The Handling and Sampling of Radical Cystectomy Specimens: A Standardized Approach for Pathological Evaluation

 , ,
, ,  ,
, {kind=link}
{kind=link}
Abstract
1. Introduction
2. Before Starting
- The correct identification of the material contained in each container sent to the pathology laboratory, ensured by the proper labeling of the containers. The contents must be accurately documented in the accompanying request form, whether paper-based or digital.
- The communication of all relevant clinical, anamnestic, and radiological information necessary for the preparation of the histopathological diagnosis.
3. Specimen Fixation
- -
- Bladder cavity distension with an injection of 150–250 mL of buffered formalin (e.g., using a large-bore needle through the bladder dome or a Foley catheter through the urethra), followed by the clamping of the distal urethra. This approach ensures the proper fixation of the mucosa and any tumors within the bladder lumen while also promoting bladder wall distension for better macroscopic evaluation [1,2,3,4]. The specimen is then immersed overnight in an adequately sized container filled with formalin [3].
- -
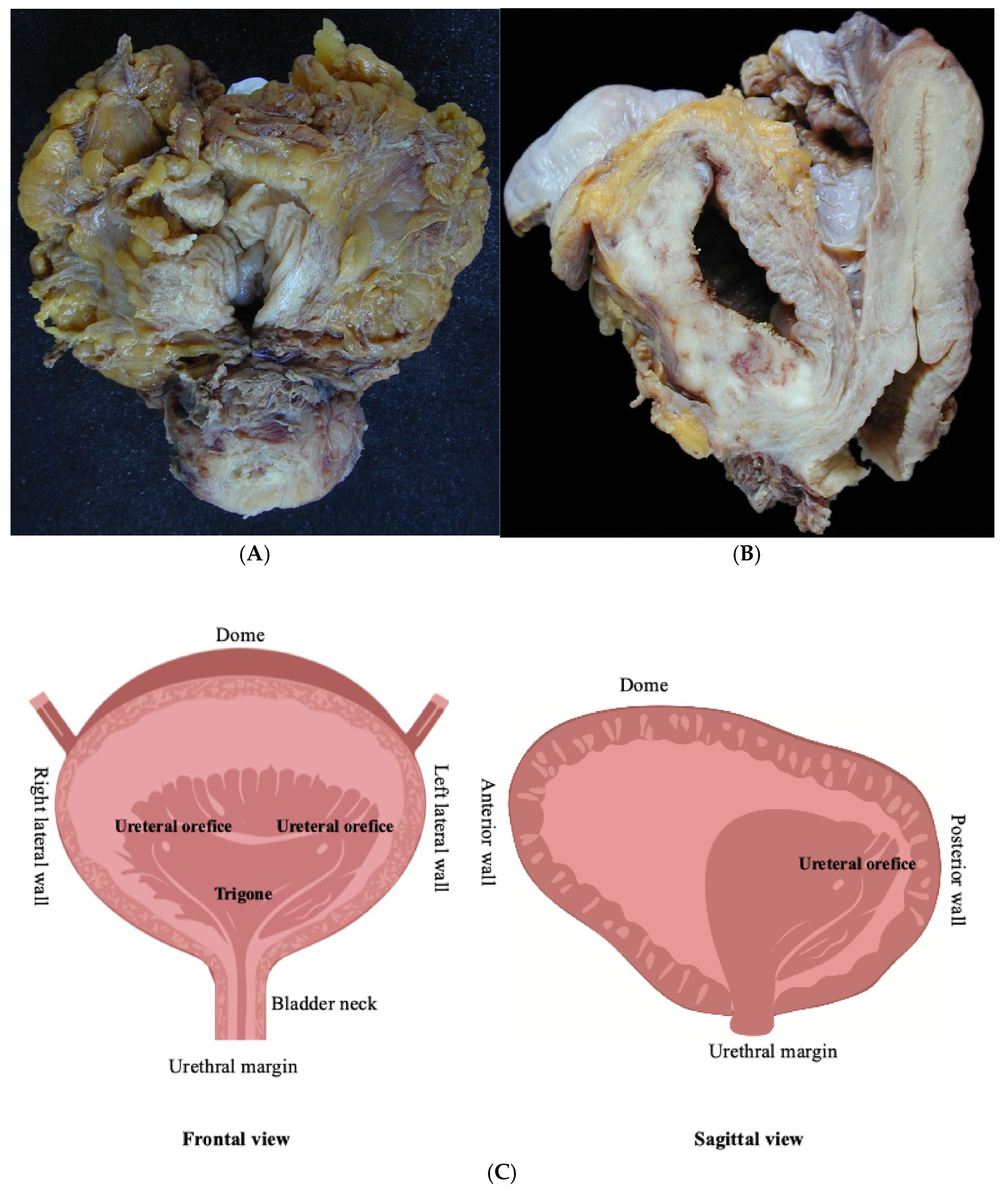
- Before immersion in a container with an adequate volume of formalin, the bladder should be opened anteriorly from the urethra to the bladder dome to ensure optimal fixation in an adequate volume of formalin [2].
