The Communication of Health Knowledge in Social Media under the Special Chinese Culture Context: The Moderating Effect of Loss of Face †


Abstract
:1. Introduction
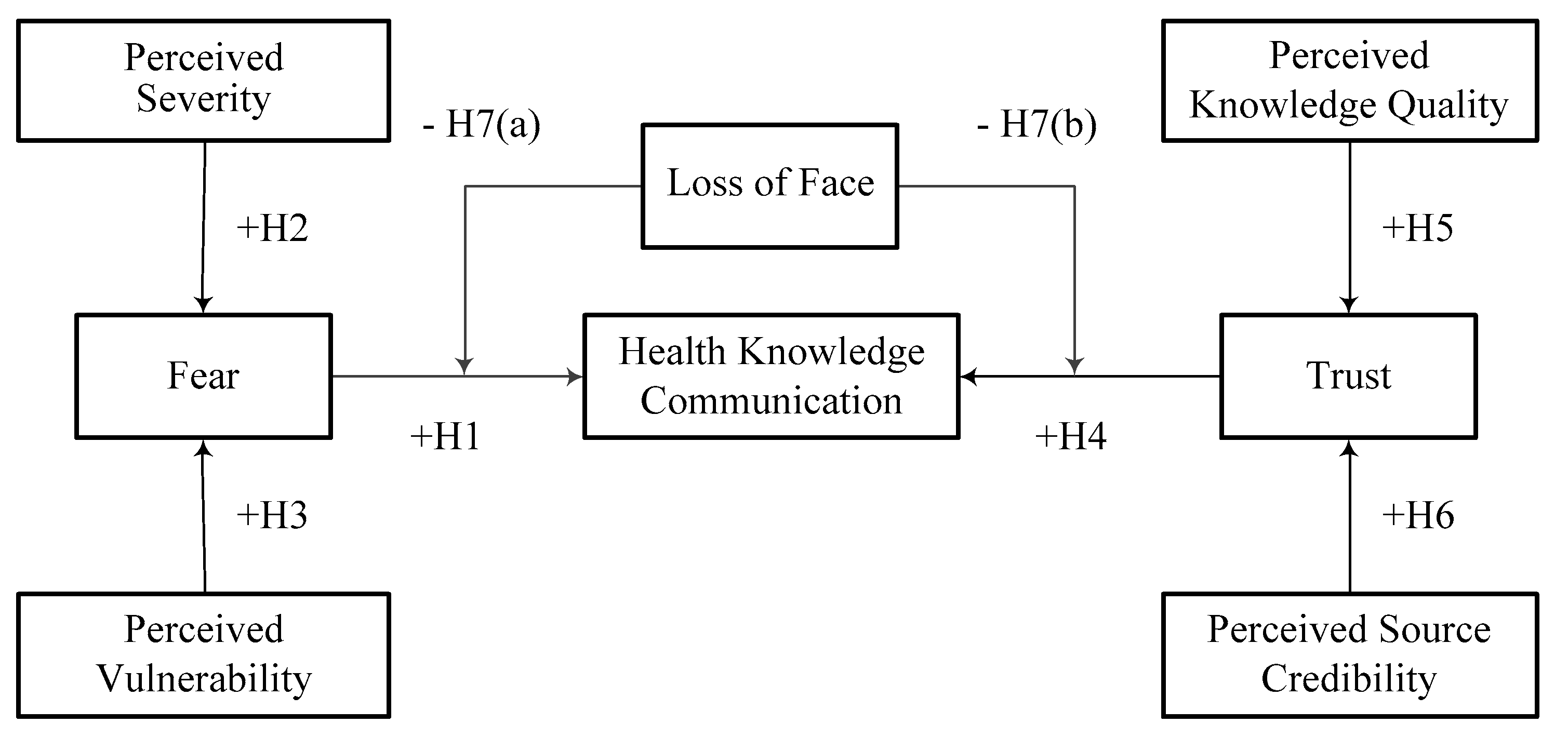
2. Theoretical Background and Hypothesis Development
2.1. Fear Communication
2.2. Trust Communication
2.3. Face Communication
3. Research Methodology
3.1. Measurement Development
3.2. Data Collection and Descriptive Analysis
4. Measurement Model
4.1. Reliability and Convergent Validity Analysis
4.2. Discriminant ValidityAnalysis
4.3. Common Method Bias
5. Results
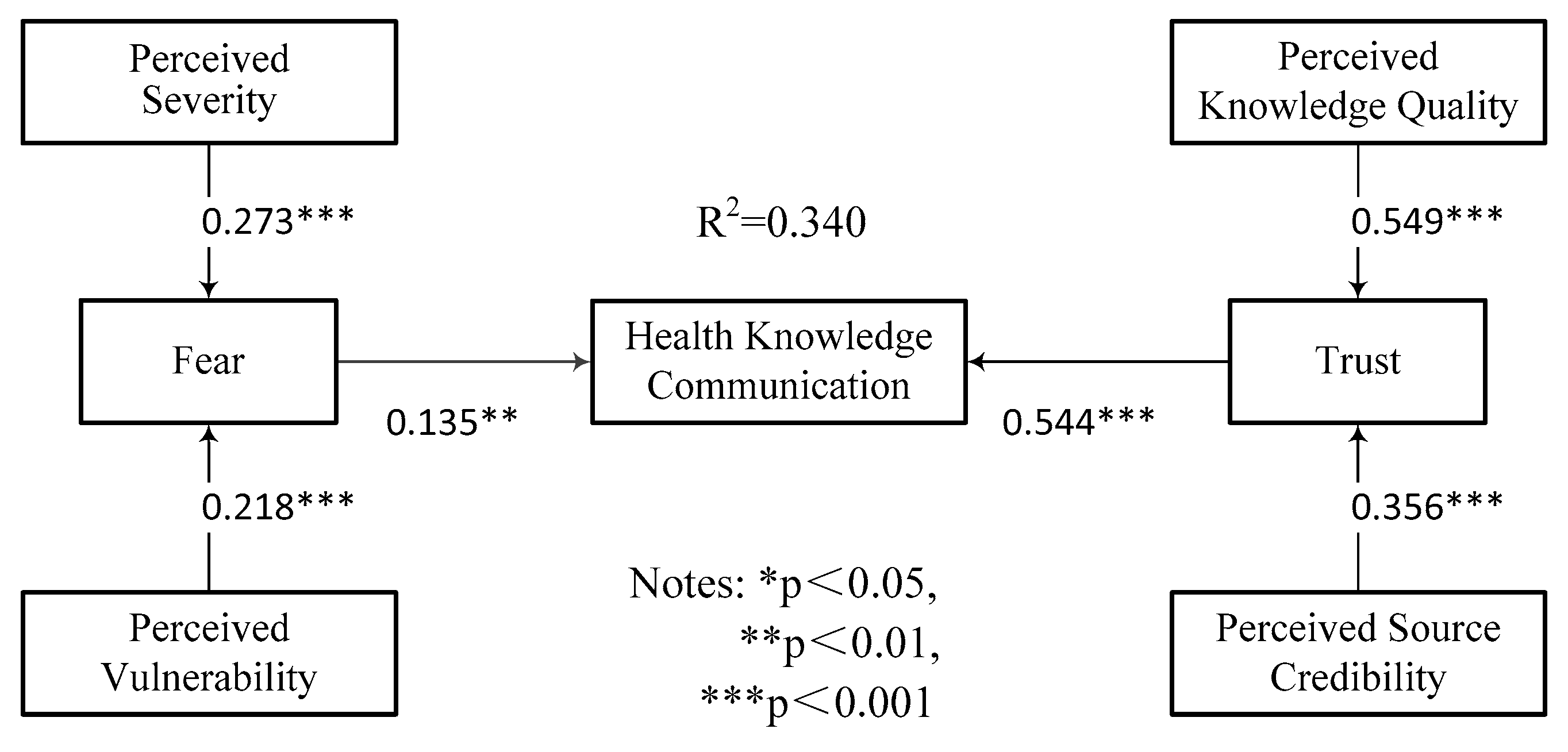
5.1. Testing of the Structure Model
5.2. Testing of the Moderating Effect
6. Discussion and Limitations
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Moorhead, S.A.; Hazlett, D.E.; Harrison, L.; Carroll, J.K.; Irwin, A.; Hoving, C. A new dimension of health care: Systematic review of the uses, benefits, and limitations of social media for health communication. J. Med. Int. Res. 2013, 15, 1106–1112. [Google Scholar] [CrossRef] [PubMed]
- Karlsen, R.; BorrásMorell, J.E.; Fernández, L.L.; Traver, S.V. A domain-based approach for retrieving trustworthy health videos from YouTube. Stud. Health Technol. Inform. 2013, 192, 1008. [Google Scholar] [PubMed]
- Barrelet, C.; Bourrier, M.; Burton-Jeangros, C.; Schindler, M. Unresolved issues in risk communication research: The case of the H1N1 pandemic (2009–2011). Influenza Other Respir. Viruses 2013, 7, 114–119. [Google Scholar] [CrossRef] [PubMed]
- Shigemura, J.; Harada, N.; Tanichi, M.; Nagamine, M.; Shimizu, K.; Katsuda, Y.; Tokuno, S.; Tsumatori, G.; Yoshino, A. Rumor-related and exclusive behavior coverage in internet news reports following the 2009 H1N1 influenza outbreak in Japan. Disaster Med. Public Health Prep. 2015, 9, 459–463. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.P.; Chen, J.; Wei, J. Tie Strength, Context Openness and Sharing Intention of Self-Deprecating Information. Chin. J. Manag. 2016, 13, 131–137. (In Chinese) [Google Scholar]
- Chua, A.Y.; Banerjee, S. Analyzing Users’ Trust for Online Health Rumors. In Proceedings of the International Conference on Asia-Pacific Digital Libraries, Seoul, Korea, 9–12 December 2015; pp. 33–38. [Google Scholar]
