
Effective Vowel Stimuli for Measuring Occlusion Effect in the Pediatric Population


Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experiment 1—Measuring the Sound Pressure Level and First Formant Frequency of Vowels
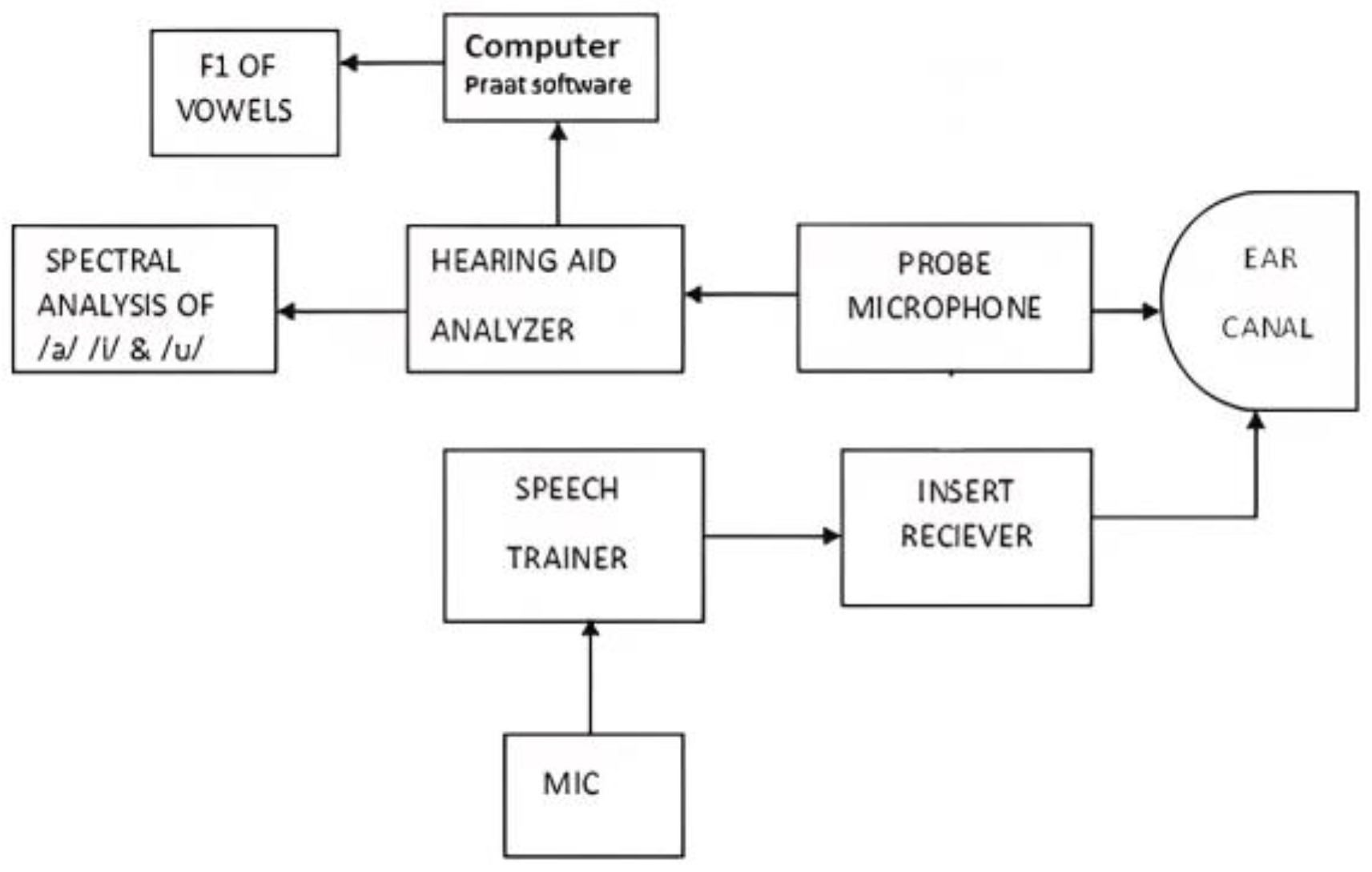
2.2.1. Instrumentation
2.2.2. Procedure
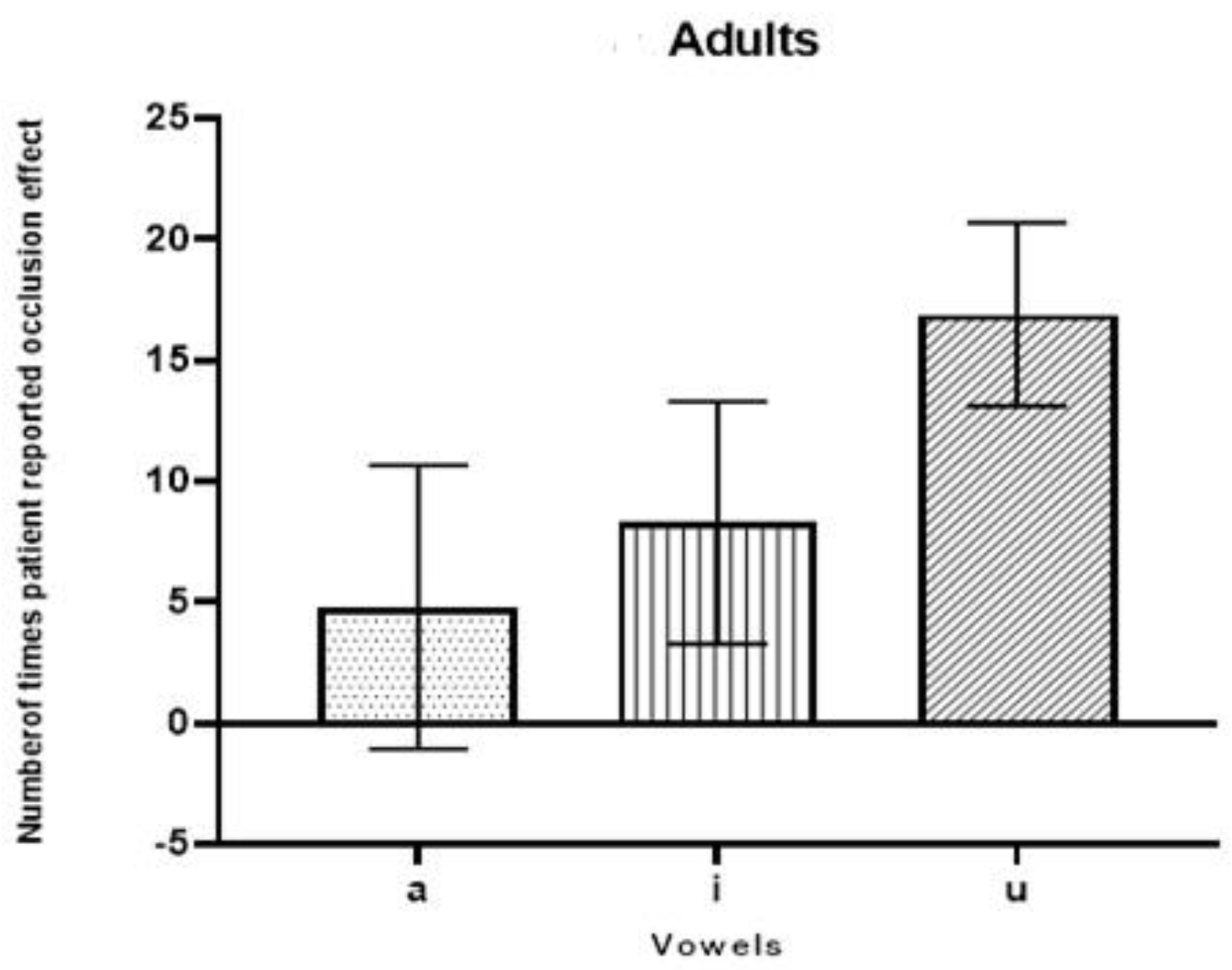
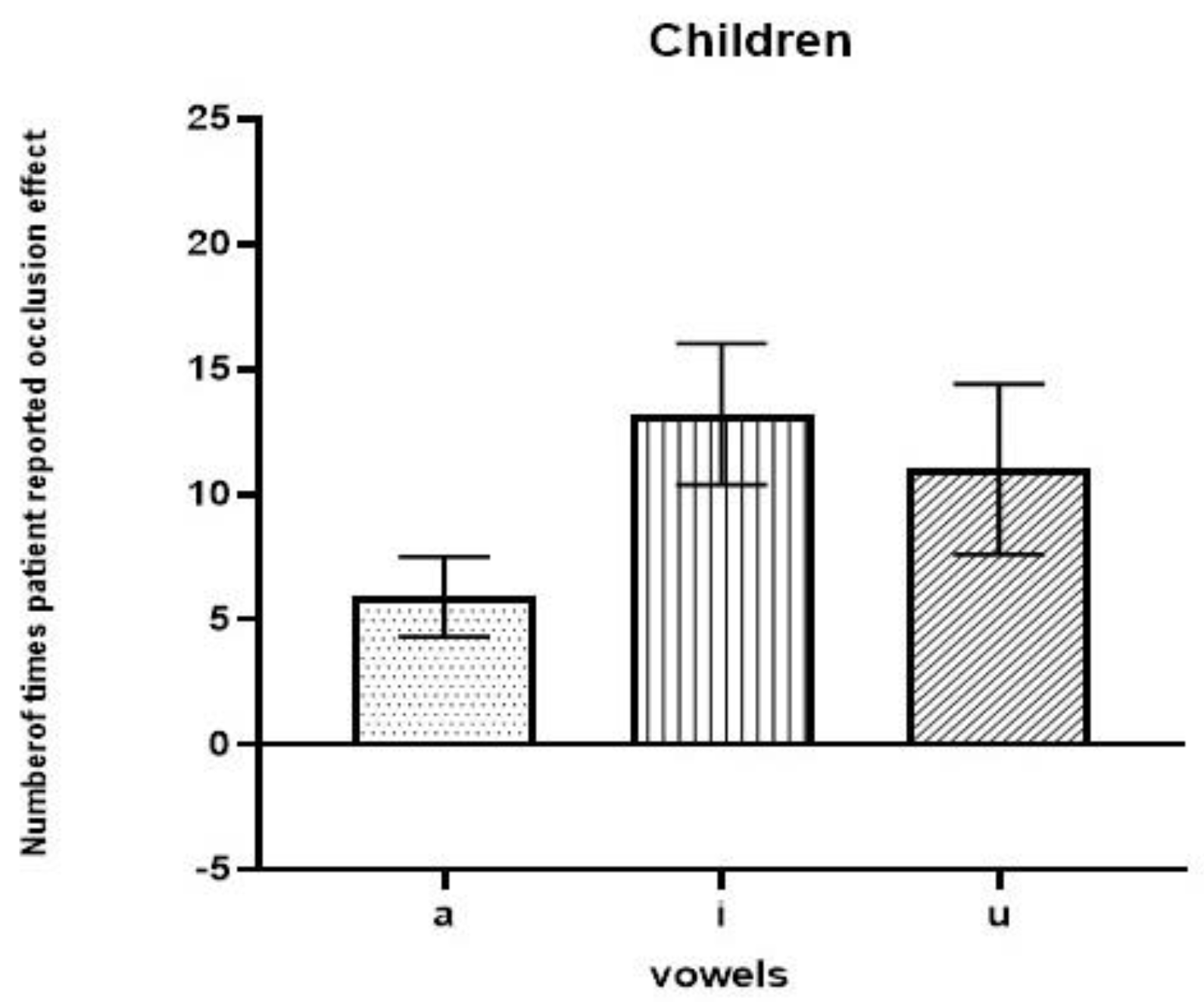
2.3. Experiment 2—Paired Comparison Method as Used to Determine the Best Vowel with Which to Assess the loudness Reflecting an Occlusion Effect
2.4. Statistical Analyses
3. Results
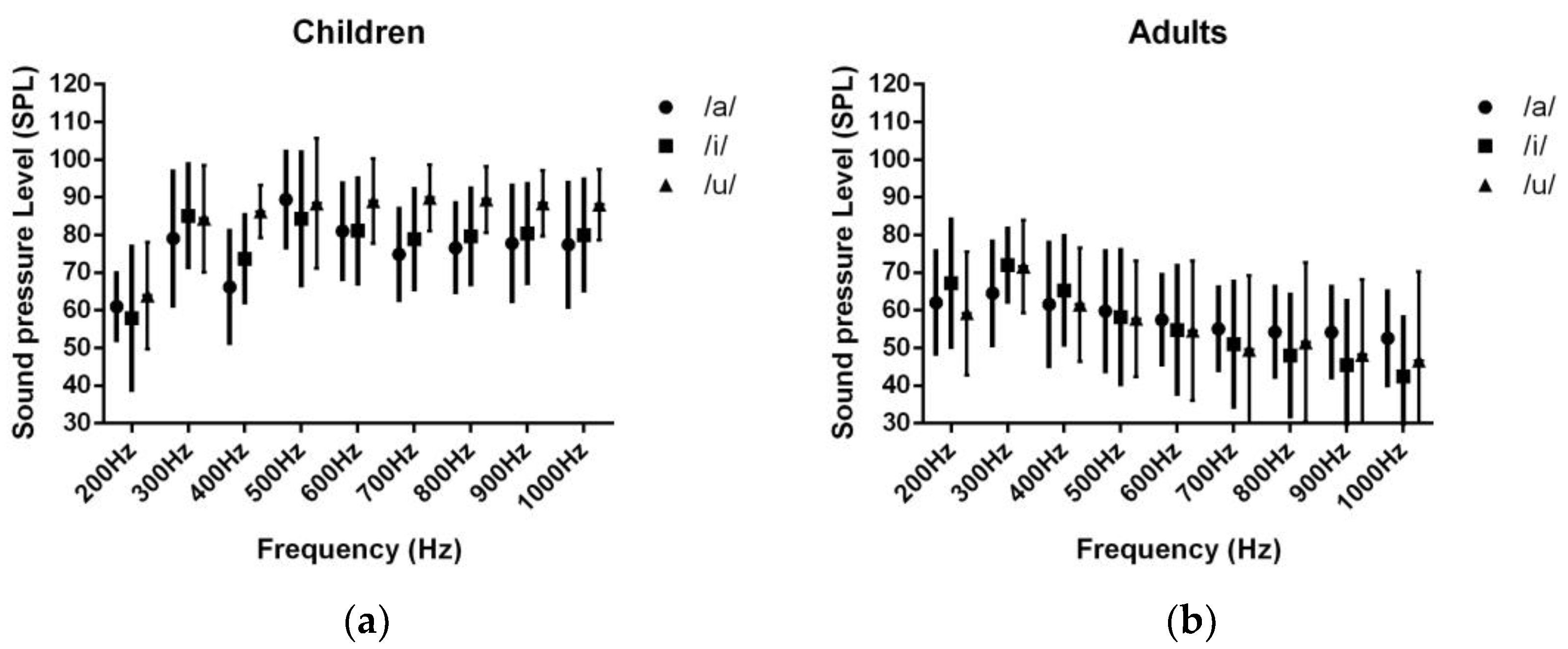
3.1. Determining the Sound Pressure Level in Each Participant’s Ear Canal
3.1.1. The Sound Pressure Level of the Vowel /a/ in Participants’ Ear Canals
3.1.2. The Sound Pressure Level of the Vowel /i/ in the Participants’ Ear Canals
3.1.3. The Sound Pressure Level of the Vowel /u/ in the Participants’ Ear Canals
3.2. Comparison of First Formant Frequencies of Vowels /a/, /i/, and /u/
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Correction Statement
References
- Pohlman, A.G.; Kranz, F.W. The Influence of Partial and Complete Occlusion of the External Auditory Canals on Air and Bone Transmitted Sound. Ann. Otolaryngol. 1926, 35, 113–121. [Google Scholar]
- Zurbrügg, T.; Stirnemannn, A.; Kuster, M.; Lissek, H. Investigations on the physical factors influencing the ear canal occlusion effect caused by hearing aids. Acta Acust. United Acust. 2014, 100, 527–536. [Google Scholar] [CrossRef]
