


Investigation of Upper Respiratory Carriage of Bacterial Pathogens among University Students in Kampar, Malaysia

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population, Design and Procedures
2.2. Swab Culture for Target Bacteria
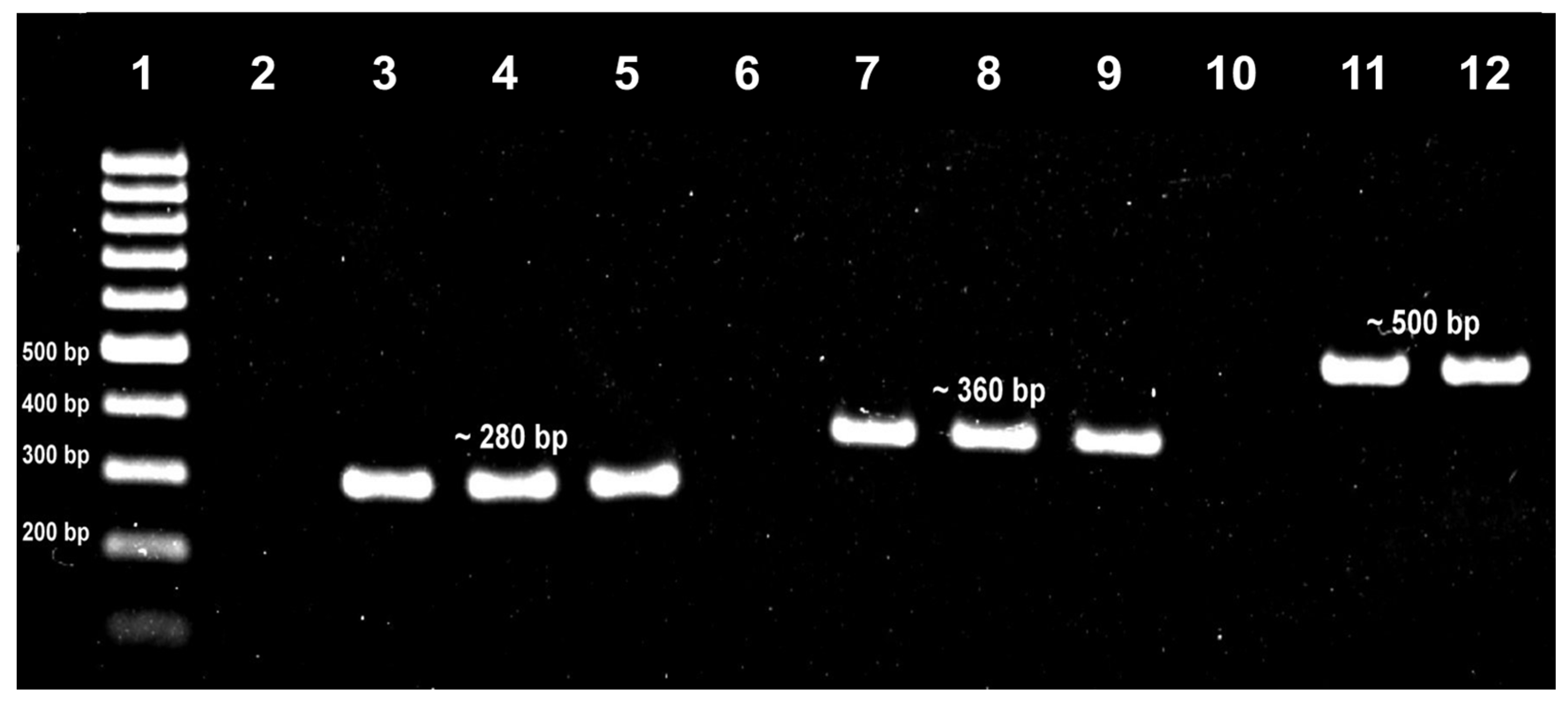
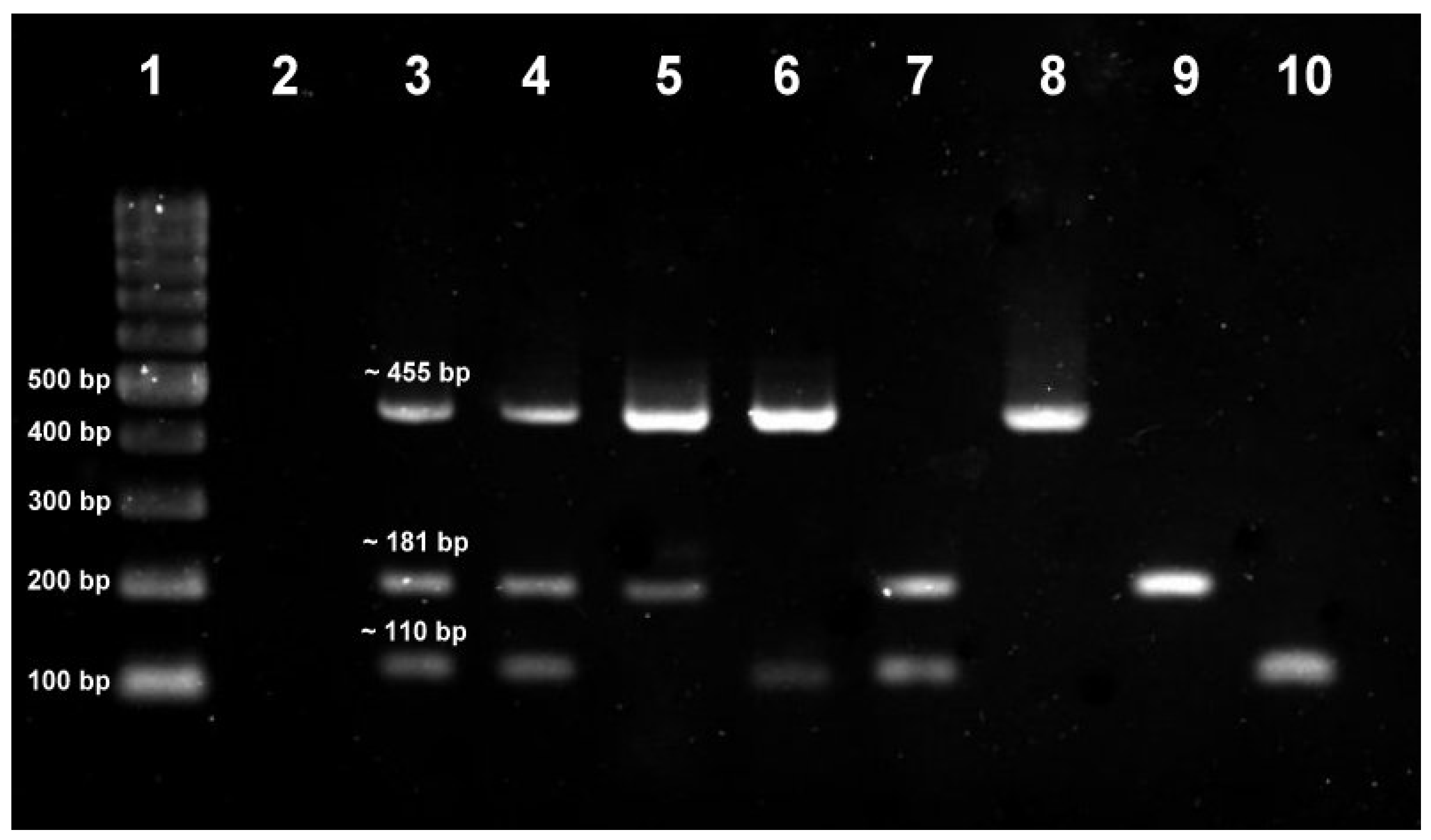
2.3. PCR Identification of Target Bacteria from Swab Cultures
2.4. Antibiotic Susceptibility Assessment of ESKAPE Target Bacteria
2.5. Data Analysis
3. Results
3.1. Subject Demographic and Health-Related Profiles
3.2. Carriage Prevalence of Target Bacteria
3.3. Bacterial Carriage by URT Sites
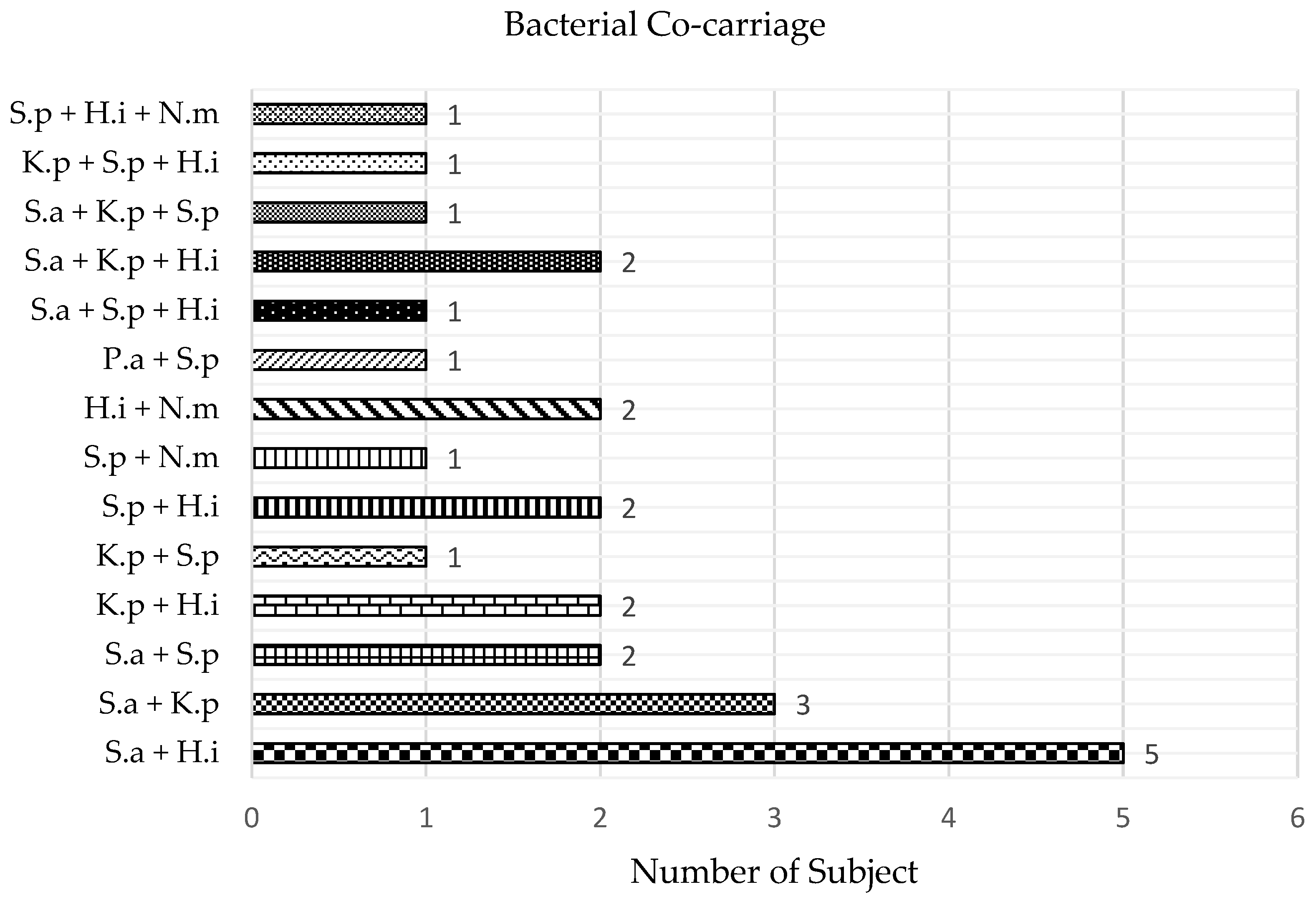
3.4. Bacterial Co-Carriage
3.5. Association between Bacterial Carriage and Host Factors
3.6. Antibiotic Susceptibility of ESKAPE Target Bacteria
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- García-Rodríguez, J.Á.; Martínez, M.J.F. Dynamics of nasopharyngeal colonization by potential respiratory pathogens. J. Antimicrob. Chemother. 2002, 50, 59–74. [Google Scholar] [CrossRef]
- Kumpitsch, C.; Koskinen, K.; Schöpf, V.; Moissl-Eichinger, C. The microbiome of the upper respiratory tract in health and disease. BMC Biol. 2019, 17, 87. [Google Scholar] [CrossRef]
- Cleary, D.W.; Clarke, S.C. The nasopharyngeal microbiome. Emerg. Top. Life Sci. 2017, 1, 297–312. [Google Scholar] [PubMed]
- Ghssein, G.; Ezzeddine, Z. The key element role of metallophores in the pathogenicity and virulence of Staphylococcus aureus: A Review. Biology 2022, 11, 1525. [Google Scholar] [CrossRef] [PubMed]
- Ghssein, G.; Ezzeddine, Z. A review of Pseudomonas aeruginosa metallophores: Pyoverdine, pyochelin and pseudopaline. Biology 2022, 11, 1711. [Google Scholar] [CrossRef]
- Tsang, R.S.W. A narrative review of the molecular epidemiology and laboratory surveillance of vaccine preventable bacterial meningitis agents: Streptococcus pneumoniae, Neisseria meningitidis, Haemophilus influenzae and Streptococcus agalactiae. Microorganisms 2021, 9, 449. [Google Scholar] [CrossRef]
- Martin, R.M.; Bachman, M.A. Colonization, infection, and the accessory genome of Klebsiella pneumoniae. Front. Cell Infect. Microbiol. 2018, 8. [Google Scholar] [CrossRef] [PubMed]
- Clark, S.C. Commensal bacteria in the upper respiratory tract regulate susceptibility to infection. Curr. Opin. Immunol. 2020, 66, 42–49. [Google Scholar] [CrossRef]
