
Prevalence and Risk Factors of Genital Human Papillomavirus Infections among Women in Lagos, Nigeria

 , , , ,
, , , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Area and Design
2.2. Study Population
2.3. Specimen Collection and Laboratory Analysis
2.4. Data Management and Analysis
2.5. Ethical Considerations
3. Results
3.1. Participants’ Sociodemographic Characteristics
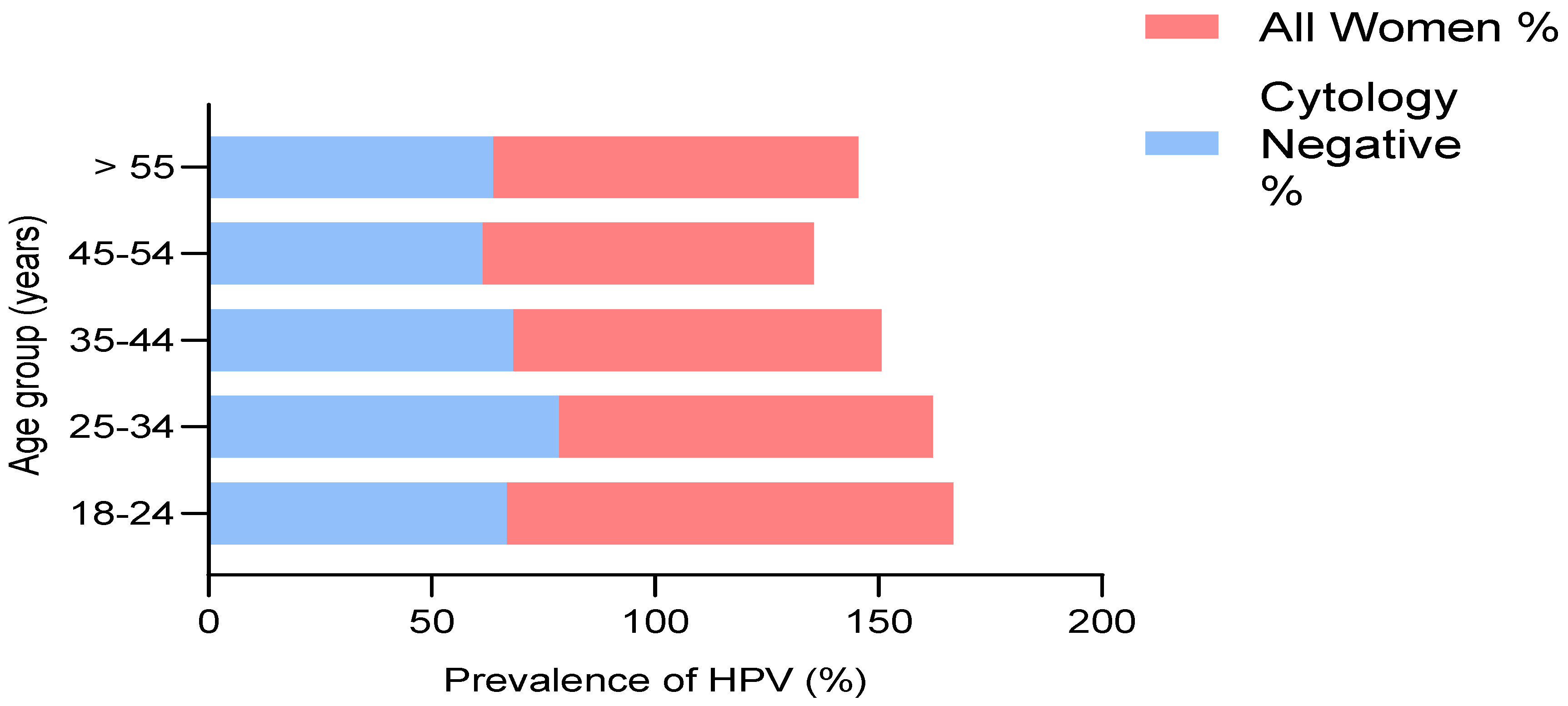
3.2. Prevalence of HPV
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bruni, L.; Diaz, M.; Castellsagué, M.; Ferrer, E.; Bosch, F.X.; de Sanjosé, S. Cervical human papillomavirus prevalence in 5 continents: Meta-analysis of 1 million women with normal cytological findings. J. Infect. Dis. 2010, 202, 1789–1799. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Z.-M.; Baker, C.C. Papillomavirus genome structure, expression, and post-transcriptional regulation. Front. Biosci.-Landmark 2006, 11, 2286–2302. [Google Scholar] [CrossRef] [PubMed]
- De Sanjosé, S.; Diaz, M.; Castellsagué, X.; Clifford, G.; Bruni, L.; Muñoz, N.; Bosch, F.X. Worldwide prevalence and genotype distribution of cervical human papillomavirus DNA in women with normal cytology: A meta-analysis. Lancet Infect. Dis. 2007, 7, 453–459. [Google Scholar] [CrossRef]
- Xi, L.F.; Toure, P.; Critchlow, C.W.; Hawes, S.E.; Dembele, B.; Sow, P.S.; Kiviat, N.B. Prevalence of specific types of human papillomavirus and cervical squamous intraepithelial lesions in consecutive, previously unscreened, West-African women over 35 years of age. Int. J. Cancer 2003, 103, 803–809. [Google Scholar] [CrossRef] [PubMed]
- Salih, M.M.; Safi, M.E.; Hart, K.; Tobi, K.; Adam, I. Genotypes of human papilloma virus in Sudanese women with cervical pathology. Infect. Agents Cancer 2010, 5, 26. [Google Scholar] [CrossRef]
- Allan, B.; Marais, D.J.; Hoffman, M.; Shapiro, S.; Williamson, A.-L. Cervical human papillomavirus (HPV) infection in South African women: Implications for HPV screening and vaccine strategies. J. Clin. Microbiol. 2008, 46, 740–742. [Google Scholar] [CrossRef][Green Version]
- Gravitt, P.E.; Kamath, A.M.; Gaffikin, L.; Chirenje, Z.M.; Womack, S.; Shah, K.V. Human papillomavirus genotype prevalence in high-grade squamous intraepithelial lesions and colposcopically normal women from Zimbabwe. Int. J. Cancer 2002, 100, 729–732. [Google Scholar] [CrossRef]
- Piras, F.; Piga, M.; De Montis, A.; Zannou, A.R.; Minerba, L.; Perra, M.T.; Murtas, D.; Atzori, M.; Pittau, M.; Maxia, C. Prevalence of human papillomavirus infection in women in Benin, West Africa. Virol. J. 2011, 8, 514. [Google Scholar] [CrossRef]
