
Associations between Fluctuating Shame, Self-Esteem, and Sexual Desire: Comparing Frequent Porn Users and a General Population Sample


Abstract
:1. Introduction
The Present Study
2. Method
2.1. Samples and Procedure
2.2. Time-Varying Variables
2.2.1. Sexual Desire
2.2.2. Lagged Sexual Desire
2.2.3. Self-Esteem/Lagged Self-Esteem
2.2.4. Shame/Lagged Shame
2.2.5. Factor Analyses of the Beep Level Variables
2.3. Time-Invariant Variables
2.3.1. Compulsive Porn Use
2.3.2. Group Membership
2.4. Data Analysis
2.5. Data Availability
3. Results
3.1. Descriptives
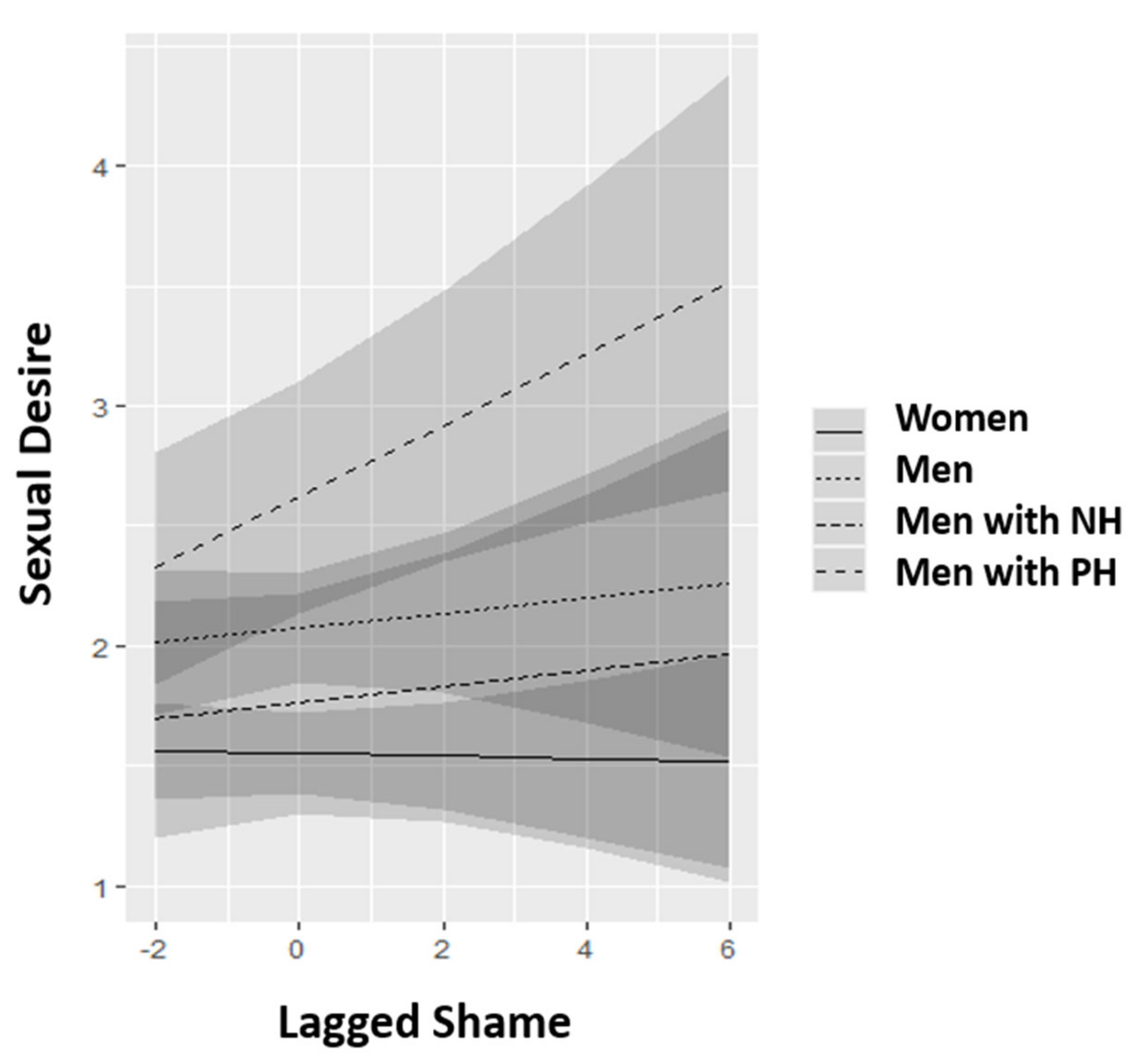
3.1.1. Contemporary and Temporal Analyses of the Associations of Shame and Sexual Desire
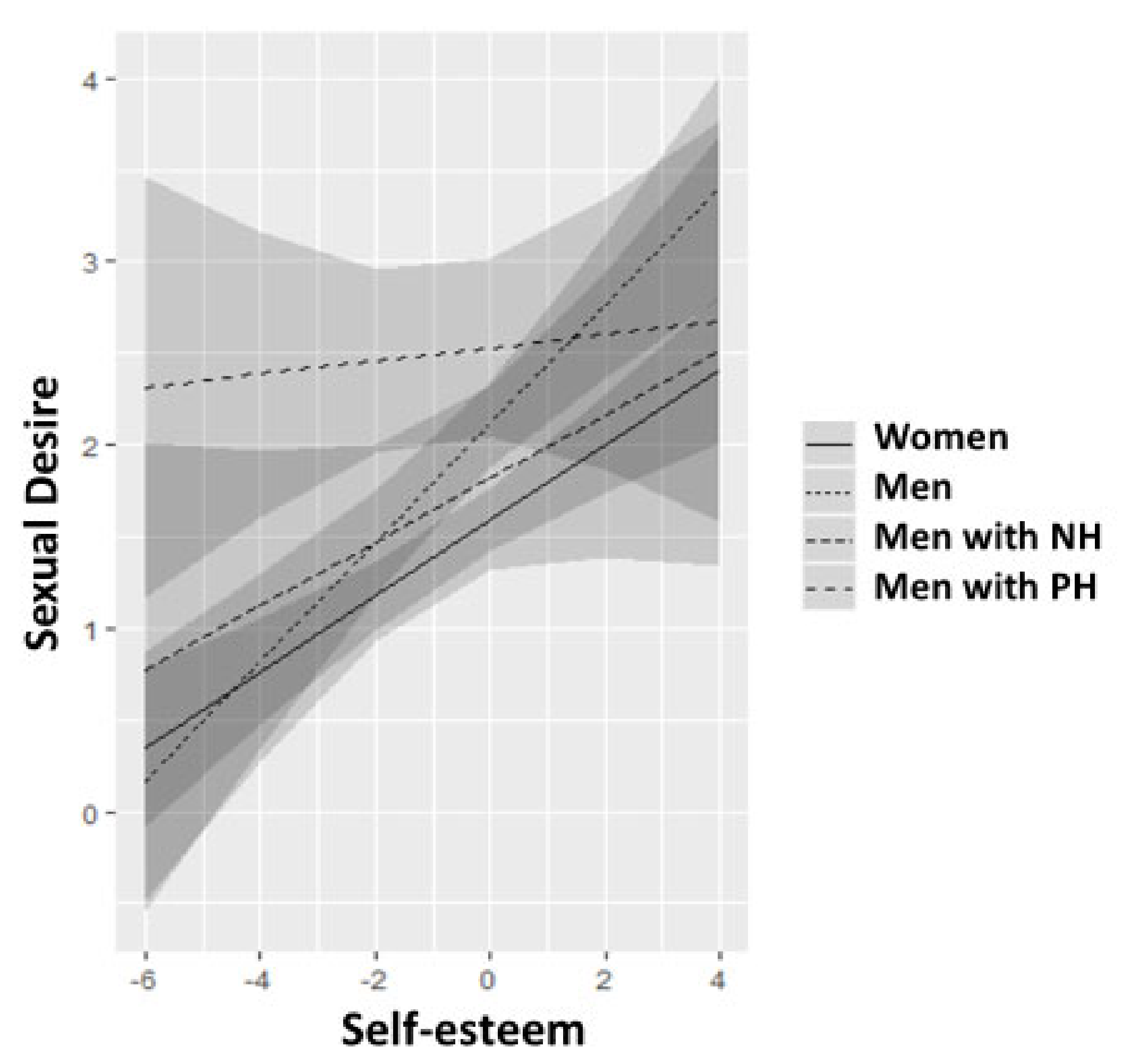
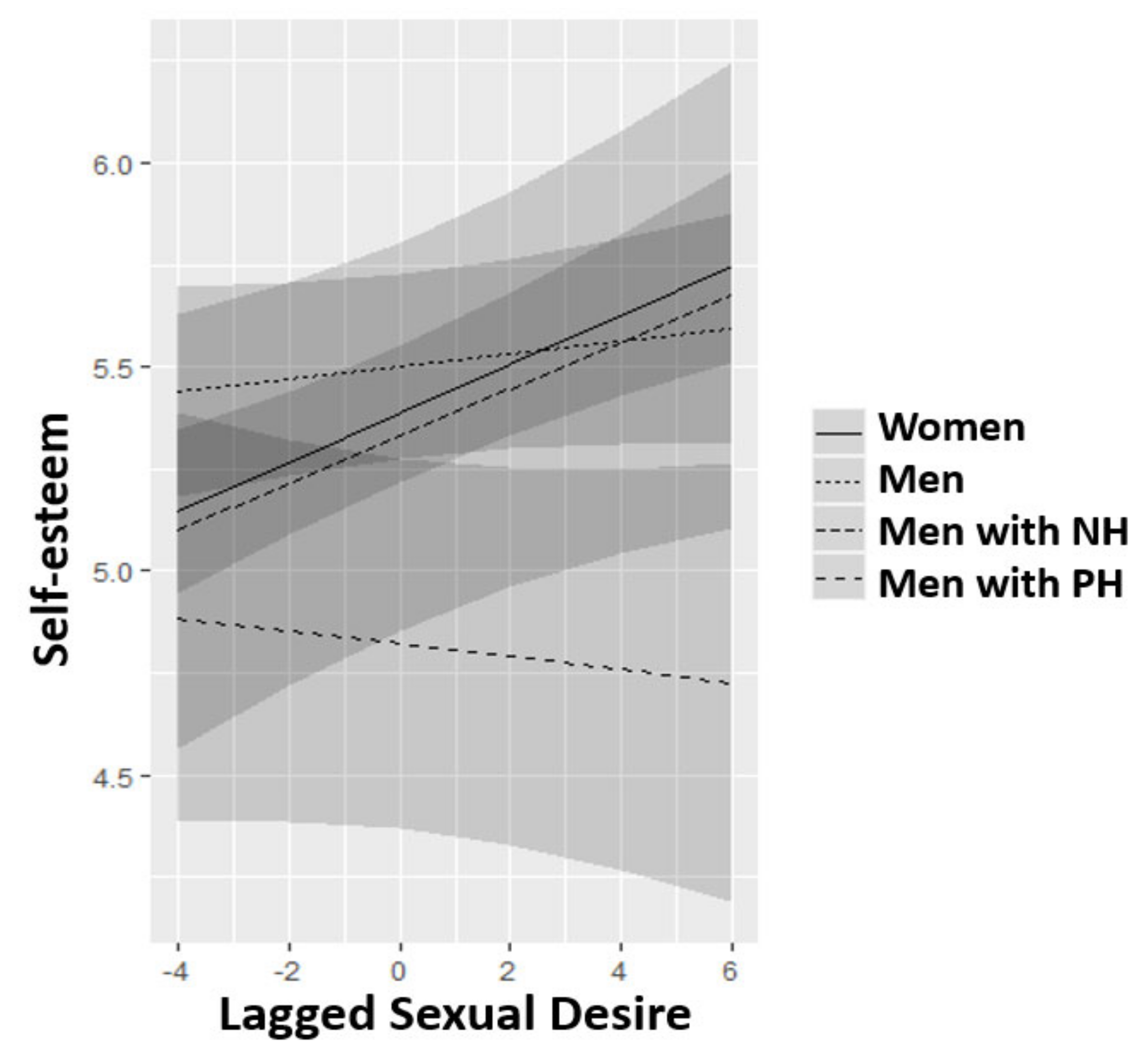
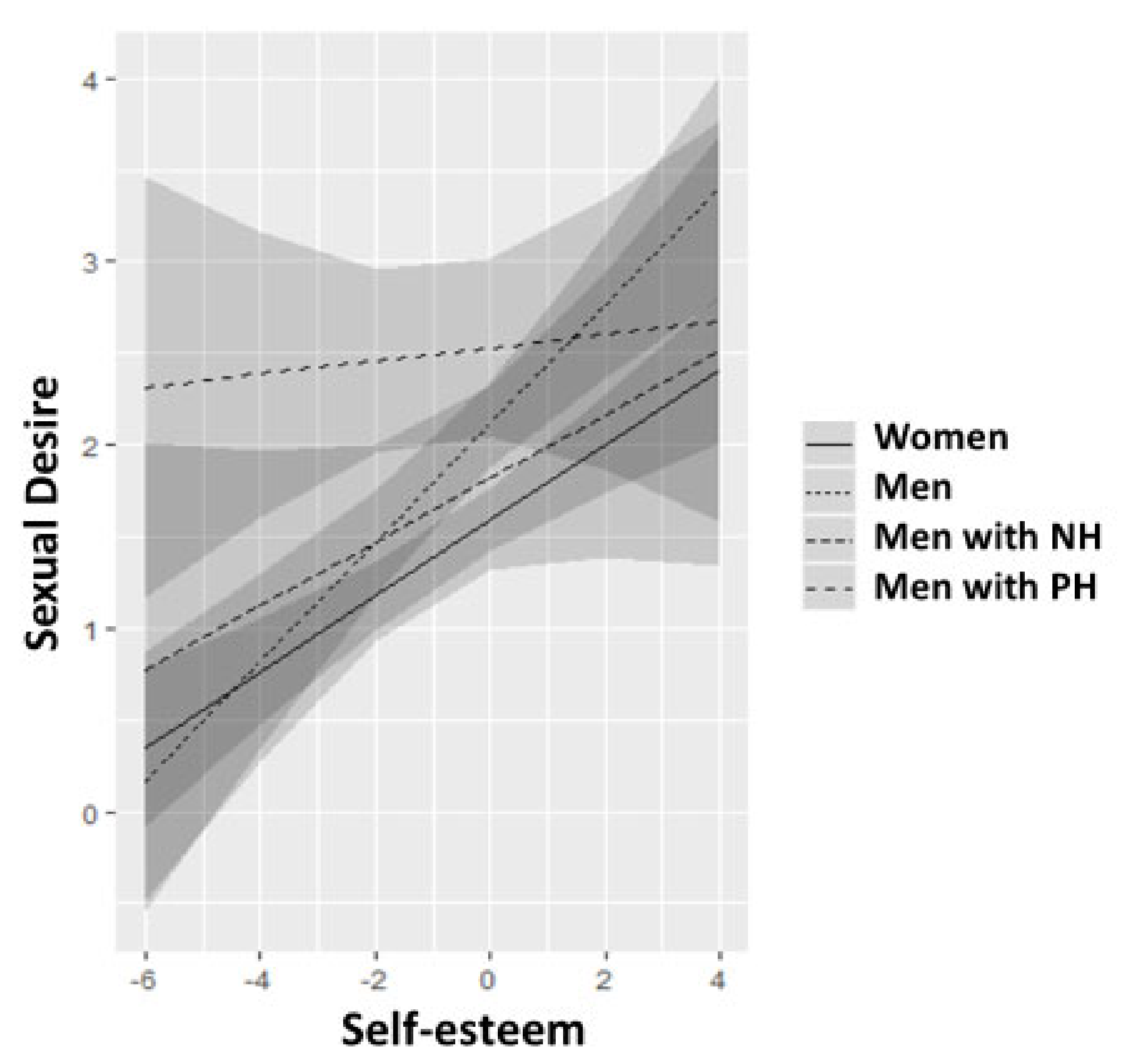
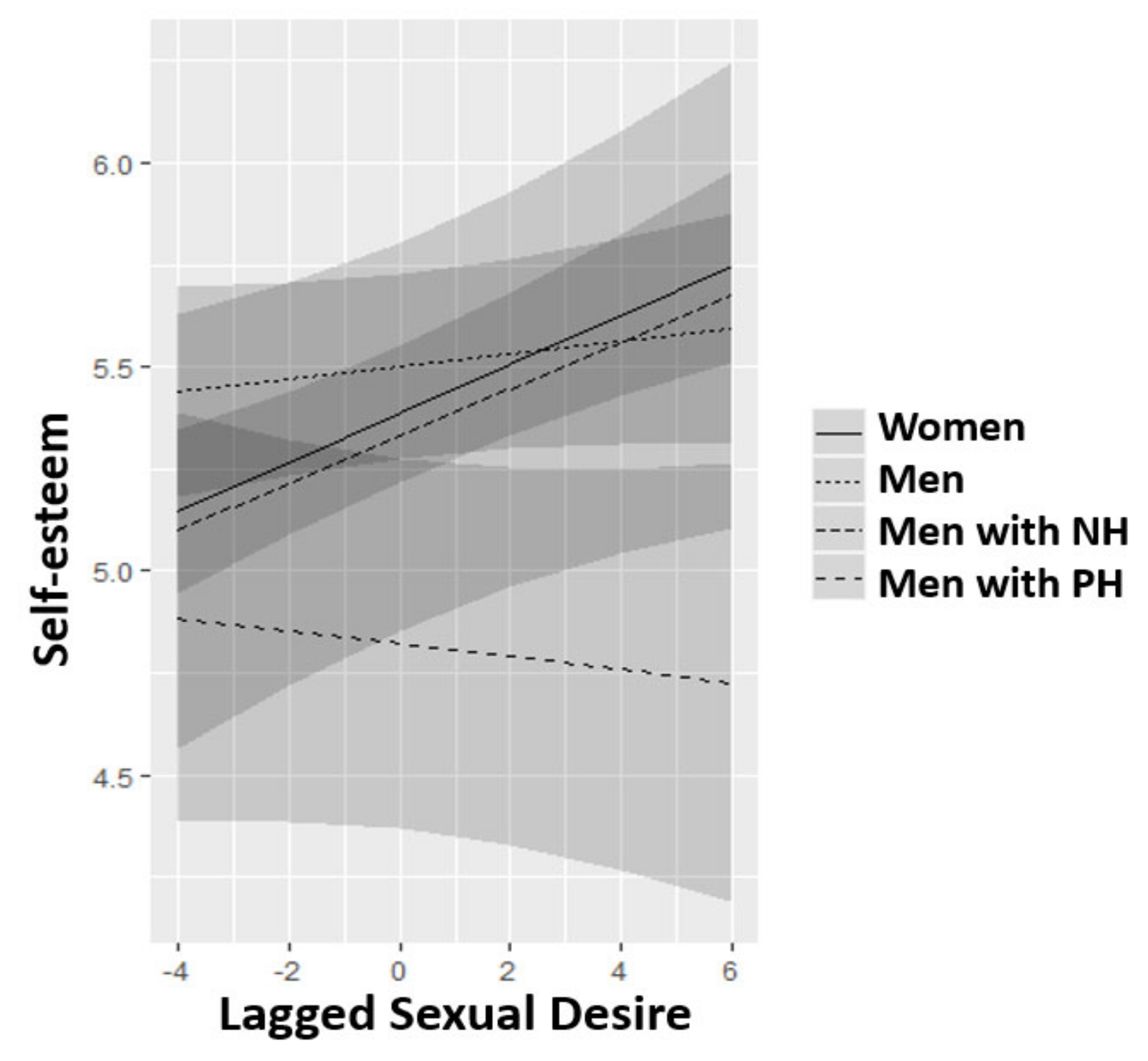
3.1.2. Contemporary and Temporal Analyses of the Associations of Self-Esteem and Sexual Desire
4. Discussion
4.1. Shame and Sexual Desire
4.2. Self-Esteem and Sexual Desire
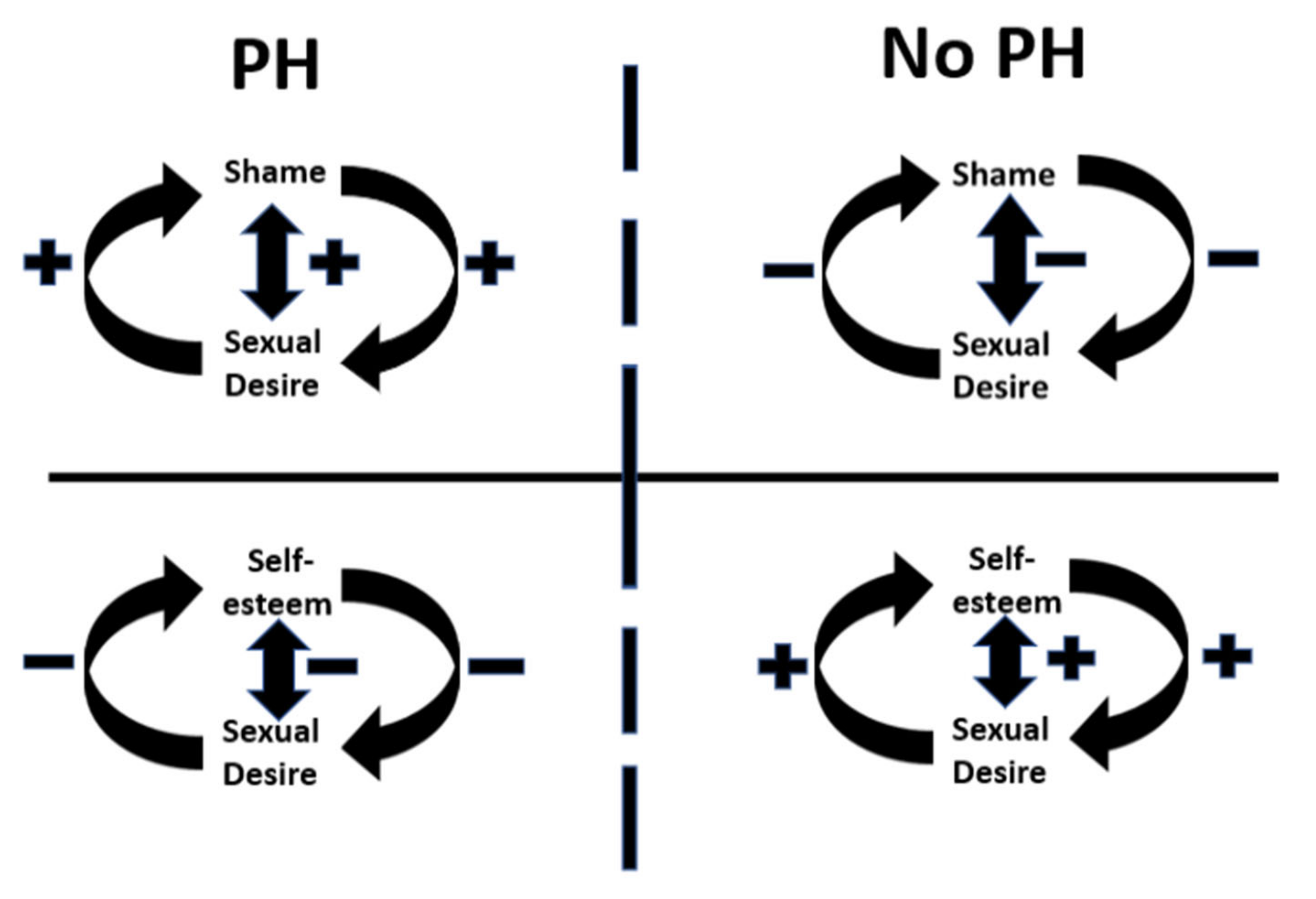
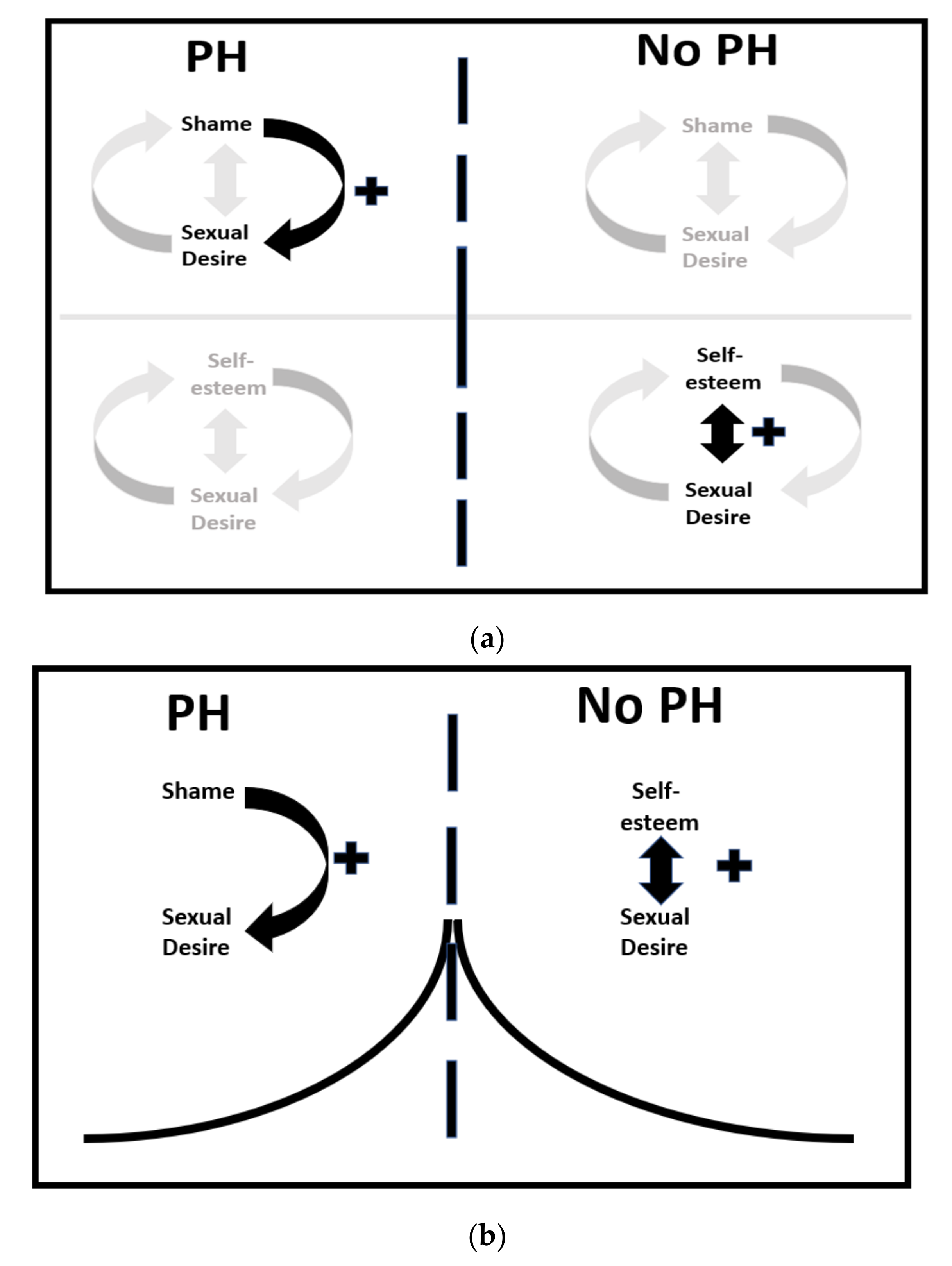
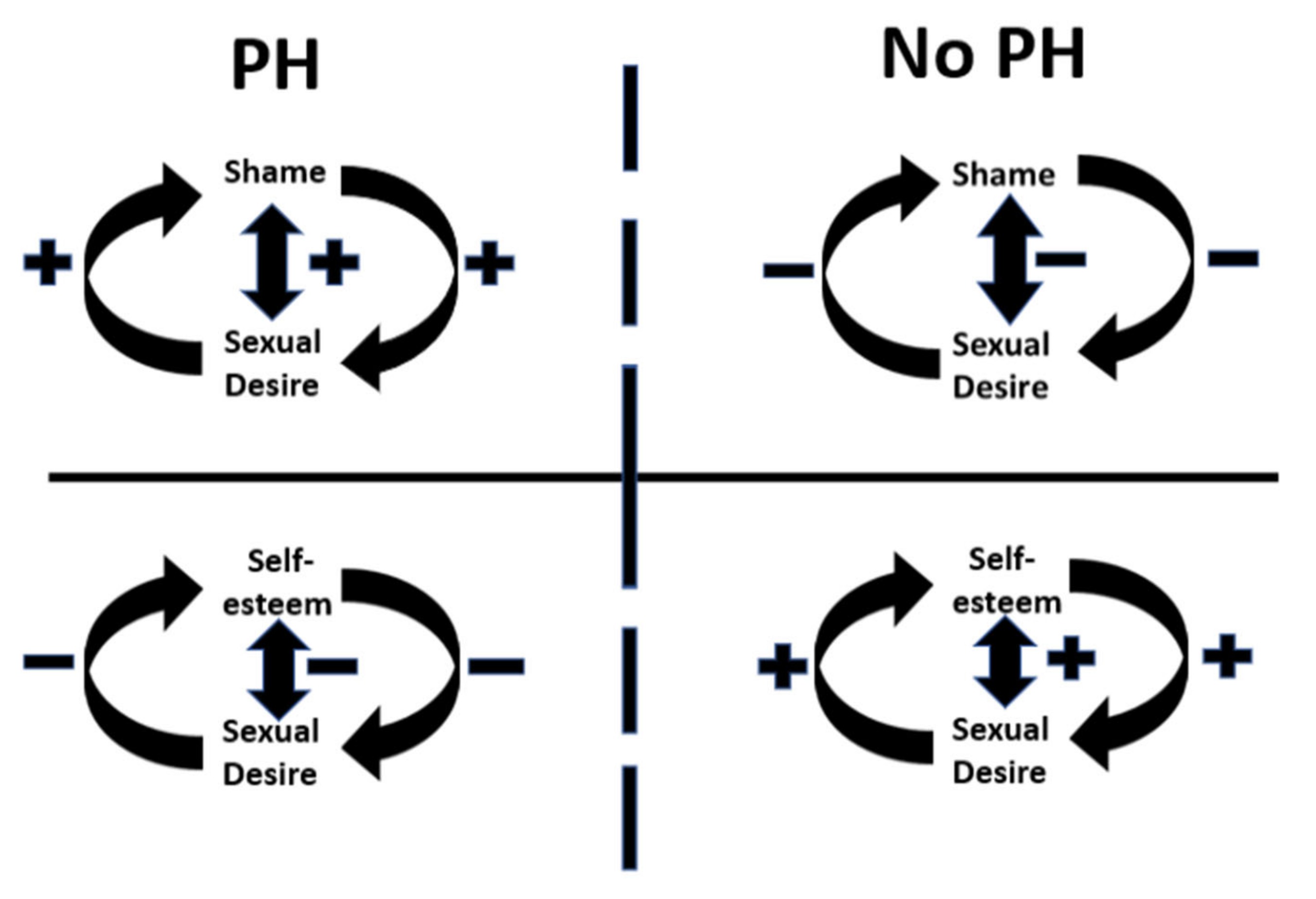
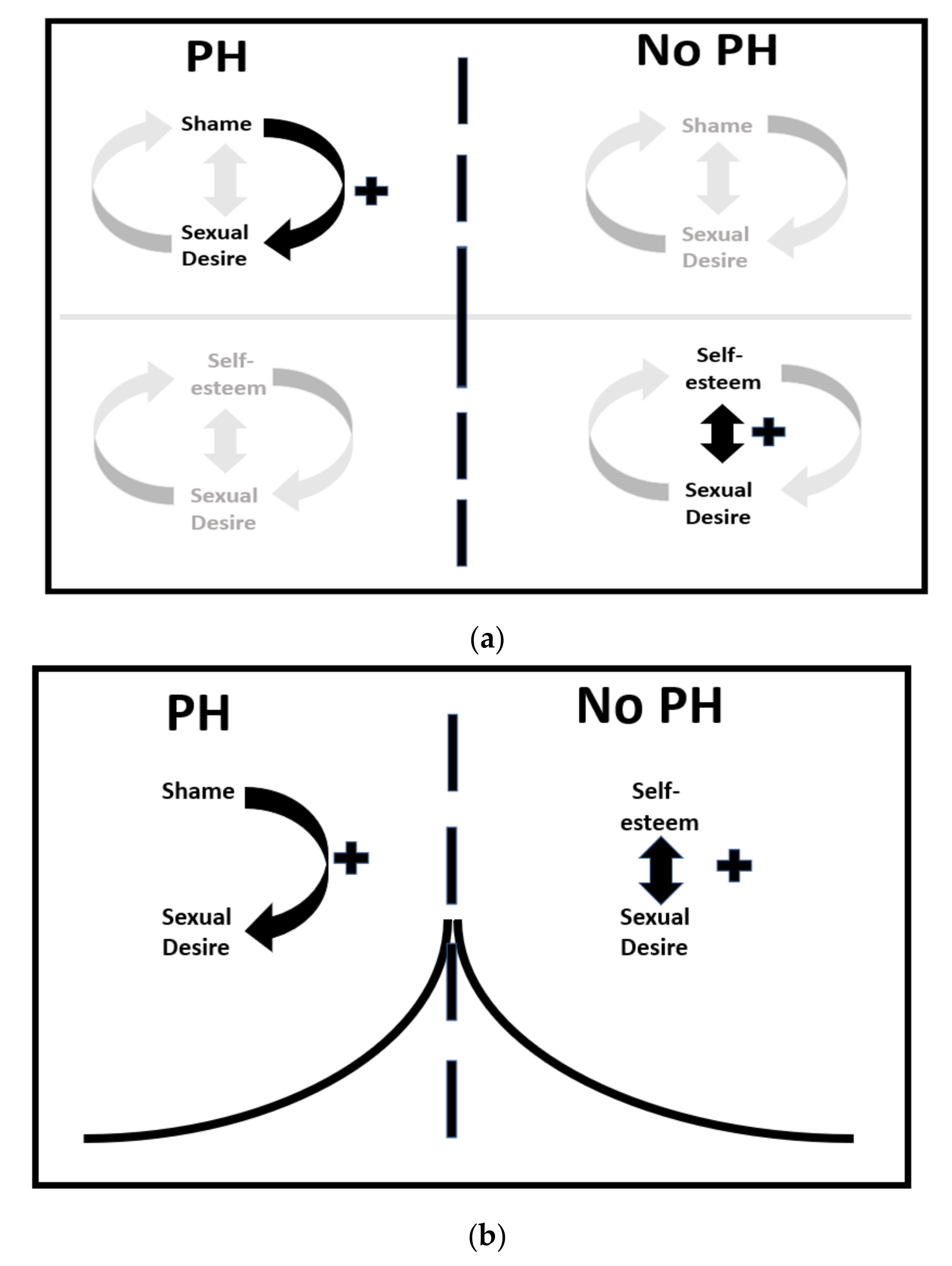
4.3. The Split Pleasure/Shame Model
4.4. Limitations
4.5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nimbi, F.M.; Tripodi, F.; Rossi, R.; Navarro-Cremades, F.; Simonelli, C. Male sexual desire: An overview of biological, psychological, sexual, relational, and cultural factors influencing desire. Sex. Med. Rev. 2020, 8, 59–91. [Google Scholar] [CrossRef]
- Levine, S.B. Reexploring the concept of sexual desire. J. Sex Marital Ther. 2002, 28, 39–51. [Google Scholar] [CrossRef]
