Diagnosis and Management of Fungal Neglected Tropical Diseases In Community Settings—Mycetoma and Sporotrichosis

Abstract
:1. Introduction
2. Methods
3. Results
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bonifaz, A.; Tirado Sánchez, A.; Calderón, L.; Saul, A.; Araiza, J.; Hernández, M.; González, G.M.; Ponce, R.M. Mycetoma: Experience of 482 cases in a single center in Mexico. PLoS Negl. Trop. Dis. 2014, 8. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Mtnez, R.; Mendez-Tovar, L.J.; Bonifaz, A.; Arenas, R.; Mayorga, J.; Welsh, O.; Vera-Cabrera, L.; Padilla-Desgarennes, M.C.; Contreras Pérez, C.; Chávez, G. Update on the epidemiology of Mycetoma in Mexico. A review of 3933 cases. Gac. Med. Mex. 2013, 149, 586–592. [Google Scholar]
- Van de Sande, W. Global burden of human mycetoma: A systemic review and metanalisis. PLoS Negl. Trop. Dis. 2013, 7. [Google Scholar] [CrossRef]
- WHO. Available online: https://www.who.int/neglected_diseases/mediacentre/WHA_69.21_Eng.pdf?ua=1 (accessed on 2 February 2019).
- Werner, A.; Werner, B. Sporotrichosis in man and animals. Int. J. Dermatol. 1994, 33, 692–700. [Google Scholar] [CrossRef] [PubMed]
- Conti, A.D. Sporotrichosis in Latin America. Mycopath 1989, 108, 113–116. [Google Scholar]
- Corcho-Berdugo, A.; Muñoz Hndez, B.; Palma-Cortes, G.; Ramirez Hndez, A.; Martínez-Rivera, M.; Frías-de León, M.; Reyes-Montes, M.; Martínez-Valadez, E.; Manjarrez-Zavala, M.; Alfaro-Ramos, L.; et al. Brote inusual de histoplasmosis en residentes del estado de México. Gaceta Med. Mex. 2011, 5, 377–384. [Google Scholar]