- Difonzo, N. Rumour research can douse digital wildfires. Nature 2013, 493, 135. [Google Scholar] [CrossRef]
- Boss, S.R.; Galletta, D.F.; Lowry, P.B.; Moody, G.D.; Polak, P. What do systems users have to fear? Using fear appeals to engender threats and fear that motivate protective security behaviors. MIS Q. 2015, 39, 837–864. [Google Scholar] [CrossRef]
- Dillard, J.P.; Plotnick, C.A.; Godbold, L.C.; Freimuth, V.S.; Edgar, T. The multiple affective outcome of aids psas: Fear appeals do more than scare people. Commun. Res. 1996, 23, 44–72. [Google Scholar] [CrossRef]
- Hoog, N.D.; Stroebe, W.; Wit, J.D. The impact of vulnerability to and severity of a health risk on processing and acceptance of fear-arousing communications: A meta-analysis. Rev. Gen. Psychol. 2007, 11, 258–285. [Google Scholar] [CrossRef]
- May, T. Public communication, risk perception, and the viability of preventive vaccination against communicable diseases. Bioethics 2005, 19, 407–421. [Google Scholar] [CrossRef]
- De Groot, J.H.B.; Semin, G.R.; Smeets, M.A.M. I can see, hear, and smell your fear: Comparing olfactory and audiovisual media in fear communication. J. Exp. Psychol. Gen. 2014, 143, 825–834. [Google Scholar] [CrossRef] [PubMed]
- Kasmaei, P.; Shokravi, F.A.; Hidarnia, A.; Hajizadeh, E.; Atrkar-Roushan, Z.; Shirazi, K.K.; Montazeri, A. Brushing behavior among young adolescents: Does perceived severity matter. BMC Public Health 2014, 14, 25. [Google Scholar] [CrossRef]
- Tamang, A.; Nepal, B.; Puri, M.; Shrestha, D. Sexual behaviour and risk perceptions among young men in border towns of Nepal. Asia Pac. Popul. J. 2001, 16, 195–210. [Google Scholar] [CrossRef]
- Nau, D.P.; Ellis, J.J.; Kline-Rogers, E.M.; Mallya, U.; Eagle, K.A.; Erickson, S.R. Gender and perceived severity of cardiac disease: Evidence that women are “tougher”. Am. J. Med. 2005, 118, 1256–1261. [Google Scholar] [CrossRef]
- Chen, L.M.; Cheng, Y.Y.; Wang, W.C.; Hsueh, C.W. The intersection between perceived severity and frequency of being bullied: A rasch measurement approach. Educ. Psychol. 2015, 35, 397–415. [Google Scholar] [CrossRef]