- Haak, B.W.; Brands, X.; Davids, M.; Peters-Sengers, H.; Kullberg, R.F.J.; van Houdt, R.; Hugenholtz, F.; Faber, D.R.; Zaaijer, H.L.; Scicluna, B.P.; et al. Bacterial and viral respiratory tract microbiota and host characteristics in adults with lower respiratory tract infections: A case-control study. Clin. Infect. Dis. 2022, 74, 776–784. [Google Scholar] [CrossRef]
- Feldman, C.; Anderson, R. Meningococcal pneumonia: A review. Pneumonia 2019, 11, 3. [Google Scholar] [CrossRef]
- Claassen-Weitz, S.; Lim, K.Y.L.; Mullally, C.; Zar, H.J.; Nicol, M.P. The association between bacteria colonizing the upper respiratory tract and lower respiratory tract infection in young children: A systematic review and meta-analysis. Clin. Microbiol. Infect. 2021, 27, 1262–1270. [Google Scholar] [CrossRef]
- Subramanian, K.; Henriques-Normark, B.; Normark, S. Emerging concepts in the pathogenesis of the Streptococcus pneumoniae: From nasopharyngeal colonizer to intracellular pathogen. Cell Microbiol. 2019, 21, e13077. [Google Scholar] [CrossRef]
- Coughtrie, A.L.; Whittaker, R.N.; Begum, N.; Anderson, R.; Tuck, A.; Faust, S.; Jefferies, J.M.; Yuen, H.M.; Roderick, P.J.; A Mullee, M.; et al. Evaluation of swabbing methods for estimating the prevalence of bacterial carriage in the upper respiratory tract: A cross sectional study. BMJ Open 2014, 4, e005341. [Google Scholar] [CrossRef] [PubMed]
- Brown, A.F.; Leech, J.M.; Rogers, T.R.; McLoughlin, R.M. Staphylococcus aureus colonization: Modulation of host immune response and impact on human vaccine design. Front. Immunol. 2014, 8, 507. [Google Scholar] [CrossRef]
- Bogaert, D.; de Groot, R.; Hermans, P.W.M. Streptococcus pneumoniae colonisation: The key to pneumococcal disease. Lancet Infect. Dis. 2004, 4, 144–154. [Google Scholar] [CrossRef] [PubMed]
- Christensen, H.; May, M.; Bowen, L.; Hickman, M.; Trotter, C. Meningococcal carriage by age: A systematic review and meta-analysis. Lancet Infect. Dis. 2010, 10, 853–861. [Google Scholar] [CrossRef]
- Schenck, L.P.; Surette, M.G.; Bowdish, D.M. Composition and immunological significance of the upper respiratory tract microbiota. FEBS Lett. 2016, 590, 3705–3720. [Google Scholar] [CrossRef]
- Pettigrew, M.M.; Gent, J.F.; Revai, K.; Patel, J.A.; Chonmaitree, T. Microbial interactions during upper respiratory tract infections. Emerg. Infect. Dis. 2008, 14, 1584–1591. [Google Scholar] [CrossRef]
- McNeil, H.C.; Clarke, S.C. Serotype prevalence of Streptococcus pneumoniae in Malaysia—The need for carriage studies. Med. J. Malays. 2016, 71, 134–138. [Google Scholar]