4. Specimen Description
- -
- The dimensions of the bladder and any other removed organs do not have a universally accepted recommendation. This is because the clinical utility of such measurements is limited, along with the inherent differences in specimen size before and after formalin fixation [1,4,5,6,7,8,9,10]. Current EAU guidelines recommend that, in female cystectomy specimens, the length of the urethral segment removed en bloc with the bladder should be checked, preferably by a urological surgeon [11].
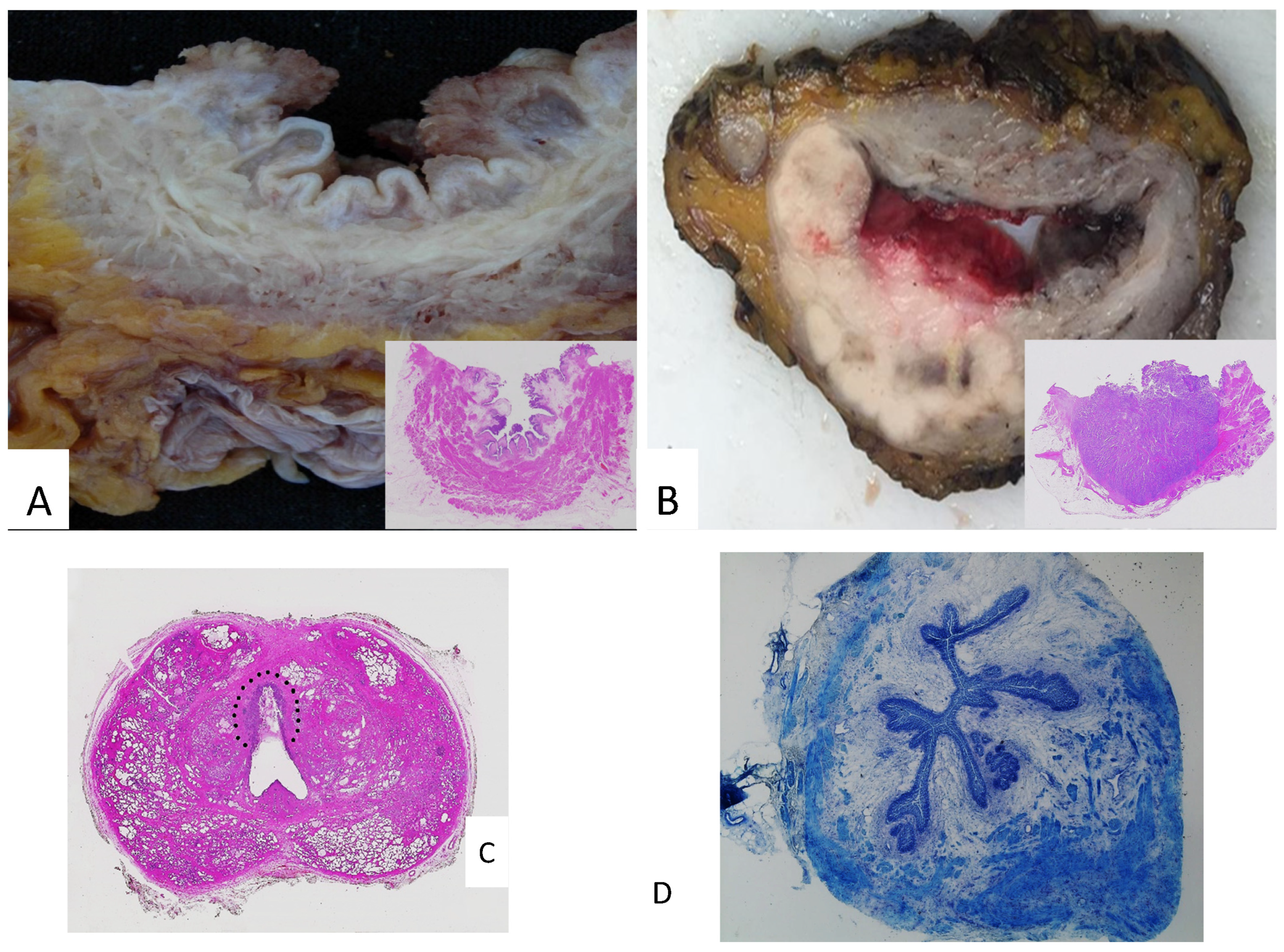
- -
- A description of the internal bladder surface (Figure 2A,B) should be carried out: maximum tumor size, location, deepest invasion, and macroscopic appearance (flat, papillary, solid nodular, polypoid, or ulcerated), along with the status of the remaining mucosa and surgical margins. In addition to the maximum tumor dimension, it is advisable to report additional tumor measurements, as tumor diameter is a predictor of recurrence and disease-specific survival [12].