- Winters, J.; Christoff, K.; Gorzalka, B.B. Dysregulated sexuality and high sexual desire: Distinct constructs? Arch. Sex. Behav. 2010, 39, 1029–1043. [Google Scholar] [CrossRef] [PubMed]
- Van Lankveld, J.; Jacobs, N.; Thewissen, V.; Dewitte, M.; Verboon, P. The associations of intimacy and sexuality in daily life. J. Soc. Pers. Relatsh. 2018, 35, 557–576. [Google Scholar] [CrossRef] [PubMed]
- Everaerd, W.; Both, S.; Laan, E. The experience of sexual emotions. Annu. Rev. Sex Res. 2006, 17, 183–199. [Google Scholar] [CrossRef]
- Kuppens, P.; Verduyn, P. Emotion dynamics. Curr. Opin. Psychol. 2017, 17, 22–26. [Google Scholar] [CrossRef]
- Bancroft, J.; Janssen, E.; Strong, D.; Carnes, L.; Vukadinovic, Z.; Long, J.S. The relation between mood and sexuality in heterosexual men. Arch. Sex. Behav. 2003, 32, 217–230. [Google Scholar] [CrossRef] [PubMed]
- Bancroft, J.; Vukadinovic, Z. Sexual addiction, sexual compulsivity, sexual impulsivity, or what? Toward a theoretical model. J. Sex Res. 2004, 41, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Janssen, E.; Macapagal, K.R.; Mustanski, B. Individual Differences in the Effects of Mood on Sexuality: The Revised Mood and Sexuality Questionnaire (MSQ-R). J. Sex Res. 2013, 50, 676–687. [Google Scholar] [CrossRef] [Green Version]
- Brom, M.; Laan, E.; Everaerd, W.; Spinhoven, P.; Trimbos, B.; Both, S. The influence of emotion upregulation on the expectation of sexual reward. J. Sex. Med. 2016, 13, 105–119. [Google Scholar] [CrossRef]
- Adams, M.; Robinson, D.W. Shame reduction, affect regulation, and sexual boundary development: Essential building blocks of sexual addiction treatment. Sex. Addict. Compuls. 2001, 8, 23–44. [Google Scholar] [CrossRef]
- Gilliland, R.; South, M.; Carpenter, B.N.; Hardy, S.A. The Roles of Shame and Guilt in Hypersexual Behavior. Sex. Addict. Compuls. 2011, 18, 12–29. [Google Scholar] [CrossRef] [Green Version]