- Bhatta, D.R.; Hamal, D.; Shrestha, R.; Parajuli, R.; Baral, N.; Subramanya, S.H.; Nayak, N.; Gokhale, S. Nasal and pharyngeal colonization by bacterial pathogens: A comparative study between preclinical and clinical sciences medical students. Can. J. Infect. Dis. Med. Microbiol. 2018, 2018, 7258672. [Google Scholar] [CrossRef] [PubMed]
- Peterson, M.E.; Mile, R.; Li, Y.; Nair, H.; Kyaw, M.H. Meningococcal carriage in high-risk settings: A systematic review. Int. J. Infect. Dis. 2018, 73, 109–117. [Google Scholar] [CrossRef]
- Nordin, S.A.; Za’im, N.A.N.; Sahari, N.N.; Jamaluddin, S.F.; Ahmadi, S.; Desa, M.N.M. Staphylococcus aureus nasal carriers among medical students in a medical school. Med. J. Malays. 2012, 67, 636–638. [Google Scholar]
- Zuridah, H.; Wirdatul, N.M.K.; Rashidah, S.; Evana, K.; Ahmad, N.M.R.; Siti, A.B.; Zakri, A.H.Z.; Izham, N.S.A.S. Carriage patterns and susceptibility testing of Staphylococcus aureus in healthy nasal carriers in UiTM. Biohealth Sci. Bull. 2011, 3, 29–36. [Google Scholar]
- Fong, I.L.; Abdul, R.E.E.; Tham, J.J.M.; Safian, N.A.; Ong, S.T.; Ng, P.P.; Hazmi, H. Prevalence and antibiotic sensitivity profiles of Staphylococcus aureus nasal carriage among preclinical and clinical medical students in a Malaysian university. Malays. J. Microbiol. 2018, 14, 351–355. [Google Scholar]
- Le, C.F.; Jefferies, J.M.; Yusof, M.Y.M.; Sekaran, S.D.; Clarke, S. The epidemiology of pneumococcal carriage and infections in Malaysia. Expert Rev. Anti-Infect. Ther. 2012, 10, 707–719. [Google Scholar] [CrossRef]
- Malik, A.S.; Ismail, A.; Pennie, R.A.; Naidu, J.V. Susceptibility pattern of Streptococcus pneumoniae among pre-school children in Kota Bharu, Malaysia. J. Trop. Pediatr. 1998, 44, 10–14. [Google Scholar] [CrossRef]
- Cleary, D.W.; Morris, D.E.; Anderson, R.A.; Jones, J.; Alattraqchi, A.G.; Rahman, N.I.A.; Ismail, S.; Razali, M.S.; Amin, R.M.; Aziz, A.A.; et al. The upper respiratory tract microbiome of indigenous Orang Asli in north-eastern Peninsular Malaysia. npj Biofilms Microbiomes 2021, 7, 1. [Google Scholar] [CrossRef]
- Morris, D.E.; on behalf of the MYCarriage group; McNeil, H.; Hocknell, R.E.; Anderson, R.; Tuck, A.C.; Tricarico, S.; Norazmi, M.N.; Lim, V.; Siang, T.C.; et al. Carriage of upper respiratory tract pathogens in rural communities of Sarawak, Malaysian Borneo. Pneumonia 2021, 13, 6. [Google Scholar] [CrossRef] [PubMed]
- Lister, A.J.J.; Le, C.F.; Cheah, E.S.G.; Desa, M.N.M.; Cleary, D.W.; Clarke, S.C. Serotype distribution of invasive, non-invasive and carried Streptococcus pneumoniae in Malaysia: A meta-analysis. Pneumonia 2021, 13, 9. [Google Scholar] [CrossRef]
