
Concomitant Severe Psoriasis and Bullous Pemphigoid Induced by COVID-19




{kind=link}
{kind=link}
Abstract
:1. Introduction
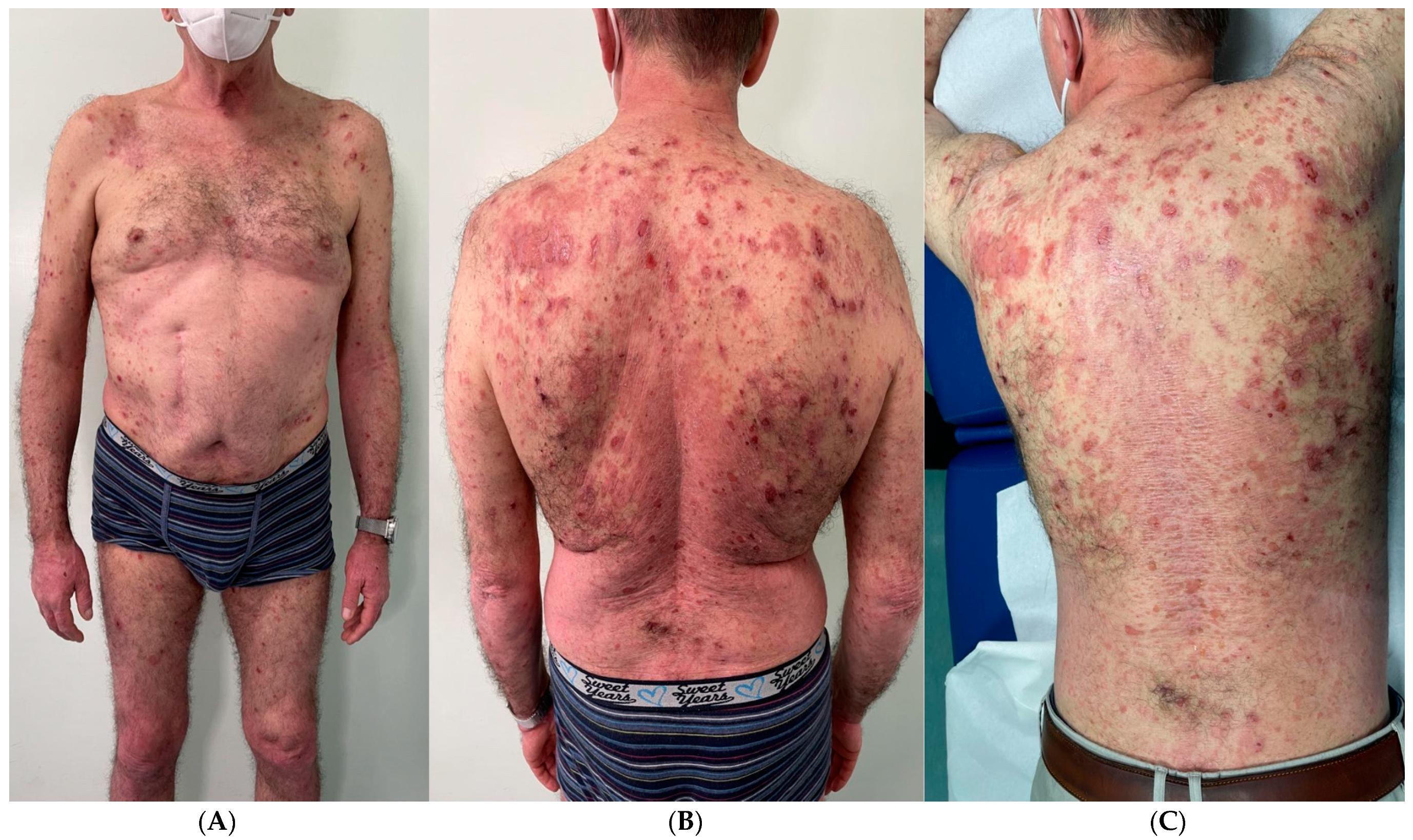
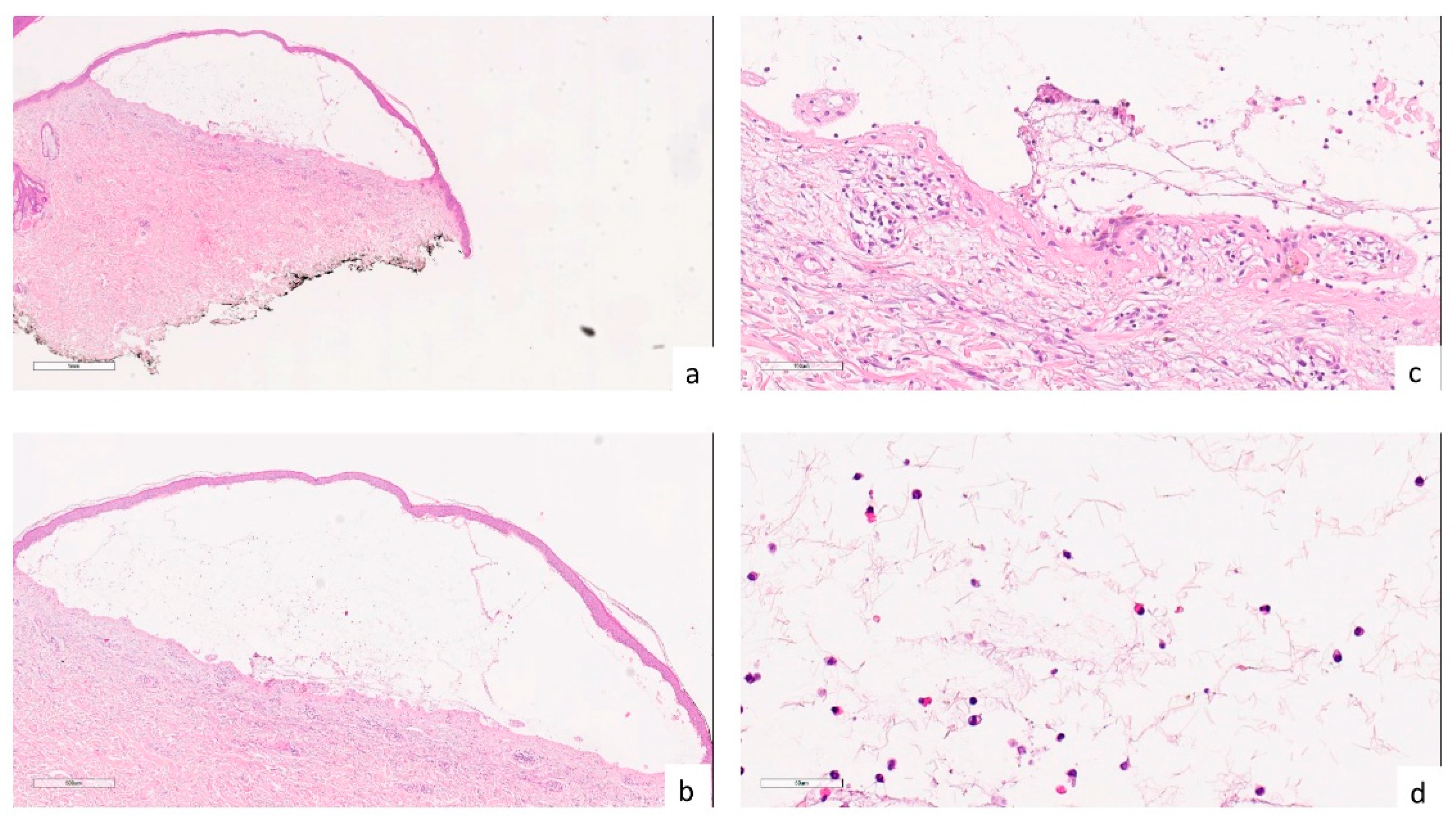
2. Detailed Case Description
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Galván Casas, C.; Català, A.; Carretero Hernández, G.; Rodríguez-Jiménez, P.; Fernández-Nieto, D.; Rodríguez-Villa Lario, A.; Navarro Fernández, I.; Ruiz-Villaverde, R.; Falkenhain-López, D.; Llamas Velasco, M.; et al. Classification of the cutaneous manifestations of COVID-19: A rapid prospective nationwide consensus study in Spain with 375 cases. Br. J. Dermatol. 2020, 183, 71–77. [Google Scholar] [PubMed]
- Martora, F.; Fabbrocini, G.; Nappa, P.; Megna, M. Impact of the COVID-19 pandemic on hospital admissions of patients with rare diseases: An experience of a Southern Italy referral center. Int. J. Dermatol. 2022, 61, e237–e238. [Google Scholar] [CrossRef] [PubMed]
- Drenovska, K.; Schmidt, E.; Vassileva, S. COVID-19 pandemic and the skin. Int. J. Dermatol. 2020, 59, 1312–1319. [Google Scholar] [CrossRef] [PubMed]
- Genovese, G.; Moltrasio, C.; Berti, E.; Marzano, A.V. Skin Manifestations Associated with COVID-19: Current Knowledge and Future Perspectives. Dermatology 2021, 237, 1–12. [Google Scholar] [PubMed]
- Marzano, A.V.; Cassano, N.; Genovese, G.; Moltrasio, C.; Vena, G.A. Cutaneous manifestations in patients with COVID-19: A preliminary review of an emerging issue. Br. J. Dermatol. 2020, 183, 431–442. [Google Scholar]
- Picone, V.; Fabbrocini, G.; Martora, L.; Martora, F. A Case of New-Onset Lichen Planus after COVID-19 Vaccination. Dermatol. Ther. 2022, 12, 801–805. [Google Scholar] [CrossRef]
- Roeder, C.; Driesch, P.V. Psoriatic erythroderma and bullous pemphigoid treated successfully with acitretin and azathioprine. Eur. J. Dermatol. 1999, 9, 537–539. [Google Scholar]
- Grän, F.; Kerstan, A.; Serfling, E.; Goebeler, M.; Muhammad, K. Current Developments in the Immunology of Psoriasis. Yale J. Biol. Med. 2020, 93, 97–110. [Google Scholar]
