Tinea Capitis Caused by Microsporum audouninii: A Report of Two Cases from Côte D’Ivoire, West Africa

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Skin Surveys
2.2. Laboratory Investigations
2.3. Ethical Declaration
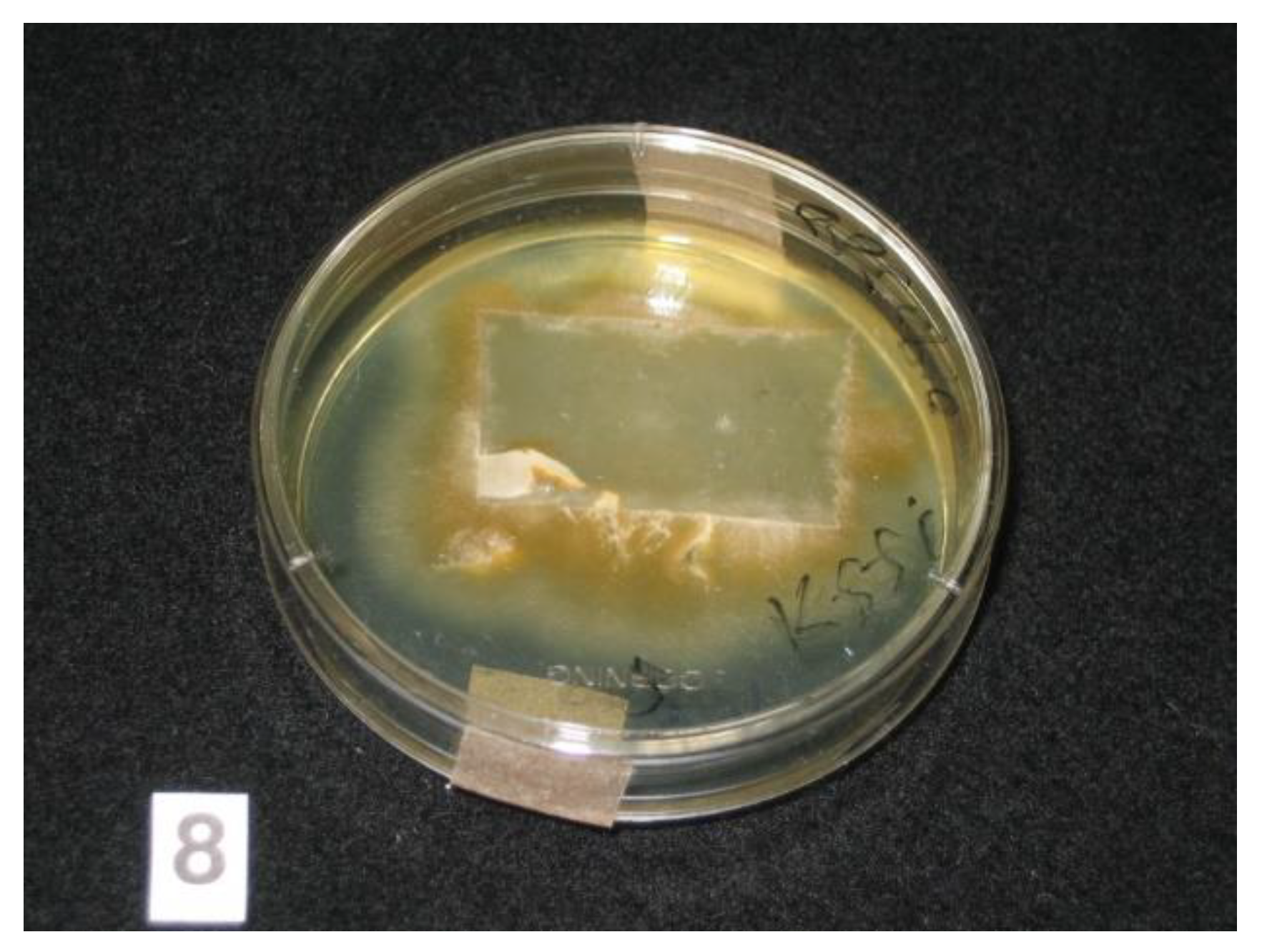
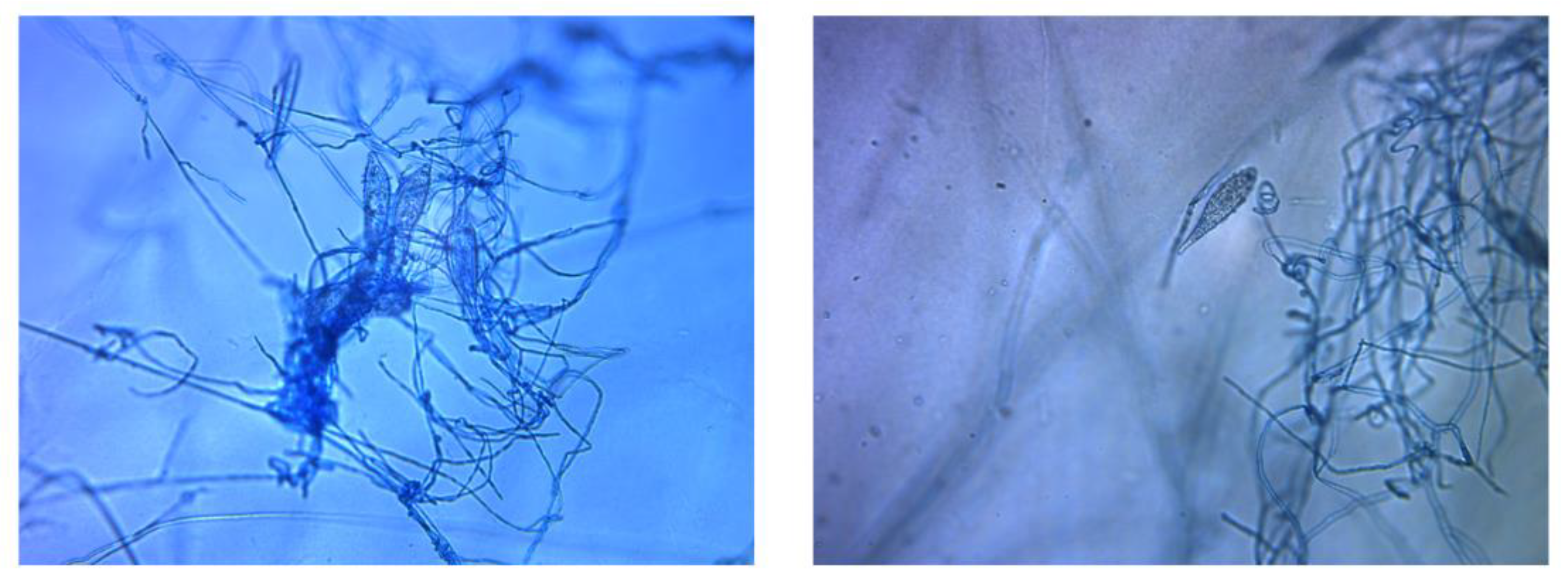
3. Case Reports and Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| M. | Microsporum |
| PCR | polymerase chain reaction |
| SDA | Sabouraud dextrose agar |
References
- Hay, R.J. Tinea Capitis: Current Status. Mycopathologia 2017, 182, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Hogewoning, A.A.; Adegnika, A.A.; Bouwes Bavinck, J.N.; Yazdanbakhsh, M.; Kremsner, P.G.; van der Raaij-Helmer, E.M.; Staats, C.C.G.; Willemze, R.; Lavrijsen, A.P.M. Prevalence and causative fungal species of tinea capitis among schoolchildren in Gabon. Mycoses 2011, 54, e354–e359. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Epidemiology and Management of Common Skin Diseases in Children in Developing Countries; World Health Organization/Department of Child and Adolescent Health and Development: Geneva, Switzerland, 2005. [Google Scholar]
- Coulibaly, O.; L’Ollivier, C.; Piarroux, R.; Ranque, S. Epidemiology of human dermatophytoses in Africa. Med. Mycol. 2018, 56, 145–161. [Google Scholar] [CrossRef] [PubMed]
- Yotsu, R.R.; Comoé, C.C.; Ainyakou, G.T.; Konan, N.; Akpa, A.; Yao, A.; Aké, J.; Vagamon, B.; Abbet, R.A.; Bedimo, R.; et al. Impact of common skin diseases on children in rural Côte d’Ivoire with leprosy and Buruli ulcer co-endemicity: A mixed methods study. PLoS Negl. Trop. Dis. 2020, 14, e0008291. [Google Scholar] [CrossRef]
- Zhan, P.; Liu, W. The Changing Face of Dermatophytic Infections Worldwide. Mycopathologia 2017, 182, 77–86. [Google Scholar] [CrossRef]
- Oke, O.O.; Onayemi, O.; Olasode, O.A.; Omisore, A.G.; Oninla, O.A. The Prevalence and Pattern of Superficial Fungal Infections among School Children in Ile-Ife, South-Western Nigeria. Dermatol. Res. Pract. 2014, 2014, 1–7. [Google Scholar] [CrossRef]
- Ayanbimpe, G.; Taghir, H.; Diya, A.; Wapwera, S. Tinea capitis among primary school children in some parts of central Nigeria. Mycoses 2008, 51, 336–340. [Google Scholar] [CrossRef]