- Van Zessen, G. Als Seks Verslavend Wordt; Boom: Amsterdam, The Netherlands, 2012. [Google Scholar]
- Van Zessen, G. Seksverslaving: Casuïstiek; Brave New Books: Amsterdam, The Netherlands, 2017. [Google Scholar]
- Van Tuijl, P.; Tamminga, A.; Meerkerk, G.J.; Verboon, P.; Leontjevas, R.; Van Lankveld, J. Three diagnoses for problematic hypersexuality; which criteria predict help-seeking gehavior? Int. J. Environ. Res. Public Health 2020, 17, 6907. [Google Scholar] [CrossRef]
- Castro-Calvo, J.; Gil-Llario, M.D.; Giménez-García, C.; Gil-Juliá, B.; Ballester-Arnal, R. Occurrence and clinical characteristics of Compulsive Sexual Behavior Disorder (CSBD): A cluster analysis in two independent community samples. J. Behav. Addict. 2020, 9, 446–468. [Google Scholar] [CrossRef] [PubMed]
- Carnes, P. Don’t Call It Love, 1st ed.; Penguin Random House: New York, NY, USA, 1992. [Google Scholar]
- Park, B.; Wilson, G.; Berger, J.; Christman, M.; Reina, B.; Bishop, F.; Klam, W.; Doan, A. Is Internet pornography causing sexual dysfunctions? A review with clinical reports. Behav. Sci. 2016, 6, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wéry, A.; Schimmenti, A.; Karila, L.; Billieux, J. Where the mind cannot dare: A case of addictive use of online pornography and its relationship with childhood trauma. J. Sex Marital Ther. 2018, 45, 114–127. [Google Scholar] [CrossRef] [PubMed]
- Meerkerk, G.-J.; van den Ende, D.V.M.; Altenburg, M.; Schoenmakers, T.M. De Opwinding Voorbij. Aard, Ernst En Omvang Van Gebruik En Problematisch Gebruik Van Online Pornografie in Nederland; IVO: Rotterdam, The Netherlands, 2011. [Google Scholar]
