
The Effect of Ultrasound Therapy and Muscle Energy Technique on a Case of a Young Adult with Thoracic Outlet Syndrome †


Abstract
1. Introduction
2. Patient Information
3. Clinical Findings
3.1. Posture
3.2. Active, Passive and Resistive Movement Tests
3.3. Sensibility
3.4. Special Test
- Adsense Test: positive.
- ULTT: positive, on the radial nerve.
- Wright/hyperabduction test: positive.
- EAST/Roos test: positive.
- Phalen test: negative.
- Cervical compression test: negative.
- Palpation: spasm of M. pectoralis minor dextra.
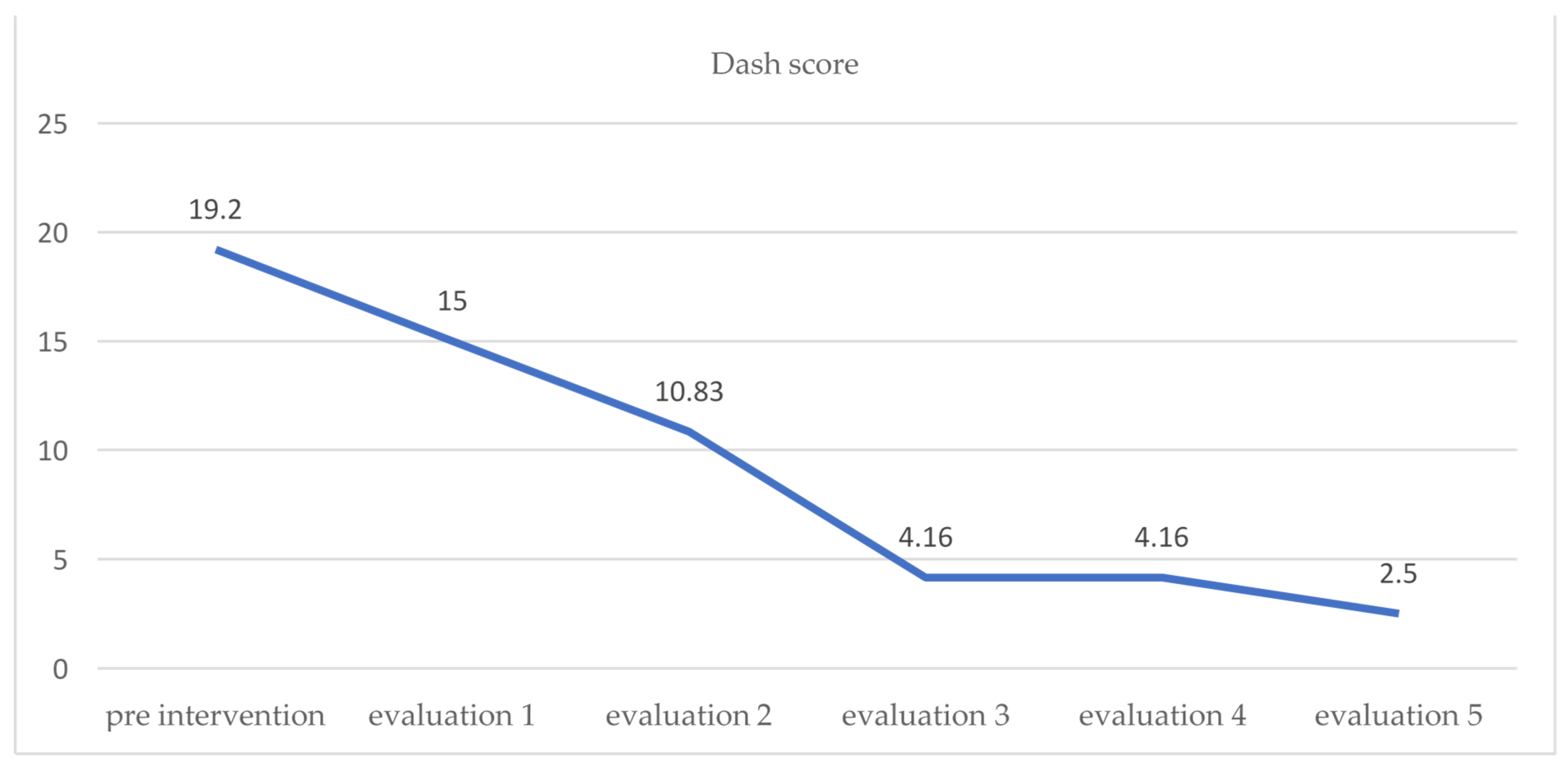
3.5. DASH Questionnaire
4. Results
5. Discussion
5.1. Ultrasound Therapy Mechanism for DASH Decrease
5.2. Muscle Energy Technique Mechanism for DASH Decrease
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Franklin, G.M. Work-related neurogenic thoracic outlet syndrome: Diagnosis and treatment. Phys. Med. Rehabil. Clin. N. Am. 2015, 26, 551–561. [Google Scholar] [CrossRef] [PubMed]
- Amper, J.M. Sindrom Outlet Dada. Jurnal Ilmiah Kesehatan Sandi Husada 2020, 9, 1083–1087. [Google Scholar] [CrossRef]
- Jones, M.R.; Prabhakar, A.; Viswanath, O.; Urits, I.; Green, J.B.; Kendrick, J.B.; Brunk, A.J.; Eng, M.R.; Orhurhu, V.; Cornett, E.M.; et al. Thoracic Outlet Syndrome: A comprehensive review of pathophysiology, diagnosis, and treatment—Pain and therapy. Pain Ther. 2019, 8, 5–18. [Google Scholar] [CrossRef] [PubMed]
- Podlaha, J. Thoracic outlet syndrome—24 years of experience. Bratisl Lek Listy. 2007, 108, 429–432. [Google Scholar] [PubMed]
- Kuswardani, K.; Amanati, S.; Yudhanto, N.U. Pengaruh Infrared, Ultrasound dan Terapi Latihan Pada Faciitis Plantaris. Jurnal Fisioterapi dan Rehabilitasi. 2018, 2, 77–86. [Google Scholar] [CrossRef]
- Patel, J.K.; Kansagara, P.R. A Study to Find out Immediate Effect of Muscle Energy Technique on Pectoralis Minor Tightness in Healthy Collegiate Individuals-An Interventional Study. Indian J. Physiother. Occup. Ther. Int. J. 2019, 13, 48. [Google Scholar] [CrossRef]
- Franchignoni, F. Minimal clinically important difference between the disabilities of the arm, shoulder, and hand outcome measure (DASH) and its shortened version (QuickDASH). J. Orthop. Sport. Phys. Ther. 2014, 44, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Starkey, C. Therapeutic Modalities; F. A. Davis: Philadelphia, PA, USA, 2013; p. 429. [Google Scholar]
- Imran, M. Effects of therapeutic ultrasound and manual physiotherapy in shoulder impingement syndrome in volleyball players. J. Islamabad MedDent. Coll. 2017, 6, 178–181. [Google Scholar]
- Santoso, I.; Satriyasa, B.K.; Munawaroh, M.; Sandi, I.N.; Muliarta, M.W. Kombinasi ultrasound Dan Dry needling LEBIH Menurunkan disabilitas Leher Dari Pada kombinasi ultrasound Dan Hold Relax Pada myofascial pain syndrom otot upper trapezius. Sport Fit. J. 2018, 6, 11–22. [Google Scholar] [CrossRef]
