
Cross-Cultural Adaptation and Psychometric Properties of the Traditional Chinese Version of the Italian Spine Youth Quality of Life (ISYQOL) Questionnaire

 ,
,  , ,
, ,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Phase 1: Translation and Cross-Cultural Adaptation of Questionnaire
2.4. Phase 2: Evaluations of Psychometric Properties of the ISYQOL-TC
2.4.1. ISYQOL
2.4.2. Chinese Version of SRS-22r
2.4.3. Other Chinese Questionnaires
2.5. Data Analysis
2.5.1. Semantic Equivalence Score
2.5.2. Content Validity Index (CVI)
2.5.3. Psychometric Property Analysis
Internal Consistency
Test–Retest Reliability
Standard Error of Measurement (SEM) and 95% Confidence Minimal Detectable Change (MDC95)
Structural Validity
Convergent and Divergent Validity
3. Results
3.1. Demographics and Clinical Data
3.2. Semantic Equivalence and Content Equivalence
3.3. Cognitive Debriefing Interviews
3.4. Internal Consistency and Test–Retest Reliability
3.5. SEM and MDC95
3.6. Ceiling Effect
3.7. Structural Validity
3.8. Construct Validity
4. Discussion
4.1. Good Internal Consistency, Test–Retest Reliability, and Unidimensionality
4.2. Comparisons with SRS22r and Other Questionnaires
4.3. Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
 | |
 | |
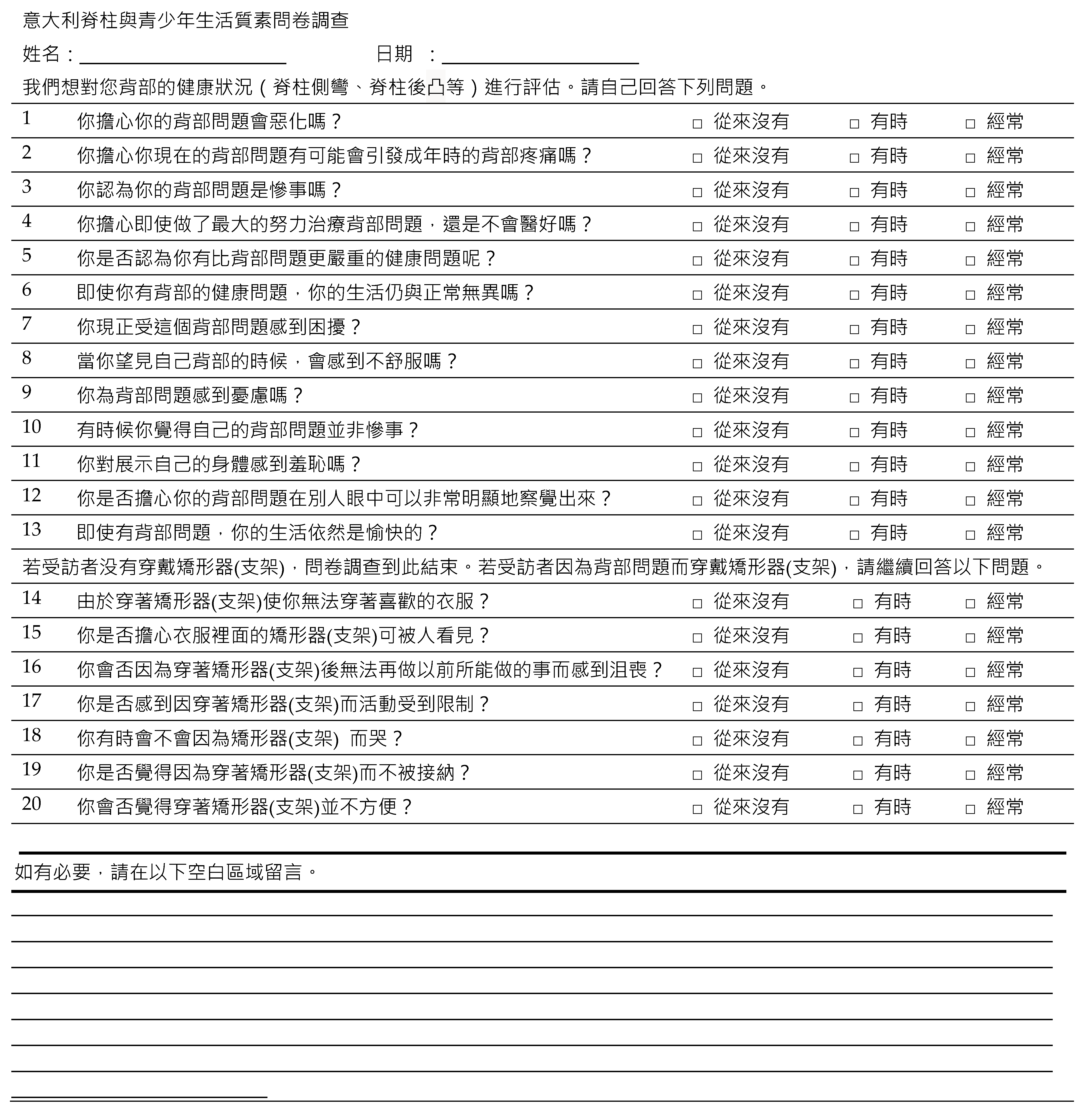
| Spine Youth Quality of Life (SYQOL) Measuring Spine Related Quality of Life | |
| We want to evaluate your well-being with regards to your back problem (scoliosis, kyphosis or something else). Try to answer all of the following questions yourself. | |
| 1. Are you afraid that your back problem may get worse? | never |
| sometimes | |
| often | |
| 2. Are you worried about having back pain as an adult because of your back problem? | never |
| sometimes | |
| often | |
| 3. Do you feel that having your back problem is a big deal? | never |
| sometimes | |
| often | |
| 4. Are you worried that, despite all your efforts to treat your back, it will not get better? | never |
| sometimes | |
| often | |
| 5. Do you think that there are other health conditions affecting other people that are more serious than your back problem? | never |
| sometimes | |
| often | |
| 6. Despite your back problem, do you think you lead a normal life? | never |
| sometimes | |
| often | |
| 7. Are you suffering because of your back problem? | never |
| sometimes | |
| often | |
| 8. Does the appearance of your back make you feel uncomfortable? | never |
| sometimes | |
| often | |
| 9. Are you worried about your back problem? | never |
| sometimes | |
| often | |
| 10. Do you think that your back problem is not a big concern to you? | never |
| sometimes | |
| often | |
| 11. Does it bother you to show your physical appearance? | never |
| sometimes | |
| often | |
| 12. Are you worried that your back problem is very visible? | never |
| sometimes | |
| often | |
| 13. Despite your back problem, do you live a happy life? | never |
| sometimes | |
| often | |
| Do you wear a brace because of your back problem? | Yes |
| No | |
| 14. Do you have to change the way that you dress because of your brace? | never |
| sometimes | |
| often | |
| 15. Are you worried that the brace is visible under your clothing? | never |
| sometimes | |
| often | |
| 16. Do you feel sad that you are unable to do some of the things that you used to do before you started wearing your brace? | never |
| sometimes | |
| often | |
| 17. Do you feel your movements are restricted while wearing your brace? | never |
| sometimes | |
| often | |
| 18. Does wearing your brace ever make you cry? | never |
| sometimes | |
| often | |
| 19. Do you feel excluded by others because you wear your brace? | never |
| sometimes | |
| often | |
| 20. Is wearing your brace uncomfortable? | never |
| sometimes | |
| often | |
| If you would like, use this space to leave a comment. __________________________________ | |
| Instructions | |
