1. Introduction
An epidemic is a function of environmental factors and a contact structure that varies over time, which in turn leads to varying transmission potential of an “infection”. We also refer the word “infection” to describe social influences exerted by a typical influential individual with a particular social problem that results in a naive (to the social problem) individual becoming involved in the problem. For example, an alcohol drinker might influence an abstainer into imitating drinking behavior and initiating alcohol drinking. Many authors have studied outbreaks of social problems and infectious diseases using compartmental transmission/influence model. Qualitative aspects of homogeneous mixing models with constant transmission potential of an infection are well understood for various applications. These models are relatively easy to analyze and can answer questions, at the population level, with good precision. Homogeneous mixing compartmental models have a long history; however, quantification of temporal transmission potential of an infectious agent, an input variable for this type of model, has been a challenge.
William Hamer first published a paper in 1906 containing an epidemic model for the transmission of measles where his observation included the incidence of new cases, in a time interval, is proportional to the product, , of the density of susceptibles (S) and the density I of infectives (I) in the population. The formulation of incidence can be explained by considering some epidemiological quantity. Consider a single susceptible individual in a homogeneously mixing population of size N. This individual contacts other members of the population at the rate c, per unit time, and a proportion of these contacts are with individuals who are “infectious”. If the probability of transmission of infection given contact is , then the rate at which the infection is transmitted to a susceptible is , per unit time, and the rate at which the susceptible population becomes infected is .
The contact rate is often a function of population density, reflecting the fact that contacts take time and saturation occurs. If c is assumed approximately proportional to N or equal to constant, incidence can be represented by terms such as (referred as mass action incidence) or (referred as standard incidence), respectively. The parameter , which includes the contact rate c, is known as a “transmission coefficient” (or “effective contact rate” or “transmission potential”) with units as . At low population densities mass action is a reasonable approximation of a much more complex contact structure; however, in general, standard incidence is more appropriate for modeling transmission for human diseases or influences for social problems. The term is sometimes referred as the force of infection, i.e., per-capita rate at which susceptible members of the host population are becoming infected. On the other hand, the transmission rate, represents the number of new infections per unit of time generated by an infected individual. The transmission rate is calculated by dividing incidence for a given time period by a disease prevalence for the same time interval.
Most infectious disease data are collected in form of incidence and/or prevalence. Prevalence of a “disease” in a population is defined as the total number of cases of the disease in the population at a given time, whereas prevalence proportion is computed by dividing the total number of cases in the population by the number of individuals in the population. It is used as an estimate of how common a condition is within a population over a certain period of time. Incidence is a measure of the risk of developing some new condition within a specified period of time. Incidence proportion (also known as cumulative incidence) is the number of new cases within a specified time period divided by the size of the population initially at risk. When the denominator is the sum of the person-time of the at-risk population, it is also known as the incidence density rate or person-time incidence rate. Using person-time rather than just time handles situations where the amount of observation time differs between people, or when the population at risk varies with time. Prevalence is a measurement of all individuals affected by the disease within a particular period of time, whereas incidence is a measurement of the number of new individuals who contract a disease during a particular period of time. So, prevalence and incidence proportion at the time t is given by and , respectively.
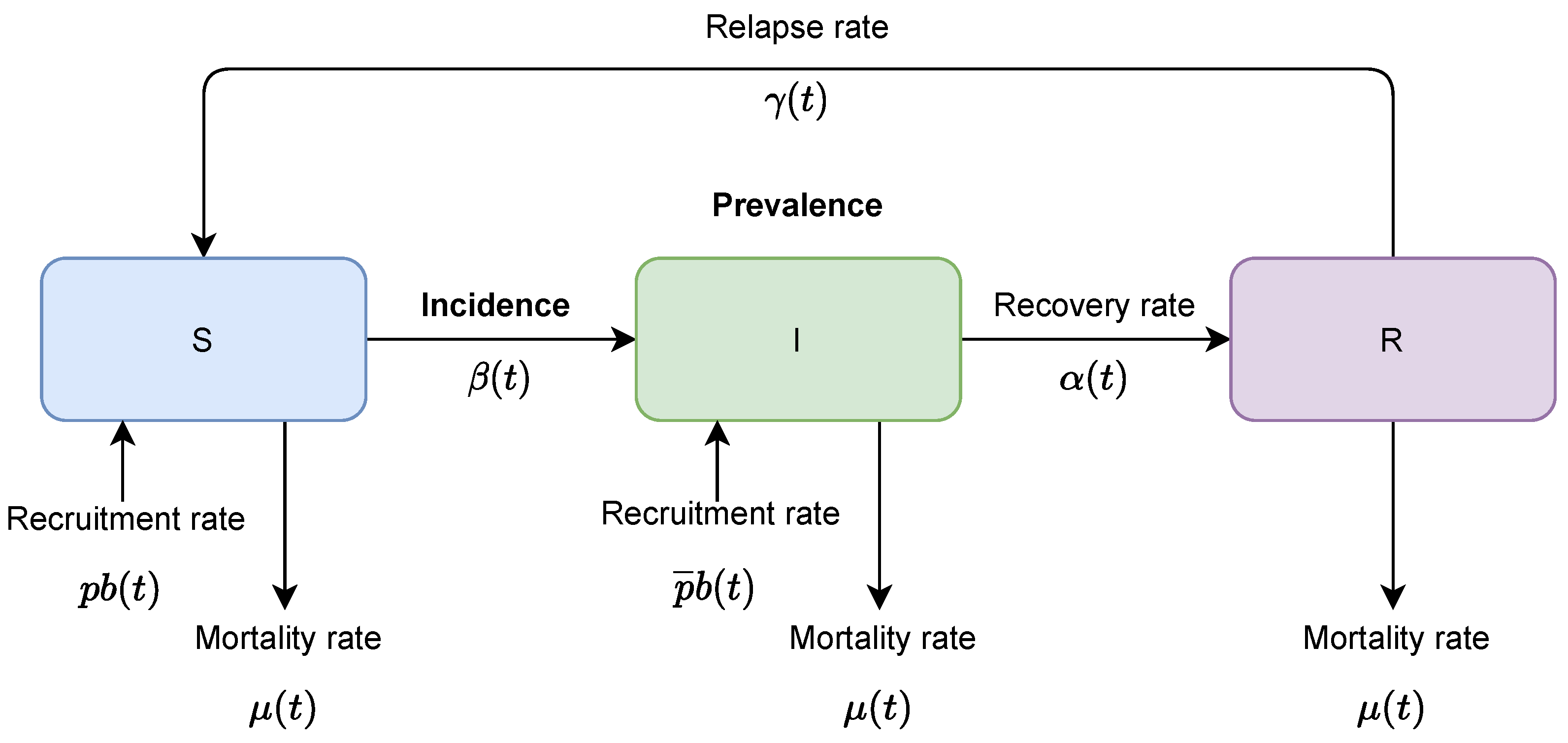
In compartmental mathematical models, varied assumptions are made based on characteristics of a modeling disease which lead modelers to focus on more important aspects of the epidemic. For example, an epidemic that occurs on a timescale that is much shorter than that of the population replenishment (that is, epidemic occurs at a much faster rate than births and deaths in the population), constant population size can be assumed. Additional common features of these models might include temporary or permanent recovery of infected individuals and a birth rate into infective class. Whether establishment or a major outbreak of an infectious disease or a social problem will occur in a population, requires extensive experience or a mathematical model of disease dynamics and estimates of the parameters of the disease model. Here, we provide a method for estimating the transmission coefficient (
), which is a key parameter in shaping the epidemic dynamics generated from the model because of nonlinearity associated with the term containing it. A suitable set of data for estimation of
includes prevalence and incidence of the outbreak in question. There are many different methods for estimating
but most of them results in an aggregate value over time. The methods in the literature include estimation using regression of prevalence and time since start of an epidemic [
1], estimating from equation for basic reproductive rate when threshold density is known [
2], estimating from equilibrium prevalence [
3,
4], using age prevalence curves [
5], inferring from behavior or contact data [
6], and iterative comparison of field prevalence data with model predictions [
7].