- Traore, I.M.A.; Zohoncon, T.M.; Dembele, A.; Djigma, F.W.; Obiri-Yeboah, D.; Traore, G.; Bambara, M.; Ouedraogo, C.; Traore, Y.; Simpore, J. Molecular characterization of high-risk human papillomavirus in women in Bobo-Dioulasso, Burkina Faso. BioMed Res. Int. 2016, 2016, 7092583. [Google Scholar] [CrossRef]
- Birrou, K.; Tagajdid, M.R.; Elkochri, S.; Abi, R.; Zouhdi, M.; Mrani, S. Human papillomavirus genotype prevalence and distribution among Moroccan women. Int. J. Res. Med. Sci. 2015, 3, 95–99. [Google Scholar] [CrossRef][Green Version]
- Castellsagué, X.; Menéndez, C.; Loscertales, M.-P.; Kornegay, J.R.; dos Santos, F.; Gómez-Olivé, F.X.; Lloveras, B.; Abarca, N.; Vaz, N.; Barreto, A. Human papillomavirus genotypes in rural Mozambique. Lancet 2001, 358, 1429–1430. [Google Scholar] [CrossRef]
- De Vuyst, H.; Steyaert, S.; Van Renterghem, L.; Claeys, P.; Muchiri, L.; Sitati, S.; Vansteelandt, S.; Quint, W.; Kleter, B.; Van Marck, E. Distribution of human papillomavirus in a family planning population in Nairobi, Kenya. Sex. Transm. Dis. 2003, 30, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Sahasrabuddhe, V.; Mwanahamuntu, M.H.; Vermund, S.; Huh, W.; Lyon, M.; Stringer, J.; Parham, G. Prevalence and distribution of HPV genotypes among HIV-infected women in Zambia. Br. J. Cancer 2007, 96, 1480–1483. [Google Scholar] [CrossRef]
- Thomas, J.; Herrero, R.; Omigbodun, A.; Ojemakinde, K.; Ajayi, I.; Fawole, A.; Oladepo, O.; Smith, J.; Arslan, A.; Munoz, N. Prevalence of papillomavirus infection in women in Ibadan, Nigeria: A population-based study. Br. J. Cancer 2004, 90, 638–645. [Google Scholar] [CrossRef]
- Gage, J.C.; Ajenifuja, K.O.; Wentzensen, N.; Adepiti, A.C.; Stoler, M.; Eder, P.S.; Bell, L.; Shrestha, N.; Eklund, C.; Reilly, M. Effectiveness of a simple rapid human papillomavirus DNA test in rural Nigeria. Int. J. Cancer 2012, 131, 2903–2909. [Google Scholar] [CrossRef] [PubMed]
- Fadahunsi, O.; Omoniyi-Esan, G.; Banjo, A.; Esimai, O.; Osiagwu, D.; Clement, F.; Iyola, S. Prevalence of high risk oncogenic human papillomavirus types in cervical smears of women attending well woman clinic in Ile Ife, Nigeria. Gynecol. Obstet. 2013, 3, 2–5. [Google Scholar]
- Adegbesan-Omilabu, M.; Okunade, K.; Omilabu, S. Oncogenic human papilloma virus infection among women attending the cytology clinic of a tertiary hospital in Lagos, South-West Nigeria. Int. J. Res. Med. Sci. 2014, 2, 625–630. [Google Scholar] [CrossRef][Green Version]