- -
- The tumor location is particularly relevant when it is in the bladder dome, especially in the absence of a previous TUR histological examination, as differential diagnosis with urachal carcinoma is required. The latter has specific sampling and staging protocols [13].
- -
- The presence or absence of the macroscopic invasion of perivesical adipose tissue or the serosa (qualifying the tumor as pT3b), as well as any lymph nodes or tumor deposits in perivesical adipose tissue, which should be carefully examined [4]. Suspected perivesical adipose tissue invasion by urothelial carcinoma should be distinguished microscopically from other conditions (e.g., peritumoral fibrosis) [13]. At this stage, inking the margin closest to the tumor is recommended [10]. Furthermore, perivesical fat should be carefully examined for lymph nodes or tumor deposits, which should be sampled accordingly [10].
- -
- The description of the internal surface of the ureteral stumps, after longitudinal opening with scissors [4].
- -
- The iliac–obturator lymph nodes removed concurrently. The lymphadenectomy specimen should be measured or, alternatively, weighed, then palpated and examined to isolate lymph nodes within the fibroadipose tissue [10]. The number and characteristics of the lymph nodes (e.g., the presence of macroscopic metastasis) should be reported. The lymph node diameter should be recorded if it cannot be determined on a histological slide [10].
5. Before Specimen Sampling
6. Specimen Sampling
- -
- Tumor (if macroscopically evident): At least one section per centimeter of tumor, with the appropriate documentation of the macroscopically identified extent within the bladder wall for accurate pathologic staging [16]. This sampling aims to assess the tumor grade and histotype thoroughly. Some authors also recommend sampling apparently normal perilesional tissue with a margin of at least 1 cm [8].
- -
- Seemingly normal mucosa from different bladder wall regions to detect occult multifocal carcinoma and/or urothelial carcinoma in situ (CIS). However, the extensive random sampling of macroscopically normal tissue is not recommended, as CIS identification in the bladder generally has limited clinical utility [4].
- -
- Ureteral and urethral surgical resection margins should be sampled to identify any in situ or invasive tumors that are not macroscopically evident. Varma et al. recommend sampling the prostatic urethral margin of RC specimens with a slightly thicker section, as the distal prostatic urethra tends to retract after surgical resection and formalin fixation [4]. Both ureteral and urethral margins are obtained by shaving unless they have already been evaluated by frozen sections [9].
- -
- Associated organs in the RC surgical specimen (see above), regardless of the presence of a macroscopically detectable tumor. This aims to rule out the microscopic extension of bladder cancer and/or other primary tumors in adjacent organs, as well as to accurately determine the pathological stage [19].
- -
- Iliac–obturator lymph nodes: while a single section is sufficient for each lymph node with a macroscopically detectable metastasis, all macroscopically negative lymph nodes should be entirely submitted, as lymph node involvement may be microscopic and is used as an indication for adjuvant therapy [1,9,18].