Some researchers have modeled time-varying transmission coefficients for diseases that follow seasonal patterns but using a predefined functional form [
8]. On the other hand, a study by Finkenstadt and Grenfell [
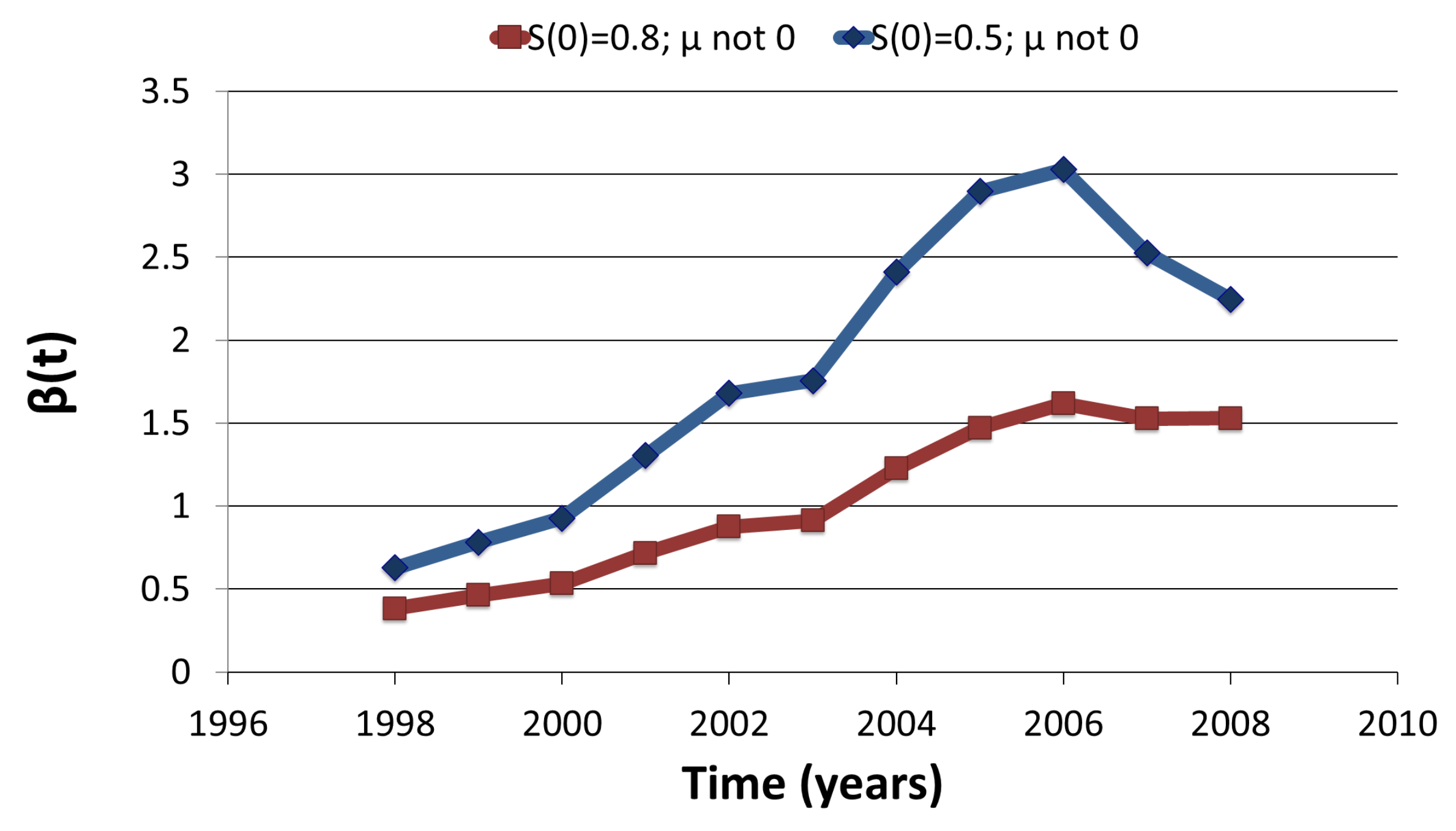
9] uses a discrete time model that allows for a temporally varying transmission parameter with a period of one year with no assumption on functional form. However, their estimation is computationally intensive and assumes that reporting interval of the available data must be an integer fraction of the serial interval of the disease. Another study by Pollicott et al. (2012), suggested first to fit the data with a pre-defined continuous function and then provide an analytical estimate of the transmission rate. However, their method was only applicable to prevalence data, with some restrictive assumptions on the initial number of susceptible or vital rates [
10]. In the current study, we provide an analytical estimation of transmission coefficient using distinct and novel mathematical approach that is not only applicable to both prevalence and incidence data but also has its applicability to wide public-health problems including social issues.
Table 1 provides a brief comparison of the estimation procedures in the Pollicott et al and the present study.
