Respondent Profile
The authors’ first intervention treated the patient by a modality of ultrasound. patient was given physiotherapy for four evaluations. In this case, the authors used the VAS parameter to evaluate pain complaints from patients. Ultrasound can help relieve shoulder pain. Ultrasonic waves are generated by the piezoelectric effect resulting from the vibration of the crystals inside the probe. A continuous mode can warm the targeted tissue and tends to be used in chronic pain conditions [
8].
The combination of the intensity and duration of ultrasound can produce both thermal and nonthermal effects. The thermal effects of ultrasound are to increase tissue temperature, improves blood flow, increase extensibility of the tissue, and reduce the viscosity of fluid elements in the tissue, while the nonthermal effects accelerate tissue metabolism by promoting cellular permeability and ion transport. Ultrasound therapy reduces pain and muscle spasms and improves contractures of joints and injured tissues [
9].
Ultrasound increases the extensibility of the skin and muscles due to its thermal effect, which affects the viscoelasticity of the tissue and can decrease muscle spasms [
10]. When ultrasound is applied with the appropriate intensity and frequency, it increases the temperature in soft tissues with high protein density [
11].
Mustafa Aziz Yildirim et al., in the paper titled “Comparison of Ultrasound Therapy of Various Durations in the Treatment of Subacromial Impingement Syndrome”, conducted a study using ultrasound on patients with a painful shoulder; in group 1, the intensity of 1.5 W/cm
2 at 8 min was given, and in group 2, the intensity of 1.5 W/cm
2 for 4 min given was. Two groups used a 5 cm
2 transducer and a circular motion transducer. In addition, other modalities of therapy, such as TENS and infrared, are also given as well as exercise therapy. The frequency of use of the tool was five times per week. It was found that ultrasound could reduce pain and increase functionality in the shoulder. According to this study, an 8-min ultrasound was more effective than a 4-min ultrasound in reducing shoulder pain. In addition, it was reported that the use of ultrasound in combination with exercise therapy or other modalities can affect the reduction of shoulder pain [
11].
According to Rohit Aiyer et al. in the article titled “Therapeutic Ultrasound for Chronic Pain Management in Joints: A Systematic Review”, ultrasound in the shoulder is effective for reducing pain if certain exercises are included for the shoulder. Because, when compared with other modalities, ultrasound is a less effective modality in reducing pain. This paper recommends combining ultrasound with pregabalin for more effective therapy [
8].
According to research conducted by Pınar Doruk Analan et al. in the article titled “Effects of Therapeutic Ultrasound and Exercise on Pain, Function, and Isokinetic Shoulder Rotator Strength of Patients with Rotator Cuff Disease”, an intensity of 1.5 W/cm
2 in a transducer area of 4.7 cm
2 was applied around the glenohumeral joint using slow circular motions. In addition to administering ultrasound, this study also provided TENS and exercise therapy on the shoulder to reduce pain and limitations in shoulder ROM. The results showed that there was a significant reduction in pain. Due to its thermal effects, ultrasound stimulates the afferent nerve fibers and provides an analgesic effect with a gate control mechanism. After the gate control is stimulated, the substantia gelatinosa is activated, which stops pain from reaching the central nerve cells. The cause of the pain can nbe due to limited ROM or due to weakness in the shoulder muscles. If only ultrasound therapy is given it is not effective. Pain may be reduced if ultrasound is given with other exercises [
12].
According Katsuyuki Morishita et al. in the article titled “Effects of Therapeutic Ultrasound on Range of Motion and Stretch Pain”, ultrasound can reduce pain. In this study, continuous ultrasound was applied with an intensity of 1.0 W/cm
2 and a frequency of 3 MHz for 10 min. The transducer was placed on the right trapezius muscle with a stroke. It was found that there was a reduction in pain. This decrease could be due to the evaporative cooling of the ultrasound gel. Tissue affected by this cooling effect can experience decreased pain. Ultrasound was more effective if exercises associated with pain relief, such as stretching or ROM exercise were applied after ultrasound [
9].