| When adding items’ scores to obtain the ISYQOL total score, it is important to remember that items’ categories are to be coded so that lower the category, more the quality of life. Thus, items investigating the presence of spine-related problems (white items) are coded 0-1-2 (0: never; 1: sometimes; 2: often). Conversely, items investigating the presence of positive thoughts (grey items) are coded 2-1-0 (2: never; 1: sometimes; 0: often). | |
| Name of Questionnaire | Number of Items | Scoring | Interpretation | Psychometric Properties |
|---|---|---|---|---|
| PHQ-9 [28,29,63,64,65] | 9 | 4-point Likert scale 0 = Not at all 1 = Several days 2 = > half the days 3 = Nearly every day Maximum score: 27 Cut-off scores: 5 (mild), 10 (moderate), 15 (severe) anxiety | Higher score indicates more severe anxiety | Cronbach’s alpha = 0.84 ICC = 0.80 |
| GAD-7 [29,66] | 7 | 4-point Likert scale 0 = Not at all 1 = Several days 2 = > half the days 3 = Nearly every day Maximum score: 21 Cut-off scores: 5 (mild), 10 (moderate), 15 (severe) anxiety | Higher score indicates more severe anxiety | Cronbach’s alpha = 0.93 ICC= 0.71–0.87 |
| MAS [30,31,67] | 7 | 5-point Likert scale, 0 (strongly agree) to 4 (strongly disagree) Maximum score: 28 | Higher scores indicate higher levels of mastery | McDonald’s ω = 0.82 CFI = 0.97 |
| NPRS [68] | 1 | 0 (no pain) to 10 (the worst imaginable pain) Maximum score: 10 | Higher score indicates more painful | Convergent Validity: Faces Pain Scale-Revised (r = 0.75 to 0.93) The visual analogue scale (r = 0.73 to 0.95) The Verbal Rating Scale (r = 0.48 to 0.79) |
| SCSQ [32,33,69,70,71,72] | 20 Active coping:12 Passive coping: 8 | 4-point Likert scale 0 = never 1 = seldom 2 = sometimes 3 = often Maximum score: 60 | Higher scores mean a higher tendency for participant to adopt the corresponding coping style | Cronbach’s alpha > 0.78 |
| ISYQOL-TC Domains | Item | Panel Expert 1 | Panel Expert 2 | Panel Expert 3 | |||
|---|---|---|---|---|---|---|---|
| Semantic Equivalence Score | Content Validity Index | Semantic Equivalence Score | Content Validity Index | Semantic Equivalence Score | Content Validity Index | ||
| Spine health | 1 | 4 | 4 | 4 | 4 | 4 | 4 |
| 2 | 4 | 4 | 4 | 4 | 4 | 4 | |
| 3 | 4 | 4 | 4 | 4 | 4 | 4 | |
| 4 | 4 | 4 | 4 | 4 | 4 | 4 | |
| 5 | 4 | 4 | 3 | 3 | 4 | 4 | |
| 6 | 4 | 4 | 4 | 4 | 4 | 4 | |
| 7 | 4 | 4 | 4 | 4 | 4 | 4 | |
| 8 | 4 | 4 | 4 | 4 | 4 | 4 | |
| 9 | 4 | 4 | 4 | 4 | 4 | 4 | |
| 10 | 4 | 4 | 4 | 4 | 4 | 4 | |
| 11 | 4 | 4 | 4 | 4 | 4 | 4 | |
| 12 | 4 | 4 | 4 | 4 | 4 | 4 | |
| 13 | 4 | 4 | 4 | 4 | 4 | 4 | |
| Brace | 14 | 4 | 4 | 4 | 4 | 4 | 4 |
| 15 | 4 | 4 | 4 | 4 | 4 | 4 | |
| 16 | 4 | 4 | 4 | 4 | 4 | 4 | |
| 17 | 4 | 4 | 4 | 4 | 4 | 4 | |
| 18 | 4 | 4 | 4 | 4 | 4 | 4 | |
| 19 | 4 | 4 | 4 | 4 | 4 | 4 | |
| 20 | 4 | 4 | 4 | 4 | 4 | 4 | |
| Overall Cronbach’s Alpha | Cronbach’s Alpha if Item Deleted | Item-Total Correlation | |
|---|---|---|---|
| Question 1 | 0.90 | 0.88 | 0.59 |
| Question 2 | 0.88 | 0.60 | |
| Question 3 | 0.87 | 0.66 | |
| Question 4 | 0.88 | 0.58 | |
| Question 5 | 0.88 | 0.52 | |
| Question 6 | 0.88 | 0.47 | |
| Question 7 | 0.87 | 0.70 | |
| Question 8 | 0.87 | 0.63 | |
| Question 9 | 0.87 | 0.70 | |
| Question 10 | 0.88 | 0.51 | |
| Question 11 | 0.88 | 0.51 | |
| Question 12 | 0.88 | 0.56 | |
| Question 13 | 0.88 | 0.47 |
| Overall Cronbach’s Alpha | Cronbach’s Alpha if Item Deleted | Item-Total Correlation | |
|---|---|---|---|
| Question 1 | 0.89 | 0.89 | 0.55 |
| Question 2 | 0.89 | 0.56 | |
| Question 3 | 0.89 | 0.68 | |
| Question 4 | 0.89 | 0.60 | |
| Question 5 | 0.89 | 0.62 | |
| Question 6 | 0.90 | 0.50 | |
| Question 7 | 0.89 | 0.73 | |
| Question 8 | 0.89 | 0.65 | |
| Question 9 | 0.88 | 0.76 | |
| Question 10 | 0.90 | 0.53 | |
| Question 11 | 0.90 | 0.50 | |
| Question 12 | 0.89 | 0.65 | |
| Question 13 | 0.90 | 0.52 |
| Overall Cronbach’s Alpha | Cronbach’s Alpha if Item Deleted | Item-Total Correlation | |