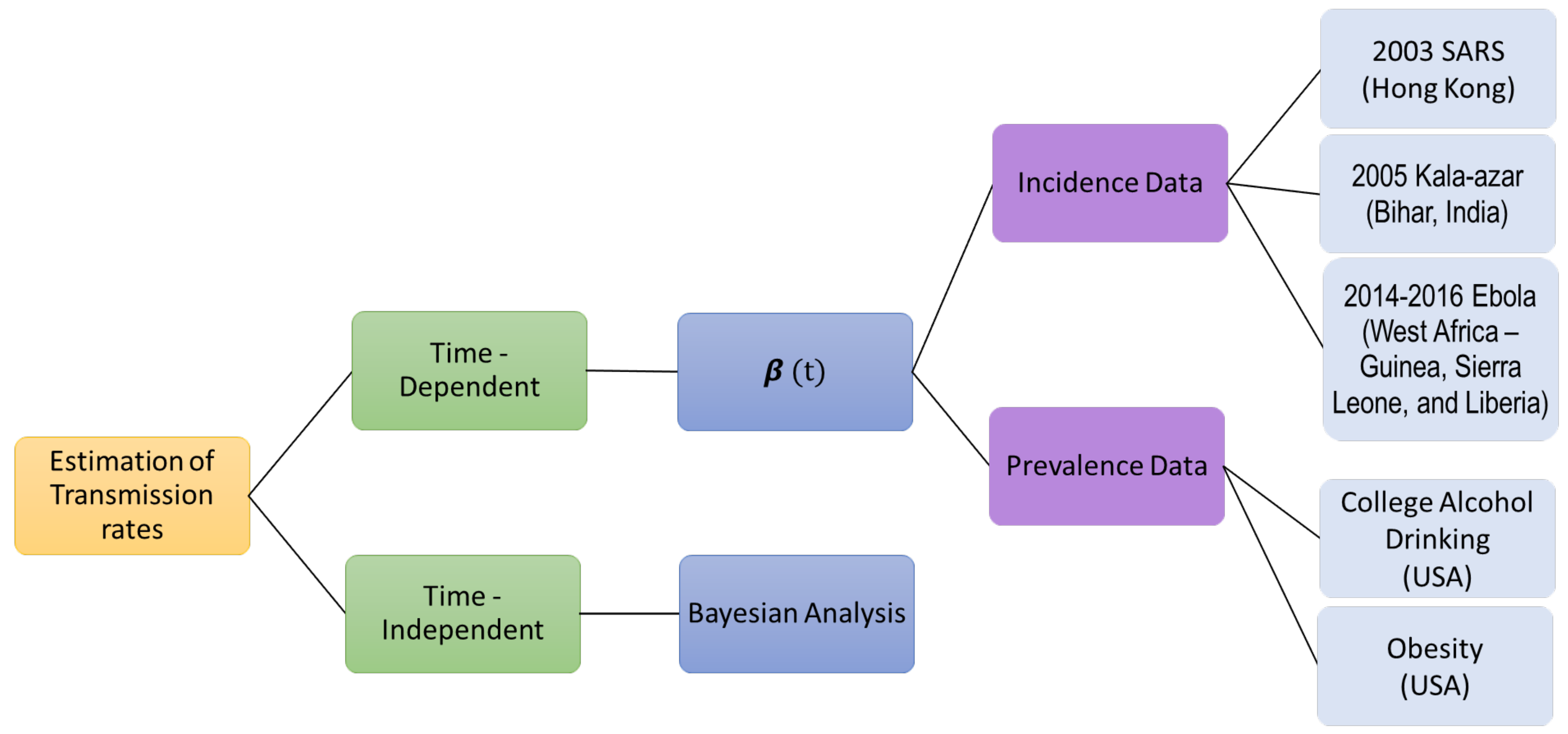
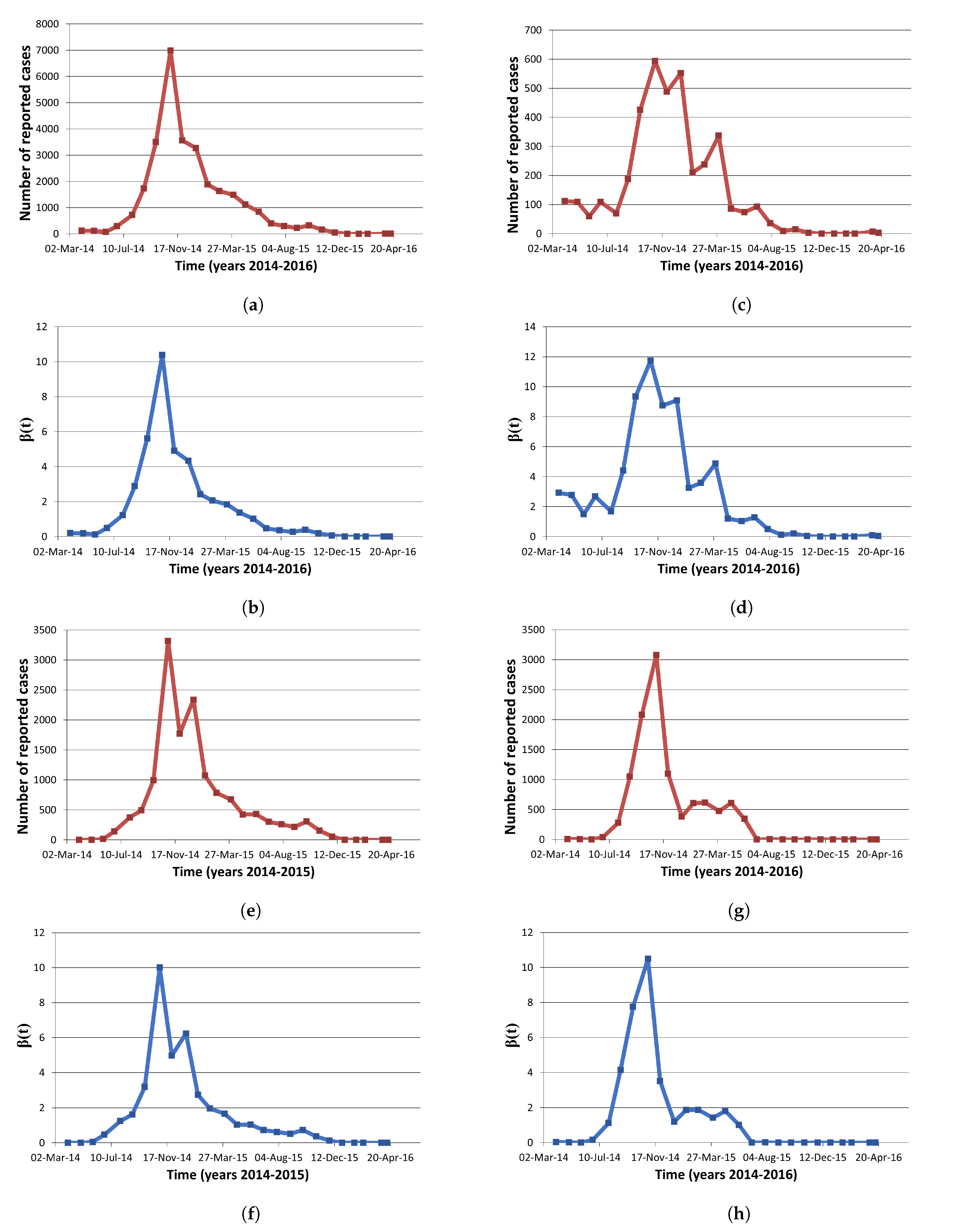
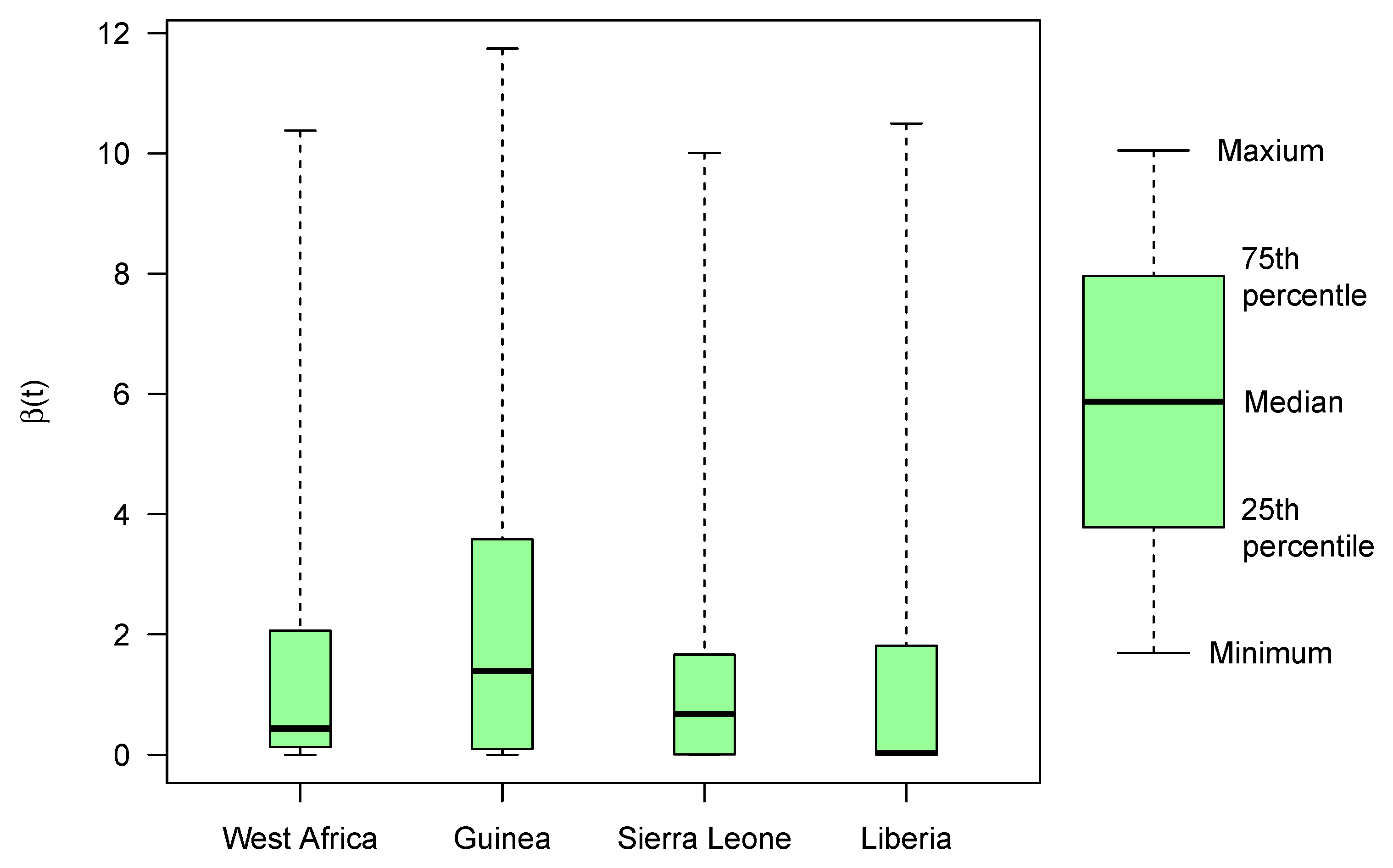
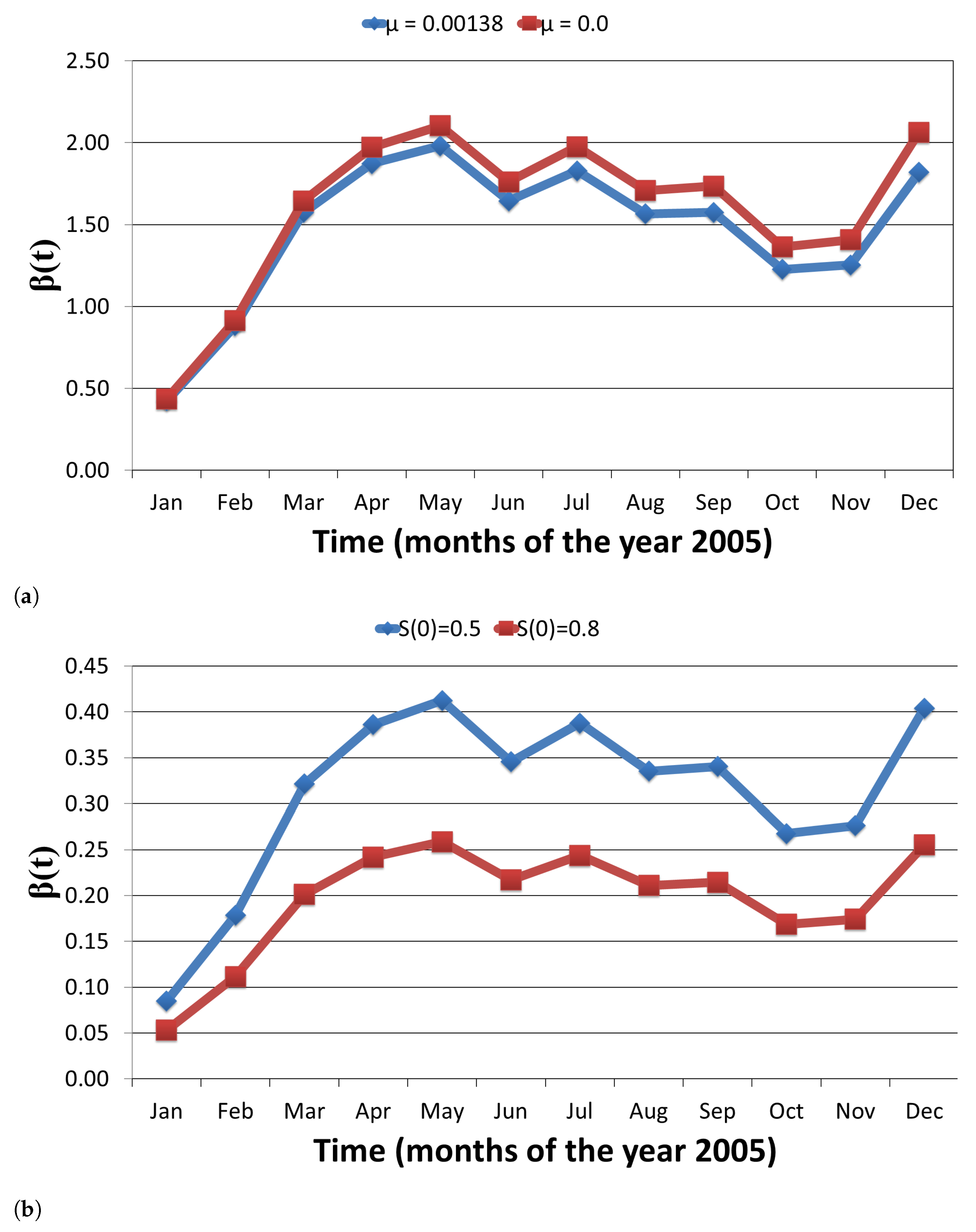
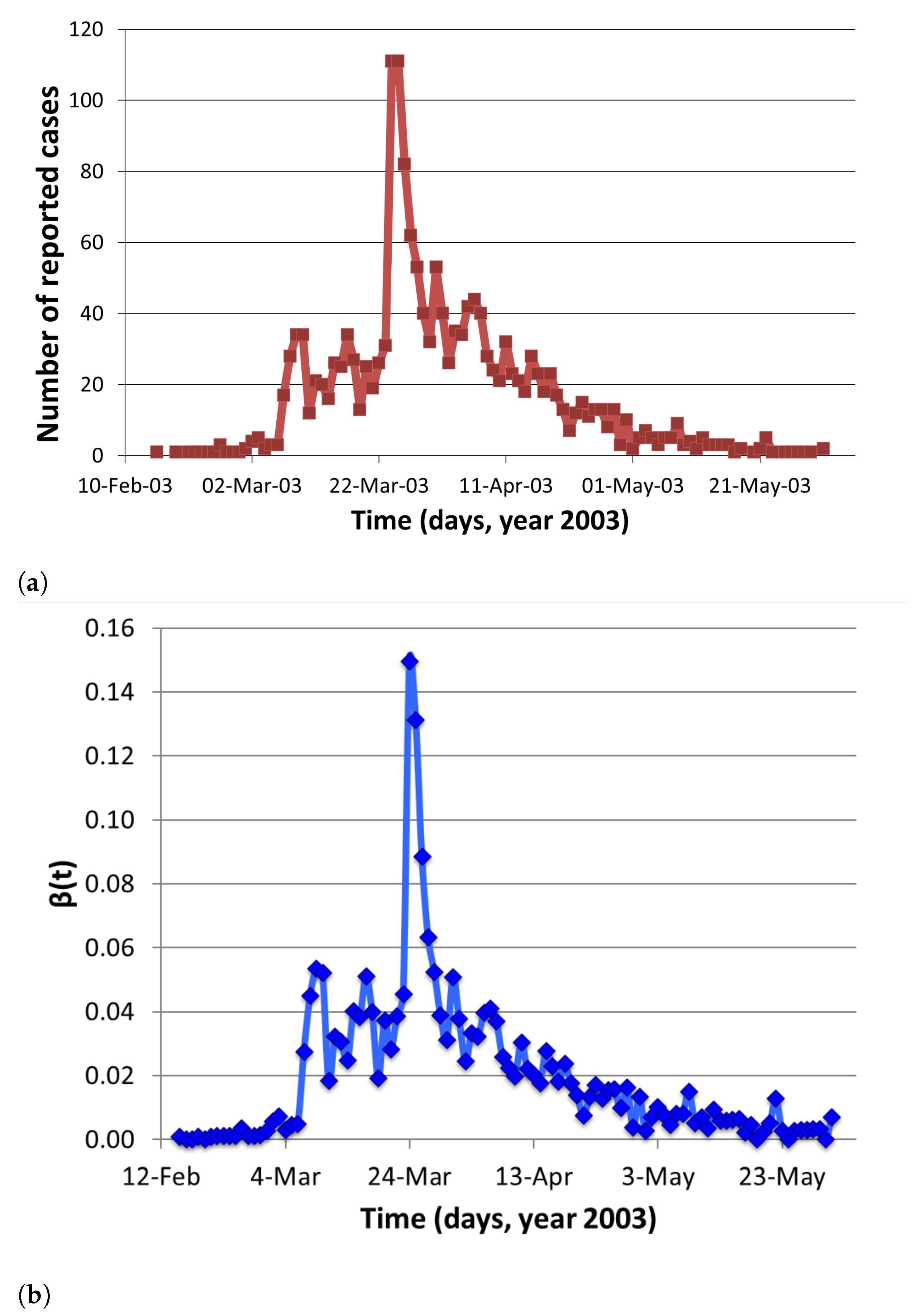
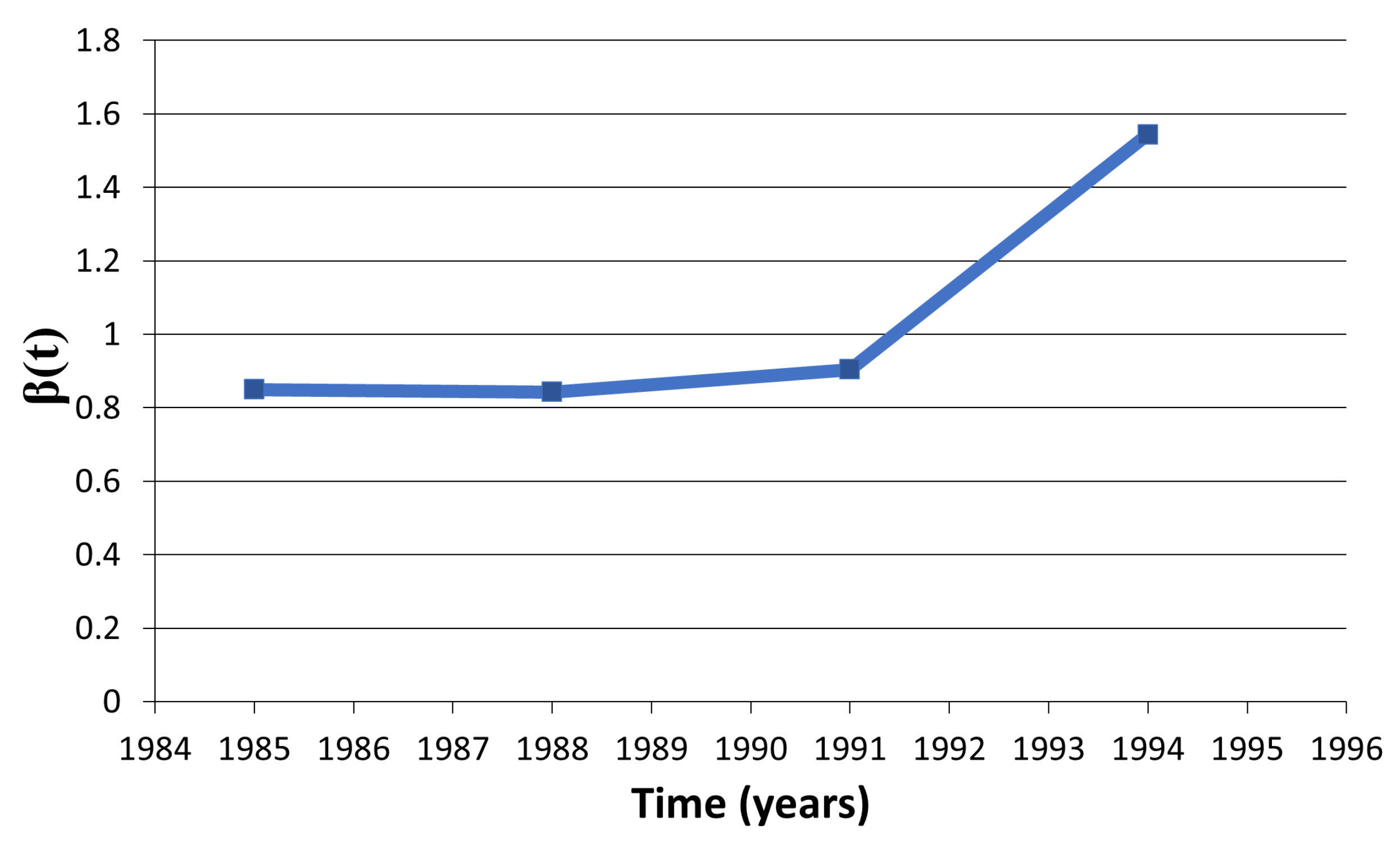
Examples of social problems such as alcohol drinking and obesity and infectious diseases such as Ebola, Visceral