- Mayorga, P.; Epinoza, H. Coccidioidomycosis in México and Central America. Mycopathol. Mycol. Appl. 1970, 41, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Martinez, R.; Hernandez-Hernandez, F.; Mendez-Tovar, LJ.; Manzano-Gayosso, P.; Bonifaz, A.; Arenas, R.; Padilla-Desgarennes Mdel, C.; Estrada, R.; Chávez, G. Paracoccidioidomycosis en Mexico. Clinical and epidemiological data from 93 new cases (1972–2012). Mycoses 2014, 57, 525–530. [Google Scholar] [CrossRef]
- Chavez, L.G.; Estrada, C.R.; Estrada, C.G.; Moreno, C.G. Cromoblastomicosis y micetoma. Informe de un caso por presentación simultanea de Fonseca pedrosoi y Nocardia brasiliensis. Dermatol. Cosm. Med. Quir. 2014, 12, 268–271. [Google Scholar]
- Estrada, C.R.; Chavez, L.G.; Estrada, C.G.; Bonifaz, A. Report of 73 cases of cutaneous sporotrichosis in Mexico. An. Bras. Dermatol. 2018, 93, 907–909. [Google Scholar] [CrossRef]
- Estrada, C.R.; Chavez-Lopez, M.G.; Estrada-Chavez, G.; Paredes-Solis, S. Specialized dermatological care for marginalized populations and education at primary care level: Is community dermatology a feasible proposal? Int. J. Dermatol. 2012, 51, 1345–1350. [Google Scholar] [CrossRef]
- Hay, R.J.; Estrada, C.R.; Grossmann, H. Managing skin disease in resource-poor environments- the role of community oriented training and control programs. Int. J. Dermatol. 2011, 50, 558–563. [Google Scholar] [CrossRef]
- El-Safi, S.; Chappuis, F.; Boelaert, M. The Challenges of Conducting Clinical Research on neglected tropical diseases in remote endemic áreas of Sudan. PLoS Negl. Trop. Dis. 2016, 10. [Google Scholar] [CrossRef] [PubMed]
- Chávez, L.G.; Estrada, C.G.; Orozco, F.M.; Solis, R.A.; Solchaga-Rosas, J.; Armendariz-Valle, F.; Estrada-Castañón, R.A. Teledermatología, un modelo de enseñanza y asistencia en atención primaria a la salud. Gac. Med. Mex. 2018, 154, 1–5. [Google Scholar]