- Hald, G.M.; Malamuth, N.M. Self-perceived effects of pornography consumption. Arch. Sex. Behav. 2007, 37, 614–625. [Google Scholar] [CrossRef]
- Rosenberg, M. Society and the Adolescent Self-Image; Princeton University Press: Princeton, NJ, USA, 1965. [Google Scholar]
- Mark, K.P.; Lasslo, J.A. Maintaining sexual desire in long-term relationships: A systematic review and conceptual model. J. Sex Res. 2018, 55, 563–581. [Google Scholar] [CrossRef]
- Steidle, C.P.; Stecher, V.J.; Pace, C.; Tseng, L.J. Correlation of improved erectile function and rate of successful intercourse with improved emotional well-being assessed with the Self-Esteem And Relationship questionnaire in men treated with sildenafil for erectile dysfunction and stratified by age. Curr. Med. Res. Opin. 2006, 22, 939–948. [Google Scholar] [CrossRef]
- Tarkowska, M.; Głowacka-Mrotek, I.; Nowikiewicz, T.; Monastyrska-Waszak, E.; Gastecka, A.; Goch, A.; Zegarski, W. Sexual functioning and self-esteem in women after mastectomy—A single-centre, non-randomised, cross-sectional study. Współczesna Onkol. 2020, 24, 106–111. [Google Scholar] [CrossRef]
- Reid, R.C.; Harper, J.M.; Anderson, E.H. Coping strategies used by hypersexual patients to defend against the painful effects of shame. Clin. Psychol. Psychother. 2009, 16, 125–138. [Google Scholar] [CrossRef] [PubMed]
- Droubay, B.A.; Shafer, K.; Butters, R.P. Sexual desire and subjective distress among pornography consumers. J. Sex Marital Ther. 2020, 46, 773–792. [Google Scholar] [CrossRef] [PubMed]
- Reid, R.C. Differentiating emotions in a sample of men in treatment for hypersexual behavior. J. Soc. Work. Pract. Addict. 2010, 10, 197–213. [Google Scholar] [CrossRef]