- Em, V.D.S.; de Wit, J.B.; Götz, H.M.; Mulder, P.G.; Neumann, M.H.; Wi, V.D.M. Incidence of sexually transmitted diseases and HIV infection in men who have sex with men related to knowledge, perceived susceptibility, and perceived severity of sexually transmitted diseases and HIV infection: Dutch MSM-Cohort Study. Sex. Transm. Dis. 2006, 33, 193–198. [Google Scholar]
- Wild, T.C.; Cunningham, J. Psychosocial determinants of perceived vulnerability to harm among adult drinkers. J. Stud. Alcohol 2001, 62, 105–113. [Google Scholar] [CrossRef]
- Hong, H. An extension of the extended parallel process model (EPPM) in television health news: The influence of health consciousness on individual message processing and acceptance. Health Commun. 2001, 26, 343–353. [Google Scholar] [CrossRef]
- Schoorman, F.D.; Mayer, R.C.; Davis, J.H. An integrative model of organizational trust: Past, present, and future. Acad. Manag. Rev. 2007, 32, 344–354. [Google Scholar] [CrossRef]
- Pavlou, P.A. Consumer acceptance of electronic commerce: Integrating trust and risk with the technology acceptance model. Int. J. Electron. Commer. 2003, 7, 101–134. [Google Scholar]
- McEvily, B.; Perrone, V.; Zaheer, A. Trust as an organizing principle. Organ. Sci. 2003, 14, 91–103. [Google Scholar] [CrossRef]
- Pace, C.S.; Martini, P.S.; Zavattini, G.C. The factor structure of the inventory of parent and peer attachment (IPPA): A survey of Italian adolescents. Personal. Individ. Differ. 2011, 51, 83–88. [Google Scholar] [CrossRef]
- Dong, K.Y. Substructures of perceived knowledge quality and interactions with knowledge sharing and innovativeness: A sensemaking perspective. J. Knowl. Manag. 2014, 18, 523–537. [Google Scholar]
- Dong, K.Y.; Vonderembse, M.A.; Ragunathan, T.S. Knowledge quality: Antecedents and consequence in project teams. J. Knowl. Manag. 2011, 15, 329–343. [Google Scholar]
- Tormala, Z.L.; Briñol, P.; Petty, R.E. When credibility attacks: The reverse impact of source credibility on persuasion. J. Exp. Soc. Psychol. 2006, 42, 684–691. [Google Scholar] [CrossRef]
- Chou, C.H.; Wang, Y.S.; Tang, T.I. Exploring the determinants of knowledge adoption in virtual communities: A social influence perspective. Int. J. Inf. Manag. 2015, 35, 364–376. [Google Scholar] [CrossRef]