- Okunade, K.S.; Nwogu, C.M.; Oluwole, A.A.; Anorlu, R.I. Prevalence and risk factors for genital high-risk human papillomavirus infection among women attending the outpatient clinics of a university teaching hospital in Lagos, Nigeria. Pan Afr. Med. J. 2017, 28, 227. [Google Scholar] [CrossRef]
- Omoare, A.A.; Ashaka, O.S.; Nasir, I.A.; Agbede, O.O. The Burden of Human Papillomavirus Infections Among Women in Nigeria: A Review Update. J. Appl. Virol. 2016, 5, 9–20. [Google Scholar] [CrossRef][Green Version]
- Bayo, S.; Bosch, F.X.; de Sanjosé, S.; Muñoz, N.; Combita, A.L.; Coursaget, P.; Diaz, M.; Dolo, A.; van den Brule, A.J.; Meijer, C.J. Risk factors of invasive cervical cancer in Mali. Int. J. Epidemiol. 2002, 31, 202–209. [Google Scholar] [CrossRef]
- World Health Organization. Human papillomavirus vaccines: WHO position paper. Wkly. Epidemiol. Rec. Relev. Épidémiologique Hebd. 2009, 84, 118–131. [Google Scholar]
- Honorable Minister for Health. Nigeria Cancer Control Plan 2018–2022; Honorable Minister for Health: Abuja, Nigeria, 2018. [Google Scholar]
- Onyenwenyi, A.; Gugu, G. Strategies for the prevention and control of cervical cancer in rural communities: A Nigerian perspective. J. Community Med. Prim. Health Care 2016, 28, 77–93. [Google Scholar]
- Hammou, R.A.; Benhessou, M.; Bouziyane, A.; Hassou, N.; Benhchekroun, M.N.; Bessi, H.; Ennaji, M.M. Oncogenic Human Papillomavirus involvement in epithelial ovarian carcinoma among women in Morocco. Bioinformation 2019, 15, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Nweke, I.; Banjo, A.; Abdulkareem, F.; Nwadike, V. Prevalence of human papilloma virus DNA in HIV positive women in Lagos University Teaching Hospital (LUTH) Lagos, Nigeria. Microbiol. Res. J. Int. 2013, 3, 400–413. [Google Scholar] [CrossRef]
- Akarolo-Anthony, S.N.; Famooto, A.O.; Dareng, E.O.; Olaniyan, O.B.; Offiong, R.; Wheeler, C.M.; Adebamowo, C.A. Age-specific prevalence of human papilloma virus infection among Nigerian women. BMC Public Health 2014, 14, 656. [Google Scholar] [CrossRef]
- Manga, M.M.; Fowotade, A.; Abdullahi, Y.M.; El-Nafaty, A.U.; Adamu, D.B.; Pindiga, H.U.; Bakare, R.A.; Osoba, A.O. Epidemiological patterns of cervical human papillomavirus infection among women presenting for cervical cancer screening in North-Eastern Nigeria. Infect. Agents Cancer 2015, 10, 39. [Google Scholar] [CrossRef]