- Griffiths, C.E.M.; Armstrong, A.W.; Gudjonsson, J.E.; Barker, J.N.W.N. Psoriasis. Lancet 2021, 397, 1301–1315. [Google Scholar] [CrossRef]
- Marasca, C.; Fornaro, L.; Martora, F.; Picone, V.; Fabbrocini, G.; Megna, M. Onset of vitiligo in a psoriasis patient on ixekizumab. Dermatol. Ther. 2021, 34, e15102. [Google Scholar] [CrossRef]
- Ruggiero, A.; Martora, F.; Picone, V.; Potestio, L.; Camela, E.; Battista, T.; Fabbrocini, G.; Megna, M. The impact of COVID-19 infection on patients with psoriasis treated with biologics: An Italian experience. Clin. Exp. Dermatol. 2022, 47, 2280–2282. [Google Scholar] [CrossRef] [PubMed]
- Miyamoto, D.; Santi, C.G.; Aoki, V.; Maruta, C.W. Bullous pemphigoid. An. Bras. Dermatol. 2019, 94, 133–146. [Google Scholar] [CrossRef]
- Moro, F.; Fania, L.; Sinagra, J.L.M.; Salemme, A.; Di Zenzo, G. Bullous Pemphigoid: Trigger and Predisposing Factors. Biomolecules 2020, 10, 1432. [Google Scholar] [CrossRef] [PubMed]
- Bernard, P.; Antonicelli, F. Bullous Pemphigoid: A Review of its Diagnosis, Associations and Treatment. Am. J. Clin. Dermatol. 2017, 18, 513–528. [Google Scholar] [CrossRef] [PubMed]
- Maronese, C.A.; Cassano, N.; Genovese, G.; Foti, C.; Vena, G.A.; Marzano, A.V. The Intriguing Links between Psoriasis and Bullous Pemphigoid. J. Clin. Med. 2022, 12, 328. [Google Scholar] [PubMed]
- Miladi, R.; Janbakhsh, A.; Babazadeh, A.; Aryanian, Z.; Ebrahimpour, S.; Barary, M.; Sio, T.T.; Wollina, U.; Goldust, M.; Mohseni Afshar, Z. Pustular psoriasis flare-up in a patient with COVID-19. J. Cosmet. Dermatol. 2021, 20, 3364–3368. [Google Scholar]
- Aram, K.; Patil, A.; Goldust, M.; Rajabi, F. COVID-19 and exacerbation of dermatological diseases: A review of the available literature. Dermatol. Ther. 2021, 34, e15113. [Google Scholar] [CrossRef]
- Olson, N.; Eckhardt, D.; Delano, A. New-Onset Bullous Pemphigoid in a COVID-19 Patient. Case Rep. Dermatol. Med. 2021, 2021, 5575111. [Google Scholar] [CrossRef]