- Major, L.H.; Coleman, R. Source credibility and evidence format: Examining the effectiveness of HIV/AID messages for young African Americans. J. Health Commun. 2012, 17, 515–531. [Google Scholar] [CrossRef]
- Ho, Y.F. On the concept of face. Am. J. Sociol. 1976, 81, 867–890. [Google Scholar] [CrossRef]
- Sue, S.; Morishima, J.K. The Mental Health of Asian Americans; Jossey-Bass: San Francisco, CA, USA, 1982; Volume 154, pp. 165–178. [Google Scholar]
- Zwaard, R.V.D.; Bannink, A. Video call or chat? Negotiation of meaning and issues of face in telecollaboration. System 2014, 4, 137–148. [Google Scholar] [CrossRef]
- Park, C.Y.; Park, H.S.; Lee, S.Y.; Moon, S. Sexual harassment in Korean college classrooms: How self-construal and gender affect students’ reporting behavior. Gend. Place Cult. 2013, 20, 432–450. [Google Scholar] [CrossRef]
- Napper, L.E.; Grimaldi, E.M.; Labrie, J.W. Parents’ and students’ perceptions of college alcohol risk: The role of parental risk perception in intentions to communicate about alcohol. Addict. Behav. 2014, 42, 114–118. [Google Scholar] [CrossRef] [PubMed]
- Tyc, V.L.; Lensing, S.; Rai, S.N.; Klosky, J.L.; Stewart, D.B.; Gattuso, J. Predicting perceived vulnerability to tobacco-related health risks and future intentions to use tobacco among pediatric cancer survivors. Patient Educ. Couns. 2006, 62, 198–204. [Google Scholar] [CrossRef] [PubMed]
- Cazier, J.A.; Shao, B.B.M.; Louis, R.D.S. Sharing information and building trust through value congruence. Inf. Syst. Front. 2007, 9, 515–529. [Google Scholar] [CrossRef]
- Awad, N.F.; Ragowsky, A. Establishing trust in electronic commerce through online word of mouth: An examination across genders. J. Manag. Inf. Syst. 2008, 24, 101–121. [Google Scholar] [CrossRef]
- Lee, M.K.O.; Rabjohn, N.; Cheung, C.M.K. The impact of electronic word-of-mouth: The adoption of online opinions in online customer communities. Internet Res. Electron. Netw. Appl. Policy 2008, 18, 229–247. [Google Scholar]
- Citrin, A.V. Information Quality Perceptions: The Role of Communication Media Characteristics. Ph.D. Thesis, Washington State University, Pullman, WA, USA, 2001; pp. 118–132. [Google Scholar]
- Zane, N.; Yeh, M. The Use of Culturally-Based Variables in Assessment: Studies on Loss of Face. In Asian American Mental Health; Springer: New York, NY, USA, 2002; pp. 123–138. [Google Scholar]