- Schweitzer, C.; Smith, D.A. Solving the “Occlusion Effect” Electronically. Hear. Instr. 1992, 43, 30–33. [Google Scholar]
- Dillon, H. Hearing Aids: Hearing Aid Earmoulds, Ear Shells and Coupling Systems; Boomerang Press: Sydney, Australia, 2013; p. 141. [Google Scholar]
- Khanna, S.M.; Tonndorf, J.; Queller, J.E. Mechanical parameters of hearing by bone conduction. J. Acoust. Soc. Am. 1976, 60, 139–154. [Google Scholar] [CrossRef] [PubMed]
- Killion, M.C. The “Hollow” Voice Occlusion Effect. In Proceedings of the 13th Danavox Symposium, Danavox, Denmark, 11–13 September 1988; Plural Publishing Inc.: Elk Grove Village, IL, USA, 1988; pp. 231–241. [Google Scholar]
- Von Békésy, G.; Peake, W.T. Experiments in Hearing. J. Acoust. Soc. Am. 1990, 88, 2905. [Google Scholar] [CrossRef]
- Homma, K.; Du, Y.; Shimizu, Y.; Puria, S. Ossicular resonance modes of the human middle ear for bone and air conduction. J. Acoust. Soc. Am. 2009, 125, 968–979. [Google Scholar] [CrossRef] [PubMed]
- Curran, J. A Forgotten Technique for Resolving The Occlusion Effect. Repr. Innov. 2012, 2, 35–40. [Google Scholar]
- MacKenzie, D.J. Open-canal fittings and the hearing aid occlusion effect. Hear. J. 2006, 59, 50–56. [Google Scholar] [CrossRef]
- Stender, T.; Appleby, R. Occlusion effect measures: Are they all created equal? Hear. J. 2009, 62, 21–25. [Google Scholar] [CrossRef]
- Hillenbrand, J.; Getty, L.A.; Clark, M.J.; Wheeler, K. Acoustic characteristics of American English vowels. J. Acoust. Soc. Am. 1995, 97, 3099–3111. [Google Scholar] [CrossRef] [PubMed]