|---|---|---|---|
| Question 1 | 0.89 | 0.89 | 0.64 |
| Question 2 | 0.89 | 0.63 | |
| Question 3 | 0.89 | 0.59 | |
| Question 4 | 0.89 | 0.53 | |
| Question 5 | 0.90 | 0.27 | |
| Question 6 | 0.89 | 0.45 | |
| Question 7 | 0.88 | 0.69 | |
| Question 8 | 0.89 | 0.62 | |
| Question 9 | 0.89 | 0.59 | |
| Question 10 | 0.89 | 0.41 | |
| Question 11 | 0.89 | 0.58 | |
| Question 12 | 0.89 | 0.49 | |
| Question 13 | 0.89 | 0.45 | |
| Question 14 | 0.89 | 0.49 | |
| Question 15 | 0.89 | 0.58 | |
| Question 16 | 0.89 | 0.58 | |
| Question 17 | 0.89 | 0.43 | |
| Question 18 | 0.89 | 0.45 | |
| Question 19 | 0.89 | 0.48 | |
| Question 20 | 0.89 | 0.49 |
| Overall Cronbach’s Alpha | Cronbach’s Alpha if Item Deleted | Item-Total Correlation | |
|---|---|---|---|
| Question 14 | 0.79 | 0.75 | 0.54 |
| Question 15 | 0.73 | 0.64 | |
| Question 16 | 0.72 | 0.67 | |
| Question 17 | 0.77 | 0.47 | |
| Question 18 | 0.77 | 0.46 | |
| Question 19 | 0.78 | 0.42 | |
| Question 20 | 0.78 | 0.40 |
| Assessments | N | Mean ± SD | Minimum | Maximum |
|---|---|---|---|---|
| Baseline | 133 | 61 ± 16 | 29 | 71 |
| 2-week follow-up | 131 | 61 ± 16 | 26 | 74 |
| ISYQOL-TC | Total | SRS-22 | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Spine Health | Brace | Function | Pain | Self-Image | Mental Health | Satisfaction | |||
| N | 0 | 0 | 0 | 68 | 57 | 4 | 31 | 12 | 2 |
| Percentage | 0% | 0% | 0% | 51.1% | 42.8% | 3.0% | 23.3% | 9.0% | 1.5% |
| Principal Component Analysis of Residuals | |||||||
|---|---|---|---|---|---|---|---|
| Raw Variance Explained by Measure | |||||||
| First Component Dimension Eigenvalue | First Component Dimension Observed Percentage | First Contrast Residuals (Second Major Component) Eigenvalue | |||||
| ISYQOL-TC Q1-20 | 16.99 | 45.9% | 2.47 | ||||
| Fit Statistics | |||||||
| Domains | Questions | Measure | SE | Infit MnSq | Infit Zstd | Outfit MnSq | Outfit Zstd |
| Spine health | 1 | −1.07 | 0.17 | 0.64 | −3.51 | 0.72 | −2.54 |
| 2 | −0.11 | 0.18 | 0.93 | −0.61 | 0.86 | −1.04 | |
| 3 | −0.08 | 0.18 | 0.87 | −1.14 | 0.79 | −1.63 | |
| 4 | 0.40 | 0.18 | 0.87 | −1.12 | 0.84 | −0.99 | |
| 5 | −1.25 | 0.17 | 1.26 | 2.07 | 1.45 | 3.29 | |
| 6 | 0.57 | 0.19 | 1.41 | 3.11 | 1.21 | 1.18 | |
| 7 | 0.04 | 0.18 | 0.80 | −1.76 | 0.75 | −1.88 | |
| 8 | 1.19 | 0.20 | 0.86 | −1.10 | 0.82 | −0.78 | |
| 9 | −0.05 | 0.18 | 0.67 | −3.11 | 0.66 | −2.70 | |
| 10 | −0.66 | 0.17 | 1.08 | 0.67 | 1.11 | 0.87 | |
| 11 | 0.89 | 0.19 | 1.25 | 1.92 | 1.28 | 1.38 | |
| 12 | 0.40 | 0.18 | 1.09 | 0.75 | 1.05 | 0.35 | |
| 13 | 1.53 | 0.21 | 1.11 | 0.82 | 1.59 | 1.94 | |
| Brace | 14 | −0.61 | 0.26 | 1.11 | 0.67 | 1.10 | 0.55 |
| 15 | −1.38 | 0.25 | 1.17 | 0.95 | 1.16 | 0.87 | |
| 16 | <0.01 | 0.26 | 1.11 | −0.69 | 1.02 | 0.16 | |
| 17 | −1.64 | 0.25 | 1.04 | 0.28 | 1.22 | 1.18 | |
| 18 | 1.70 | 0.33 | 1.17 | 0.81 | 1.01 | 0.16 | |
| 19 | 2.31 | 0.37 | 0.98 | <0.01 | 0.84 | −0.11 | |
| 20 | −2.16 | 0.26 | 0.92 | −0.46 | 0.96 | −0.13 | |
References
- Zheng, Y.; Wu, X.; Dang, Y.; Yang, Y.; Reinhardt, J.D.; Dang, Y. Prevalence and determinants of idiopathic scoliosis in primary school children in Beitang district, Wuxi, China. J. Rehabil. Med. 2016, 48, 547–553. [Google Scholar] [CrossRef] [PubMed]
- Yılmaz, H.; Zateri, C.; Kusvuran Ozkan, A.; Kayalar, G.; Berk, H. Prevalence of adolescent idiopathic scoliosis in Turkey: An epidemiological study. Spine J. 2020, 20, 947–955. [Google Scholar] [CrossRef] [PubMed]
- Singh, H.; Shipra; Sharma, V.; Sharma, I.; Sharma, A.; Modeel, S.; Gupta, N.; Gupta, G.; Pandita, A.K.; Butt, M.F.; et al. The first study of epidemiology of adolescent idiopathic scoliosis shows lower prevalence in females of Jammu and Kashmir, India. Am. J. Transl. Res. 2022, 14, 1100–1106. [Google Scholar] [PubMed]
- Konieczny, M.R.; Senyurt, H.; Krauspe, R. Epidemiology of adolescent idiopathic scoliosis. J. Child Orthop. 2013, 7, 3–9. [Google Scholar] [CrossRef]