- Lavalle, P.; Padilla, M.C.; Perez, J.; Reynoso, S. Contribución al conocimiento de los micetomas en el estado de Guerrero, México. Origen disctribución geográfica y evolución de 100 casos de micetomas. Dermatol. Rev. Mex. 1988, 42, 232–238. [Google Scholar]
- Chávez, G.; Estrada, R.; Bonifaz, A. Perianal actinomycetoma, experience of 20 cases. Int. J. Dermatol. 2002, 41, 491–493. [Google Scholar] [CrossRef] [PubMed]
- Estrada-Chavez, G.; Estrada, R.; Fernandez, R.; Arenas, R.; Reyes, A.; Guevara, C.; Chávez-López, G. Cervical and middle actinomycetomas from Guerrero State, Mexico. Int. J. Dermatol. 2017, 56, 1146–1149. [Google Scholar] [CrossRef] [PubMed]
- Estrada-Chavez, G.; Estrada, R.; Chavez, G.; Vega Memije, M.; Guzmán, R.; García-Lechuga, M.; Granados, J.; Rangel-Gamboa, L. HLA Class II alleles in human sporotrichosis in Mexican Amerindians. Asia-Pacif. J. Blood Types Genes 2018, 2, 183–190. [Google Scholar]
- Ahmed, A.O.; Van-Leeuwen, W.; Fahal, A.; Van de Sande, W. Mycetoma caused by Madurella mycetomatis: A neglected infectious burden. Lancet Infect. Dis. 2004, 4, 566–574. [Google Scholar] [CrossRef]
- Torres, G.E.; Niebla, M.A. Mycetoma. Clinical and Microbiological Monograph; Scholar Press: Brivibas gatve, Riga, 2015. [Google Scholar]
- Mehantappa, H.; Sruthi, P.; Kusuma, V.; Niveditha, S.R.; Kumar, S.A. Cytological diagnosis of actinomycosis. and eumycetoma. A report of two cases. Diagn. Cytopathol. 2010, 38, 918–920. [Google Scholar]
- Fahal, A.H.; Sjeikh, H.E.; Lider, M.A.; Homeida, M.A.; El Arabi, Y.E.; Mahgoub, E.S. Ultrasonic imaging in mycetoma. Br. J. Surg. 1997, 78, 765–766. [Google Scholar]
- Mubarak, B.S.; Fahal, A.H.; Mudawi, M.A.; El Samani, W.M.; Fathelrahman, R.O.; Eiman, S.A.; El Nour, M.; El Rayah, M.M.; El Sheikh Rahman, M.A.; Suliman, H.S.; et al. A holistic approach to the mycetoma management. PLoS Negl. Trop. Dis. 2018, 12. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| VARIABLE | VALUES | |