7. Handling the Post-Chemotherapy Bladder
8. Issue in Prostate Sampling
9. Frozen Sections
10. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Athanazio, D.A.; Amorim, L.S.; da Cunha, I.W.; Távora, F.; Cavalcanti, M.S.; Bezerra, S.M.; Assis, E.; da Silva, I.C.; Korkes, F.; Fernandes, R.; et al. Handling and pathology reporting guidelines for bladder epithelial neoplasms—Recommendations from the Brazilian Society of Pathology / Brazilian Society of Urology / Brazilian Society of Clinical Oncology. Surg. Exp. Pathol. 2024, 7, 8. [Google Scholar] [CrossRef]
- Chandra, A.; Griffiths, D.; McWilliam, L.J. Best practice: Gross examination and sampling of surgical specimens from the urinary bladder. J. Clin. Pathol. 2010, 63, 475–479. [Google Scholar] [CrossRef] [PubMed]
- Murali, D.V.S.D.; Chandra, D.A.; McWilliam, D.L. Dataset for Histopathological Reporting of Tumours of the Urinary Collecting System (Renal Pelvis, Ureter, Urinary Bladder and Urethra). Report: Royal College of Pathologists; 2021; ISBN 978-94-92671-23-3. Available online: https://www.rcpath.org/profession/guidelines/cancer-datasets-and-tissue-pathways.html (accessed on 15 February 2025).
- Varma, M.; Dormer, J. Macroscopy of specimens from the genitourinary system. J. Clin. Pathol. 2024, 77, 177–183. [Google Scholar] [PubMed]
- Griffin, J.; Hartmann, A.; Comperat, E. Variation in cystectomy pathology reporting practice—Results from an international survey of 212 pathologists. Virchows Archiv. 2024, 485, 879–888. [Google Scholar]
- Hussain, S.A.; Oughton, J.B.; Whelan, R.S.; Green, A.; Hubbard, R.; Kennish, S.; Senior, E.; Kendall, J.; McCready, D.; Collinson, F.J.; et al. INVEST: A phase Ib window of opportunity study of atezolizumab administered either intravesically or direct tumour injection in patients with bladder cancer prior to radical cystectomy. J. Clin. Oncol. 2024, 42, TPS710-TPS. [Google Scholar] [CrossRef]
- Compérat, E.; Oszwald, A.; Wasinger, G.; Hansel, D.E.; Montironi, R.; van der Kwast, T.; Witjes, J.A.; Amin, M.B. Updated pathology reporting standards for bladder cancer: Biopsies, transurethral resections and radical cystectomies. World J. Urol. 2022, 40, 915–927. [Google Scholar]
- Aron, M.; Zhou, M. Urothelial Carcinoma: Update on Staging and Reporting, and Pathologic Changes Following Neoadjuvant Chemotherapies. Surg. Pathol. Clin. 2022, 15, 661–679. [Google Scholar]
- Cho, Y.M.; Ro, J.Y. Bladder Cancer: Specimen Handling and Reporting. In Urinary Bladder Pathology; Zhou, H., Guo, C.C., Ro, J.Y., Eds.; Springer International Publishing: Cham, Switzerland, 2021; pp. 211–227. [Google Scholar]
- Sanders, M.L.; Warren, A.Y.; Varma, M. Uropathology macroscopy: A pragmatic approach. Diagn. Histopathol. 2020, 26, 312–319. [Google Scholar]
- (EAU) EAoU. EAU Guidelines. Edn. Presented at the EAU Annual Congress Paris 2024. Report Arnhem; EAU Guidelines Office: Arnhem, The Netherlands, 2024; ISBN 978-94-92671-23-3. Available online: https://uroweb.org/guidelines (accessed on 16 February 2025).
- Soave, A.; John, L.M.; Dahlem, R.; Minner, S.; Engel, O.; Schmidt, S.; Kluth, L.A.; Fisch, M.; Rink, M. The Impact of Tumor Diameter and Tumor Necrosis on Oncologic Outcomes in Patients With Urothelial Carcinoma of the Bladder Treated With Radical Cystectomy. Urology 2015, 86, 92–98. [Google Scholar] [CrossRef]
- Compérat, E.; Srigley, J.R.; Brimo, F.; Delahunt, B.; Koch, M.; Lopez-Beltran, A.; Reuter, V.; Samaratunga, H.; Shanks, J.H.; Tsuzuki, T.; et al. Dataset for the reporting of carcinoma of the bladder-cystectomy, cystoprostatectomy and diverticulectomy specimens: Recommendations from the International Collaboration on Cancer Reporting (ICCR). Virchows Arch. 2020, 476, 521–534. [Google Scholar]
- Cheng, L.; Montironi, R.; Davidson, D.D.; Lopez-Beltran, A. Staging and reporting of urothelial carcinoma of the urinary bladder. Mod. Pathol. 2009, 22 (Suppl. S2), S70–S95. [Google Scholar] [PubMed]
- Mazzucchelli, R.; Scarpelli, M.; Lopez-Beltran, A.; Cheng, L.; Di Primio, R.; Montironi, R. A contemporary update on pathology reporting for urinary bladder cancer. Int. J. Immunopathol. Pharmacol. 2012, 25, 565–571. [Google Scholar]
- Amin, M.B.E.S.; Greene, F.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; et al. AJCC Cancer Staging Manual, 8th ed.; Springer: New York, NY, USA, 2016. [Google Scholar]
- Gaisa, N.T.; Wilms, H.; Wild, P.J.; Jakse, G.; Heidenreich, A.; Knuechel, R. In cystectomy specimens with bladder cancer whole organ embedding increases the detection rate of histopathological parameters, but not of those with prognostic significance. Virchows Arch. 2015, 466, 423–432. [Google Scholar] [PubMed]
- Pathologists CoA. Cancer Protocol Templates. 2023. Available online: https://www.cap.org/protocols-and-guidelines/cancer-reporting-tools/cancer-protocol-templates (accessed on 1 January 2020).