- Wong, A.Y.L.; Chan, C.; Hiller, C.; Yung, P.S.H.; Lau, K.K.L.; Samartzis, D.; Surgenor, B. Is Scoliosis Associated with Dance Injury in Young Recreational Dancers? A Large-Scale Cross-Sectional Epidemiological Study. J. Dance Med. Sci. 2022, 26, 41–49. [Google Scholar] [CrossRef]
- Wong, A.Y.L.; Samartzis, D.; Cheung, P.W.H.; Cheung, J.P.Y. How Common Is Back Pain and What Biopsychosocial Factors Are Associated with Back Pain in Patients with Adolescent Idiopathic Scoliosis? Clin. Orthop. Relat. Res. 2019, 477, 676–686. [Google Scholar] [CrossRef]
- Tones, M.; Moss, N.; Polly, D.W., Jr. A review of quality of life and psychosocial issues in scoliosis. Spine 2006, 31, 3027–3038. [Google Scholar] [CrossRef]
- Caronni, A.; Sciumè, L.; Donzelli, S.; Zaina, F.; Negrini, S. ISYQOL: A Rasch-consistent questionnaire for measuring health-related quality of life in adolescents with spinal deformities. Spine J. 2017, 17, 1364–1372. [Google Scholar] [CrossRef]
- Bagó, J.; Pérez-Grueso, F.J.; Les, E.; Hernández, P.; Pellisé, F. Minimal important differences of the SRS-22 Patient Questionnaire following surgical treatment of idiopathic scoliosis. Eur. Spine J. 2009, 18, 1898–1904. [Google Scholar] [CrossRef]
- Asher, M.; Min Lai, S.; Burton, D.; Manna, B. The reliability and concurrent validity of the scoliosis research society-22 patient questionnaire for idiopathic scoliosis. Spine 2003, 28, 63–69. [Google Scholar] [CrossRef]
- Garg, B.; Mehta, N.; Swamy, A.M.; Kumar, S.; Dixit, V.; Gupta, V. Reliability and validity of a cross-culturally adapted Hindi version of the SRS-22r questionnaire in Indian patients. Spine Deform. 2020, 8, 885–891. [Google Scholar] [CrossRef] [PubMed]
- Asher, M.A.; Lai, S.M.; Glattes, R.C.; Burton, D.C.; Alanay, A.; Bago, J. Refinement of the SRS-22 Health-Related Quality of Life questionnaire Function domain. Spine 2006, 31, 593–597. [Google Scholar] [CrossRef]
- Monticone, M.; Nava, C.; Leggero, V.; Rocca, B.; Salvaderi, S.; Ferrante, S.; Ambrosini, E. Measurement properties of translated versions of the Scoliosis Research Society-22 Patient Questionnaire, SRS-22: A systematic review. Qual. Life Res. 2015, 24, 1981–1998. [Google Scholar] [CrossRef] [PubMed]
- Forest, C.; Parent, E.; Chémaly, O.; Barchi, S.; Donzelli, S.; Negrini, S.; Fortin, C. Cross-cultural French-Canadian adaptation and psychometric assessment of the Italian Spine Youth Quality of Life (ISYQOL) questionnaire. Spine J. 2022, 22, 1893–1902. [Google Scholar] [CrossRef] [PubMed]
- Caronni, A.; Donzelli, S.; Zaina, F.; Negrini, S. The Italian Spine Youth Quality of Life questionnaire measures health-related quality of life of adolescents with spinal deformities better than the reference standard, the Scoliosis Research Society 22 questionnaire. Clin. Rehabil. 2019, 33, 1404–1415. [Google Scholar] [CrossRef] [PubMed]
- Alanazi, M.H.; Parent, E.C.; Bettany-Saltikov, J.; Hill, D.; Southon, S. Convergent validity, ceiling, and floor effects of the English-ISYQOL against established quality of life questionnaires (SRS-22r and SAQ) and curve angles in adolescents with idiopathic scoliosis. Stud. Health Technol. Inform. 2021, 280, 225–230. [Google Scholar]
- Fallatah, S.M.; Emam, S.; Al-Ghamdi, G.; Almatrafi, F. Cross-cultural adaptation and validation of the Italian Spine Youth Quality of Life (ISYQOL) questionnaire’s Arabic version. Medicine 2021, 100, e28063. [Google Scholar] [CrossRef]
- Kinel, E.; Korbel, K.; Janusz, P.; Kozinoga, M.; Czaprowski, D.; Kotwicki, T. Polish Adaptation of the Italian Spine Youth Quality of Life Questionnaire. J. Clin. Med. 2021, 10, 2081. [Google Scholar] [CrossRef]
- Liu, S.; Liang, J.; Xu, N.; Mai, S.; Wang, Q.; Zeng, L.; Du, C.; Du, Y.; Zeng, Y.; Yu, M.; et al. Reliability and validity of simplified Chinese version of the Italian spine youth quality of life questionnaire in adolescents with idiopathic scoliosis. BMC Musculoskelet. Disord. 2021, 22, 568. [Google Scholar] [CrossRef]