- Nikita, F.; Nikitha, M.; Narasimhan, S.V. Vowel Space Area in Individuals with Parkinson’s disease. In Proceedings of the International Symposium Frontiers of Research on Speech and Music (FRSM), Kharagpur, India, 4–5 August 2016; Indian Institute of Technology: New Delhi, India, 2016. [Google Scholar]
- Peterson, G.E.; Barney, H.L. Control methods used in a study of the vowels. J. Acoust. Soc. Am. 1952, 24, 175–184. [Google Scholar] [CrossRef]
- Fulton, B.; Martin, L. Drilling a vent often fails to give relief from occlusion. Hear. J. 2006, 59, 40–45. [Google Scholar] [CrossRef]
- Jafari, M.; Rahbar, N.; Sameni, J.; Keihani, M.R. Comparison of occlusion effect in normal hearing subjects via real ear measurement and audiometric Bing test. Audiol. Internet 2009, 17, 16–24. Available online: http://ezproxy.uky.edu/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=a9h&AN=43255946&site=ehost-live&scope=site (accessed on 20 May 2023).
- Small, S.A.; Hatton, J.L.; Stapells, D.R. Effects of bone oscillator coupling method, placement location, and occlusion on bone-conduction auditory steady-state responses in infants. Ear Hear. 2007, 28, 83–98. [Google Scholar] [CrossRef] [PubMed]
- Arehart, K.H.; Burns, E.M. Ear-canal impedance and reflection coefficient in human infants and adults. J. Acoust. Soc. Am. 1993, 94, 2617–2638. [Google Scholar]