According to research conducted by Xia Peng et al. in the paper “Effectiveness of Ultrasound Therapy for Myofascial Pain Syndrome: A Systematic Review and Meta-Analysis”, sensor change at the trigger and target levels have been studied extensively by detecting pain thresholds for both muscle and tissue. The overlying superficial layers (subcutaneous tissue and skin) are subjected to different stimuli that reduce pain. It was found that pain was reduced after using ultrasound modalities. The methods used in this paper were ultrasound mode parameters such as continuous and intermittent. The continuous type was more effective in reducing pain than the intermittent type, although the effect was only slight. In addition to administering an ultrasound, other exercises can be given to reduce the pain [
13].
Supporting the five articles above is the work of Elisa Lioce et al. in the study titled “Personalized Therapeutic Ultrasound in Shoulder Disease: Multimodal Assessment and Results”. In this study, an ultrasound was performed with the inclusion criteria of the patient having a clinical diagnosis of shoulder pain in the tendon/bursa/joint and the following exclusion criteria: patients with contraindications to ultrasound, who had neurological disease or deficits, or who were following pharmacological therapy. Ten patients met these criteria. Ultrasound was used in all patients at an intensity of 1.5 W/cm
2, and the transducer was moved against the skin in a circular motion. The choice of ultrasound frequency was very important. The frequency was 1 MHz for the deepest network and 3 MHz for the superficial part with continuous and intermittent types. Treatment time was 5 and 10 min. It was found that almost all patients experienced a decrease in pain and an increase in shoulder ROM. Only one patient had no reduction on the pain scale. This patient had rotator cuff tendinopathy and was younger than the other patients. Time spent on strenuous activities and overuse of the affected shoulder make ultrasound therapy unlikely to be effective in these patients. Therefore, in addition to the correct setting of frequency, intensity, and time, the effectiveness of ultrasound on shoulder pain can also be seen from the patient’s use of the painful shoulder. In addition, ultrasound, with the addition of other interventions, can overcome the condition of pain in the shoulder [
8].
The
Figure 1 shows the results of four patient evaluations using the visual analog scale parameters (VAS).
In this case study, after performing ultrasound twice a week for 5 min, at an intensity of 1.5 W/cm
2 as continuous type with a frequency of 1 MHz, positive results were obtained on the pain scale, namely a significant decrease because the patient was still using the sore shoulder to take part in strenuous activity, although not frequently. The results of the pain scale can be seen in
Figure 1. On the first evaluation, the patient had severe pain with VAS of 8. There was no reduction in pain on the second evaluation. In the third evaluation with the same procedure, there was a decrease in pain to VAS of 7 and in the fourth evaluation there was a decrease to VAS of 6. Constant pain in the second and fourth evaluations. In addition to using ultrasound, pain reduction was assisted by other exercises such as stretching in this case study.
The second intervention performed on the patient, in this case, was stretching with a stretching technique. Stretching is an exercise that forces changes in the musculotendinous structure to achieve a change in length. The purpose of stretching is to increase the range of motion (ROM), reduce stiffness or pain, and prepare for physical activity. Stretching to promote semi-permanent ROM repair largely depends on achieving “stretch tolerance” [
14].
According to Phil Page in the article titled “Current Concepts in Muscle Stretching For Exercise And Rehabilitation”, stretching can increase the flexibility and extensibility of the shoulder and the ROM of the shoulder joint. Stretching can align the collagen fibers in the muscle during healing. The increase in ROM is not due to the lengthening of the muscle but to an increase in stretch tolerance or the ability to withstand more muscle stretch. In addition, to be more effective before stretching, contract the muscles [
14].
According to Ozge Tahran, et al. in the article titled “Effects of Modified Posterior Shoulder Stretching Exercises on Shoulder Mobility, Pain, and Dysfunction in Patients With Subacromial Impingement Syndrome”, stretching is effective in increasing flexibility, ROM in the shoulder joint, and SPADI values. This occurs because the critical mass in the viscosity of the muscle–tendon unit decreases, so there is an increase in joint flexibility and ROM. In this article, stretching during internal rotation of the shoulder and external rotation of the shoulder found that there was the stretching of the capsule and glenohumeral ligament when stretching the internal rotation of the shoulder and stretching of the capsule and the posterior part of the deltoid muscle when moving adduction horizontally. Stretching increased locomotion in the glenohumeral joint and scapular kinematics by changing the size of the subacromial space [
15].