- Reid, R.C.; Stein, J.A.; Carpenter, B.N. Understanding the roles of shame and neuroticism in a patient sample of hypersexual men. J. Nerv. Ment. Dis. 2011, 199, 263–267. [Google Scholar] [CrossRef] [PubMed]
- Reid, R.C.; Temko, J.; Moghaddam, J.F.; Fong, T.W. Shame, rumination, and self-compassion in men assessed for hypersexual disorder. J. Psychiatr. Pract. 2014, 20, 260–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Lankveld, J.; Hubben, D.; Dewitte, M.; Dingemans, M.E.; den Butter, C.; Grauvogl, A. Effects of Partner Presence in the Lab on Sexual Arousal. J. Sex Med. 2014, 11, 697–708. [Google Scholar] [CrossRef] [PubMed]
- Csikszentmihalyi, M. Validity and Reliability of the Experience-Sampling Method; Springer: New York, NY, USA, 2014; ISBN 978-94-017-9087-1. [Google Scholar]
- Verhagen, S.J.W.; Hasmi, L.; Drukker, M.; Van Os, J.; Delespaul, P.A.E.G. Use of the experience sampling method in the context of clinical trials. Evid. Based Ment. Health 2016, 19, 86–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graham, C.A.; Sanders, S.A.; Milhausen, R.R.; McBride, K.R. Turning On and Turning Off: A Focus Group Study of the Factors That Affect Women’s Sexual Arousal. Arch. Sex. Behav. 2004, 33, 527–538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kernis, M.H. TARGET ARTICLE: Toward a conceptualization of optimal self-esteem. Psychol. Inq. 2003, 14, 1–26. [Google Scholar] [CrossRef]
- Mazereel, V.; Vansteelandt, K.; Menne-Lothmann, C.; Decoster, J.; Derom, C.; Thiery, E.; Rutten, B.P.; Jacobs, N.; Van Os, J.; Wichers, M.; et al. The complex and dynamic interplay between self-esteem, belongingness and physical activity in daily life: An experience sampling study in adolescence and young adulthood. Ment. Health Phys. Act. 2021, 21, 100413. [Google Scholar] [CrossRef]