- Kulkarni, G.S.; Black, P.C.; Sridhar, S.S.; Zlotta, A.R.; Shayegan, B.; Rendon, R.A.; Chung, P.; Van der Kwast, T.; Alimohamed, N.; Fradet, Y.; et al. 2025 Canadian Urological Association Expert Report: Muscle-invasive bladder cancer. Can. Urol. Assoc. J. 2025, 19, E1–E16. [Google Scholar] [PubMed]
- Varma, M.; Williamson, S. Clinical utility of histopathology data: Urological cancers. J. Clin. Pathol. 2022, 75, 506–513. [Google Scholar]
- Saunders, K.E.; Gerken, N.; Khani, F.; Williamson, S.R.; Wobker, S.E. Current gross examination and reporting patterns of post-neoadjuvant chemotherapy cystectomy specimens: Is it time for a standardized approach? Am. J. Clin. Pathol. 2024, 161, 483–489. [Google Scholar]
- Saunders, K.E.; Cody Craig, J.; Hoerres, D.L.; Maygarden, S.J.; Wobker, S.E. Less Is More: Evaluation of Gross Examination Protocol for Cystectomy Specimens Following Neoadjuvant Chemotherapy. Am. J. Clin. Pathol. 2022, 158, 383–388. [Google Scholar] [CrossRef]
- Petrelli, F.; Coinu, A.; Cabiddu, M.; Ghilardi, M.; Vavassori, I.; Barni, S. Correlation of pathologic complete response with survival after neoadjuvant chemotherapy in bladder cancer treated with cystectomy: A meta-analysis. Eur. Urol. 2014, 65, 350–357. [Google Scholar]
- Van Ginkel, N.; Hermans, T.J.N.; Meijer, D.; Boormans, J.L.; Voortman, J.; Mertens, L.; van Beek, S.C.; Vis, A.N. Survival outcomes of patients with muscle-invasive bladder cancer according to pathological response at radical cystectomy with or without neo-adjuvant chemotherapy: A case-control matching study. Int. Urol. Nephrol. 2022, 54, 3145–3152. [Google Scholar] [CrossRef]
- Nitta, M.; Kuroda, S.; Nagao, K.; Higure, T.; Zakoji, H.; Miyakita, H.; Usui, Y.; Hasegawa, M.; Kawamura, Y.; Shoji, S.; et al. Effect of neoadjuvant chemotherapy in patients undergoing radical cystectomy for muscle-invasive bladder cancer: A retrospective, multi-institutional study. Jpn. J. Clin. Oncol. 2020, 50, 73–79. [Google Scholar]
- Edge, S.B. American Joint Committee on Cancer. AJCC Cancer Staging Manual, 8th ed.; Springer: New York, NY, USA, 2017. [Google Scholar]
- Ichihara, K.; Masumori, N.; Kitamura, H.; Hasegawa, T.; Tsukamoto, T. Clinical outcomes of urothelial carcinoma of the prostate detected in radical cystectomy specimens. Int. J. Clin. Oncol. 2014, 19, 152–156. [Google Scholar] [CrossRef] [PubMed]
- Knoedler, J.J.; Boorjian, S.A.; Tollefson, M.K.; Cheville, J.C.; Thapa, P.; Tarrell, R.F.; Frank, I. Urothelial carcinoma involving the prostate: The association of revised tumour stage and coexistent bladder cancer with survival after radical cystectomy. BJU Int. 2014, 114, 832–836. [Google Scholar] [CrossRef] [PubMed]
- Montironi, R.; Cheng, L.; Mazzucchelli, R.; Scarpelli, M.; Kirkali, Z.; Montorsi, F.; Lopez-Beltran, A. Critical evaluation of the prostate from cystoprostatectomies for bladder cancer: Insights from a complete sampling with the whole mount technique. Eur. Urol. 2009, 55, 1305–1309. [Google Scholar] [PubMed]
- Varinot, J.; Camparo, P.; Roupret, M.; Bitker, M.O.; Capron, F.; Cussenot, O.; Witjes, J.A.; Compérat, E. Full analysis of the prostatic urethra at the time of radical cystoprostatectomy for bladder cancer: Impact on final disease stage. Virchows Arch. 2009, 455, 449–453. [Google Scholar]