- Dean, A.G.; Arner, T.G.; Sunki, G.G.; Friedman, R.; Lantinga, M.; Sangam, S.; Zubieta, J.C.; Sullivan, K.M.; Brendel, K.A.; Gao, Z.; et al. Epi Info™, Version 7.2.2.6; A Database and Statistics Program for Public Health Professionals; CDC: Atlanta, GA, USA, 2011.
- Satzke, C.; Turner, P.; Virolainen-Julkunen, A.; Adrian, P.V.; Antonio, M.; Hare, K.M.; Henao-Restrepo, A.M.; Leach, A.J.; Klugman, K.P.; Porter, B.D.; et al. Standard method for detecting upper respiratory carriage of Streptococcus pneumoniae: Updated recommendations from the World Health Organization Pneumococcal Carriage Working Group. Vaccine 2013, 32, 165–179. [Google Scholar] [CrossRef]
- Xirogianni, A.; Tzanakaki, G.; Karagianni, E.; Markoulatos, P.; Kourea-Kremastinou, J. Development of a single-tube polymerase chain reaction assay for the simultaneous detection of Haemophilus influenzae, Pseudomonas aeruginosa, Staphylococcus aureus, and Streptococcus spp. directly in clinical samples. Diagn. Microbiol. Infect. Dis. 2009, 63, 121–126. [Google Scholar] [CrossRef] [PubMed]
- Thong, K.L.; Lai, M.Y.; Teh, C.S.J.; Chua, K.H. Simultaneous detection of methicillin-resistant Staphylococcus aureus, Acinetobacter baumannii, Escherichia coli, Klebsiella pneumoniae and Pseudomonas aeruginosa by multiplex PCR. Trop. Biomed. 2011, 28, 21–31. [Google Scholar] [PubMed]
- Jiang, L.X.; Ren, H.Y.; Zhou, H.J.; Zhao, S.H.; Hou, B.Y.; Yan, J.P.; Qin, T.; Chen, Y. Simultaneous detection of 13 key bacterial respiratory pathogens by combination of multiplex PCR and capillary electrophoresis. Biomed. Environ. Sci. 2017, 30, 549–561. [Google Scholar] [PubMed]
- Lee, C.-T.; Hsiao, K.-M.; Chen, J.-C.; Su, C.-C. Multiplex polymerase chain reaction assay developed to diagnose adult bacterial meningitis in Taiwan. APMIS 2015, 123, 945–950. [Google Scholar] [CrossRef] [PubMed]
- Tzanakaki, G.; Tsopanomichalou, M.; Kesanopoulos, K.; Matzourani, R.; Sioumala, M.; Tabaki, A.; Kremastinou, J. Simultaneous single-tube PCR assay for the detection of Neisseria meningitidis, Haemophilus influenzae type b and Streptococcus pneumoniae. Clin. Microbiol. Infect. 2005, 11, 386–390. [Google Scholar] [CrossRef]
- CLSI. Performance Standards for Antimicrobial Susceptibility Testing. In CLSI Supplement M100, 30th ed.; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2020. [Google Scholar]
- Magiorakos, A.-P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef]