- Thewissen, V.; Bentall, R.P.; Oorschot, M.; à Campo, J.; Van Lierop, T.; Van Os, J.; Myin-Germeys, I. Emotions, self-esteem, and paranoid episodes: An experience sampling study. British. J. Clin. Psychol. 2011, 50, 178–195. [Google Scholar] [CrossRef] [PubMed]
- Kisjes, H.; Kruk, M. Lust AlsLast; Lucht BV: Hilversum, The Netherlands, 2021. [Google Scholar]
- Walton, M.T.; Cantor, J.M.; Bhullar, N.; Lykins, A.D. Hypersexuality: A critical review and introduction to the “Sexhavior Cycle”. Arch. Sex. Behav. 2017, 46, 2231–2251. [Google Scholar] [CrossRef]
- Grubbs, J.B.; Perry, S.L. Moral incongruence and pornography use: A critical review and integration. J. Sex Res. 2018, 56, 29–37. [Google Scholar] [CrossRef] [Green Version]
- Kahneman, D.; Krueger, A.B.; Schkade, D.A.; Schwarz, N.; Stone, A.A. A Survey Method for Characterizing Daily Life Experience: The Day Reconstruction Method. Science 2004, 306, 1776–1780. [Google Scholar] [CrossRef] [PubMed]
- Epskamp, S.; van Borkulo, C.D.; van der Veen, D.C.; Servaas, M.N.; Isvoranu, A.-M.; Riese, H.; Cramer, A.O.J. Personalized Network Modeling in Psychopathology: The Importance of Contemporaneous and Temporal Connections. Clin. Psychol. Sci. 2018, 6, 416–427. [Google Scholar] [CrossRef] [PubMed]
- Delespaul, P.A.E.G. Assessing Schizophrenia in Daily Life: The Experience Sampling Method; Universitaire Pers: Maastricht, The Netherlands, 1995. [Google Scholar]
- McDonald, R.P. Test-Theory: A Unified Approach; Lawrence Erlbaum: Mahwah, NJ, USA, 1999. [Google Scholar]
- Wiley, J.F. MultilevelTools: Multilevel and Mixed Effects Model Diagnostics and Effect Sizes. R package version 0.1.1. 2020. Available online: https://CRAN.R-project.org/package=multilevelTools (accessed on 30 November 2021).