- Yoo, Y.; Kim, J.M.; Choi, E.; Park, H.S.; Cho, M.S.; Sung, S.H.; Park, S. The Effect of Complete Prostate Examination of Radical Cystoprostatectomy Specimen on the Final Stage of Urothelial Carcinoma of the Urinary Bladder and the Detection of Prostate Cancer. Arch. Pathol. Lab. Med. 2023, 147, 665–675. [Google Scholar]
- Claps, F.; Pavan, N.; Umari, P.; Rizzo, M.; Barbone, F.; Giangreco, M.; Liguori, G.; Mir, C.M.; Bussani, R.; Trombetta, C. Incidence, predictive factors and survival outcomes of incidental prostate cancer in patients who underwent radical cystectomy for bladder cancer. Minerva Urol. Nephrol. 2021, 73, 349–356. [Google Scholar]
- Montironi, R.; Lopez Beltran, A.; Mazzucchelli, R.; Cheng, L.; Scarpelli, M. Handling of radical prostatectomy specimens: Total embedding with large-format histology. Int. J. Breast Cancer. 2012, 2012, 932784. [Google Scholar]
- Mazzucchelli, R.; Marzioni, D.; Tossetta, G.; Pepi, L.; Montironi, R. Bladder Cancer Sample Handling and Reporting: Pathologist’s Point of View. Front. Surg. 2021, 8, 754741. [Google Scholar]
- Osman, Y.; El-Tabey, N.; Abdel-Latif, M.; Mosbah, A.; Moustafa, N.; Shaaban, A. The value of frozen-section analysis of ureteric margins on surgical decision-making in patients undergoing radical cystectomy for bladder cancer. BJU Int. 2007, 99, 81–84. [Google Scholar]
- Raj, G.V.; Tal, R.; Vickers, A.; Bochner, B.H.; Serio, A.; Donat, S.M.; Herr, H.; Olgac, S.; Dalbagni, G. Significance of intraoperative ureteral evaluation at radical cystectomy for urothelial cancer. Cancer 2006, 107, 2167–2172. [Google Scholar]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sanguedolce, F.; Cormio, A.; Zanelli, M.; Zizzo, M.; Palicelli, A.; Filosa, A.; Falagario, U.G.; Galosi, A.B.; Cormio, L.; Carrieri, G.; et al. The Handling and Sampling of Radical Cystectomy Specimens: A Standardized Approach for Pathological Evaluation. Methods Protoc. 2025, 8, 35. https://doi.org/10.3390/mps8020035
Sanguedolce F, Cormio A, Zanelli M, Zizzo M, Palicelli A, Filosa A, Falagario UG, Galosi AB, Cormio L, Carrieri G, et al. The Handling and Sampling of Radical Cystectomy Specimens: A Standardized Approach for Pathological Evaluation. Methods and Protocols. 2025; 8(2):35. https://doi.org/10.3390/mps8020035
Chicago/Turabian StyleSanguedolce, Francesca, Angelo Cormio, Magda Zanelli, Maurizio Zizzo, Andrea Palicelli, Alessandra Filosa, Ugo Giovanni Falagario, Andrea Benedetto Galosi, Luigi Cormio, Giuseppe Carrieri, and et al. 2025. "The Handling and Sampling of Radical Cystectomy Specimens: A Standardized Approach for Pathological Evaluation" Methods and Protocols 8, no. 2: 35. https://doi.org/10.3390/mps8020035
APA StyleSanguedolce, F., Cormio, A., Zanelli, M., Zizzo, M., Palicelli, A., Filosa, A., Falagario, U. G., Galosi, A. B., Cormio, L., Carrieri, G., & Mazzucchelli, R. (2025). The Handling and Sampling of Radical Cystectomy Specimens: A Standardized Approach for Pathological Evaluation. Methods and Protocols, 8(2), 35. https://doi.org/10.3390/mps8020035