- Guo, J.; Lau, A.H.; Chau, J.; Ng, B.K.; Lee, K.M.; Qiu, Y.; Cheng, J.C.; Lam, T.P. A validation study on the traditional Chinese version of Spinal Appearance Questionnaire for adolescent idiopathic scoliosis. Eur. Spine J. 2016, 25, 3186–3193. [Google Scholar] [CrossRef]
- Eremenco, S.L.; Cella, D.; Arnold, B.J. A comprehensive method for the translation and cross-cultural validation of health status questionnaires. Eval. Health Prof. 2005, 28, 212–232. [Google Scholar] [CrossRef]
- Terwee, C.B.; Mokkink, L.B.; Knol, D.L.; Ostelo, R.W.; Bouter, L.M.; de Vet, H.C. Rating the methodological quality in systematic reviews of studies on measurement properties: A scoring system for the COSMIN checklist. Qual. Life Res. 2012, 21, 651–657. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.H.; Lenderking, W.; Jin, Y.; Wyrwich, K.W.; Gelhorn, H.; Revicki, D.A. Is Rasch model analysis applicable in small sample size pilot studies for assessing item characteristics? An example using PROMIS pain behavior item bank data. Qual. Life Res. 2014, 23, 485–493. [Google Scholar] [CrossRef]
- Reeve, B.B.; McFatrich, M.; Mack, J.W.; Pinheiro, L.C.; Jacobs, S.S.; Baker, J.N.; Withycombe, J.S.; Lin, L.; Mann, C.M.; Villabroza, K.R.; et al. Expanding construct validity of established and new PROMIS Pediatric measures for children and adolescents receiving cancer treatment. Pediatr. Blood Cancer 2020, 67, e28160. [Google Scholar] [CrossRef]
- Kinel, E.; Korbel, K.; Kozinoga, M.; Czaprowski, D.; Stępniak, Ł.; Kotwicki, T. The Measurement of Health-Related Quality of Life of Girls with Mild to Moderate Idiopathic Scoliosis-Comparison of ISYQOL versus SRS-22 Questionnaire. J. Clin. Med. 2021, 10, 4806. [Google Scholar] [CrossRef]
- Babaee, T.; Esfandiari, E.; Rouhani, N.; Nakhaee, M.; Saeedi, M.; Hedayati, Z.; Jalali, M.; Moradi, V. The Italian Spine Youth Quality of Life questionnaire: Reliability and validity of the Persian version in adolescents with spinal deformities. Spine Deform. 2022, 10, 775–782. [Google Scholar] [CrossRef] [PubMed]
- Cheung, K.M.; Senkoylu, A.; Alanay, A.; Genc, Y.; Lau, S.; Luk, K.D. Reliability and concurrent validity of the adapted Chinese version of Scoliosis Research Society-22 (SRS-22) questionnaire. Spine 2007, 32, 1141–1145. [Google Scholar] [CrossRef] [PubMed]
- Richardson, L.P.; McCauley, E.; Grossman, D.C.; McCarty, C.A.; Richards, J.; Russo, J.E.; Rockhill, C.; Katon, W. Evaluation of the Patient Health Questionnaire-9 Item for detecting major depression among adolescents. Pediatrics 2010, 126, 1117–1123. [Google Scholar] [CrossRef]
- Lin, Q.; Bonkano, O.; Wu, K.; Liu, Q.; Ali Ibrahim, T.; Liu, L. The Value of Chinese Version GAD-7 and PHQ-9 to Screen Anxiety and Depression in Chinese Outpatients with Atypical Chest Pain. Ther. Clin. Risk Manag. 2021, 17, 423–431. [Google Scholar] [CrossRef]
- Pearlin, L.I.; Schooler, C. The structure of coping. J. Health Soc. Behav. 1978, 19, 2–21. [Google Scholar] [CrossRef]
- Pearlin, L.I.; Lieberman, M.A.; Menaghan, E.G.; Mullan, J.T. The stress process. J. Health Soc. Behav. 1981, 22, 337–356. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y. Reliability and validity of the simplified Coping Style Questionnaire. Chin. J. Clin. Psychol. 1998, 6, 114–115. [Google Scholar]
- Yu, H.; Li, M.; Li, Z.; Xiang, W.; Yuan, Y.; Liu, Y.; Li, Z.; Xiong, Z. Coping style, social support and psychological distress in the general Chinese population in the early stages of the COVID-19 epidemic. BMC Psychiatry 2020, 20, 426. [Google Scholar] [CrossRef] [PubMed]
- Ho, K.Y.; Li, W.H.; Lam, K.W.; Chui, S.Y.; Chan, C.F. Psychometric properties of the Chinese version of the fatigue scale-adolescent. BMC Cancer 2015, 15, 938. [Google Scholar] [CrossRef]
- Lynn, M.R. Determination and quantification of content validity. Nurs. Res. 1986, 35, 382–385. [Google Scholar] [CrossRef] [PubMed]