- Yotsu, R.R.; Kouadio, K.; Vagamon, B.; N’Guessan, K.; Akpa, A.J.; Yao, A.; Aké, J.; Abbet, R.A.; Agbor, B.T.A.; Bedimo, R.; et al. Skin disease prevalence study in schoolchildren in rural Côte d’Ivoire: Implications for integration of neglected skin diseases (skin NTDs). PLoS Negl. Trop. Dis. 2018, 12, e0006489. [Google Scholar] [CrossRef]
- Makimura, K.; Mochizuki, T.; Hasegawa, A.; Uchida, K.; Saito, H.; Yamaguchi, H. Phylogenetic classification of Trichophyton mentagrophytes complex strains based on DNA sequences of nuclear ribosomal internal transcribed spacer 1 regions. J. Clin. Microbiol. 1998, 36, 2629–2633. [Google Scholar] [CrossRef]
- White, T.J.; Bruns, T.; Lee, S.; Taylor, J. Amplification and Direct Sequencing of Fungal Ribosomal RNA Genes for Phylogenetics; Innis, M.A., Gelfand, D.H., Sninsky, J.J., White, T.J., Eds.; Academic Press: New York, NY, USA, 1990; pp. 315–322. [Google Scholar]
- Robert, V.; Stegehuis, G.; Stalpers, J. The MycoBank Engine and Related Databases. Available online: https://www.mycobank.org/ (accessed on 1 December 2020).
- Robert, V.; Vu, D.; Amor, A.B.H.; van de Wiele, N.; Brouwer, C.; Jabas, B.; Szoke, S.; Dridi, A.; Triki, M.; Daoud, S.B.; et al. MycoBank gearing up for new horizons. IMA Fungus 2013, 4, 371–379. [Google Scholar] [CrossRef]
- Havlickova, B.; Czaika, V.A.; Friedrich, M. Epidemiological trends in skin mycoses worldwide. Mycoses 2008, 51, 2–15. [Google Scholar] [CrossRef] [PubMed]
- Koffi, A.P.; Yao, T.A.K.; Barogui, Y.T.; Diez, G.; Djakeaux, S.; Zahiri, M.H.; Sopoh, G.E.; Santos, S.; Asiedu, K.; Johnson, R.C.; et al. Integrated approach in the control and management of skin neglected tropical diseases in three health districts of Côte d’Ivoire. BMC Public Health 2020, 20, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Barogui, Y.T.; Diez, G.; Anagonou, E.; Johnson, R.C.; Gomido, I.C.; Amoukpo, H.; Bachirou, Z.S.; Houezo, J.G.; Saizonou, R.; Sopoh, G.E.; et al. Integrated approach in the control and management of skin neglected tropical diseases in Lalo, Benin. PLoS Negl. Trop. Dis. 2018, 12, e0006584. [Google Scholar] [CrossRef] [PubMed]
- Fulgence, K.K.; Abibatou, K.; Vincent, D.; Henriette, V.; Etienne, A.K.; Kiki-Barro, P.C.; Yavo, W.; Koné, M.; Menan, E.I.H. Tinea capitis in schoolchildren in southern Ivory Coast. Int. J. Dermatol. 2013, 52, 456–460. [Google Scholar] [CrossRef]