- Auwal, I.K.; Aminu, M.; Atanda, A.T.; Tukur, J.; Sarkinfada, F. Prevalence and Risk Factors of High Risk Human Papillomavirus Infections among Women Attending Gynaecology Clinics in Kano, Northern Nigeria. Bayero J. Pure Appl. Sci. 2014, 6, 67–71. [Google Scholar] [CrossRef]
- Anoruo, O.; Bristow, C.; Mody, N.; Klausner, J.D. Estimated prevalence of human papillomavirus among Nigerian women: A systematic review and meta-analysis. Afr. J. Reprod. Health 2022, 26, 89–96. [Google Scholar]
- Leyh-Bannurah, S.-R.; Prugger, C.; de Koning, M.N.; Goette, H.; Lellé, R.J. Cervical human papillomavirus prevalence and genotype distribution among hybrid capture 2 positive women 15 to 64 years of age in the Gurage zone, rural Ethiopia. Infect. Agents Cancer 2014, 9, 31. [Google Scholar] [CrossRef]
- Blossom, D.; Beigi, R.; Farrell, J.; Mackay, W.; Qadadri, B.; Brown, D.; Rwambuya, S.; Walker, C.; Kambugu, F.; Abdul-Karim, F. Human papillomavirus genotypes associated with cervical cytologic abnormalities and HIV infection in Ugandan women. J. Med. Virol. 2007, 79, 758–765. [Google Scholar] [CrossRef]
- Mbulawa, Z.Z.; Coetzee, D.; Williamson, A.-L. Human papillomavirus prevalence in South African women and men according to age and human immunodeficiency virus status. BMC Infect. Dis. 2015, 15, 459. [Google Scholar] [CrossRef] [PubMed]
- Dube Mandishora, R.S.; Christiansen, I.K.; Chin’ombe, N.; Duri, K.; Ngara, B.; Rounge, T.B.; Meisal, R.; Ambur, O.H.; Palefsky, J.M.; Stray-Pedersen, B. Genotypic diversity of anogenital human papillomavirus in women attending cervical cancer screening in Harare, Zimbabwe. J. Med. Virol. 2017, 89, 1671–1677. [Google Scholar] [CrossRef]
- Lindau, S.T.; Drum, M.L.; Gaumer, E.; Surawska, H.; Jordan, J.A. Prevalence of high-risk human papillomavirus among older women. Obstet. Gynecol. 2008, 112, 979–989. [Google Scholar] [CrossRef] [PubMed]
- Nejo, Y.T.; Olaleye, D.O.; Odaibo, G.N. Molecular characterisation of genital human papillomavirus among women in Southwestern, Nigeria. PLoS ONE 2019, 14, e0224748. [Google Scholar] [CrossRef] [PubMed]
- Esere, M.O. Effect of Sex Education Programme on at-risk sexual behaviour of school-going adolescents in Ilorin, Nigeria. Afr. Health Sci. 2008, 8, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Veldhuijzen, N.J.; Snijders, P.J.; Reiss, P.; Meijer, C.J.; van de Wijgert, J.H. Factors affecting transmission of mucosal human papillomavirus. Lancet Infect. Dis. 2010, 10, 862–874. [Google Scholar] [CrossRef]