- Turner, R.E.; Walters, T.C.; Monaghan, J.J.M.; Patterson, R.D. A statistical, formant-pattern model for segregating vowel type and vocal-tract length in developmental formant data. J. Acoust. Soc. Am. 2009, 125, 2374–2386. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Potamianos, A.; Narayanan, S. Acoustics of children’s speech: Developmental changes of temporal and spectral parameters. J. Acoust. Soc. Am. 1999, 105, 1455–1468. [Google Scholar] [CrossRef] [PubMed]
- Švec, J.G.; Granqvist, S. Tutorial and guidelines on measurement of a sound pressure level in voice and speech. J. Speech Lang. Hear. Res. 2018, 61, 441–461. [Google Scholar] [CrossRef] [PubMed]
- IBM Corp. IBM SPSS Statistics for Windows Version 24.0; IBM Corp.: Armonk, NY, USA, 2016. [Google Scholar]
- MacKenzie, D.J.; Mueller, H.G.; Ricketts, T.A.; Konkle, D.F. The hearing aid occlusion effect. Hear. J. 2004, 57, 30. [Google Scholar] [CrossRef]
- Feigin, J.A.; Kopun, J.G.; Stelmachowicz, P.G.; Gorga, M.P. Probe-tube microphone measures of ear-canal sound pressure levels in infants and children. Ear Hear. 1989, 10, 254–258. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Frequency | Children | Adults | F Value | p | ||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||
| 200 Hz | 61.0 | 8.756 | 62.10 | 13.57 | 0.04 | 0.832 |
| 300 Hz | 79.10 | 17.717 | 64.50 | 13.58 | 4.27 | 0.053 |
| 400 Hz | 66.20 | 14.741 | 61.60 | 16.25 | 0.43 | 0.516 |
| 500 Hz | 89.40 | 12.651 | 59.80 | 15.80 | 21.38 | 0.001 *** |
| 600 Hz | 81.0 | 12.667 | 57.50 | 11.73 | 18.52 | 0.001 *** |