- Goon, P.K.C.; Bello, O.; Adamczyk, L.A.; Chan, J.Y.H.; Sudhoff, H.; Banfield, C.C. COVID-19 dermatoses: Acral vesicular pattern evolving into bullous pemphigoid. Skin Health Dis. 2020, 1, e6. [Google Scholar] [CrossRef]
- Shakoei, S.; Kalantari, Y.; Nasimi, M.; Tootoonchi, N.; Ansari, M.S.; Razavi, Z.; Etesami, I. Cutaneous manifestations following COVID-19 vaccination: A report of 25 cases. Dermatol. Ther. 2022, 35, e15651. [Google Scholar] [CrossRef]
- Shibabaw, T. Inflammatory Cytokine: IL-17A Signaling Pathway in Patients Present with COVID-19 and Current Treatment Strategy. J. Inflamm. Res. 2020, 13, 673–680. [Google Scholar] [CrossRef] [PubMed]
- Picone, V.; Martora, F.; Fabbrocini, G.; Marano, L. “COVID arm”: Abnormal side effect after Moderna COVID-19 vaccine. Dermatol. Ther. 2022, 35, e15197. [Google Scholar] [PubMed]
- Martora, F.; Picone, V.; Fornaro, L.; Fabbrocini, G.; Marasca, C. Can COVID-19 cause atypical forms of pityriasis rosea refractory to conventional therapies? J. Med. Virol. 2022, 94, 1292–1293. [Google Scholar] [PubMed]
- Martora, F.; Fabbrocini, G.; Marasca, C. Pityriasis rosea after Moderna mRNA-1273 vaccine: A case series. Dermatol. Ther. 2022, 35, e15225. [Google Scholar]
- McMahon, D.E.; Kovarik, C.L.; Damsky, W.; Rosenbach, M.; Lipoff, J.B.; Tyagi, A.; Chamberlin, G.; Fathy, R.; Nazarian, R.M.; Desai, S.R.; et al. Clinical and pathologic correlation of cutaneous COVID-19 vaccine reactions including V-REPP: A registry-based study. J. Am. Acad. Dermatol. 2022, 86, 113–121. [Google Scholar] [CrossRef]
- McMahon, D.E.; Amerson, E.; Rosenbach, M.; Lipoff, J.B.; Moustafa, D.; Tyagi, A.; Desai, S.R.; French, L.E.; Lim, H.W.; Thiers, B.H.; et al. Cutaneous reactions reported after Moderna and Pfizer COVID-19 vaccination: A registry-based study of 414 cases. J. Am. Acad. Dermatol. 2021, 85, 46–55. [Google Scholar] [CrossRef]