- Mak, W.W.S.; Chen, S.X.; Lam, A.G.; Yiu, V.F.L. Understanding distress the role of face concern among Chinese Americans, European Americans, Hong Kong Chinese, and mainland Chinese. Couns. Psychol. 2008, 37, 219–248. [Google Scholar] [CrossRef]
- Fornell, C.; Larcker, D.F. Evaluating structural equation models with unobservable variables and measurement error. J. Mark. Res. 1981, 18, 39–50. [Google Scholar] [CrossRef]
- Podsakoff, P.M.; Mackenzie, S.B.; Lee, J.Y.; Podsakoff, N.P. Common method biases in behavioral research: A critical review of the literature and recommended remedies. J. Appl. Psychol. 2003, 8, 879–903. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Range | Number | Percentage(%) | |
|---|---|---|---|---|
| Gender | Male | 132 |  | 40.1 |
| Female | 197 | 59.9 | ||
| Age | 18 below | 3 |  | 0.9 |
| 18~25 | 201 | 61.1 | ||
| 26~30 | 103 | 31.3 | ||
| 31~40 | 15 | 4.6 | ||
| 41~50 50 above | 6 1 | 1.8 0.3 | ||
| Income level | 1000 below | 131 |  | 39.8 |
| 1000~3000 | 79 | 24.0 | ||
| 3001~5000 | 28 | 8.5 | ||
| 5001~7000 | 24 | 7.3 | ||
| 7001~10,000 | 38 | 11.6 | ||
| 10,000 above | 29 | 8.8 | ||
| Variables | Items | Loadings | Cronbach’sAlphas | CR | AVE |
|---|---|---|---|---|---|
| Perceived Severity | PES1 | 0.967 | 0.968 | 0.9791 | 0.9398 |
| PES2 | 0.979 | ||||
| PES3 | 0.963 | ||||
| Perceived Vulnerability | PEV1 | 0.952 | 0.9352 | 0.9586 | 0.8854 |
| PEV2 | 0.924 | ||||
| PEV3 | 0.947 | ||||
| Fear | FEA1 | 0944 | 0.9526 | 0.9694 | 0.9134 |
| FEA2 FEA3 | 0.955 0.968 | ||||
| Perceived Knowledge Quality | PKQ1 | 0.844 | 0.9292 | 0.9441 | 0.7383 |
| PKQ2 PKQ3 PKQ4 PKQ5 PKQ6 | 0.896 0.848 0.788 0.879 0.895 | ||||
| Perceived Source Credibility | PSC1 | 0.914 | 0.9301 | 0.9503 | 0.8271 |
| PSC2 PSC3 PSC4 | 0.868 0.920 0.936 | ||||
| Trust | TRU1 | 0.966 | 0.9588 | 0.9733 | 0.9238 |
| TRU2 TRU3 | 0.957 0.961 | ||||
| Loss of Face | LOF1 LOF2 | 0.777 0.834 | 0.751 | 0.8567 | 0.6662 |
| LOF3 LOF4 | 0.837 0.754 | ||||
| Health Knowledge Communication | HKC1 | 0.969 | 0.9596 | 0.9738 | 0.9252 |
| HKC2 | 0.957 | ||||
| HKC3 | 0.960 |
| PES | PEV | FEA | PKQ | PSC | TRU | LOF | HKC | |