- Rosseel, Y. lavaan: An RPackage for Structural Equation Modeling. J. Stat. Softw. 2012, 48, 1. [Google Scholar] [CrossRef] [Green Version]
- R Core Team R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing, Vienna, Austria. 2021. Available online: https://www.R-project.org/ (accessed on 30 November 2021).
- Meerkerk, G.J.; Van den Eijnden, R.J.J.M.; Vermulst, A.A.; Garretsen, H.F.L. The compulsive internet use scale (CIUS): Some psychometric properties. CyberPsychol. Behav. 2009, 12, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peters, G. Ufs: Quantitative Analysis Made Accessible. R Package Version 0.4.3. 2021. Available online: https://CRAN.R-project.org/package=ufs (accessed on 30 November 2021).
- Bates, D.; Maechler, M.; Bolker, B.; Walker, S. Fitting linear mixed-effects models using lme4. J. Stat. Softw. 2015, 67, 1–48. [Google Scholar] [CrossRef]
- Hamaker, E.L.; Grasman, R.P.P.P. To center or not to center? Investigating inertia with a multilevel autoregressive model. Front. Psychol. 2015, 5, 1492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Granger, C.W.J. Investigating Causal Relations by Econometric Models and Cross-spectral Methods. Econometrica 1969, 37, 424. [Google Scholar] [CrossRef]
- Aguinis, H.; Gottfredson, R.K.; Culpepper, S.A. Best-practice recommendations for estimating cross-level interaction effects using multilevel modeling. J. Manag. 2013, 39, 1490–1528. [Google Scholar] [CrossRef]
- Hox, J.J.; Moerbeek, M.; Van de Schoot, R.; Van de Schoot, R. Multilevel Analysis; Taylor & Francis: Beijing, China, 2017. [Google Scholar]
- Lenth, R. Emmeans: Estimated Marginal Means, Aka Least-Squares Means. R Package Version 1.5.1. 2020. Available online: https://CRAN.R-project.org/package=emmeans (accessed on 30 November 2021).