- Polit, D.F.; Beck, C.T. Nursing Research: Principles and Methods; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2004. [Google Scholar]
- Linacre, J.M. A User’s Guide to WINSTEPS Ministep Rasch-Model Computer Programs; Winsteps: Chicago, IL, USA, 2011. [Google Scholar]
- Terwee, C.B.; Bot, S.D.; de Boer, M.R.; van der Windt, D.A.; Knol, D.L.; Dekker, J.; Bouter, L.M.; de Vet, H.C. Quality criteria were proposed for measurement properties of health status questionnaires. J. Clin. Epidemiol. 2007, 60, 34–42. [Google Scholar] [CrossRef] [PubMed]
- De Vet, H.C.W. Measurement in Medicine: A Practical Guide; Cambridge University Press: Cambridge, UK, 2011. [Google Scholar]
- Gagnon, J.C.; Barber, B.R. The SAGE Encyclopedia of Educational Research, Measurement, and Evaluation; Frey, B.B., Ed.; Sage Publications: Beverly Hills, CA, USA, 2018; p. 668. [Google Scholar]
- Fortin, C.; Feldman, D.E.; Cheriet, F.; Gravel, D.; Gauthier, F.; Labelle, H. Reliability of a quantitative clinical posture assessment tool among persons with idiopathic scoliosis. Physiotherapy 2012, 98, 64–75. [Google Scholar] [CrossRef]
- Tsutakawa, R.K.; Johnson, J.C. The effect of uncertainty of item parameter estimation on ability estimates. Psychometrika 1990, 55, 371–390. [Google Scholar] [CrossRef]
- Carmines, E.G.; Zeller, R.A. Reliability and Validity Assessment; Sage Publications: Beverly Hills, CA, USA, 1979. [Google Scholar]
- Conrad, K.J.; Conrad, K.M.; Dennis, M.L.; Riley, B.B.; Funk, R.; Stein, M.A.; Dennis, M.L. Dimensionality, hierarchical structure, age generalizability, and criterion validity of the GAIN’s Behavioral Complexity Scale. Psychol. Assess. 2012, 24, 913–924. [Google Scholar] [CrossRef]
- Reeve, B.B.; Hays, R.D.; Bjorner, J.B.; Cook, K.F.; Crane, P.K.; Teresi, J.A.; Thissen, D.; Revicki, D.A.; Weiss, D.J.; Hambleton, R.K.; et al. Psychometric evaluation and calibration of health-related quality of life item banks: Plans for the Patient-Reported Outcomes Measurement Information System (PROMIS). Med. Care 2007, 45 (Suppl. S1), S22–S31. [Google Scholar] [CrossRef]
- Bond, T.G.; Fox, C.M. Applying the Rasch Model: Fundamental Measurement in the Human Sciences; Lawrence Erlbaum Associates, Inc.: Mahwah, NJ, USA, 2001. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: Abingdon, UK, 2013. [Google Scholar]
- Rao, D.; Gela, N.; Daley, E.M.; Kattezham, R.; Rodriguez, G.; Cella, D. Developing a measure of health-related quality of life for women with cervical dysplasia resulting from human papillomavirus infection. Int. J. STD AIDS 2010, 21, 697–701. [Google Scholar] [CrossRef] [PubMed]
- Wright, B.D. Fundamental measurement for psychology. In The New Rules of Measurement: What Every Psychologist and Educator Should Know; Embretson, S.E., Hershberger, S.L., Eds.; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 1999; pp. 65–104. [Google Scholar]
- Negrini, S.; Zaina, F.; Buyukaslan, A.; Fortin, C.; Karavidas, N.; Kotwicki, T.; Korbel, K.; Parent, E.; Sanchez-Raya, J.; Shearer, K.; et al. Cross-cultural validation of the Italian Spine Youth Quality of Life questionnaire: The ISYQOL international. Eur. J. Phys. Rehabil. Med. 2023, 59, 364–376. [Google Scholar] [CrossRef]
- Parent, E.; Lin, A.; Shearer, K.; Southon, S.; Donzelli, S.; Negrini, S. Comparison of the test-retest reliability of the English translation of the ISYQOL scale (Italian Spine Youth Quality-of-life) to other self-image questionnaires in adolescents with idiopathic scoliosis. In Proceedings of the 13th International Conference on Conservative Management of Spinal Deformities (SOSORT), Dubrovnik, Croatia, 20 April 2018. [Google Scholar]
- Perline, R.; Wright, B.D.; Wainer, H. The Rasch Model as Additive Conjoint Measurement. Appl. Psychol. Meas. 1979, 3, 237–255. [Google Scholar] [CrossRef]
- Freidel, K.; Petermann, F.; Reichel, D.; Steiner, A.; Warschburger, P.; Weiss, H.R. Quality of life in women with idiopathic scoliosis. Spine 2002, 27, E87–E91. [Google Scholar] [CrossRef]