|---|---|---|---|---|---|---|---|---|
| PES | 0.9694 | |||||||
| PEV | 0.4609 | 0.9410 | ||||||
| FEA | 0.3729 | 0.3432 | 0.9557 | |||||
| PKQ | 0.4718 | 0.3488 | 0.2309 | 0.8592 | ||||
| PSC | 0.3648 | 0.2865 | 0.1613 | 0.6195 | 0.9095 | |||
| TRU | 0.4300 | 0.2692 | 0.1831 | 0.6459 | 0.6676 | 0.9611 | ||
| LOF | 0.3644 | 0.1866 | 0.2023 | 0.1983 | 0.1624 | 0.1738 | 0.8162 | |
| HKC | 0.3292 | 0.2363 | 0.2341 | 0.5626 | 0.5361 | 0.5682 | 0.1334 | 0.9619 |
| Hypothesis | Model 1 | Model 2 | Model 2A | Model 2B | Result | |
|---|---|---|---|---|---|---|
| Main Effect | H1:FEA→HKC | 0.135 ** | 0.132 ** | 0.086 ns | 0.114 * | Supported |
| H2:PES→FEA | 0.273 *** | 0.273 *** | 0.273 *** | 0.273 *** | Supported | |
| H3:PEV→FEA | 0.218 *** | 0.218 *** | 0.218 *** | 0.218 *** | Supported | |
| H4:TRU→HKC | 0.544 *** | 0.542 *** | 0.543 *** | 0.914 *** | Supported | |
| H5:PKQ→TRU | 0.549 *** | 0.549 *** | 0.549 *** | 0.549 *** | Supported | |
| H6:PSC→TRU | 0.356 *** | 0.356 *** | 0.356 *** | 0.356 *** | Supported | |
| LOF→HKC | 0.012 ns | −0.042 ns | 0.291 * | |||
| Interaction Effect | H7a:FEA × LOF→HKC | 0.082 ns | Not Supported | |||
| H7b:TRU × LOF→HKC | −0.519 ** | Supported | ||||
| Model Evaluation | R2 | 0.340 | 0.340 | 0.340 | 0.367 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ma, F.; Huo, C. The Communication of Health Knowledge in Social Media under the Special Chinese Culture Context: The Moderating Effect of Loss of Face. Proceedings 2017, 1, 150. https://doi.org/10.3390/IS4SI-2017-03997
Ma F, Huo C. The Communication of Health Knowledge in Social Media under the Special Chinese Culture Context: The Moderating Effect of Loss of Face. Proceedings. 2017; 1(3):150. https://doi.org/10.3390/IS4SI-2017-03997
Chicago/Turabian StyleMa, Feicheng, and Chaoguang Huo. 2017. "The Communication of Health Knowledge in Social Media under the Special Chinese Culture Context: The Moderating Effect of Loss of Face" Proceedings 1, no. 3: 150. https://doi.org/10.3390/IS4SI-2017-03997
APA StyleMa, F., & Huo, C. (2017). The Communication of Health Knowledge in Social Media under the Special Chinese Culture Context: The Moderating Effect of Loss of Face. Proceedings, 1(3), 150. https://doi.org/10.3390/IS4SI-2017-03997