- Ménan, E.I.H.; Zongo-Bonou, O.; Rouet, F.; Kiki-Barro, P.C.; Yavo, W.; N’Guessan, F.N.; Koné, M. Tinea capitis in schoolchildren from lvory Coast (western Africa). A 1998-1999 cross-sectional study. Int. J. Dermatol. 2002, 41, 204–207. [Google Scholar] [CrossRef]
- Chah, K.F.; Majiagbe, K.A.; Kazeem, H.M.; Ezeanyika, O.; Agbo, I.C. Dermatophytes from skin lesions of domestic animals in Nsukka, Enugu State, Nigeria. Vet. Dermatol. 2012, 23. [Google Scholar] [CrossRef]
- Jain, N.; Sharma, M. Biodiversity of keratinophilic fungal flora in university campus, Jaipur, India. Iran J. Public Health 2012, 41, 27–33. [Google Scholar]
- Carod, J.F.; Ratsitorahina, M.; Raherimandimby, H.; Hincky Vitrat, V.; Ravaolimalala Andrianaja, V.; Contet-Audonneau, N. Outbreak of Tinea capitis and corporis in a primary school in Antananarivo, Madagascar. J. Infect. Dev. Ctries. 2011, 5, 732–736. [Google Scholar] [CrossRef]
- Coulibaly, O.; Thera, M.A.; Piarroux, R.; Doumbo, O.K.; Ranque, S. High dermatophyte contamination levels in hairdressing salons of a West African suburban community. Mycoses 2015, 58, 65–68. [Google Scholar] [CrossRef]
- Nweze, E.I.; Eke, I.E. Dermatophytes and dermatophytosis in the eastern and southern parts of Africa. Med. Mycol. 2018, 56, 13–28. [Google Scholar] [CrossRef]
- Coulibaly, O.; Kone, A.K.; Niaré-Doumbo, S.; Goïta, S.; Gaudart, J.; Djimdé, A.A.; Piarroux, R.; Doumbo, O.K.; Thera, M.A.; Ranque, S. Dermatophytosis among Schoolchildren in Three Eco-climatic Zones of Mali. PLoS Negl. Trop. Dis. 2016, 10, e0004675. [Google Scholar] [CrossRef] [PubMed]
- Espinel-Ingroff, A. History of medical mycology in the United States. Clin. Microbiol. Rev. 1996, 9, 235–272. [Google Scholar] [CrossRef] [PubMed]
- Brito-Santos, F.; Figueiredo-Carvalho, M.H.G.; Coelho, R.A.; Sales, A.; Almeida-Paes, R. Tinea Capitis by Microsporum audouinii: Case Reports and Review of Published Global Literature 2000–2016. Mycopathologia 2017, 182, 1053–1060. [Google Scholar] [CrossRef] [PubMed]
- Zink, A.; Papanagiotou, V.; Todorova, A.; Seidl, H.-P.; Niedermeier, A.; Ring, J.; Traidl-Hoffmann, C. Outbreak of Microsporum audouinii in Munich—The return of infectious fungi in Germany. Mycoses 2014, 57, 765–770. [Google Scholar] [CrossRef]