Leishmaniasis (or Kala-azar), and SARS are used to show relevance of the analytical work. The available data of US college alcohol drinking and obesity outbreak in US include prevalence trends, whereas incidence data of Ebola outbreak in West Africa (Guinea, Sierra Leone, and Liberia), Kala-azar outbreak in Bihar, and SARS epidemic in Hong Kong are used for the estimation.
In this paper, we compute time-dependent and -independent transmission coefficient of Ebola virus disease along with other health care problems such as college alcohol drinking, the obesity epidemic in United States, the spread of Visceral Leshmaniasis, and the spread of the 2003 SARS Outbreak in Hong Kong. The remaining paper is stratified as follows:
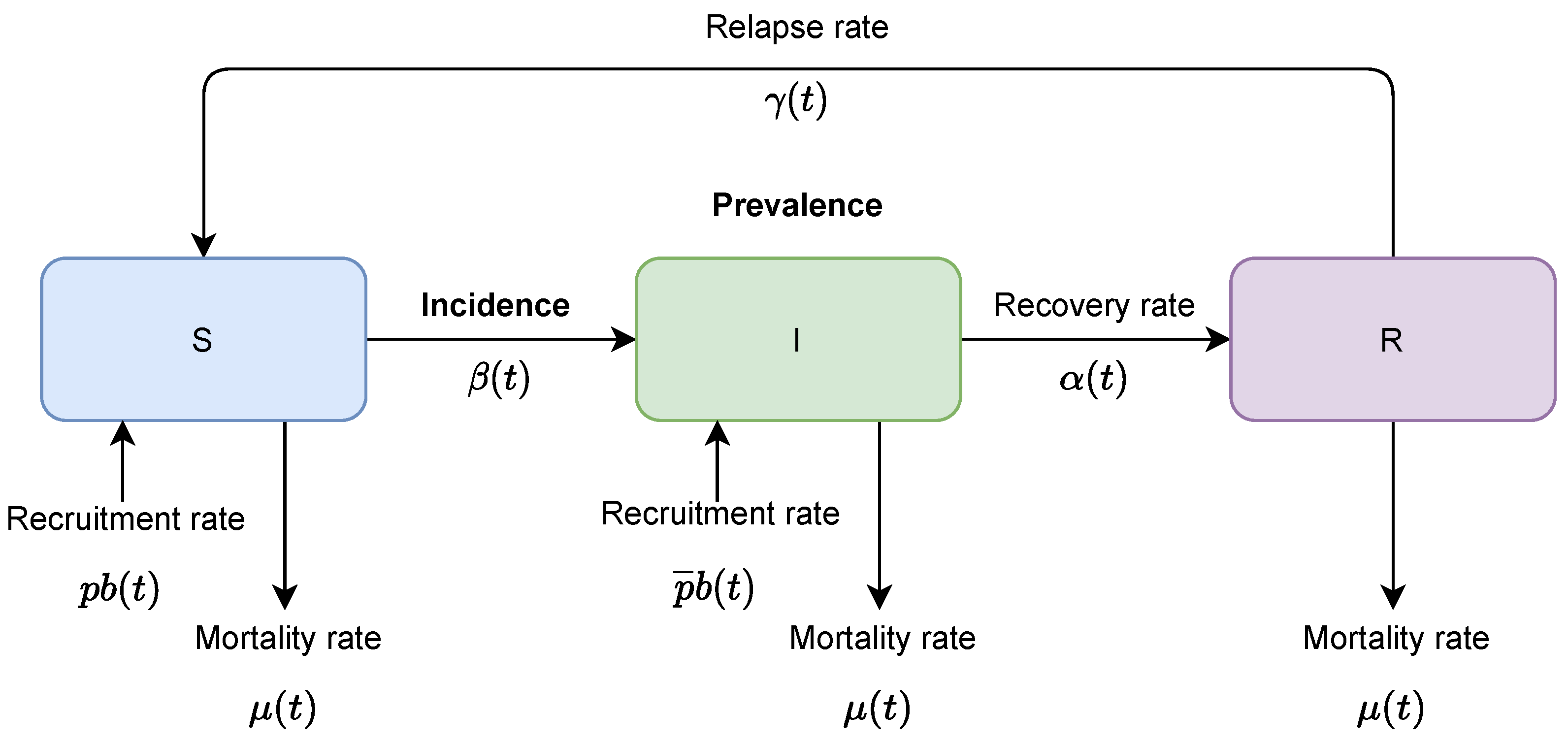
Section 2 provides a compartmental SIR model and two analytical expressions of transmission coefficients based on prevalence and incidence data; examples for computing coefficient over time using each of the two expressions and field data are shown in
Section 3; and finally, the results are discussed in
Section 4.