- Clarke, M.A.; Gage, J.C.; Ajenifuja, K.O.; Wentzensen, N.A.; Adepiti, A.C.; Wacholder, S.; Burk, R.D.; Schiffman, M. A population-based cross-sectional study of age-specific risk factors for high risk human papillomavirus prevalence in rural Nigeria. Infect. Agents Cancer 2011, 6, 12. [Google Scholar] [CrossRef] [PubMed]
- Ojiyi, E.; Okeudo, C.; Dike, E.; Anolue, F.; Onyeka, U.; Audu, B.; Ngadda, H. The prevalence and predictors of human papilloma virus infection of the cervix at a university teaching hospital in northern Nigeria. Internet J. Gynecol. Obstet. 2012, 16, 1–19. [Google Scholar]


{kind=link}
| All Participants | Cytology-Negative Participants | ||||||
|---|---|---|---|---|---|---|---|
| Variables | Categories | N/P 30/135 | OR (95% CI) | p-Value | N/P 16/113 | OR (95% CI) | p-Value |
| Age (years) | 18–24 | 0/6 | - | - | 0/4 | - | - |
| 25–34 | 6/31 | 1.15 (0.29–4.62) | 0.85 | 6/29 | 0.35 (0.04–3.15) | 0.35 | |
| 35–44 | 12/57 | 1.06 (0.30–3.68) | 0.93 | 6/47 | 0.56 (0.06–5.05) | 0.60 | |
| 45–54 | 8/23 | 0.64 (0.17–2.46) | 0.52 | 3/19 | 0.45 (0.04–4.82) | 0.51 | |
| ≥55 | 4/18 | 1.0 (referent) | 1/14 | 1.0 | |||
| MS | Married | 23/103 | 1.0 | 13/86 | 1.0 | ||
| Divorced/Widowed/Separated | 3/15 | 1.05 (0.32–3.43) | 0.93 | 0/14 | 1.53 (0.38–0.69) | 0.55 | |
| Not married | 4/17 | 1.18 (0.23–6.13) | 0.85 | 3/13 | - | - | |
| ES | No schooling | 1/3 | 1.0 | 0/1 | 1.0 | ||
| Primary | 1/6 | 2.00 (0.09–44.35) | 0.66 | 0/4 | 1.0 | - | |
| Secondary | 4/23 | 1.92 (0.16–23.35) | 0.61 | 2/17 | - | - | |
| Tertiary | 24/103 | 1.43 (0.14–14.36) | 0.76 | 14/91 | - | - | |
| Alcohol use | No | 23/110 | 1.0 | 14/95 | 1.0 | ||
| Yes | 7/25 | 0.75 (0.29–1.93) | 0.55 | 2/18 | 1.33 (0.28–6.34) | 0.72 | |
| Smoking | No | 30/133 | 1.0 | 16/111 | 1.0 | ||
| Yes | 0/2 | - | - | 0/2 | - | - | |
| All Participants | Cytology-Negative Participants | ||||||
|---|---|---|---|---|---|---|---|
| Variables | Categories | N/P 30/135 | OR (95% CI) | p-Value | N/P 16/113 | OR (95% CI) | p-Value |
| AFS (years) | ≤16 | 12/48 | 1.0 | 5/43 | 1.0 | ||
| 17–20 | 10/30 | 0.75 (0.29–1.95) | 0.55 | 9/22 | 0.28 (0.08–0.95) | 0.04 | |
| ≥21 | 8/57 | 1.78 (0.67–4.72) | 0.25 | 2/48 | 2.79 (0.51–15.13) | 0.23 | |
| AFP (years) | <17 years | 7/34 | 1.0 | 2/28 | 1.0 | ||
| 17–19 years | 3/27 | 1.85 (0.44–7.85) | 0.40 | 2/22 | 0.79 (0.10–6.03) | 0.82 | |
| 20–24 years | 1/17 | 3.50 (0.40–30.80) | 0.26 | 0/13 | - | - | |
| ≥25 years | 7/5 | 0.15 (0.04–0.60) | 0.01 | 4/4 | 0.07 (0.01–0.52) | 0.01 | |
| Parity | Not pregnant | 5/22 | 1.0 | 4/20 | 1.0 | ||
| 1–4 pregnancies | 13/68 | 1.19 (0.38–3.71) | 0.77 | 6/60 | 2.00 (0.51–7.81) | 0.32 | |