- Català, A.; Muñoz-Santos, C.; Galván-Casas, C.; Roncero Riesco, M.; Revilla Nebreda, D.; Solá-Truyols, A.; Giavedoni, P.; Llamas-Velasco, M.; González-Cruz, C.; Cubiró, X.; et al. Cutaneous reactions after SARS-CoV-2 vaccination: A cross-sectional Spanish nationwide study of 405 cases. Br. J. Dermatol. 2022, 186, 142–152. [Google Scholar]
- Cebeci Kahraman, F.; Savaş Erdoğan, S.; Aktaş, N.D.; Albayrak, H.; Türkmen, D.; Borlu, M.; Arıca, D.A.; Demirbaş, A.; Akbayrak, A.; Polat Ekinci, A.; et al. Cutaneous reactions after COVID-19 vaccination in Turkey: A multicenter study. J. Cosmet. Dermatol. 2022, 21, 3692–3703. [Google Scholar] [CrossRef]
- Bellinato, F.; Fratton, Z.; Girolomoni, G.; Gisondi, P. Cutaneous Adverse Reactions to SARS-CoV-2 Vaccines: A Systematic Review and Meta-Analysis. Vaccines 2022, 10, 1475. [Google Scholar]
- Gao, P.; Cai, S.; Liu, Q.; Du, M.; Liu, J.; Liu, M. Effectiveness and Safety of SARS-CoV-2 Vaccines among Children and Adolescents: A Systematic Review and Meta-Analysis. Vaccines 2022, 10, 421. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martora, F.; Battista, T.; Fabbrocini, G.; Megna, M. Concomitant Severe Psoriasis and Bullous Pemphigoid Induced by COVID-19. Trop. Med. Infect. Dis. 2023, 8, 107. https://doi.org/10.3390/tropicalmed8020107
Martora F, Battista T, Fabbrocini G, Megna M. Concomitant Severe Psoriasis and Bullous Pemphigoid Induced by COVID-19. Tropical Medicine and Infectious Disease. 2023; 8(2):107. https://doi.org/10.3390/tropicalmed8020107
Chicago/Turabian StyleMartora, Fabrizio, Teresa Battista, Gabriella Fabbrocini, and Matteo Megna. 2023. "Concomitant Severe Psoriasis and Bullous Pemphigoid Induced by COVID-19" Tropical Medicine and Infectious Disease 8, no. 2: 107. https://doi.org/10.3390/tropicalmed8020107
APA StyleMartora, F., Battista, T., Fabbrocini, G., & Megna, M. (2023). Concomitant Severe Psoriasis and Bullous Pemphigoid Induced by COVID-19. Tropical Medicine and Infectious Disease, 8(2), 107. https://doi.org/10.3390/tropicalmed8020107