- Thomas, E.; Cavallaro, A.R.; Mani, D.; Bianco, A.; Palma, A. The efficacy of muscle energy techniques in symptomatic and asymptomatic subjects: A systematic review. Chiropr. Man. Ther. 2019, 27, 35. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.-S.; Lee, K.-C. The effect of applying the muscle energy technique to neck muscles on the forward head posture. J. Korean Soc. Integr. Med. 2021, 9, 173–181. [Google Scholar]
- Junaid, M.; Yaqoob, I.; Shakil Ur Rehman, S.; Ghous, M. Effects of post-isometric relaxation, myofascial trigger point release and routine physical therapy in management of acute mechanical neck pain: A randomized controlled trial. J. Pak. Med. Assoc. 2020, 70, 1688–1692. [Google Scholar] [CrossRef] [PubMed]
- Widodo, A.F.; Tien, C.-W.; Chen, C.-W.; Lai, S.-C. Isotonic and isometric exercise interventions improve the hamstring muscles’ strength and flexibility: A narrative review. Healthcare 2022, 10, 811. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Joint | Movement | Normal ROM | ROM | Pain (VAS) | Description (Altered Movement) |
|---|---|---|---|---|---|
| Flexion | Positive (3.4/10) | Negative | |||
| 90°–0°–45° | 130°–0°–30° | ||||
| Extension | Positive (4.6/10) | Negative | |||
| Abduction | Positive (3.5/10) | Negative | |||
| Shoulder | 180°–0°–45° | 105°–0°–45° | |||
| Adduction | Negative | Negative | |||
| Endorotation | Negative | Negative | |||
| 35°–0°–40° | 35°–0°–35° | ||||
| Exorotation | Positive (3.5/10) | Negative |
| Joint | Movement | ROM Normal | ROM | End Feel | Pain (VAS) |
|---|---|---|---|---|---|
| Flexion | Firm | Positive (2.4/10) | |||
| 90°–0°–45° | 145°–0°–35° | ||||
| Extension | Firm | Positive (2.5/10) | |||
| Abduction | Firm | Positive (2.2/10) | |||
| Shoulder | 180°–0°–45° | 120°–0°–45° | |||
| Adduction | Firm | Negative | |||
| Endorotation | Firm | Negative | |||
| 35°–0°–40° | 35°–0°–40° | ||||
| Exorotation | Firm | Positive (2/10) |
| Joint | Movement | MMT | VAS |
|---|---|---|---|
| Flexion | 5 | Positive (3.4/10) | |
| Extension | * | Positive (4.6/10) | |
| Shoulder | Abduction | * | Positive (3.5/10) |
| Adduction | 5 | Negative | |
| Endorotation | * | Positive (3.5/10) | |
| Exorotation | 5 | Negative |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santoso, I.; Karnadipa, T.; Putri, S.E. The Effect of Ultrasound Therapy and Muscle Energy Technique on a Case of a Young Adult with Thoracic Outlet Syndrome. Proceedings 2022, 83, 55. https://doi.org/10.3390/proceedings2022083055
Santoso I, Karnadipa T, Putri SE. The Effect of Ultrasound Therapy and Muscle Energy Technique on a Case of a Young Adult with Thoracic Outlet Syndrome. Proceedings. 2022; 83(1):55. https://doi.org/10.3390/proceedings2022083055
Chicago/Turabian StyleSantoso, Iman, Triana Karnadipa, and Safitry Eka Putri. 2022. "The Effect of Ultrasound Therapy and Muscle Energy Technique on a Case of a Young Adult with Thoracic Outlet Syndrome" Proceedings 83, no. 1: 55. https://doi.org/10.3390/proceedings2022083055
APA StyleSantoso, I., Karnadipa, T., & Putri, S. E. (2022). The Effect of Ultrasound Therapy and Muscle Energy Technique on a Case of a Young Adult with Thoracic Outlet Syndrome. Proceedings, 83(1), 55. https://doi.org/10.3390/proceedings2022083055