- Hosuru Subramanya, S.; Thapa, S.; Dwedi, S.K.; Gokhale, S.; Sathian, B.; Nayak, N.; Bairy, I. Streptococcus pneumoniae and Haemophilus species colonization in health care workers: The launch of invasive infections? BMC Res. Notes. 2016, 9, 66. [Google Scholar] [CrossRef]
- Karapinar, B.A.; Yürüyen, C.; Gürler, N.; Kayacan, C. Nasopharyngeal carriage of Neisseria meningitidis among medical school students in Turkey. Biomed Res. 2019, 30, 1–5. [Google Scholar] [CrossRef]
- Farida, H.; Severin, J.A.; Gasem, M.H.; Keuter, M.; van den Broek, P.; Hermans, P.W.; Wahyono, H.; Verbrugh, H.A. Nasopharyngeal carriage of Klebsiella pneumoniae and other Gram-negative bacilli in pneumonia-prone age groups in Semarang, Indonesia. J. Clin. Microbiol. 2013, 51, 1614–1616. [Google Scholar] [CrossRef]
- Humphreys, H.; Fitzpatick, F.; Harvey, B.J. Gender differences in rates of carriage and bloodstream infection caused by methicillin-resistant Staphylococcus aureus: Are they real, do they matter and why? Clin. Infect. Dis. 2015, 61, 1708–1714. [Google Scholar]
- Suhaili, Z.; Rafee, P.; Mat Azis, N.; Yeo, C.C.; Nordin, S.A.; Abdul Rahim, A.R.; Al-Obaidi, M.M.J.; Mohd Desa, M.N. Characterization of resistance to selected antibiotics and Panton-Valentine leukocidin-positive Staphylococcus aureus in a healthy student population at a Malaysian University. Germs 2018, 8, 21–30. [Google Scholar] [CrossRef]
- McMillan, M.; Walters, L.; Mark, T.; Lawrence, A.; Leong, L.E.X.; Sullivan, T.; Rogers, G.B.; Andrews, R.M.; Marshall, H.S. B part of it study: A longitudinal study to assess carriage of Neisseria meningitidis in first year university students in South Australia. Hum. Vaccin Immunother. 2018, 15, 987–994. [Google Scholar] [CrossRef] [PubMed]
- Breakwell, L.; Whaley, M.; Khan, U.I.; Bandy, U.; Alexander-Scott, N.; Dupont, L.; Vanner, C.; Chang, H.-Y.; Vuong, J.T.; Martin, S.; et al. Meningococcal carriage among a university student population–United States, 2015. Vaccine 2018, 36, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Kepenekli Kadayifci, E.; Güneşer Merdan, D.; Soysal, A.; Karaaslan, A.; Atıcı, S.; Durmaz, R.; Boran, P.; Turan, İ.; Söyletir, G.; Bakır, M. Prevalence of Neisseria meningitidis carriage: A small-scale survey in Istanbul, Turkey. J. Infect. Dev. Ctries. 2016, 10, 413–417. [Google Scholar] [CrossRef]
- Ministry of Health Malaysia, Health Facts. 2019. Available online: http://www.moh.gov.my/moh/resources/Penerbitan/Penerbitan%20Utama/HEALTH%20FACTS/Healh%20Facts%202019_Booklet.pdf (accessed on 3 January 2023).