- Molenaar, P.C.M. A manifesto on psychology as idiographic science: Bringing the person back into scientific psychology, this time forever. Meas. Interdiscip. Res. Perspect. 2004, 2, 201–218. [Google Scholar] [CrossRef]
- Petrican, R.; Burris, C.T.; Moscovitch, M. Shame, sexual Compulsivity, and eroticizing flirtatious others: An Experimental Study. J. Sex Res. 2013, 52, 98–109. [Google Scholar] [CrossRef] [PubMed]
- Kraus, S.W.; Krueger, R.B.; Briken, P.; First, M.B.; Stein, D.J.; Kaplan, M.S.; Voon, V.; Abdo, C.H.N.; Grant, J.E.; Atalla, E.; et al. Compulsive sexual behaviour disorder in the ICD-11. World Psychiatry 2018, 1, 109–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Challenges in Sexual and Reproductive Health: Technical Consultation on Sexual Health. 2002. Geneva: World Health Organization. Available online: http://www.who.int/reproductive-health/publications/sexualhealth/defining_sh.pdf (accessed on 30 November 2021).
- Williams, D.J.; Thomas, J.N.; Prior, E.E. Are sex and pornography addiction valid disorders? Adding a leisure science perspective to the sexological critique. Leis. Sci. 2020, 42, 306–321. [Google Scholar] [CrossRef]
- Goodman, A. Sexual Addiction: Designation and Treatment. J. Sex. Marital Ther. 1992, 18, 303–314. [Google Scholar] [CrossRef]
- Kafka, M.P. Hypersexual Disorder: A Proposed Diagnosis for DSM-V. Arch. Sex. Behav. 2010, 39, 377–400. [Google Scholar] [CrossRef]
- Kafka, M.P. What happened to hypersexual disorder? Arch. Sex. Behav. 2014, 43, 1259–1261. [Google Scholar] [CrossRef]
- Bőthe, B.; Potenza, M.N.; Griffiths, M.D.; Kraus, S.W.; Klein, V.; Fuss, J.; Demetrovics, Z. The development of the Compulsive Sexual Behavior Disorder Scale (CSBD-19): An ICD-11 based screening measure across three languages. J. Behav. Addict. 2020, 9, 247–258. [Google Scholar] [CrossRef] [PubMed]
- Reis, H.T.; Gable, S.L. Event-sampling and other methods for studying everyday experience. In Handbook of Research Methods in Social and Personality Psychology; Reis, H.T., Judd, C.M., Reis, H.T., Judd, C.M., Eds.; Cambridge University Press: New York, NY, USA, 2000; pp. 190–222. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Descriptives (Min–Max) | M (SD) | Self-Esteem | Shame | Age | Sexual Activity |
|---|---|---|---|---|---|
| Sexual desire (1–7) 1 | 1.83 (0.85) | −0.08 | 0.22 ** | −0.17 * | 0.49 *** |
| Self-esteem (1–7) 1 | 5.37 (0.80) | −0.23 ** | 0.05 | −0.02 | |
| Shame (1–7) 1 | 1.29 (0.68) | −0.25 ** | 0.37 *** | ||
| Age (yrs, 18–68) | 39.5 (12.3) | −0.34 *** | |||
| Sexual activity (p/wk, 0–21) | 2.62 (2.98) |
| Women (1) n = 87 | Men (2) n = 46 | Men with NH (3) n = 10 | Men with PH (4) n = 11 | F- and p-Value ANOVA 2 | |
|---|---|---|---|---|---|
| M (SD) | M (SD) | M (SD) | M (SD) | Group Differences | |
| Time-Varying Variables | |||||
| Sexual desire 1 | 1.59 (0.75) | 2.11 (0.94) | 1.81 (0.61) | 2.52 (0.82) | F(3150) = 7.2; p < 0.001 |
| d (1–2) = −0.4; d (1–4) = −1.3 | |||||
| Self-esteem 1 | 5.37 (0.71) | 5.53 (0.70) | 5.25 (0.90) | 4.81 (1.43) | F (3150) = 2.57; p = 0.06 |
| d (2–4) = 0.7 | |||||
| Shame 1 | 1.16 (0.29) | 1.19 (0.40) | 1.34 (0.58) | 2.62 (1.76) | F(3150) = 26.2; p < 0.001 |
| d (1–4) = −1.3; d (2–4) = −0.4; d (3–4) = −1.4 | |||||
| Person Level Variables | |||||
| Age (yrs) | 39.3 (10.7) | 46.2 (11.4) | 24.1 (6.5) | 24.0 (3.9) | F(3148) = 20.2; p < 0.001 |
| d (1–2) = −0.9; d (1–3) = 1.1; d (1–4) = 1.3; d (2–3) = 1.7; d (2–4) = 1.8 | |||||
| Compulsive porn use (p/wk) | - | - | 1.37 (0.22) | 2.10 (0.35) | t (17.2) = −5.7; p < 0.001 |
| d = 2.6 | |||||
| Sexual activity (p/wk) | 1.93 (1.98) | 2.22 (2.11) | 3.30 (2.00) | 9.09 (5.22) | F(3150) = 30.4; p < 0.001 |
| d (1–4) = −3.3; d (2–4) = −3.4; d (3–4) = −1.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Tuijl, P.; Verboon, P.; van Lankveld, J.J.D.M. Associations between Fluctuating Shame, Self-Esteem, and Sexual Desire: Comparing Frequent Porn Users and a General Population Sample. Sexes 2022, 3, 1-19. https://doi.org/10.3390/sexes3010001
van Tuijl P, Verboon P, van Lankveld JJDM. Associations between Fluctuating Shame, Self-Esteem, and Sexual Desire: Comparing Frequent Porn Users and a General Population Sample. Sexes. 2022; 3(1):1-19. https://doi.org/10.3390/sexes3010001
Chicago/Turabian Stylevan Tuijl, Piet, Peter Verboon, and Jacques J. D. M. van Lankveld. 2022. "Associations between Fluctuating Shame, Self-Esteem, and Sexual Desire: Comparing Frequent Porn Users and a General Population Sample" Sexes 3, no. 1: 1-19. https://doi.org/10.3390/sexes3010001
APA Stylevan Tuijl, P., Verboon, P., & van Lankveld, J. J. D. M. (2022). Associations between Fluctuating Shame, Self-Esteem, and Sexual Desire: Comparing Frequent Porn Users and a General Population Sample. Sexes, 3(1), 1-19. https://doi.org/10.3390/sexes3010001