- Sacheli, R.; Adjetey, C.; Darfouf, R.; Harag, S.; Huynen, P.; Meex, C.; Descy, J.; Melin, P.; Arrese, J.; Hayette, M.-P. A one-year survey of Microsporum audouinii infections in Belgium: Epidemiological and genotypic characterization. Clin. Microbiol. Infect. 2016, 22, 285. [Google Scholar] [CrossRef]
- Kieliger, S.; Glatz, M.; Cozzio, A.; Bosshard, P.P. Tinea capitis and tinea faciei in the Zurich area—An 8-year survey of trends in the epidemiology and treatment patterns. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 1524–1529. [Google Scholar] [CrossRef]
- Miranda, M.F.; Silva, A.J. New uses of vinyl tape for reliable collection and diagnosis of common superficial mycoses. SKINmed Dermatol. Clin. 2003, 2, 156–158. [Google Scholar] [CrossRef]
- Raghukumar, S.; Ravikumar, B.C. Potassium hydroxide mount with cellophane adhesive tape: A method for direct diagnosis of dermatophyte skin infections. Clin. Exp. Dermatol. 2018, 43, 895–898. [Google Scholar] [CrossRef]
- Porto, J.A. The use of cellophane tape in the diagnosis of Tinea versicolor. J. Investig. Dermatol. 1953, 21, 229–231. [Google Scholar] [CrossRef]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yotsu, R.R.; Kouadio, K.; Yao, A.; Vagamon, B.; Takenaka, M.; Murota, H.; Makimura, K.; Nishimoto, K. Tinea Capitis Caused by Microsporum audouninii: A Report of Two Cases from Côte D’Ivoire, West Africa. Trop. Med. Infect. Dis. 2021, 6, 9. https://doi.org/10.3390/tropicalmed6010009
Yotsu RR, Kouadio K, Yao A, Vagamon B, Takenaka M, Murota H, Makimura K, Nishimoto K. Tinea Capitis Caused by Microsporum audouninii: A Report of Two Cases from Côte D’Ivoire, West Africa. Tropical Medicine and Infectious Disease. 2021; 6(1):9. https://doi.org/10.3390/tropicalmed6010009
Chicago/Turabian StyleYotsu, Rie Roselyne, Kouamé Kouadio, Aubin Yao, Bamba Vagamon, Motoi Takenaka, Hiroyuki Murota, Koichi Makimura, and Katsutaro Nishimoto. 2021. "Tinea Capitis Caused by Microsporum audouninii: A Report of Two Cases from Côte D’Ivoire, West Africa" Tropical Medicine and Infectious Disease 6, no. 1: 9. https://doi.org/10.3390/tropicalmed6010009
APA StyleYotsu, R. R., Kouadio, K., Yao, A., Vagamon, B., Takenaka, M., Murota, H., Makimura, K., & Nishimoto, K. (2021). Tinea Capitis Caused by Microsporum audouninii: A Report of Two Cases from Côte D’Ivoire, West Africa. Tropical Medicine and Infectious Disease, 6(1), 9. https://doi.org/10.3390/tropicalmed6010009