| 700 Hz | 74.90 | 11.995 | 55.10 | 10.90 | 14.91 | 0.001 *** |
| 800 Hz | 76.60 | 11.711 | 54.30 | 11.86 | 17.89 | 0.001 *** |
| 900 Hz | 77.80 | 15.215 | 54.20 | 11.97 | 14.86 | 0.001 *** |
| 1000 Hz | 77.40 | 16.311 | 52.60 | 12.38 | 14.66 | 0.001 *** |
| Frequency | Children | Adults | F Value | p | ||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||
| 200 Hz | 57.9 | 18.94 | 67.2 | 16.87 | 1.34 | 0.262 |
| 300 Hz | 85.1 | 13.58 | 72 | 9.56 | 6.21 | 0.023 * |
| 400 Hz | 73.7 | 11.5 | 65.3 | 14.31 | 2.09 | 0.165 |
| 500 Hz | 84.3 | 17.56 | 58.2 | 17.67 | 10.97 | 0.004 ** |
| 600 Hz | 81.1 | 13.92 | 54.8 | 16.88 | 14.44 | 0.001 *** |
| 700 Hz | 78.9 | 13.18 | 51.0 | 16.54 | 17.38 | 0.001 *** |
| 800 Hz | 79.6 | 12.58 | 48.0 | 16.09 | 23.93 | 0.000 *** |
| 900 Hz | 80.4 | 13.08 | 45.4 | 17.03 | 26.56 | 0.000 *** |
| 1000 Hz | 80.0 | 14.67 | 42.4 | 15.72 | 31.20 | 0.000 *** |
| Frequency | Children | Adults | F Value | p | ||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||
| 200 Hz | 63.90 | 14.14 | 59.2 | 16.33 | 0.47 | 0.500 |
| 300 Hz | 84.30 | 14.15 | 71.6 | 12.33 | 4.576 | 0.046 * |
| 400 Hz | 86.20 | 6.97 | 61.5 | 15.05 | 22.7 | 0.001 *** |
| 500 Hz | 88.40 | 17.28 | 57.7 | 15.39 | 17.8 | 0.000 *** |
| 600 Hz | 89.0 | 11.29 | 54.6 | 18.51 | 25.15 | 0.001 *** |
| 700 Hz | 89.9 | 8.78 | 49.5 | 19.79 | 34.79 | 0.001 *** |
| 800 Hz | 89.4 | 8.78 | 51.5 | 21.13 | 27.43 | 0.001 *** |
| 900 Hz | 88.4 | 8.72 | 48.2 | 19.93 | 34.12 | 0.001 *** |