| ≥5 pregnancies | 12/45 | 0.85 (0.27–2.72) | 0.79 | 6/33 | 1.10 (0.28–4.38) | 0.89 | |
| LSP | 1 | 12/56 | 1.0 | 8/52 | 1.0 | ||
| 2–4 | 15/62 | 0.89 (0.38–2.05) | 0.78 | 7/49 | 1.08 (0.36–3.19) | 0.89 | |
| ≥5 | 3/17 | 1.21 (0.31–4.81) | 0.78 | 1/12 | 1.85 (0.21–16.19) | 0.58 | |
| Condom use | No | 14/92 | 1.0 | 6/82 | 1.0 | ||
| Yes | 16/43 | 0.41 (0.18–0.91) | 0.03 | 10/31 | 0.23 (0.08–0.68) | 0.01 | |
| All Participants | Cytology-Negative Participants | ||||||
|---|---|---|---|---|---|---|---|
| Variables | Categories | N/P 30/135 | OR (95% CI) | p-Value | N/P 16/113 | OR (95% CI) | p-Value |
| Clinical Characteristics | |||||||
| HSTI | No | 24/68 | 1 | 14/54 | 1 | ||
| Yes | 6/67 | 3.94 (1.51–10.25) | 0.005 | 2/59 | 7.65 (1.66–35.21) | 0.01 | |
| HGW | Absent | 27/112 | 1 | 16/95 | 1 | ||
| Present | 3/23 | 1.85 (0.52–6.61) | 0.34 | 0/18 | - | - | |
| HCU | No | 26/116 | 1 | 16/100 | 1 | ||
| Yes | 4/19 | 1.06 (0.33–3.39) | 0.92 | 0/13 | - | - | |
| HCF | No | 26/120 | 1 | 16/101 | 1 | ||
| Yes | 4/15 | 0.81 (0.25–2.65) | 0.73 | 0/12 | - | - | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ashaka, O.S.; Omoare, A.A.; James, A.B.; Adeyemi, O.O.; Oladiji, F.; Adeniji, K.A.; Okunade, K.S.; Agbede, O.O. Prevalence and Risk Factors of Genital Human Papillomavirus Infections among Women in Lagos, Nigeria. Trop. Med. Infect. Dis. 2022, 7, 386. https://doi.org/10.3390/tropicalmed7110386
Ashaka OS, Omoare AA, James AB, Adeyemi OO, Oladiji F, Adeniji KA, Okunade KS, Agbede OO. Prevalence and Risk Factors of Genital Human Papillomavirus Infections among Women in Lagos, Nigeria. Tropical Medicine and Infectious Disease. 2022; 7(11):386. https://doi.org/10.3390/tropicalmed7110386
Chicago/Turabian StyleAshaka, Oluwaseyi Sedowhe, Adesuyi Ayodeji Omoare, Ayorinde Babatunde James, Oluwapelumi Olufemi Adeyemi, Femi Oladiji, Kayode Adebamiji Adeniji, Kehinde Sharafadeen Okunade, and Olajide Olubunmi Agbede. 2022. "Prevalence and Risk Factors of Genital Human Papillomavirus Infections among Women in Lagos, Nigeria" Tropical Medicine and Infectious Disease 7, no. 11: 386. https://doi.org/10.3390/tropicalmed7110386
APA StyleAshaka, O. S., Omoare, A. A., James, A. B., Adeyemi, O. O., Oladiji, F., Adeniji, K. A., Okunade, K. S., & Agbede, O. O. (2022). Prevalence and Risk Factors of Genital Human Papillomavirus Infections among Women in Lagos, Nigeria. Tropical Medicine and Infectious Disease, 7(11), 386. https://doi.org/10.3390/tropicalmed7110386