- Freidel, K.; Reichel, D.; Steiner, A.; Warschburger, P.; Petermann, F.; Weiss, H.R. Idiopathic scoliosis and quality of life. Stud. Health Technol. Inform. 2002, 88, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Haraldstad, K.; Christophersen, K.A.; Helseth, S. Health-related quality of life and pain in children and adolescents: A school survey. BMC Pediatr. 2017, 17, 174. [Google Scholar] [CrossRef] [PubMed]
- Henning, E.R.; Turk, C.L.; Mennin, D.S.; Fresco, D.M.; Heimberg, R.G. Impairment and quality of life in individuals with generalized anxiety disorder. Depress. Anxiety 2007, 24, 342–349. [Google Scholar] [CrossRef] [PubMed]
- Barrera, T.L.; Norton, P.J. Quality of life impairment in generalized anxiety disorder, social phobia, and panic disorder. J. Anxiety Disord. 2009, 23, 1086–1090. [Google Scholar] [CrossRef]
- Cerea, S.; Ghisi, M.; Pitteri, M.; Guandalini, M.; Strober, L.B.; Scozzari, S.; Crescenzo, F.; Calabrese, M. Coping Strategies and Their Impact on Quality of Life and Physical Disability of People with Multiple Sclerosis. J. Clin. Med. 2021, 10, 5607. [Google Scholar] [CrossRef]
- Beka, A.; Dermitzaki, I.; Christodoulou, A.; Kapetanos, G.; Markovitis, M.; Pournaras, J. Children and adolescents with idiopathic scoliosis: Emotional reactions, coping mechanisms, and self-esteem. Psychol. Rep. 2006, 98, 477–485. [Google Scholar] [CrossRef]
- Adobor, R.D.; Rimeslatten, S.; Steen, H.; Brox, J.I. School screening and point prevalence of adolescent idiopathic scoliosis in 4000 Norwegian children aged 12 years. Scoliosis 2011, 6, 23. [Google Scholar] [CrossRef] [PubMed]
- Cheng, J.C.; Castelein, R.M.; Chu, W.C.; Danielsson, A.J.; Dobbs, M.B.; Grivas, T.B.; Gurnett, C.A.; Luk, K.D.; Moreau, A.; Newton, P.O.; et al. Adolescent idiopathic scoliosis. Nat. Rev. Dis. Primers 2015, 1, 15030. [Google Scholar] [CrossRef] [PubMed]
- Tambe, A.D.; Panikkar, S.J.; Millner, P.A.; Tsirikos, A.I. Current concepts in the surgical management of adolescent idiopathic scoliosis. Bone Jt. J. 2018, 100, 415–424. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Cameron, I.M.; Crawford, J.R.; Lawton, K.; Reid, I.C. Psychometric comparison of PHQ-9 and HADS for measuring depression severity in primary care. Br. J. Gen. Pract. 2008, 58, 32–36. [Google Scholar] [CrossRef]
- Tsai, F.J.; Huang, Y.H.; Liu, H.C.; Huang, K.Y.; Huang, Y.H.; Liu, S.I. Patient health questionnaire for school-based depression screening among Chinese adolescents. Pediatrics 2014, 133, e402–e409. [Google Scholar] [CrossRef]
- Zhang, C.; Wang, T.; Zeng, P.; Zhao, M.; Zhang, G.; Zhai, S.; Meng, L.; Wang, Y.; Liu, D. Reliability, Validity, and Measurement Invariance of the General Anxiety Disorder Scale Among Chinese Medical University Students. Front. Psychiatry 2021, 12, 648755. [Google Scholar] [CrossRef]
- Lim, Z.X.; Chua, W.L.; Lim, W.S.; Lim, A.Q.; Chua, K.C.; Chan, E.Y. Psychometrics of the Pearlin Mastery Scale among Family Caregivers of Older Adults Who Require Assistance in Activities of Daily Living. Int. J. Environ. Res. Public Health 2022, 19, 4639. [Google Scholar] [CrossRef]
- Jensen, M.P.; McFarland, C.A. Increasing the reliability and validity of pain intensity measurement in chronic pain patients. Pain 1993, 55, 195–203. [Google Scholar] [CrossRef]
- Wang, Y.; Xiao, H.; Zhang, X.; Wang, L. The Role of Active Coping in the Relationship Between Learning Burnout and Sleep Quality Among College Students in China. Front. Psychol. 2020, 11, 647. [Google Scholar] [CrossRef]
- Chen, X.; Liu, T.; Luo, J.; Ren, S. Data for teenagers’ stressor, mental health, coping style, social support, parenting style and self-efficacy in South China. Data Brief 2020, 29, 105202. [Google Scholar] [CrossRef] [PubMed]