| 1000 Hz | 88.1 | 9.36 | 46.6 | 23.69 | 26.52 | 0.001 *** |
| Vowels | Children F1 | Adults F1 | F | p | ||||
|---|---|---|---|---|---|---|---|---|
| Mean | Md | SD | Mean | Md | SD | |||
| /a/ | 746.77 | 704.92 | 108.38 | 650.33 | 732.53 | 180.27 | 2.102 | 0.164 |
| /i/ | 391.55 | 413.50 | 74.66 | 264.32 | 245.02 | 28.67 | 18.747 | 0.001 *** |
| /u/ | 520.40 | 492.88 | 107.41 | 371.14 | 295.04 | 154.82 | 6.949 | 0.017 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shetty, H.N.; Narasimhan, S.V.; Mahanthesh, S. Effective Vowel Stimuli for Measuring Occlusion Effect in the Pediatric Population. J. Otorhinolaryngol. Hear. Balance Med. 2023, 4, 7. https://doi.org/10.3390/ohbm4020007
Shetty HN, Narasimhan SV, Mahanthesh S. Effective Vowel Stimuli for Measuring Occlusion Effect in the Pediatric Population. Journal of Otorhinolaryngology, Hearing and Balance Medicine. 2023; 4(2):7. https://doi.org/10.3390/ohbm4020007
Chicago/Turabian StyleShetty, Hemanth Narayan, Srirangam Vijayakumar Narasimhan, and Sharath Mahanthesh. 2023. "Effective Vowel Stimuli for Measuring Occlusion Effect in the Pediatric Population" Journal of Otorhinolaryngology, Hearing and Balance Medicine 4, no. 2: 7. https://doi.org/10.3390/ohbm4020007
APA StyleShetty, H. N., Narasimhan, S. V., & Mahanthesh, S. (2023). Effective Vowel Stimuli for Measuring Occlusion Effect in the Pediatric Population. Journal of Otorhinolaryngology, Hearing and Balance Medicine, 4(2), 7. https://doi.org/10.3390/ohbm4020007