Figure 1 represents the overview of this paper.
4. Discussion
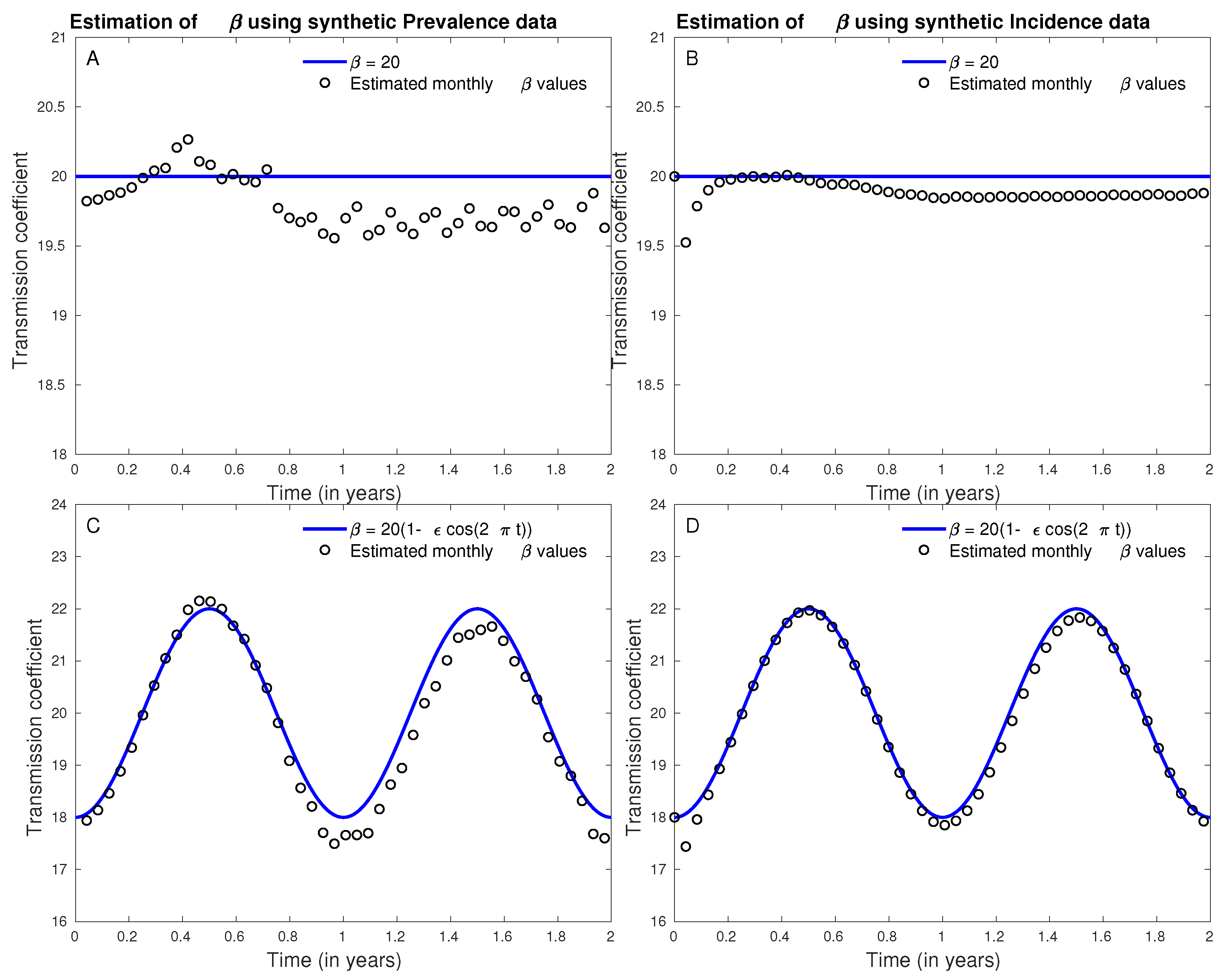
Compartmental models have provided valuable insights into the epidemiology of many infectious diseases. Transmission coefficient, a product of contact rate and probability of transmission given a contact, is a parameter in the compartmental model which naturally varies over time. This coefficient had the greatest effect on predictions of dynamics of disease or social problem and difficult to estimate. However, due to lack of detailed data as well as complexities involved in numerical estimating this parameter, most studies estimate it as a time-independent parameter averaging it over the course of epidemic. In this study, we present a method to estimate time-dependent transmission rate using two types of data commonly reported during infectious disease outbreaks: the time series of the number of infectives (or prevalence) and the number of new cases generated during a period of time (or incidence). By deriving an analytical method that uses a standard deterministic model and these data sets to directly estimate , this new approach resolves the computational challenges often involved with more complex model. By applying our approach to several infectious diseases, we illustrate applicability of our methods in various contexts. Moreover, similar approaches can be applied with any appropriate mathematical model to derive time-dependent transmission rate for diseases whose dynamics may need to incorporate other factors such as environment (for. e.g., role of waterbodies in cholera spread) or vector dynamics (for. e.g., impact of mosquito in dengue transmission).