- Torigoe, H.; Seki, M.; Yamashita, Y.; Sugaya, A.; Maeno, M. Detection of Haemophilus influenzae by loop-mediated isothermal amplification (LAMP) of the outer membrane protein P6 gene. Jpn. J. Infect. Dis. 2007, 60, 55–58. [Google Scholar]
- Cleary, D.; Devine, V.; Morris, D.; Osman, K.; Gladstone, R.; Bentley, S.; Faust, S.; Clarke, S. Pneumococcal vaccine impacts on the population genomics of non-typeable Haemophilus influenzae. Microb. Genom. 2018, 4, e000209. [Google Scholar] [CrossRef]
- Margolis, E.; Yates, A.; Levin, B.R. The ecology of nasal colonization of Streptococcus pneumoniae, Haemophilus influenzae and Staphylococcus aureus: The role of competition and interactions with host’s immune response. BMC Microbiol. 2010, 10, 59. [Google Scholar] [CrossRef]
- Falagas, M.E.; Mourtzoukou, E.G.; Vardakas, K.Z. Sex differences in the incidence and severity of respiratory tract infections. Respir. Med. 2007, 101, 1845–1863. [Google Scholar] [CrossRef] [PubMed]
- Vázquez-Martínez, E.R.; García-Gómez, E.; Camacho-Arroyo, I.; González-Pedrajo, B. Sexual dimorphism in bacterial infections. Biol. Sex Differ. 2018, 9, 27. [Google Scholar] [CrossRef]
- Ibrahim, J.N.; Eghnatios, E.; El Roz, A.; Fardoun, T.; Ghssein, G. Prevalence, antimicrobial resistance and risk factors for campylobacteriosis in Lebanon. J. Infect. Dev. Ctries. 2019, 13, 11–20. [Google Scholar] [CrossRef]
- Trigunaite, A.; Dimo, J.; Jørgensen, T.N. Suppressive effects of androgens on the immune system. Cell. Immunol. 2015, 294, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Kamada, M.; Irahara, M.; Maegawa, M.; Yasui, T.; Takeji, T.; Yamada, M.; Tezuka, M.; Kasai, Y.; Aono, T. Effect of hormone replacement therapy on post-menopausal changes of lymphocytes and T cell subsets. J. Endocrinol. Investig. 2000, 23, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Simell, B.; Kilpi, T.M.; Käyhty, H. Pneumococcal carriage and otitis media induce salivary antibodies to pneumococcal capsular polysaccharides in children. J. Infect. Dis. 2002, 186, 1106–1114. [Google Scholar] [CrossRef] [PubMed]
- Garbutt, C.; Simmons, G.; Patrick, D.; Miller, T. The public hand hygiene practices of New Zealanders: A national survey. New Zealand Med. J. 2007, 120, U2810. [Google Scholar]
- Mackert, M.; Liang, M.C.; Champlin, S. “Think the sink:” Preliminary evaluation of a handwashing promotion campaign. Am. J. Infect. Control 2013, 41, 275–277. [Google Scholar] [CrossRef] [PubMed]
- Immunise4Life. The Malaysian National Immunisation Programme (NIP). Available online: https://immunise4life.my/the-malaysian-national-immunisation-programme-nip/ (accessed on 12 March 2023).