According to research by Ji Eun Kim et al. in the article titled “The Effect Of a Janda-based Stretching Program, Range of Motion, Muscular Strength, and Pain in Middle-aged Women With Self-reported Muscular Skeletal Symptoms”, treatment was given to relieve musculoskeletal pain by protecting tissues and maintaining good body alignment and recovery. It was found that regular stretching exercises could increase flexibility, ROM in the shoulder region, pelvic-lumbar stability, and muscle function in normal adults [
16].
According to research conducted by Nicole D. Harshbarger et al. in the article titled “The Effectiveness of Shoulder Stretching and Joint Mobilizations on Posterior Shoulder Tightness” in the internal glenohumeral rotation of the shoulder, there was a consistent increase in ROM due to the stretching intervention accompanied by joint mobilization of the shoulder. This combination could increase shoulder ROM in patients suffering from posterior shoulder tightness. Regular stretching reduces pain owing to limited ROM and muscle tightness [
17].
According to research by Carrie A. Rowlett et al. in the article titled “Efficacy of Instrument-Assisted Soft Tissue Mobilisation in Comparison to Gastrocnemius-Soleus Stretching for Dorsiflexion Range of Motion: A Randomised Controlled Trial”, between 15 and 30 min and more than 30 min durations resulted an increase in ankle dorsiflexion ROM. However, the duration is not a benchmark for the effectiveness of stretching if it is not performed correctly. When stretching is applied, the Golgi tendon organ plays a role in stretching the muscle from the muscle spindle, and then the sarcomere lengthens, and when it is released, the muscle contractile relaxes, which returns the sarcomere back to normal [
18].
Supporting the five articles above is the work of Ken Kusano et al. in the paper titled “Acute Effect and Time Course of Extension and Internal Rotation Stretching of the Shoulder on Infraspinatus Muscle Hardness”. The stretching position used was that the patient is positioned on their stomach and the shoulders were in an internal rotation and extension position, placed behind the back with the hands facing up. There is an increase in ROM after the stretching intervention after 20 s because there is flexibility; the technique of stretching, position, and duration can affect the effectiveness of stretching [
19].
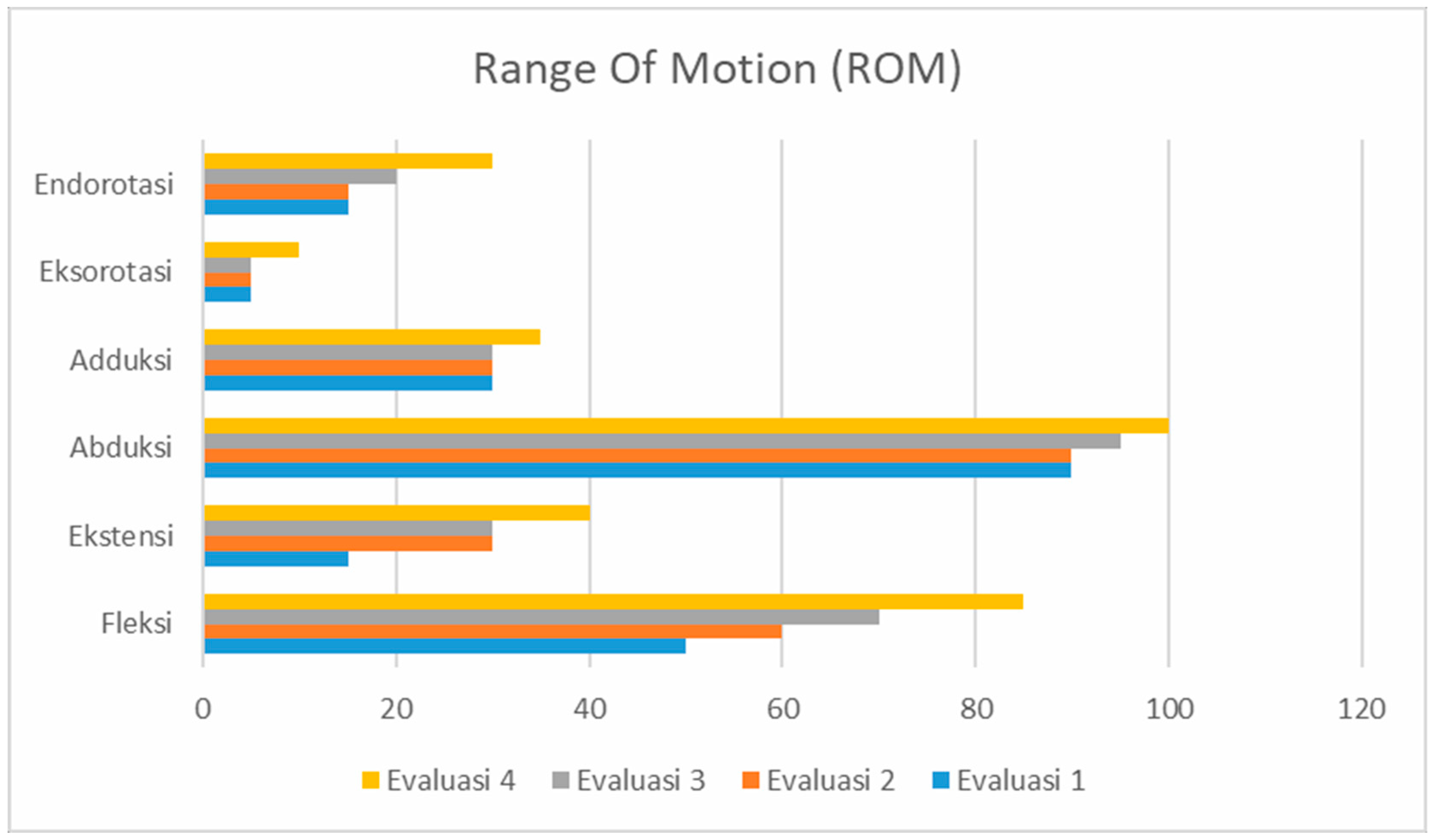
The
Figure 2 is the result of four patient evaluations using the range of motion (ROM) and SPADI parameters to strengthen the research.