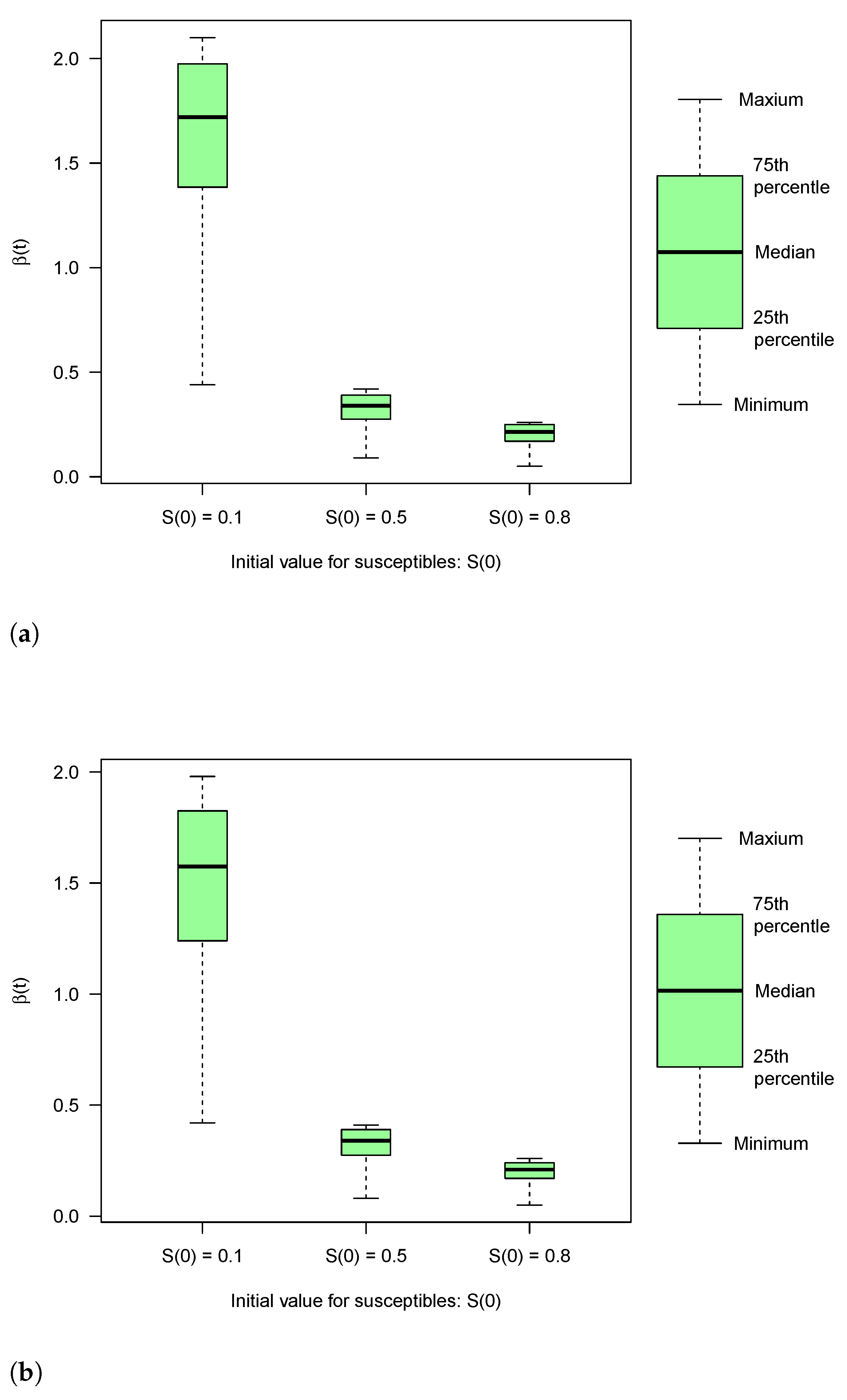
Utility of approach presented in this manuscript is demonstrated using several public-health problems including Ebola, Visceral Leishmaniasis, US college alcohol drinking and obesity outbreak in the US. In particular, we estimated the temporal estimates of transmission rate for Ebola during 2014–2016 outbreak in West Africa (aggregated) as well as for individual countries of Liberia, Guinea and Sierra Leone. Our results though limited by the accuracy of data, demonstrated the wide-variability in transmission risks across the three countries. Moreover, we found that our temporal estimates of transmission risk followed the pattern of incidence closely, but slightly delayed, reflecting the substantial contribution of transmission risk towards the nature of disease progression. During the times of public-health emergencies due to an infectious disease outbreaks such as Ebola outbreak in West Africa or ongoing COVID-19 pandemic, effective reproductive numbers are often estimated using incidence data to understand the progression of disease and inform strategies to curb the transmission. Although estimates of effective reproductive numbers are useful, combining it with estimation of time-varying transmission risk through our approach can be more informative to inform public-health decision-making. Transmission risk at a particular time is a product of contacts and probability of transmission. Thus, it can be used to make short term predictions about new infections as well as it can inform how much reduction in contact patterns or risk of transmission (through mask/vaccination/hygiene) can reduce the transmission parameter sufficiently to reverse the trend of an epidemic.
In the current study, we used simple deterministic model along with simple integration numerical techniques to show how commonly reported data (incidence and prevalence) can be used in informing temporal transmission risk, and thus manage public-health challenges more effectively. Practical application of our approach would improve with use of more complex models (appropriate) as well more sophisticated integration techniques. Moreover, analytical derivation can be used to understand the impact of changes in any other input parameter (such as smaller/longer quarantine periods) on transmission risk in a straight-forward way. Similarly, an area of future research can expand presented framework to understand how incomplete data may alter the quality of parameter estimation. Therefore, value of analysis reported here is as a beginning point for future research that will build on current approach to develop computational models that can inform policies in swift manner during public-health emergencies. We believe using our methods can provide good approximation of time-dependent transmission coefficients and goodness of approximation should increase with use of more sophisticated modeling techniques.


 ,
, 

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}