- CodeBlue. Malaysia Chooses PCV10 Pneumococcal Vaccine, Immunisation Starts December. Available online: https://codeblue.galencentre.org/2020/11/24/malaysia-chooses-pcv10-pneumococcal-vaccine-immunisation-starts-december/ (accessed on 12 March 2023).
- WHO. Prioritization of Pathogens to Guide Discovery, Research and Development of New Antibiotics for Drug-Resistant Bacterial Infections, Including Tuberculosis; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Tacconelli, E.; Carrara, E.; Savoldi, A.; Harbarth, S.; Mendelson, M.; Monnet, D.L.; Pulcini, C.; Kahlmeter, G.; Kluytmans, J.; Carmeli, Y.; et al. Discovery, research, and development of new antibiotics: The WHO priority list of antibiotic-resistant bacteria and tuberculosis. Lancet Infect. Dis. 2018, 18, 318–327. [Google Scholar] [CrossRef] [PubMed]
- Cheng, M.P.; René, P.; Cheng, A.P.; Lee, T.C. Back to the future: Penicillin-susceptible Staphylococcus aureus. Am. J. Med. 2016, 129, 1331–1333. [Google Scholar] [CrossRef]
- Wyres, K.L.; Holt, K.E. Klebsiella pneumoniae as a key trafficker of drug resistance genes from environmental to clinically important bacteria. Curr. Opin. Microbiol. 2018, 45, 131–139. [Google Scholar] [CrossRef]
- Shaikh, S.; Fatima, J.; Shakil, S.; Rizvi, S.M.D.; Kamal, M.A. Antibiotic resistance and extended spectrum beta-lactamases: Types, epidemiology and treatment. Saudi J. Biol. Sci. 2015, 22, 90–101. [Google Scholar] [CrossRef]
- Haque, M.; A Rahman, N.A.; McKimm, J.; Kibria, G.M.; Majumder, A.A.; Haque, S.Z.; Islam, Z.; Abdullah, S.L.B.; Daher, A.M.; Zulkifli, Z.; et al. Self-medication of antibiotics: Investigating practice among university students at the Malaysian National Defence University. Infect. Drug Resist. 2019, 12, 1333–1351. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Target Bacterium | Target Gene | Primer Sequences (5′ → 3′) | Amplicon Size | Reference |
|---|---|---|---|---|
| S. aureus | nuc | Forward: GCGATTGATGGTGATACGGTT Reverse: AGCCAAGCCTTGGAACTAAAGC | 279 bp | [32] |
| K. pneumoniae | mdh | Forward: GCGTGGCGGTAGATCTAAGTCATA Reverse: TTCAGCTCCGCCACAAAGGTA | 364 bp | [33] |
| P. aeruginosa | oprL | Forward: ATGGAAATGCTGAAATTCGGC Reverse: CTTCTTCAGCTCGACGCGACG | 504 bp | [34] |
| S. pneumoniae | lytA | Forward: TGCCTCAAGTCGGCGTGCAA Reverse: CTGCTCACGGCTAATGCCCCAT | 455 bp | [35] |
| H. influenzae | bex | Forward: TATCACACAAATAGCGGTTGG Reverse: GGCCAAGAGATACTCATAGAACG | 181 bp | [36] |
| N. meningitidis | ctrA | Forward: GCTGCGGTAGGTGGTTCAA Reverse: TTGTCGCGGATTTGCAACTA | 110 bp | [36] |
| Host Factor | Overall Bacterial Carriage | Bacterial Carriage, n (%) | |||
|---|---|---|---|---|---|
| n (%) | p-value a | Single sp. | Multiple spp. | p-value b | |
| Gender | |||||
| Male | 39 (78) | 0.006 * | 21 (42) | 18 (36) | 0.005 * |
| Female | 25 (50) | 18 (36) | 7 (14) | ||
| Ethnicity | |||||
| Malay | 2 (66.7) | 0.99 | 2 (66.7) | 0 (0) | 0.96 |
| Chinese | 59 (64.1) | 35 (38) | 24 (26.1) | ||