|---|---|---|
| GENDER | Male | = 85 (75.2%) |
| Female | = 28 (24.8%) | |
| AGE | Adults > 18a | = 104 (92.0%) |
| Children < 18a | = 9 (8.0%) | |
| OCCUPATION | Farmers | = 53 (48.6%) |
| Housewives | = 23 (21.1%) | |
| Others | = 37 (30.3%) | |
| AFFECTED AREA | Feet | = 34 (30.1%) |
| Legs | = 11 (9.7%) | |
| Upper limbs | = 22 (19.5%) | |
| Pelvic area | = 19 (16.8%) | |
| Abdomen | = 6 (5.3%) | |
| Trunk | = 17 (15.1%) | |
| Cervical column | = 4 (3.5%) | |
| MYCOLOGY | Cultures (+) | = 82 |
| Direct Exam (+) | = 101 | |
| Biopsy | = 79 | |
| X ray | = 75 | |
| CT | = 7 | |
| TYPE OF MYCETOMA | Actinomycetoma | = 81 (78.6%) |
| Eumycetoma | = 22 (21.4%) | |
| ACTINOMYCETES | Nocardia brasiliensis | = 64 (70.4%) |
| Nocardia spp | = 19 (20.9%) | |
| Actinomadura madurae | = 6 ( 6.6%) | |
| N. otitidis caviarum | = 2 (2.1%) | |
| FUNGI | Madurella mycetomatis | = 16 (72.8%) |
| Trematosphaeria grisea | = 3 (13.7%) | |
| Scedosporium boydii | = 2 ( 9.0%) | |
| Phomopsis longicola | = 1 ( 4.5%) | |
| EVOLUTION | <five years | = 84 (74.3%) |
| >five years | = 29 (25.7%) | |
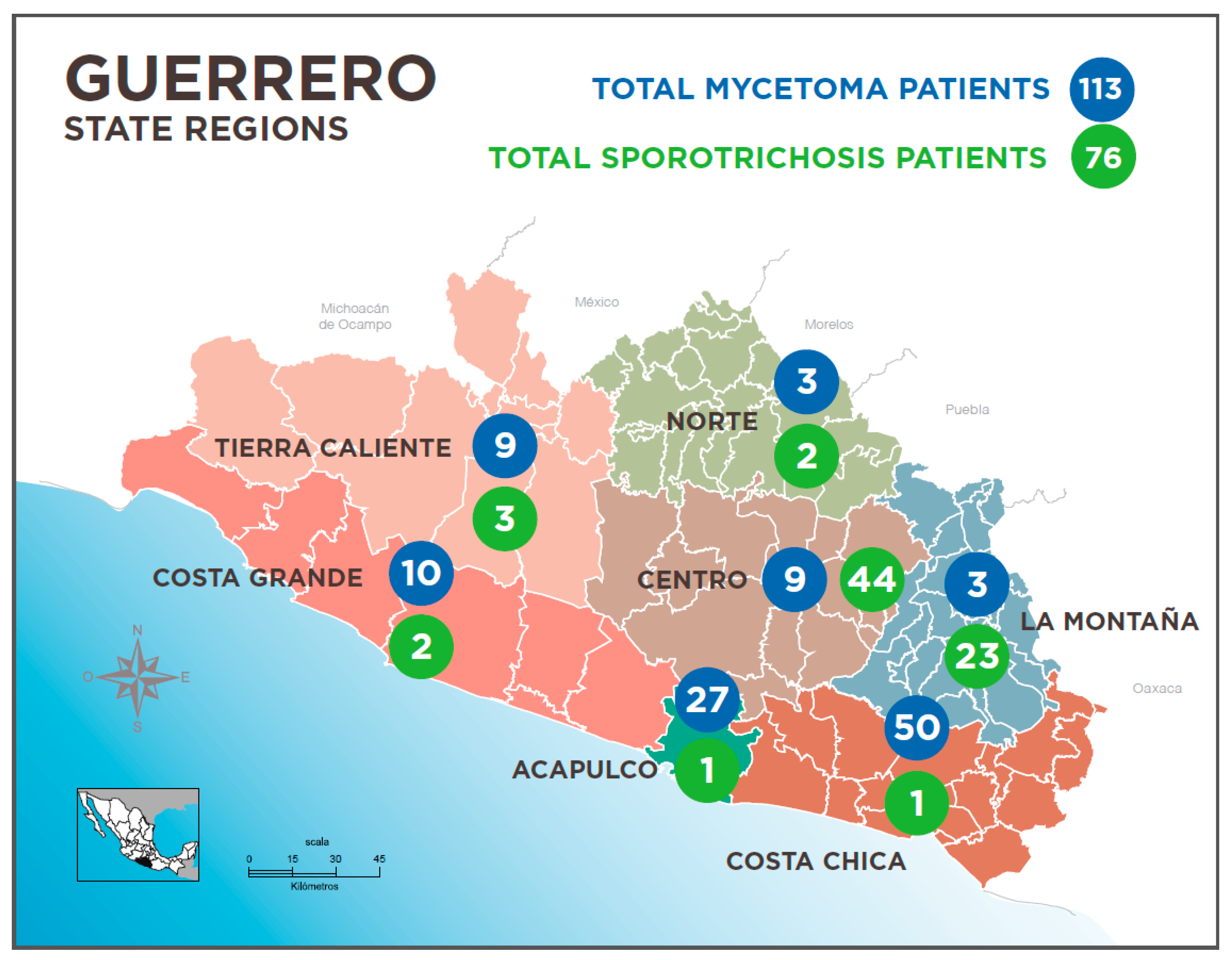
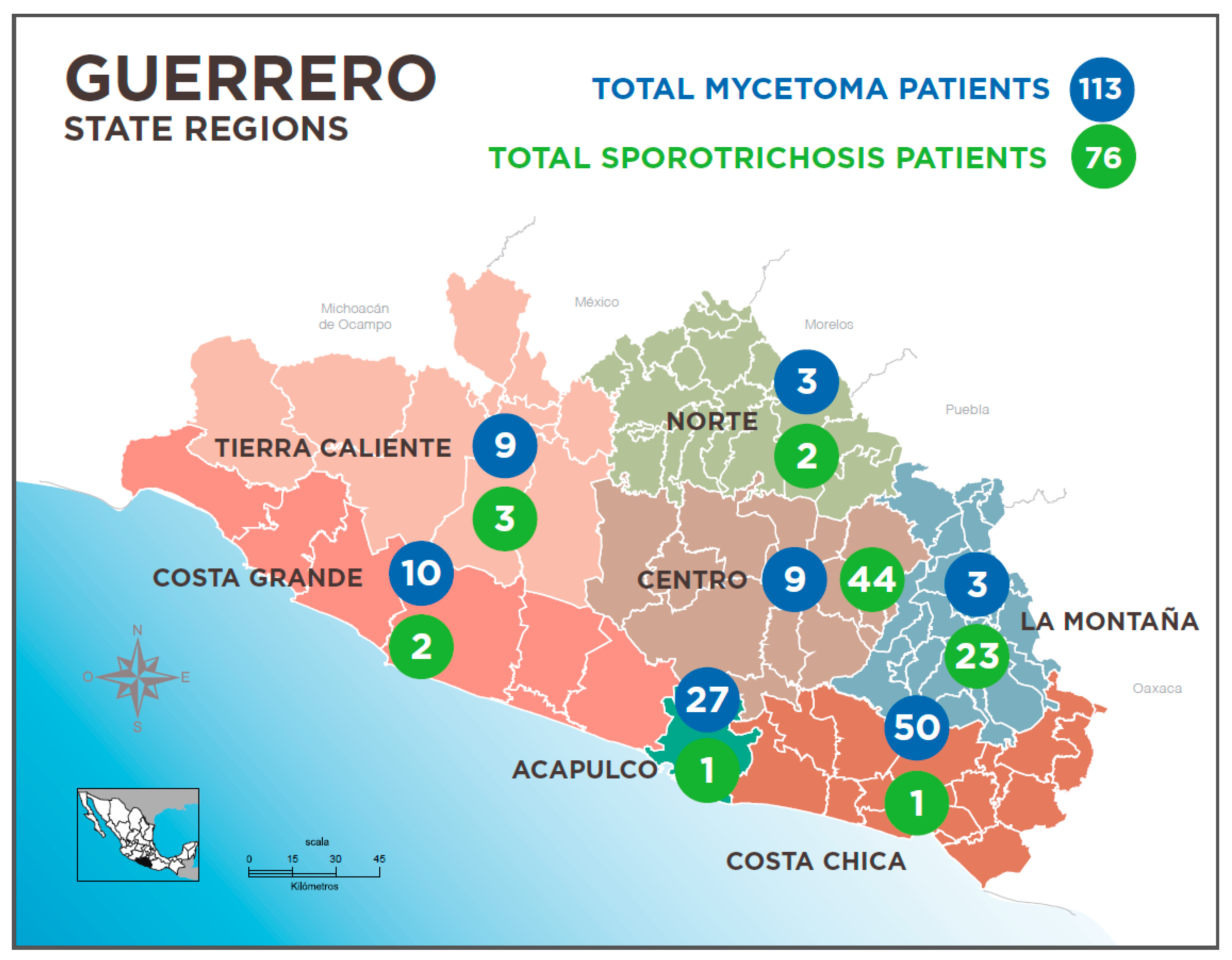
| REGION | Costa Chica | = 50 (44.2%) |
| Acapulco | = 27 (23.9%) | |
| Costa Grande | = 10 (8.8%) | |
| Tierra Caliente | = 9 (8.0%) | |
| Centro | = 9 (8.0%) | |
| Norte | = 5 (4.4%) | |
| Montaña | = 3 (2.7%) | |
| VARIABLE | VALUES | |
| GENDER | Male | = 35 (46.0%) |
| Female | = 41 (54.0%) | |
| AGE | Adults > 18 | = 39 (51.3%) |
| Children < 18 | = 37 (48.7%) | |
| OCCUPATION | Farmers | = 62 (81.6%) |
| Students | = 2 (2.6%) | |
| Children not working | = 12 (15.8%) | |
| AFFECTED AREA | Upper limbs | = 32 (42.1%) |