- Xiao, H.; Li, X.; Zhou, Z.; Liu, H.; Hu, C.; Liu, T.; Chen, D.; You, L. Negative coping style mediates the relationship between negative mental and suicide risk among migrant workers in China. Sci. Rep. 2022, 12, 305. [Google Scholar] [CrossRef] [PubMed]
- Cui, S.; Jiang, Y.; Shi, Q.; Zhang, L.; Kong, D.; Qian, M.; Chu, J. Impact of COVID-19 on Anxiety, Stress, and Coping Styles in Nurses in Emergency Departments and Fever Clinics: A Cross-Sectional Survey. Risk Manag. Healthc. Policy 2021, 14, 585–594. [Google Scholar] [CrossRef] [PubMed]
| Number of Participants | Gender N (%) | Mean Age ±SD (years) | Curve Classification N (%) | Mean Curve Degree ±SD (°) |
|---|---|---|---|---|
| Brace (n = 57) | F = 48 (84%) M = 9 (16%) | 13.5 ± 1.9 | T: 1 (2%) TL: 13 (23%) L: 2 (4%) 2-curve: 33 (58%) 3-curve: 8 (14%) | 28 ± 9 |
| No brace (n = 76) | F = 51 (67%) M = 25 (33%) | 14.2 ± 2.1 | T: 10 (13%) TL: 21 (27.6%) L: 1 (1.3%) 2-curve: 39 (51.3%) 3-curve: 5 (6.6%) | 26 ± 12 |
| Total (n = 133) | F = 99 (74%) M = 34 (25%) | 13.9 ± 2.1 | T: 11 (8%) TL: 34 (26%) L: 3 (2%) 2-curve: 72 (54%) 3-curve: 13 (10%) | 27 ± 11 |
| Questionnaire | Cronbach’s Alpha | ICC (95% Confidence Interval) | Mean ± SD (Raw Scores) | Mean ± SD (%) | SEM | MDC95 |
|---|---|---|---|---|---|---|
| ISYOQL-TC (No brace) n = 76 | 0.90 ** | 0.95 (0.92–0.97) ** | 8 ± 6 | 63 ± 18 | 4% | 12% |
| ISYOQL-TC (Brace) n = 57 | 0.89 ** | 0.96 (0.94–0.98) ** | 13 ± 7 | 59 ± 11 | 2% | 6% |
| Spine health domain n = 133 | 0.89 ** | 0.95 (0.93–0.96) ** | 8 ± 5 | 1 | 3 | |
| Brace domain n = 57 | 0.79 ** | 0.96 (0.93–0.98) ** | 5 ± 3 | 1 | 1 |
| SRS-22r Domains | ISYQOL-TC Interval Measure (%) | |||
|---|---|---|---|---|
| Mean ± SD | No Brace | Brace | Total | |
| Function | 24 ± 2 | 0.34 ** | 0.41 ** | 0.38 ** |
| Pain | 23 ± 2 | 0.41 ** | 0.33 ** | 0.41 ** |
| Self-image | 19 ± 3 | 0.58 ** | 0.64 ** | 0.59 ** |
| Mental health | 21 ± 3 | 0.55 ** | 0.56 ** | 0.55 ** |
| Satisfaction | 8 ± 1 | 0.24 ** | 0.24 ** | 0.26 ** |
| Total | 95 ± 9 | 0.63 ** | 0.67 ** | 0.65 ** |
| ISYQOL-TC Interval Measure (%) | ||||
|---|---|---|---|---|
| Mean ± SD | No Brace | Brace | Total | |
| SCSQ-A | 19 ± 7 | 0.11 | 0.10 | 0.103 |
| SCSQ-P | 9 ± 5 | −0.14 | −0.13 | −0.135 |
| PHQ-9 | 4 ± 4 | −0.43 ** | −0.41 ** | −0.46 ** |
| GAD-7 | 3 ± 4 | −0.40 ** | −0.43 ** | −0.43 ** |
| MAS | 16 ± 5 | 0.43 ** | 0.43 ** | 0.44 ** |
| NPRS | 1 ± 2 | −0.38 ** | −0.41 ** | −0.39 ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheng, A.Y.; Jim, P.K.; Kwan, N.W.; Chan, S.W.W.; Cheung, J.P.Y.; Cheung, P.W.H.; Negrini, S.; Cheung, C.K.C.; Wong, A.Y.L.; Parent, E.C. Cross-Cultural Adaptation and Psychometric Properties of the Traditional Chinese Version of the Italian Spine Youth Quality of Life (ISYQOL) Questionnaire. Healthcare 2023, 11, 2683. https://doi.org/10.3390/healthcare11192683
Cheng AY, Jim PK, Kwan NW, Chan SWW, Cheung JPY, Cheung PWH, Negrini S, Cheung CKC, Wong AYL, Parent EC. Cross-Cultural Adaptation and Psychometric Properties of the Traditional Chinese Version of the Italian Spine Youth Quality of Life (ISYQOL) Questionnaire. Healthcare. 2023; 11(19):2683. https://doi.org/10.3390/healthcare11192683
Chicago/Turabian StyleCheng, Ava Ying, Pik Kwan Jim, Ning Wai Kwan, Stephen W. W. Chan, Jason P. Y. Cheung, Prudence W. H. Cheung, Stefano Negrini, Chelsia K. C. Cheung, Arnold Y. L. Wong, and Eric C. Parent. 2023. "Cross-Cultural Adaptation and Psychometric Properties of the Traditional Chinese Version of the Italian Spine Youth Quality of Life (ISYQOL) Questionnaire" Healthcare 11, no. 19: 2683. https://doi.org/10.3390/healthcare11192683
APA StyleCheng, A. Y., Jim, P. K., Kwan, N. W., Chan, S. W. W., Cheung, J. P. Y., Cheung, P. W. H., Negrini, S., Cheung, C. K. C., Wong, A. Y. L., & Parent, E. C. (2023). Cross-Cultural Adaptation and Psychometric Properties of the Traditional Chinese Version of the Italian Spine Youth Quality of Life (ISYQOL) Questionnaire. Healthcare, 11(19), 2683. https://doi.org/10.3390/healthcare11192683