| Indian | 3 (60) | 2 (40) | 1 (20) | ||
| NIP Vaccination | |||||
| Yes | 18 (66.7) | 0.88 | 11 (40.7) | 7 (25.9) | 0.99 |
| No | 12 (66.7) | 7 (38.9) | 5 (27.8) | ||
| Unsure | 34 (61.8) | 21 (38.2) | 13 (23.6) | ||
| Previous URT Symptoms | |||||
| Yes | 24 (68.6) | 0.52 | 13 (37.1) | 11 (31.4) | 0.56 |
| No | 40 (61.5) | 26 (40) | 14 (21.5) | ||
| Previous Antibiotic Intake | |||||
| Yes | 2 (40) | 0.35 | 1 (20) | 1 (20) | 0.53 |
| No | 62 (65.3) | 38 (40) | 24 (25.3) | ||
| Antibiotics | Susceptibility | ||
|---|---|---|---|
| Susceptible | Intermediate | Resistant | |
| S. aureus (n = 31) | |||
| Chloramphenicol | 29 (93.5%) | 2 (6.5%) | 0 (0%) |
| Ciprofloxacin | 31 (100%) | 0 (0%) | 0 (0%) |
| Doxycycline | 30 (96.8%) | 0 (0%) | 1 (3.2%) |
| Gentamicin | 30 (96.8%) | 1 (3.2%) | 0 (0%) |
| Methicillin | 30 (96.8%) | 0 (0%) | 1 (3.2%) |
| Penicillin G | 15 (48.4%) | 0 (0%) | 16 (51.6%) |
| Quinupristin-dalfopristin | 21 (67.7%) | 8 (25.8%) | 2 (6.5%) |
| Trimethoprim/sulfamethoxazole | 31 (100%) | 0 (0%) | 0 (0%) |
| Tetracycline | 30 (96.8%) | 0 (0%) | 1 (3.2%) |
| K. pneumoniae (n = 12) | |||
| Ampicillin | 0 (0%) | 0 (0%) | 12 (100%) |
| Chloramphenicol | 12 (100%) | 0 (0%) | 0 (0%) |
| Cefpodoxime | 12 (100%) | 0 (0%) | 0 (0%) |
| Ceftazidine | 12 (100%) | 0 (0%) | 0 (0%) |
| Ceftriaxone | 12 (100%) | 0 (0%) | 0 (0%) |
| Gentamicin | 12 (100%) | 0 (0%) | 0 (0%) |
| Imipenem | 12 (100%) | 0 (0%) | 0 (0%) |
| Tetracycline | 12 (100%) | 0 (0%) | 0 (0%) |
| P. aeruginosa (n = 1) | |||
| Ceftazidime | 1 (100%) | 0 (0%) | 0 (0%) |
| Ciprofloxacin | 1 (100%) | 0 (0%) | 0 (0%) |
| Gentamicin | 1 (100%) | 0 (0%) | 0 (0%) |
| Imipenem | 1 (100%) | 0 (0%) | 0 (0%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ong, H.H.; Toh, W.K.; Thong, L.Y.; Phoon, L.Q.; Clarke, S.C.; Cheah, E.S.G. Investigation of Upper Respiratory Carriage of Bacterial Pathogens among University Students in Kampar, Malaysia. Trop. Med. Infect. Dis. 2023, 8, 269. https://doi.org/10.3390/tropicalmed8050269
Ong HH, Toh WK, Thong LY, Phoon LQ, Clarke SC, Cheah ESG. Investigation of Upper Respiratory Carriage of Bacterial Pathogens among University Students in Kampar, Malaysia. Tropical Medicine and Infectious Disease. 2023; 8(5):269. https://doi.org/10.3390/tropicalmed8050269
Chicago/Turabian StyleOng, Hing Huat, Wai Keat Toh, Li Ying Thong, Lee Quen Phoon, Stuart C. Clarke, and Eddy Seong Guan Cheah. 2023. "Investigation of Upper Respiratory Carriage of Bacterial Pathogens among University Students in Kampar, Malaysia" Tropical Medicine and Infectious Disease 8, no. 5: 269. https://doi.org/10.3390/tropicalmed8050269
APA StyleOng, H. H., Toh, W. K., Thong, L. Y., Phoon, L. Q., Clarke, S. C., & Cheah, E. S. G. (2023). Investigation of Upper Respiratory Carriage of Bacterial Pathogens among University Students in Kampar, Malaysia. Tropical Medicine and Infectious Disease, 8(5), 269. https://doi.org/10.3390/tropicalmed8050269