <0.01 | |||
| Not married | 74,411 (29.3%) | 14,157 (31.4%) | 88,568 (29.7%) | |
| Married | 175,055 (69.0%) | 30,183 (67.0%) | 205,238 (68.7%) | |
| Other | 4092 (1.6%) | 719 (1.6%) | 4811 (1.6%) | |
| Time absent from work in the last 12 months (n, %) | <0.01 | |||
| None | 37,724 (14.9%) | 5675 (12.6%) | 43,399 (14.5%) | |
| <3 months | 141,324 (55.7%) | 17,990 (39.9%) | 159,314 (53.4%) | |
| 3–6 months | 37,581 (14.8%) | 8704 (19.3%) | 46,285 (15.5%) | |
| 6+ months | 28,893 (11.4%) | 11,460 (25.4%) | 40,353 (13.5%) | |
| Not employed | 8036 (3.2%) | 1230 (2.7%) | 9266 (3.1%) | |
| Independent Variable 1 | aOR 2 | 95%-CI | aAME 2 | 95%-CI | ||
|---|---|---|---|---|---|---|
| Sex (Ref.: Male) | ||||||
| Female | 1.11 | 1.08 | 1.13 | 0.012 | 0.009 | 0.016 |
| Age (in years) | 1.002 | 1.001 | 1.003 | 0.0003 | 0.0001 | 0.0004 |
| Nationality (Ref.: Germany) | ||||||
| Portugal/Spain/Italy/Greece | 1.22 | 1.12 | 1.33 | 0.026 | 0.014 | 0.038 |
| Yugoslav successor state | 1.53 | 1.41 | 1.65 | 0.059 | 0.046 | 0.072 |
| Turkey | 1.56 | 1.45 | 1.68 | 0.062 | 0.051 | 0.074 |
| Other | 1.07 | 1.00 | 1.14 | 0.008 | 0.000 | 0.017 |
| Occupational position (Ref: Skilled labor) | ||||||
| Semi-skilled/unskilled labor | 1.13 | 1.10 | 1.17 | 0.016 | 0.013 | 0.020 |
| Trainee/unemployed | 1.03 | 0.96 | 1.10 | 0.003 | −0.005 | 0.012 |
| Type of employment (Ref.: Full time) | ||||||
| Part-time | 1.04 | 1.01 | 1.08 | 0.005 | 0.001 | 0.009 |
| Unemployed | 1.30 | 1.25 | 1.35 | 0.034 | 0.029 | 0.040 |
| Other | 1.01 | 0.95 | 1.07 | 0.001 | −0.006 | 0.008 |
| Occupation (Ref.: Manufacturing) | ||||||
| Services | 1.00 | 0.97 | 1.03 | 0.000 | −0.004 | 0.003 |
| Technical/professional | 0.96 | 0.93 | 1.00 | −0.004 | −0.009 | 0.000 |
| Administrative | 0.96 | 0.93 | 1.00 | −0.005 | −0.009 | 0.000 |
| Other | 0.92 | 0.89 | 0.96 | −0.010 | −0.014 | −0.006 |
| Diagnosis (Ref: Skeletal system) | ||||||
| Dorsopathies | 1.17 | 1.14 | 1.20 | 0.019 | 0.016 | 0.022 |
| Soft tissue disorders | 1.20 | 1.15 | 1.25 | 0.022 | 0.017 | 0.027 |
| Significant interaction effects (p < 0.05) | ||||||
| Sex by diagnostic group | ||||||
| Arthropathies, female vs. male | 0.0000 | −0.0042 | 0.0061 | |||
| Dorsopathies, female vs. male | 0.0110 | 0.0084 | 0.0155 | |||
| Soft tissue, female vs. male | 0.0530 | 0.0438 | 0.0623 | |||
| Age by sex | ||||||
| Male, age | 0.0010 | 0.0005 | 0.0008 | |||
| Female, age | −0.0002 | −0.0004 | 0.00003 | |||
| Age by occupational group | ||||||
| Skilled labor, age | 0.0005 | 0.0003 | 0.0006 | |||
| Semi-skilled/unskilled labor, age | 0.0004 | 0.0001 | 0.0008 | |||
| Trainee/unemployed, age | −0.0014 | −0.0019 | −0.0010 | |||
| Age by nationality | ||||||
| Germany, age | 0.0002 | 0.0001 | 0.0004 | |||
| Portugal/Spain/Italy/Greece, age | 0.0008 | −0.0006 | 0.0022 | |||
| Yugoslav successor state, age | 0.0017 | 0.0004 | 0.0030 | |||
| Turkey, age | 0.0020 | 0.0006 | 0.0033 | |||
| Other, age | −0.0001 | −0.0010 | 0.0008 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brzoska, P.; Annac, K.; Yilmaz-Aslan, Y. Intersectional Differences in Health Care Outcomes among Patients with Musculoskeletal Disorders in Germany. Reports 2023, 6, 20. https://doi.org/10.3390/reports6020020
Brzoska P, Annac K, Yilmaz-Aslan Y. Intersectional Differences in Health Care Outcomes among Patients with Musculoskeletal Disorders in Germany. Reports. 2023; 6(2):20. https://doi.org/10.3390/reports6020020
Chicago/Turabian StyleBrzoska, Patrick, Kübra Annac, and Yüce Yilmaz-Aslan. 2023. "Intersectional Differences in Health Care Outcomes among Patients with Musculoskeletal Disorders in Germany" Reports 6, no. 2: 20. https://doi.org/10.3390/reports6020020
APA StyleBrzoska, P., Annac, K., & Yilmaz-Aslan, Y. (2023). Intersectional Differences in Health Care Outcomes among Patients with Musculoskeletal Disorders in Germany. Reports, 6(2), 20. https://doi.org/10.3390/reports6020020