| Lower limbs | = 16 (21.1%) | |
| Face | = 16 (21.1%) | |
| Trunk | = 4 (5.3%) | |
| Other | = 8 (10.4%) | |
| MYCOLOGY | Cultures | = 52 (+) |
| IDR (Skin Test) 1 | = 45 (+) | |
| Biopsy | = 31 | |
| CLINICAL FORM | Lymphangitic | = 43 (56.8%) |
| Fixed | = 24 (32.2%) | |
| Disseminated | = 8 (11.0%) | |
| EVOLUTION | <1 year | = 18 (23.7%) |
| <5 years | = 41 (53.9%) | |
| >5 years | = 17 (22.4%) | |
| REGION | Centre | = 44 (57.9%) |
| High Mountain | = 23 (30.3%) | |
| Others | = 9 (11.8%) | |
| TREATMENT | Treated | = 56 (73.7%) |
| Not treated | = 20 (26.3%) | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Estrada-Castañón, R.; Estrada-Chávez, G.; Chávez-López, M.d.G. Diagnosis and Management of Fungal Neglected Tropical Diseases In Community Settings—Mycetoma and Sporotrichosis. Trop. Med. Infect. Dis. 2019, 4, 81. https://doi.org/10.3390/tropicalmed4020081
Estrada-Castañón R, Estrada-Chávez G, Chávez-López MdG. Diagnosis and Management of Fungal Neglected Tropical Diseases In Community Settings—Mycetoma and Sporotrichosis. Tropical Medicine and Infectious Disease. 2019; 4(2):81. https://doi.org/10.3390/tropicalmed4020081
Chicago/Turabian StyleEstrada-Castañón, Roberto, Guadalupe Estrada-Chávez, and María de Guadalupe Chávez-López. 2019. "Diagnosis and Management of Fungal Neglected Tropical Diseases In Community Settings—Mycetoma and Sporotrichosis" Tropical Medicine and Infectious Disease 4, no. 2: 81. https://doi.org/10.3390/tropicalmed4020081
APA StyleEstrada-Castañón, R., Estrada-Chávez, G., & Chávez-López, M. d. G. (2019). Diagnosis and Management of Fungal Neglected Tropical Diseases In Community Settings—Mycetoma and Sporotrichosis. Tropical Medicine and Infectious Disease, 4(2), 81. https://doi.org/10.3390/tropicalmed4020081