After stretching for 5 to 10 min with a frequency of 2 times per week, for 10 repetitions with a count of 8 s, there was an increase in ROM, especially in shoulder flexion movements, because the functional ability to be improved in this case study is the ability to raise the hand. On the first evaluation, shoulder flexion movement is so limited that the patient cannot perform activities such as picking up objects in high places, or tying and combing hair. Up to the evaluation, four patients could raise their hands more than 80 degrees and perform self-care activities such as tying and combing hair and pick up objects in high places; although there are still limitations such as pain and compensatory movements, the condition of these patients is progressing.
ROM results can be seen in
Figure 2. As seen from the figure above, in the first therapy the right shoulder flexion movement of 50° in the second therapy increased to 60° and in the third and fourth therapy, the ROM increased to 70° and 85°. In the shoulder extension movement, the first therapy ROM was 15°. In the second therapy, the ROM increased to 30°. In the third therapy, the ROM remained the same as in the second therapy. Then in the fourth therapy, there was an increase in the ROM to 40°. In the shoulder abduction movement in the first therapy and the second therapy, there was no increase in the ROM, which was 90°; in the third therapy there was an increase in the ROM to 90°. In the fourth therapy, there was also an increase in ROM to 100°. In adduction movement, there was no increase in the ROM in the first, second, or third therapy; it was 30°. In the fourth therapy, there was an increase in ROM to 35°. For exorotation, the first, second, and third therapy constant ROM was 5°; in the fourth therapy, there was an increase in ROM to 10°. For endorotation, there was no increase in ROM from the first to the second therapy, which was 15°. In the third therapy, there was an increase in the ROM to 20°, and in the fourth therapy, there was an increase in ROM to 40°.
In this case study, it can be seen that decreasing pain scale and increasing ROM can decrease SPADI values, as seen in
Figure 3.
As seen from the figure above, there is an increase in SPADI from the first evaluation, 67%, then in the second evaluation to 64%. In the third evaluation there was no increase or decrease. In the last evaluation, there was a drastic increase, namely to 53%. When there is a decrease in pain and there is an increase in the ROM, it can reduce the SPADI value.
In addition to the intervention the author provides in this case study, the author also provides a home program to patients, namely stretching independently at home. After four physiotherapy evaluations (14 February 2020, 20 February 2020, 24 February 2020, and 5 March 2020) following interventions given to patients, improvement in the patients’ conditions was observed. This was evidenced by a decrease in shoulder pain from 8 to 7, an increase in ROM in the shoulder region, and a decrease in SPADI values.






{kind=link}
{kind=link}
{kind=link}